

Abstract
Liposarcoma of the larynx is a rare entity, typically well differentiated with a good prognosis. We present a patient who presented to ENT clinic with a 3-month history of hoarseness. Contrast-enhanced computed tomography of the neck demonstrated a 2.5-cm mass of the true vocal cord, which biopsy demonstrated to be dedifferentiated liposarcoma of the larynx. The patient went on to total laryngectomy with planned adjuvant radiation therapy. The presentation and imaging findings of laryngeal liposarcoma are nonspecific, but this neoplasm should be considered in the differential of masses in the head and neck.
Keywords: Liposarcoma, Larynx
Introduction
Liposarcoma of the larynx can be difficult to diagnose because of vague symptoms, nonspecific imaging findings, and the rare nature of the disease. It is often not on the differential diagnosis of either clinicians or radiologists. We present a case of liposarcoma that is unusual both in its histology and location, as the liposarcoma was of the dedifferentiated subtype, and the tumor was glottic in origin.
Case report
A 55-year-old man presented to ENT clinic with a 3-month history of hoarseness. The patient denied any dysphagia, odynophagia, weight loss, precipitating factors, or additional symptoms. The patient had a 40 pack-year smoking history. Flexible laryngoscopy performed in the ENT clinic demonstrated a large, firm, fibrous appearing mass on the right true vocal cord, extending into the anterior commissure and into the subglottis, causing moderate to severe airway obstruction. The patient underwent contrast-enhanced computed tomography of the neck, which demonstrated a 2.5-cm oval-enhancing mass along the true vocal cord extending along the anterior commissure (Fig. 1, Fig. 2, Fig. 3). No cartilage erosion, extralaryngeal spread, or lymphadenopathy was present. Of note, the lesion did not contain fat. Subsequently, the patient underwent direct laryngoscopy (Fig. 4) and biopsy forceps were used to take multiple biopsies of the mass and debulk the lesion to alleviate airway obstruction. Pathology demonstrated dedifferentiated liposarcoma. The patient had no metastatic disease at the time of presentation and went on to total laryngectomy. Surgical pathology demonstrated a 3.5-cm polypoid tumor arising from the submucosa with overlying mucosal ulceration. Histologically, the tumor was poorly demarcated with infiltrative growth pattern into adjacent laryngeal structures. The tumor cells displayed significant atypia and pleomorphism with numerous mitoses. Extensive sampling of the tumor showed no evidence of adipocytic differentiation; however, MDM2 immunostain showed scattered nuclear positivity leading to a diagnosis of intermediate grade dedifferentiated liposarcoma of the right true vocal cord (Fig. 5). Surgical margins were negative, and the patient was referred to radiation oncology for adjuvant radiation therapy, with plans to undergo IMRT with 6600 cGy delivered in 33 fractions.
Fig. 1.

Axial CT of the neck demonstrates the 2.5-cm oval-enhancing mass along the true vocal cords with involvement of the anterior commissure, marked by arrow. The lesion does not demonstrate evidence of extralaryngeal spread, cartilage erosion, or paraglottic invasion. CT, computed tomography.
Fig. 2.
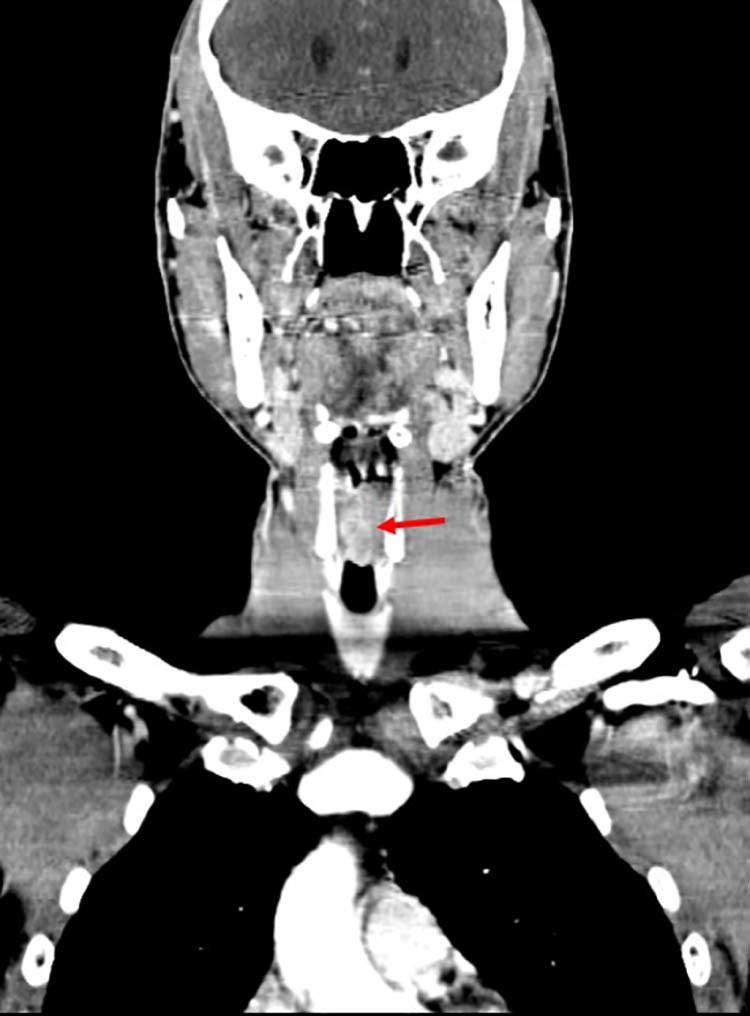
Coronal CT of the neck demonstrates the 2.5-cm oval-enhancing mass along the true vocal cords with involvement of the anterior commissure, marked by arrow. The lesion does not demonstrate evidence of extralaryngeal spread, cartilage erosion, or paraglottic invasion. CT, computed tomography.
Fig. 3.
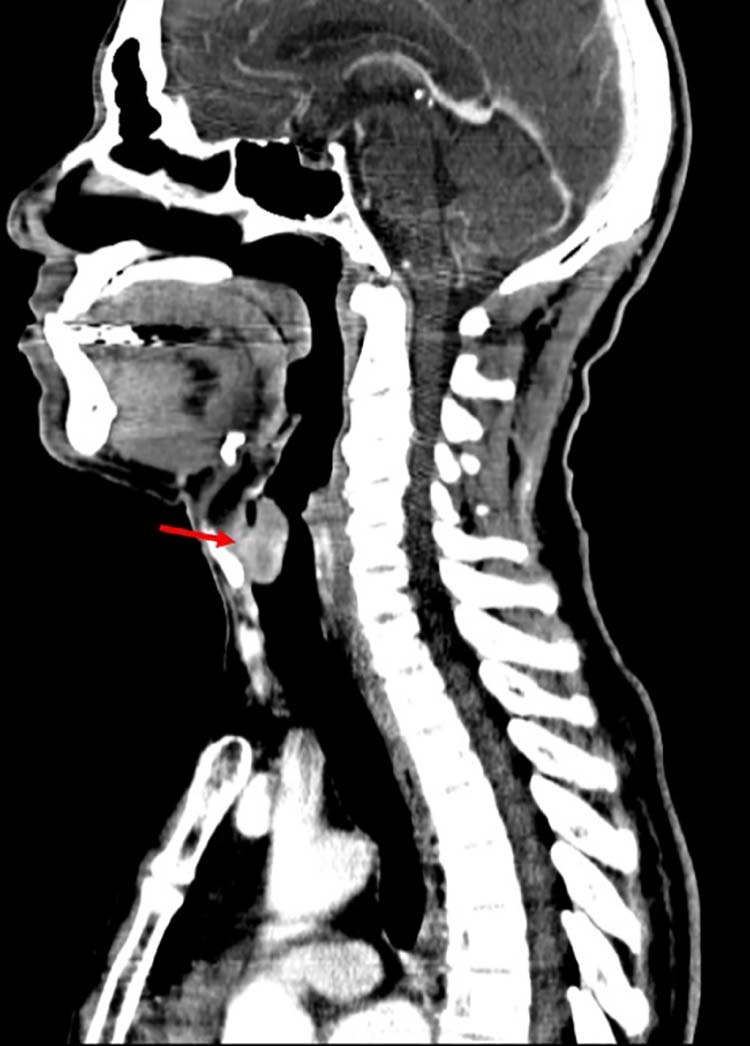
Sagittal CT of the neck demonstrates the 2.5-cm oval-enhancing mass along the true vocal cords with involvement of the anterior commissure, marked by arrow. The lesion does not demonstrate evidence of extralaryngeal spread, cartilage erosion, or paraglottic invasion. CT, computed tomography.
Fig. 4.

Image from direct laryngoscopy demonstrates a large, fibrous appearing mass arising from the right true vocal cord, causing airway obstruction.
Fig. 5.

(A) Low power magnification shows a polypoid tumor (star) with ulcerated surface (arrow). (B) The tumor originates in the submucosa which is partially ulcerated (arrow head: overlying squamous epithelium; arrow: ulcerated mucosa). (C) The tumor is composed of highly malignant cells with marked atypia and pleomorphism. Mitoses (arrow) are readily identified. Note the absence of adipocytic differentiation. (D) MDM2 immunohistochemistry is positive (at various degrees) in the nucleus of tumor cells (arrows).
Discussion
The presentation of laryngeal liposarcoma is nonspecific and includes airway obstruction, dysphagia, hoarseness, and odynophagia. It is most common in men and typically presents in those over the age of 40 [1]. There are 4 histologic subtypes of liposarcoma: well-differentiated liposarcoma, dedifferentiated liposarcoma, myxoid liposarcoma, and pleomorphic liposarcoma. Liposarcoma is typically well differentiated with low potential for metastasis, not of the dedifferentiated subtype as seen in this patient.
Liposarcoma is most common in the retroperitoneum and lower extremities, and rarely presents in the head and neck region. Approximately 5%-9% of liposarcomas are in the head and neck, and of those in the head and neck region, up to 9% are of the larynx [2]. When liposarcoma is present in the larynx, the most common location is of the supraglottic area [3]. A previous review of 37 cases of liposarcoma of the larynx identified only 4 reported cases of glottic disease [4]. Liposarcoma of the larynx has a high potential for recurrence, even when presenting as well-differentiated disease. Diagnosis is often delayed as the presentation mimics that of lipomas [1].
The mainstay of management is wide local excision. Radiation has been shown to improve local control. Chemotherapy has variable efficacy depending on the primary location of the tumor [5]. The imaging appearance of liposarcoma of the larynx is not well described. Although liposarcoma is typically described as a fat-containing lesion, this case illustrates the variability in presentation and necessity of a broad differential diagnosis for masses in this region.
Footnotes
Competing Interests: The authors have declared that no competing interests exist.
References
- 1.Cummings C.W., Flint P.W. 5th ed. Mosby/Elsevier; Philadelphia, PA: 2015. Cummings otolaryngology head & neck surgery; pp. 1601–1633. (Malignant tumors of the larynx). Chapter 106. [Google Scholar]
- 2.Nili F., Baghai F., Aghai A., Etebarian A. Well-differentiated liposarcoma of the floor of the mouth: Report of a rare case and review of the literature. J Oral Maxillofac Pathol. 2016;20(2):312–315. doi: 10.4103/0973-029X.185984. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kodiyan J., Rudman J.R., Roswo D.E., Thomas G.R. Lipoma and liposarcoma of the larynx: case reports and literature review. Am J Otolaryngol. 2015;36(4):611–615. doi: 10.1016/j.amjoto.2014.07.003. [DOI] [PubMed] [Google Scholar]
- 4.Han Y., Yang L., Liu T., Wang J., Li H., Yu G. Liposarcoma of the larynx: report of a case and review of the literature. Int J Clin Exp Pathol. 2015;8(1):1068–1072. [PMC free article] [PubMed] [Google Scholar]
- 5.Nassif N.A., Tseng W., Borges C., Chen P., Eisenberg B. Recent advances in the management of liposarcoma. F1000Res. 2016;5:2907. doi: 10.12688/f1000research.10050.1. [DOI] [PMC free article] [PubMed] [Google Scholar]