

Abstract
Background
Moyamoya disease (MMD) is characterized by progressive stenosis of intracranial arteries in the circle of Willis with unknown etiology even after the identification of a Moyamoya susceptible gene, RNF213. Recently, differences in epigenetic regulations have been investigated by a case-control study in MMD. Here, we employed a disease discordant monozygotic twin-based study design to unmask potential confounders.
Methods
Circulating genome-wide microRNA (miRNome) profiling was performed in MMD-discordant monozygotic twins, non-twin-MMD patients, and non-MMD healthy volunteers by microarray followed by qPCRvalidation, using blood samples. Differential plasma-microRNAs were further quantified in endothelial cells differentiated from iPS cell lines (iPSECs) derived from another independent non-twin cohort. Lastly, their target gene expression in the iPSECs was analyzed.
Results
Microarray detected 309 plasma-microRNAs in MMD-discordant monozygotic twins that were also detected in the non-twin cohort. Principal component analysis of the plasma-microRNA expression level demonstrated distinct 2 groups separated by MMD and healthy control in the twin- and non-twin cohorts. Of these, differential upregulations of hsa-miR-6722-3p/− 328-3p were validated in the plasma of MMD (absolute log2 expression fold change (logFC) > 0.26 for the twin cohort; absolute logFC > 0.26, p < 0.05, and q < 0.15 for the non-twin cohort). In MMD derived iPSECs, hsa-miR-6722-3p/− 328-3p showed a trend of up-regulation with a 3.0- or higher expression fold change. Bioinformatics analysis revealed that 41 target genes of miR-6722-3p/− 328-3p were significantly down-regulated in MMD derived iPSECs and were involved in STAT3, IGF-1-, and PTEN-signaling, suggesting a potential microRNA-gene expression interaction between circulating plasma and endothelial cells.
Conclusions
Our MMD-discordant monozygotic twin-based study confirmed a novel circulating microRNA signature in MMD as a potential diagnostic biomarker minimally confounded by genetic heterogeneity. The novel circulating microRNA signature can contribute for the future functional microRNA analysis to find new diagnostic and therapeutic target of MMD.
Electronic supplementary material
The online version of this article (10.1186/s12920-018-0385-3) contains supplementary material, which is available to authorized users.
Keywords: Circulating microRNA, Moyamoya disease, Discordant monozygotic twins, iPS cells, Endothelial cells
Background
Moyamoya disease (MMD) is a rare cerebrovascular disorder with unknown cause, characterized by progressive occlusion of the internal carotid arteries and their main branches in the circle of Willis along with the development of an abnormal collateral network known as “moyamoya vessels” [1]. The predominant histopathological feature of MMD is fibrocellular thickening of the intima and attenuation of the media in the affected arterial wall [2–4]. Emerging next generation studies revealed novel genetic aspects of MMD including disease susceptible polymorphisms across the genome in diverse ethnicities [5–7]. In particular, identification of RNF213 gene as a MMD-susceptible gene provided cutting edge impact on MMD research [8, 9]. Endothelial cell (EC) dysfunction has been demonstrated in vitro using iPS cell lines with an RNF213 gene polymorphism (i.e., rs112735431) [10–12], although the primary histopathological features were not reproduced in the intracranial cerebral arteries of RNF213 knock-out mice or in transgenic mice overexpressing RNF213 [11, 13–15].
Recently, several case-control studies have investigated the association between microRNA and MMD upon a non-twin cohort basis [16–18]. MicroRNAs constitute short non-coding RNAs that negatively regulate gene expression at a post-transcriptional level [19]. As they are stable in the sera/plasma and can regulate multiple genes, circulating microRNAs are expected to represent potential diagnostic and prognostic biomarkers of several diseases including stroke [19–21]. Moreover, epigenetic disease studies can particularly benefit from disease-discordant monozygotic twin study design by controlling many potential confounders such as genetic factors, age, and sex [20].
We, therefore, conducted circulating genome-wide microRNA (miRNome) profiling in cohorts of MMD-discordant monozygotic twins, non-twin MMD cases, and healthy controls to unmask potential confounders from a previously reported microRNA signature in MMD [16, 17]. We further studied endothelial microRNA expression using iPS cell lines of another independent non-twin cohort as an in vitro MMD model. Using a published endothelial transcriptome microarray dataset, which has been studied in the exact same cohort, microRNA-gene expression network was analyzed. Understanding the circulating microRNA signature from a discordant monozygotic twin-based study may be invaluable for providing novel insights toward blood biomarker discovery. Furthermore, insights from plasma and endothelial microRNA expression relationships may contribute to provide a potential therapeutic target of MMD.
Methods
A total of 27 Japanese individuals, including 13 patients with MMD and 14 healthy individuals were included. Two subjects with MMD had participated in previous linkage studies [22, 23]. MMD was diagnosed by magnetic resonance angiography (MRA) or catheter angiography in the Department of Neurosurgery at Hokkaido University Hospital or the referral hospitals between 1987 and 2011 based on the published guideline [24]. Quasi-Moyamoya disease was excluded in this study. We used angiographical stages evaluated according to the MRA stage grading system [25] at the closest timing of blood sampling for analysis. The normal control group consisted of healthy volunteers without any recorded or family history of neurological diseases, including MMD. All normal healthy controls were recruited at the Department of Neurology Hokkaido University Graduate School of Medicine, except for one unaffected MMD-discordant monozygotic twin. In the circulating miRNome microarray study, a pair of MMD-discordant monozygotic twins and a non-twin cohort (nine unrelated subjects with MMD and 10 healthy controls) were included. In the experiment using endothelial cells derived from iPS cell line (iPSECs), another independent non-twin cohort (three patients with MMD and three healthy controls) was recruited, comprising exactly same individuals participated in our previous in vitro iPSEC study [12]. Demographics and clinical features of all study participants were summarized in Table 1.
Table 1.
Demographics and clinical features of the study participants
| Age (y) | Sex | Disease type | Disease stage | Familial MMD | EC/IC bypass | Comorbidity | Brain lesion | rs112735431 (RNF213) | ||
|---|---|---|---|---|---|---|---|---|---|---|
| at sampling | at onset | |||||||||
| Circulating miRNome microarray analysis | ||||||||||
| MMD-Discordant Monozygotic Twins | ||||||||||
| Affected Twin | 12 | 3 | F | TIA | 3 | Yes | Yes | No | No | AG |
| Non-affected Twin | 12 | – | F | – | – | Yes | – | No | No | AG |
| Non-Twin cohort | ||||||||||
| MMD, n = 9 | 49.7 ± 5.4 | 37.3 ± 7.3 | 66.7% | All TIA | 3 | 56.0% | 100% | 11% | 67% | All AG |
| Control, n = 10 | 51.7 ± 3.6 | – | 70% | – | – | 0% | 0% | 0% | – | All GG |
| P-value | 0.75 | 1.0 | ||||||||
| iPSEC-microRNA and gene expression analysis | ||||||||||
| MMD, n = 3 | 41.0 ± 3.6 | 39.1 ± 4.0 | 67% | All TIA | 3 | TIA | 67% | 33% | 0% | All AG |
| Control, n = 3 | 50.0 ± 2.0 | – | 0% | – | – | 0% | 0% | 0% | – | All GG |
Disease stage indicates MRA grade of the advanced hemisphere if a difference between hemispheres exists. Comorbidity observed in study participants was hypertension. Age (years) was expressed as the mean ± SEM and Disease stage was expressed as median in the non-twin cohort. F female, EC/IC bypass: extracranial-intracranial bypass, TIA transient ischemic attack. A: minor and G: major allele for rs112735431 of the RNF213 gene
Detailed methods for blood sample and iPSEC collection/purification, RNA isolation or extraction from plasma or iPSECs, microRNA expression microarray and quantitative real-time polymerase chain reaction (qPCR) analysis, bioinformatics analysis for microRNA-gene expression network and molecular pathway analysis, as well as statistics were provided in supplementary materials and methods (see Additional file 1: Supplementary materials and methods). In brief, differential plasma-microRNA expression microarray analysis was performed in MMD-discordant twin and in non-twin cohorts, respectively. In MMD-discordant monozygotic twins, a set of differential plasma-microRNAs was identified that exhibited a greater than 0.26-absolute expression log fold change between the affected and non-affected monozygotic twins. In the non-twin cohort, a set of differential plasma-microRNAs was identified that exhibited a greater than 0.26-absolute expression log fold change and a less than 0.05 p-value computed by unpaired t-test corrected by Welch’s method between MMD and controls followed by multiple testing correction using Storey’s Bootstrapping false discovery rate (FDR) method (q value < 0.15). Raw data of the microarray experiments can be accessed through the National Center for Biotechnology Information Gene Expression Omnibus (NCBI GEO accession number GSE100488).
Results
Circulating miRNome profiling demonstrated distinct 2 groups separated by MMD and healthy control
We recruited a pair of MMD-discordant monozygotic twins with familial occurrence of MMD as shown in Fig. 1a to conduct disease-discordant monozygotic twin-based circulating miRNome profiling. Although familial occurrence of MMD comprises approximately 15% of reported cases in Japan, MMD-discordant monozygotic twins are extremely rare [3]. MRAs (Fig. 1b-c) demonstrated bilateral occlusion of ICAs with developed moyamoya vessels in the affected twin (II-3 in the pedigree tree), whereas ICAs of the non-affected twin (II-2) were intact. Genome-wide microRNA expression microarray (SurePrint® G3 Human miRNA microarray (Release 21.0, Agilent)) detected 309 plasma-microRNAs (12.1% of 2549 detectable microRNAs) in this pair of MMD-discordant monozygotic twins. Of these, 151 microRNAs were up-regulated and 36 were down-regulated in the affected compared to the non-affected twin (imposed threshold for expression log2-fold change (logFC); 0.26) (Fig. 1d). The detection rate of plasma-microRNA was higher than that reported in the manufacturer’s application note, and comparable with that in a previous publication studying circulating microRNA in MMD using the same microarray platform [16]. The top five up-regulated plasma-microRNAs in the affected twin were hsa-miR-150-5p (logFC: 2.2), hsa-let-7a-5p (logFC: 2.1), hsa-miR-122-5p (logFC: 2.0), hsa-miR-4419b (logFC: 1.7), and hsa-miR-126-3p (logFC: 1.6), whereas the top five down-regulated plasma-microRNAs were hsa-miR-144-3p (logFC: − 2.1), hsa-miR-8073 (logFC: − 1.5), hsa-miR-6741-5p (logFC: − 1.4), hsa-miR-1237-3p (logFC: − 1.1), and hsa-miR-33b-3p (logFC: − 1.0).
Fig. 1.

Family pedigree, angiographical features, and plasma-microRNA expression in the Moyamoya disease-discordant monozygotic twins. a Family pedigree tree demonstrating the family members of the MMD-discordant monozygotic twins. Individuals I-1 and II-3 had never participated in previous linkage studies. The affected twin (II-3) experienced an epileptic seizure and transient paraparesis when crying at 3 years of age and underwent EC/IC bypass. She did not develop any recurrent stroke, including TIA after bypass surgeries. The non-affected twin (II-2) underwent MRI and MR angiography (MRA) scans when she was 3 and 12 years old without any evidence of cerebrovascular diseases, including MMD. Individual I-1 was diagnosed as MMD when he was 9 years old and underwent bypass surgeries in another hospital. Individuals I-2 and II-1 also provided blood samples and had MRI/MRA scans in our hospital. Their MRI/A showed no evidence of MMD (data not shown). b-c MRA demonstrates cerebral arteries of the affected twin (II-3) when she was 12 years old (b), showing severe stenosis of ICAs and proximal MCAs on both hemispheres and complete disappearance of ACA on the right hemisphere, indicating MRA grade 3 on both hemispheres. Distal portions of bilateral MCAs are depicted by blood supplies from EC/IC bypasses via superficial temporal arteries, whereas MRA of the non-affected twin (II-2) when she was 12 years old demonstrates no steno/occlusive change in the cerebral arteries (c). “Rt” indicates the right hemisphere. d Scatter plots demonstrate the plasma-microRNA expression for 309 plasma-microRNAs detected in the MMD-discordant monozygotic twins by microarray. Horizontal and vertical axes indicate normalized log2-microRNA expression signals for each microRNA in the affected and non-affected twins, respectively. Red dots indicate microRNAs exhibiting a 0.26- or greater log2-fold change and blue dots indicate microRNAs exhibiting a − 0.26 or less log2-fold change in the affected twin relative to the non-affected twin. Black dots indicate microRNAs exhibiting log2-fold change in between − 0.26 and 0.26
Using the same microarray platform, we studied circulating miRNome profiles in nine Japanese patients with MMD and 10 unrelated healthy individuals as a non-twin cohort, identifying 546 plasma-microRNAs with detection call (21.4% of 2549 detectable microRNAs). Because microRNAs detected in the twins were predominantly detected in the non-twin cohort (Fig. 2a), we performed a principal component analysis for the 309 plasma-microRNA level in the discordant twins and the non-twin cohort together (Fig. 2b) and identified distinct 2 clusters. One cluster included the affected monozygotic twin and patients with MMD from the non-twin cohort. The other included non-affected monozygotic twins and healthy controls. Component 2 (Y-axis) was the main component separating MMD and non-MMD control. Top 30 microRNAs with higher absolute PCA scores for each microRNA for the component 2 were listed, showing top 30 plasma microRNAs contributing group segregation between MMD and control (Please see Additional file 2: Table S1). This result suggested that the circulating microRNA expression pattern was associated with MMD even in the MMD-discordant monozygotic twins. Because pediatric monozygotic twins share genetic variants predominantly [20] and many life style environments, differential microRNAs may contribute to the discordance of MMD in the monozygotic twins with fewer confounders relative to a general non-twin based case-control study.
Fig. 2.
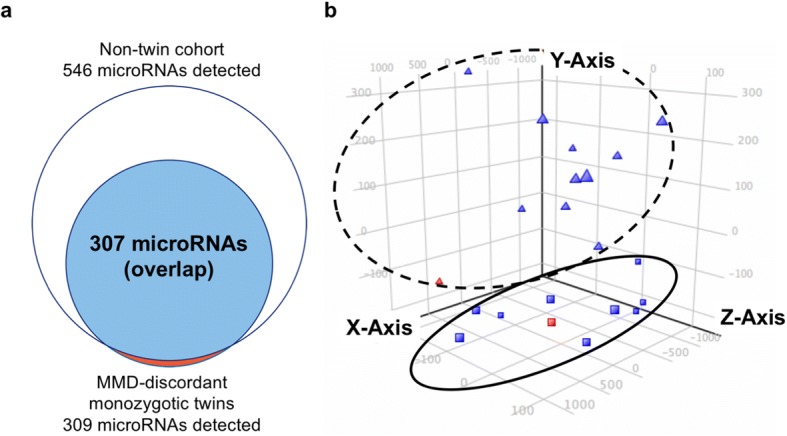
Circulating microRNA expression profiling in the MMD-discordant monozygotic twins and non-twin cohorts. a Venn diagram depicts a white circle as a collection of 546 plasma-microRNAs detected in the non-twin cohort (9 MMDs and 10 controls) and a red circle as a collection of 309 plasma-microRNAs detected in the discordant twins. The overlapping closed blue circle represents a set of 307 plasma-microRNAs, indicating predominant plasma-microRNAs detected in the discordant twins (99.4%) were also detected in the non-twin cohort. b Three-dimensional PCA plots demonstrate 2 distinct clusters in the circulating microRNA profile separated by MMD and controls. Each dot represents the expression profile of the 309 plasma-microRNAs detected by microarray in the discordant twins without any differential expression analysis. The affected MMD-discordant monozygotic twin (red square) and MMD patients in the non-twin cohort (blue squares) can be grouped (circled in solid line), whereas the non-affected twin (red triangle) and healthy control individuals in the non-twin cohort (blue triangles) can also be grouped (circled in dotted line). Component 2 (Y-axis) was the main component separating MMD and non-MMD control, including MMD-discordant monozygotic twins
Differential microRNA expression analysis highlighted 17 plasma-microRNAs in MMD
Based on the distinct circulating microRNA profile associated with MMD, we next performed differential microRNA expression analysis between MMD and healthy controls in the MMD-discordant monozygotic twin and non-twin cohorts using microarray dataset. In the MMD-discordant monozygotic twins, we found 187 differential plasma-microRNAs (151 up-regulated and 36 down-regulated in the affected twin; imposed threshold: absolute logFC > 0.26; Fig. 3a), whereas in the non-twin cohort, we found 49 differential plasma-microRNAs (30 up-regulated and 19 down-regulated in MMD; imposed threshold: absolute logFC > 0.26, p < 0.05, q < 0.15; Fig. 3b). From these independent sets of differential plasma-microRNAs, we identified 17 plasma-microRNAs that overlapped between the twin and non-twin cohorts. We confirmed that these plasma-microRNAs were consistently up- (12 microRNAs) or down-regulated (five microRNAs) in the affected monozygotic twin and patients with MMD in the non-twin cohort (Table 2). Of note, 12 microRNAs, including hsa-miR-6722-3p, hsa-miR-328, and hsa-miR-150 were found in the top 30 microRNA list correlated with MMD based on the principal component analysis (Please see Additional file 2: Table S1).
Fig. 3.
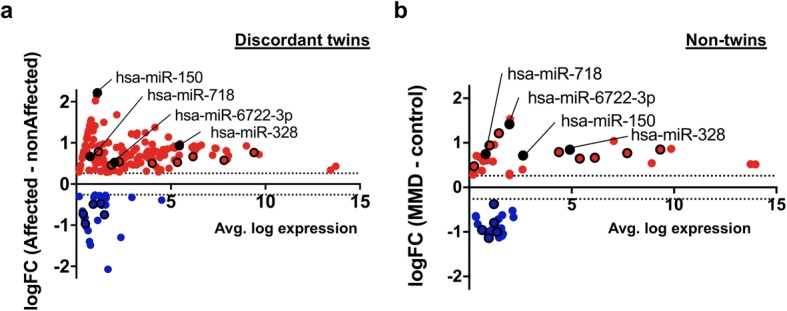
Differential plasma microRNA expression profile in the twin and non-twin cohorts. a-b M-A plot (M = log2 fold change, A = averaged log2 expression) demonstrated the 187-differential plasma-microRNAs (151 up-regulated and 36 down-regulated) in the MMD-discordant monozygotic twins (threshold: absolute log-FC > 0.26; (a)), and 49-differential plasma-microRNAs (30 up-regulated and 19 down-regulated) in the non-twin cohort (threshold: absolute log-FC > 0.26 and p < 0.05; (b)). Seventeen plasma-microRNAs were further highlighted with black circle that showed significant differential expression between MMD and non-MMD both in the twin and non-twin cohort. Of these, 4 microRNAs shown in the plot were validated by real-time qPCR
Table 2.
Differential plasma-microRNAs from discordant monozygotic twin-based study
| MicroRNA ID | Discordant twins | Non-twin cohort | ||
|---|---|---|---|---|
| Log2 fold change | Log2 fold change | p value | q value | |
| hsa-miR-150 | 2.218 | 0.714 | 0.28 | 0.123 |
| hsa-miR-328 | 0.931 | 0.845 | 0.028 | 0.123 |
| hsa-miR-3610 | 0.786 | 0.475 | 0.019 | 0.105 |
| hsa-miR-6089 | 0.765 | 0.850 | 0.005 | 0.045 |
| hsa-miR-718 | 0.669 | 0.749 | 0.030 | 0.128 |
| hsa-miR-3665 | 0.665 | 0.665 | 0.023 | 0.120 |
| hsa-miR-6800-5p | 0.576 | 0.769 | 0.004 | 0.042 |
| hsa-miR-762 | 0.540 | 1.215 | 0.009 | 0.060 |
| hsa-miR-6850-5p | 0.528 | 0.646 | 0.031 | 0.128 |
| hsa-miR-6722-3p | 0.527 | 1.415 | 0.001 | 0.038 |
| hsa-miR-940 | 0.503 | 0.791 | 0.002 | 0.038 |
| hsa-miR-4532 | 0.464 | 0.940 | 0.024 | 0.121 |
| hsa-miR-7845-5p | −0.468 | −1.004 | 0.002 | 0.038 |
| hsa-miR-623 | −0.491 | −0.797 | 0.027 | 0.123 |
| hsa-miR-595 | −0.726 | −0.958 | 0.005 | 0.045 |
| hsa-miR-6737-3p | −0.746 | −0.373 | 0.000 | 0.019 |
| hsa-miR-4481 | −0.965 | −1.136 | 0.002 | 0.038 |
Table listed 17 differential microRNAs that were consistently up- or down-regulated in the affected monozygotic twin and patients with MMD in the non-twin cohort. Log2 fold change indicates relative plasma-microRNA expression level in MMD to control
A total of 8586 messenger RNAs (mRNAs) were predicted as “target genes” of these 17 differential microRNAs by the IPA® tool and miRmap web interface [26]. We further filtered these 8586 genes and obtained 1069 target gene names according to the IPA knowledge-based disease or function terms, including “Cardiovascular diseases”, “Neurological diseases”, and “Vascular physiology” as relevant genes associated with MMD. Table S2 shows the number of target genes for each of the 17 differential microRNAs in detail (see Additional file 3: Table S2).
These 1069-target genes included genes known to be associated with MMD [3, 4, 27], such as RNF213, fibroblast growth factors (FGF2, 7, 14, and 17), hepatocyte growth factor (HGF), platelet derived growth factor B (PDGFB), tumor transforming growth factor beta receptors (TGFBR1 and 2), tumor necrosis factor superfamily member genes (TNFSF4 and 12), and vascular endothelial growth factor A (VEGF A). Notably, hsa-miR-6722-3p can regulate multiple MMD-related genes including RNF213, FGF2 (also known as basic FGF), insulin like growth factor 1 receptor (IGF1R), as well as kinase insert domain receptor (KDR, also known as VEGFR2). Whereas, hsa-328-3p can regulate corticotropin releasing hormone (CRH), protein kinase, cGMP-dependent type I (PRKG1), progesterone receptor (PGR), and others, which are known to be associated with vascular endothelial cell or smooth muscle cell function.
qPCR verification of hsa-miR-328-3p and − 6722-3p in the plasma and iPSECs
To validate the results from microarray analysis, we performed real-time qPCR for the plasma-microRNAs of interest using a modified ΔΔCT method [28]. Thus, from the 17 differential microRNAs highlighted by the plasma-microRNA microarray analysis (Table 2), we quantified the relative expression level of hsa-miR-150-5p, − 328-3p, − 6722-3p, and − 718 using plasma samples of the non-twin cohort because these microRNAs were more up-regulated in the affected MMD-discordant twins, more significantly up-regulated in patients with MMD in the non-twin cohort, or have target genes relevantly related to MMD (see the rationale for this selection in Additional file 1: Supplementary materials and methods). We confirmed that hsa-miR-150-5p, − 328-3p, and − 6722-3p were significantly up-regulated in the plasma of MMD (p < 0.05) (Fig. 4a), which was consistent with the microarray result. Conversely, hsa-miR-718 was not amplified by real-time qPCR presumably due to low abundance in the plasma samples analyzed in this study, which was suggested by lower expression signal in the microarray result (Fig. 3b). Although Fig. 4a indicated that there were 2 types of the miR-328-3p and 150-5p plasma expression pattern (elevated and non-elevated), these 4 elevated samples did not match each other. There was no common trend in these elevated samples.
Fig. 4.
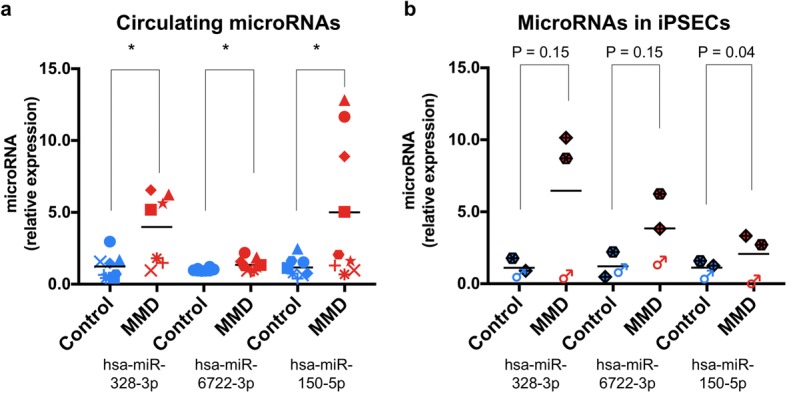
Quantification of microRNA expression in the plasma and iPSECs. a Column scatter graphs demonstrating relative plasma-microRNA expression levels for hsa-miR-328-3p (left), − 6722-3p (middle), and 150-5p (right), quantified by real-time PCR in the non-twin cohort (MMD n = 9; red dots, control n = 8; blue dots). There was a significant difference in each plasma-microRNA expression level between MMD and control groups (hsa-miR-328-3p, 4.0 ± 0.9 and 1.2 ± 0.3, p = 0.011; hsa-miR-6722-3p, 1.4 ± 0.1 and 1.0 ± 0.03, p = 0.049, hsa-miR-150-5p, 5.0 ± 1.6 and 1.2 ± 0.2, p = 0.043, respectively. *p < 0.05). Data represent the mean ± SEM. b Column scatter graphs demonstrating relative iPSEC-microRNA expression levels for hsa-miR-328-3p (left), − 6722-3p (middle), and 150-5p (right), quantified by real-time PCR in another non-twin cohort (MMD n = 3; red dots, control n = 3; blue dots, please refer to Table 1). There was a trend of difference in the respective hsa-miR-328-3p and − 6722-3p expression levels in iPSECs between MMD and control groups (hsa-miR-328-3p, 6.5 ± 3.0 and 1.1 ± 0.3, p = 0.15; hsa-miR-6722-3p, 3.8 ± 1.4 and 1.2 ± 0.5, p = 0.15). Conversely, no trend of difference was observed in hsa-miR-150-5p between MMD and control groups (2.1 ± 1.0 and 1.1 ± 0.3, p = 0.40, respectively). Data represents as mean ± SEM. Each individual data was plotted by same color and same shape code
To investigate the expression levels of these microRNAs in the ECs of MMD, we employed an in vitro MMD-iPSEC model, comprising differentiated and cultured ECs from iPS cell lines derived from another independent non-twin cohort (Table 1). The purity of iPSECs were confirmed by FACS plot (Please see Additional file 4: Figure S1). We found a trend of up-regulation of hsa-miR-328-3p and − 6722-3p in the iPSECs derived from MMD with a 3.0- or higher expression fold change, although it did not reach statistical significance by t-test due to small sample size. Whereas, there was no trend of difference in hsa-miR-150-5p expression level in iPSECs between MMD and the control (p = 0.40) (Fig. 4b).
MicroRNA-gene expression network analysis suggests a regulatory role of hsa-miR-328-3p/− 6722-3p involving biological pathways in endothelial cells of MMD
Based on the results from qPCR validations, hsa-miR-328-3p and − 6722-3p were identified as differential microRNAs of MMD, which may be associated with the phenotypic discordance in the MMD-discordant monozygotic twins. As these microRNAs showed a significant upregulation in the plasma in MMD and a trend of differential up-regulation in the MMD-iPSECs, we interrogated the regulatory role of hsa-miR-328-3p/− 6722-3p in their target gene expression. Based on the aforementioned target gene prediction, 327 target genes of hsa-miR-328-3p/− 6722-3p were identified (287 for hsa-miR-6722-3p and 48 for hsa-miR-328-3p) (please see Additional file 3: Table S2). We analyzed an experimentally validated microarray dataset from our previous publication that investigated gene expression profile in the iPSECs derived from the same MMD and healthy control individuals (n = 3, respectively, Table 1) as well as differentiated/cultured under identical conditions [12]. Of these 327 target genes, 41 genes (12.5%) were significantly down-regulated (logFC range − 2.0 to − 0.6, p < 0.05, q < 0.15), and 14 genes (4.3%) were significantly up-regulated (log-FC: range 0.6 to 2.6, p < 0.05, q < 0.15) in MMD-iPSECs. The gene list was presented in the Additional file 5: Table S3. This result suggested that significant down-regulation of these 41 genes might be associated with epigenetic regulation of the up-regulated hsa-miR-328-3p and − 6722-3p in MMD-iPSECs.
We annotated these 41 down-regulated genes in the MMD-iPSECs using IPA tool. Thus, the least five genes down-regulated in the MMD-iPSECs were ADAM metallopeptidase domain 12 (ADAM12, log-FC: − 2.0), cyclin dependent kinase 6 (CDK6, log-FC: − 2.0), additional sex combs like 3, transcriptional regulator (ASXL3, log-FC: − 1.9), pappalysin 1 (PAPPA, also known as insulin-like growth factor-dependent IGF binding protein-4 protease, log-FC: − 1.8), and RNF213 (log-FC: − 1.6). IPA canonical pathway analysis for these 41 down-regulated genes demonstrated the top three canonical pathways, namely the signal transducer and activator of transcription 3 (STAT3) pathway, insulin-like growth factor 1 (IGF-1) signaling, and phosphatase and tensin homolog (PTEN) signaling, which are known angiogenesis and vascular homeostasis-related pathways (Fig. 5). In addition, these genes were also involved in autophagy, extracellular signal regulated kinase 5 (ERK5) signaling, phagosome maturation, and the inflammasome pathway, which comprise inflammation or infection-related signaling pathways.
Fig. 5.
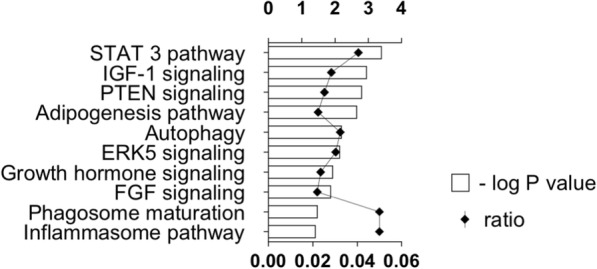
Top 10 canonical pathways involved by the 41 significantly down-regulated genes in MMD-iPSECs. Graph showing the top 10 canonical pathways from IPA® pathway analysis involved by the 41 significantly down-regulated genes in MMD-iPSECs that were predicted as target genes of significantly up-regulated hsa-miR-328-3p and − 6722-3p in MMD-iPSECs. The ratio expresses the number of differentially down-regulated genes in our dataset over the total number of genes in each canonical pathway based on the IPA knowledge database (represented in the lower X axis). P values for the significance of each pathway were computed based on the number of genes involved in the pathway by using Fisher’s exact test, and negatively log10 transformed (represented in the upper X axis)
Discussion
We conducted circulating genome-wide microRNA profiling in MMD using a disease-discordant monozygotic twins-based design to discover a less confounded microRNA signature. Result was validated in an independent non-twin MMD cohort. Thus, our strategy could reduce the effect of many possible confounders (i.e., genetic heterogeneity) affecting the findings from a general non-twin-based case-control study. We observed that plasma-microRNA expression profiling could clearly separate MMD and healthy control in the MMD-discordant monozygotic twin- and the non-twin cohort. From differential microRNA expression analysis between MMD and controls, a novel 17 differential plasma-microRNAs signature was identified, since 16 of these plasma-microRNAs have not been reported in the previous exploratory study for circulating microRNA signature in MMD using non-twin based study design [16, 17]. We have successfully validated differential upregulation of hsa-miR-6722-3p/− 328-3p/− 150-5p in the plasma of MMD patients. We also found a trend of upregulation of hsa-miR-6722-3p/− 328-3p in MMD-iPSECs. Furthermore, some of their predicted target genes were significantly downregulated in MMD-iPSECs, suggesting a role of epigenetic regulation of circulating microRNA in endothelial cells in MMD. This is the first observation of possible microRNA-gene expression network between the plasma and endothelial cells in MMD.
Circulating microRNA signature in MMD in comparison with that from a previous non-twin-based case-control study
Dai et al. first reported 94 differential circulating microRNAs in Chinese Han MMD compared to ethnicity-matched normal controls [16] using the same microarray platform. Zhao et al. next specifically analyzed serum microRNA let-7 family expression in the sera of MMD as a regulator of the RNF213 gene [17]. Because both studies employed a general non-twin-based study design and found circulating microRNA signatures as candidates for blood biomarkers in MMD, we considered that our MMD-discordant monozygotic twin-based design could provide additional insights to their findings. In particular, the MMD-discordant monozygotic twins that participated in the present study shared age, sex, ethnicity, and an RNF213 founder mutation polymorphism (rs112735431). Moreover, the affected twin was clinically stable without recurrent transient ischemic attack (TIA), recent surgery (approximately 9 years prior to blood sampling), or ischemic parenchymal lesion. Therefore, the distinct circulating microRNA profile detected in the discordant twins could likely explain the phenotypic discordance between MMD and non-MMD with minimal confounders. Notably, our group and Dai et al. both demonstrated that hsa-miR-595 constituted a differentially down-regulated plasma-microRNA in MMD [16]. Future study to analyze the functional role of hsa-miR-595 in MMD with different subsets of Asian ethnicity may provide important insights to understand the epigenetic aspects of MMD. However, we also identified numerous discrepancies in the results of circulating microRNA signature in MMD between the two publications. Several possible reasons for this discrepancy exist in addition to the difference in study design. First, the plasma sample processing for the array experiment fundamentally differed between studies. Dai et al. pooled plasma samples from 10 individuals with MMD and controls and undertook two microarray experiments for the two plasma pools, whereas we performed microarray experiments using 21 individual (non-pooled) samples. This difference might affect the cluster analysis used to detect the difference of microRNA profile between MMD and control. Second, the imposed threshold to determine differential microRNA in MMD is different. Third, the subgroup of ethnicity in study participants was also different (Japanese or Chinese-Han). As some differences have been observed in the genetic and epidemiological features of MMD in Chinese Han and Japanese or Korean patients [29], this may result in a difference in the circulating microRNA signature. Future work expanding the study population toward non-Asian MMD would also be invaluable to address the inter-ethnic difference/variability of clinical MMD phenotype [30].
Plasma and iPSEC microRNA expression and gene regulation in MMD
The differential up-regulation of hsa-mir-6722-3p and − 328-3p in the plasma of MMD was validated in this study. As well, there was a trend of elevated expression of those microRNAs in the iPSECs (3.0- or higher fold change in MMD compared to healthy control), suggesting possible association in the microRNA expression between circulating plasma and endothelial cells in MMD. Although the functional role of circulating microRNAs is often unclear, they are considered to be secreted actively from cells and involved in inter-cellular communications [31]. From the target gene analysis, a set of 41 genes was confirmed as targets of the up-regulated hsa-mir-6722-3p and − 328-3p in MMD-iPSECs and these genes were further experimentally demonstrated to exhibit significant down-regulation in MMD-iPSECs from the same host with exactly the same differentiation/cultural conditions from our previous publication [12]. The molecular types of the 41 gene products include enzyme (i.e., RNF213), growth factor (i.e., FGF), ion channel, kinase, peptidase, phosphatase, transcription regulator (i.e., STAT3), transmembrane receptor (i.e., IGF1R), and transporter (see Additional file 5: Table S3). IPA canonical pathway analysis revealed that these 41 down-regulated genes were involved in angiogenesis, vascular homeostasis-related signaling/pathways (STAT-3 pathway, IGF-1 signaling, and PTEN signaling), or inflammatory-related biological pathways (ERK signaling, inflammasome pathway). These facts suggest a possible plasma microRNA-endothelial gene expression network as an epigenetic regulation of endothelial biological function of MMD. For example, endothelial STAT3 plays a key role in angiogenesis and extracellular matrix remodeling [32]. IGF-1 has been shown to protect vascular function by promoting nitric oxide production from the endothelium and vascular smooth muscle cells [33]. PTEN plays critical roles for vascular homeostasis by regulating signals via multiple vascular growth factors and responses to shear stress via integrins [34, 35]. Taken together, these 41 down-regulated genes in MMD-iPSECs may play a role in endothelial biological functions via the microRNA-gene expression network in MMD. In addition, these 41 genes were also suggested to be involved in other inflammatory-related pathways. A recent study reported that pro-inflammatory cytokines activated the transcription of RNF213, the product of which plays a role in ECs for proper gene expression in response to inflammatory signals from environments [36]. Our data thus provide additional insights into the potential network of RNF213 gene expression regulation via up-regulated hsa-miR-6722-3p/− 328-3p in MMD.
There are several limitations in this study. First, the sample size was small and limited to the Japanese population. Second, this cross-sectional study sampled plasma at a single time point after development of MMD. Third, the disease type of MMD was limited to TIA-type MMD. Fourth, the differentially expressed plasma-microRNAs in MMD that have not been validated by qPCR should be quantified to verify the microarray result, since we have set less stringent cutoff calling to determine differential plasma-microRNAs in the microarray experiment. Finally, functional validation of the differential plasma-microRNAs was lacking not only in the iPSECs but in other cell types, including vascular smooth muscle cells and circulating immune cells (i.e., monocytes, T lymphocytes, and vascular progenitor cells). Addressing these limitations would be invaluable to consolidate the circulating microRNA signature as a blood biomarker in MMD and potentially uncover disease etiology. Although there are many challenges in the clinical trial designs for rare diseases [37], we think it is necessary to conduct a validation study of the present study with the adequate sample size calculation in an independent cohort.
Conclusions
This study demonstrated a distinct circulating microRNA expression profile in MMD through a unique MMD-discordant monozygotic twin-based study design. A plasma-microRNA dataset presented in this study can provide a seed to discover blood biomarker for MMD with minimal possible confounders. Furthermore, to our knowledge, this is the first study showing that the microRNA-gene expression network may play a role in epigenetic regulation of endothelial function via angiogenesis, vascular homeostasis, and inflammatory-related pathways as a potential therapeutic target for MMD.
Additional files
Supplementary Materials and Methods. Details supporting the main methods in the manuscript body are provided necessary to comprehend the results. (DOCX 35 kb)
Table S1. A list of microRNAs with respective top 15 and least 15 PCA scores. A list of microRNAs with respective top 15 and least 15 PCA scores (correlation value) for each microRNA for the component 2 (Y-axis) were provided, which separated MMD and control, based on the principal component analysis for the 309 plasma-microRNAs (Please see Fig. 2b). (DOCX 14 kb)
Table S2. Number of filtered target genes and target gene symbols for each of 17 differential circulating microRNAs in MMD, predicted by microRNA Target Filter implemented in IPA® (QIAGEN) and the miRmap web interface. The target genes were filtered based on their biological function analyzed using “Bioprofiler” implemented in IPA® (QIAGEN). As there is some overlap across microRNAs with respect to their target genes, so the total number of target genes at the bottom of the list is not a simple summation of each number of target genes. (DOCX 17 kb)
Figure S1. FACS plot to confirm the purity of iPSECs. The purity of the iPSECs after 5–6 times passages was confirmed as high as 91–97% in all clones using anti-CD31 antibody with the FACS. (TIF 1011 kb)
Table S3. The 41 target genes of hsa-miR-6722-3p/328-3p that were significantly down-regulated in MMD-iPSECs. Expression log2 fold change (log2 FC), p-value, and q-value were obtained from our previous publication (Hamauchi et al. 2016 [12]). Molecule type for each gene was obtained from the IPA tool. (DOCX 19 kb)
Acknowledgements
The authors are grateful to patients and their families for their participation in this study. We express appreciation to all the doctors and secretaries for their patient recruitment, treatment, technical, and/or clerical assistance. We also express appreciation to Dr. Michelle Y Cheng, Ph.D. (Department of Neurosurgery, Stanford University School of Medicine) for the technical support for English writing and critical comment to the manuscript. We are also thankful to Dr. Izumi Yanatori, Ph.D. for the critical comments regarding the manuscript (Department of Biochemistry, Stanford University School of Medicine). We also would like to thank Editage (www.editage.jp) for English language editing service.
Funding
This work was supported in part by a grant from the Japanese Ministry of Health, Labor and Welfare for the project of the Research Committee on Spontaneous Occlusion of the Circle of Willis (Moyamoya disease), the Mihara award (2012) from Charitable Trust Mihara Cerebrovascular Disorder Research Promotion Fund (to K.H), and a research grant (2014) from SENSHIN Medical Research Foundation (to K.H).
Availability of data and materials
The data used and/or analyzed during the current study are available from the corresponding author on reasonable request. Raw data of the microarray experiments can be accessed through the National Center for Biotechnology Information Gene Expression Omnibus (NCBI GEO accession number GSE100488).
Abbreviations
- CRH
corticotropin releasing hormone
- FGF
fibroblast growth factor
- HGF
hepatocyte growth factor
- IGF1R
insulin like growth factor 1 receptor
- iPSECs
endothelial cells differentiated from iPS cell line
- KDR
kinase insert domain receptor
- logFC
log2-fold change
- miRNome
Circulating genome-wide microRNA
- MMD
Moyamoya diease
- MRA
magnetic resonance angiography
- mRNA
messenger RNA
- PDGFB
platelet derived growth factor beta
- qPCR
quantitative polymerase chain reaction
- TGFBR
tumor transforming growth factor beta receptor
- TNFSF
tumor necrosis factor superfamily member genes
- VEGFA
vascular endothelial growth factor A
- PRKG1
protein kinase, cGMP-dependent type I
- PGR
progesterone receptor
- ADAM12
ADAM metallopeptidase domain 12
- CDK6
cyclin dependent kinase 6
- ASXL3
additional sex combs like 3 transcriptional regulator
- PAPPA
pappalysin 1
- STAT3
signal transducer and activator of transcription 3
- IGF-1
insulin-like growth factor 1
- PTEN
phosphatase and tensin homolog
- ERK5
extracellular signal regulated kinase 5
- TIA
transient ischemic attack
Authors’ contributions
HU performed experiments, analyzed data including completion of the statistical analysis, discussed results, drafted the manuscript and revised the original manuscript. MI designed research, acquired clinical information, assisted in experiments, analyzed data including completion of the statistical analysis, discussed results, listed affiliations, drafted the manuscript and revised the original manuscript. KK treated patients, acquired clinical information, and discussed results. YH assisted in experiments and discussed results. SH assisted in experiments and discussed results. ST assisted in linkable anonymizing and discussed results. HS supervised research, recruited normal healthy control volunteers, and discussed results. KH designed and supervised research, treated patients, acquired clinical information, and discussed results. All authors have read and approved this manuscript.
Ethics approval and consent to participate
The present study was approved by the Hokkaido University Graduate School of Medicine medical ethics committee on human experimentation, including genetic analysis (14–053). Written informed consent was obtained from all participants (or guardians) to participate in this study.
Consent for publication
Written informed consent was obtained from all participants (or guardians) whose individual data were presented for publication in this study in any form.
Competing interests
HU, YH, ST, HS: Nothing to report relating to this study. MI received research fellowship from SENSHIN Medical Research Foundation fellowship for research abroad (2015). SH received a grant funded by Grant-in-Aid for Scientific Research (Grant Number 17 K1662007). KK received a grant funded by Grant-in-Aid for Scientific Research (Grant Number JP15K1028605) and research support from Nihon Medi-Physics Co., Ltd. KH serves on the executive editorial board of Neurologia Medico-Chirurgica and the editorial board of the Journal of Stroke & Cerebrovascular Diseases.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Haruto Uchino, Email: uchinoh@stanford.edu.
Masaki Ito, Phone: +81-11-706-5987, Email: masakiitou-nsu@umin.ac.jp.
Ken Kazumata, Email: kazumata@med.hokudai.ac.jp.
Yuka Hama, Email: hama@pop.med.hokudai.ac.jp.
Shuji Hamauchi, Email: hamashuji@yahoo.co.jp.
Shunsuke Terasaka, Email: terasaka@kashiwaba-nougeka.or.jp.
Hidenao Sasaki, Email: h-isasak@med.hokudai.ac.jp.
Kiyohiro Houkin, Email: houkin@med.hokudai.ac.jp.
References
- 1.Suzuki J, Takaku A. Cerebrovascular “moyamoya” disease. Disease showing abnormal net-like vessels in base of brain. Arch Neurol. 1969;20:288–299. doi: 10.1001/archneur.1969.00480090076012. [DOI] [PubMed] [Google Scholar]
- 2.Masuda J, Ogata J, Yutani C. Smooth muscle cell proliferation and localization of macrophages and T cells in the occlusive intracranial major arteries in moyamoya disease. Stroke. 1993;24:1960–1967. doi: 10.1161/01.STR.24.12.1960. [DOI] [PubMed] [Google Scholar]
- 3.Kuroda S, Houkin K. Moyamoya disease: current concepts and future perspectives. Lancet Neurol. 2008;7:1056–1066. doi: 10.1016/S1474-4422(08)70240-0. [DOI] [PubMed] [Google Scholar]
- 4.Houkin K, Ito M, Sugiyama T, Shichinohe H, Nakayama N, Kazumata K, et al. Review of past research and current concepts on the etiology of moyamoya disease. Neurol Med Chir (Tokyo) 2012;52:267–277. doi: 10.2176/nmc.52.267. [DOI] [PubMed] [Google Scholar]
- 5.Shoemaker LD, Clark MJ, Patwardhan A, Chandratillake G, Garcia S, Chen R, et al. Disease Variant Landscape of a Large Multiethnic Population of Moyamoya Patients by Exome Sequencing. G3 Genes|Genomes|Genetics. 2016;6:41–49. doi: 10.1534/g3.115.020321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Mukawa M, Nariai T, Onda H, Yoneyama T, Aihara Y, Hirota K, et al. Exome sequencing identified CCER2 as a novel candidate gene for Moyamoya disease. J Stroke Cerebrovasc Dis. 2017;26:150–161. doi: 10.1016/j.jstrokecerebrovasdis.2016.09.003. [DOI] [PubMed] [Google Scholar]
- 7.Cecchi AC, Guo D, Ren Z, Flynn K, Santos-Cortez RLP, Leal SM, et al. RNF213 rare variants in an ethnically diverse population with Moyamoya disease. Stroke. 2014;45:3200–3207. doi: 10.1161/STROKEAHA.114.006244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kamada F, Aoki Y, Narisawa A, Abe Y, Komatsuzaki S, Kikuchi A, et al. A genome-wide association study identifies RNF213 as the first Moyamoya disease gene. J Hum Genet. 2011;56:34–40. doi: 10.1038/jhg.2010.132. [DOI] [PubMed] [Google Scholar]
- 9.Liu W, Morito D, Takashima S, Mineharu Y, Kobayashi H, Hitomi T, et al. Identification of RNF213 as a susceptibility gene for Moyamoya disease and its possible role in vascular development. PLoS One. 2011;6:e22542. doi: 10.1371/journal.pone.0022542. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hitomi T, Habu T, Kobayashi H, Okuda H, Harada KH, Osafune K, et al. Downregulation of Securin by the variant RNF213 R4810K (rs112735431, G>A) reduces angiogenic activity of induced pluripotent stem cell-derived vascular endothelial cells from moyamoya patients. Biochem Biophys Res Commun. 2013;438:13–19. doi: 10.1016/j.bbrc.2013.07.004. [DOI] [PubMed] [Google Scholar]
- 11.Kobayashi H, Matsuda Y, Hitomi T, Okuda H, Shioi H, Matsuda T, et al. Biochemical and functional characterization of RNF213 (Mysterin) R4810K, a susceptibility mutation of Moyamoya disease, in angiogenesis in vitro and in vivo. J Am Heart Assoc. 2015;4:e002146. doi: 10.1161/JAHA.115.002496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hamauchi S, Shichinohe H, Uchino H, Yamaguchi S, Nakayama N, Kazumata K, et al. Cellular functions and gene and Protein expression profiles in endothelial cells derived from Moyamoya disease-specific iPS cells. PLoS One. 2016;11:e0163561. doi: 10.1371/journal.pone.0163561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Sonobe S, Fujimura M, Niizuma K, Nishijima Y, Ito A, Shimizu H, et al. Temporal profile of the vascular anatomy evaluated by 9.4-T magnetic resonance angiography and histopathological analysis in mice lacking RNF213: a susceptibility gene for moyamoya disease. Brain Res. 2014;1552:64–71. doi: 10.1016/j.brainres.2014.01.011. [DOI] [PubMed] [Google Scholar]
- 14.Ito A, Fujimura M, Niizuma K, Kanoke A, Sakata H, Morita-Fujimura Y, et al. Enhanced post-ischemic angiogenesis in mice lacking RNF213; a susceptibility gene for moyamoya disease. Brain Res. 2015;1594:310–320. doi: 10.1016/j.brainres.2014.11.014. [DOI] [PubMed] [Google Scholar]
- 15.Sonobe S, Fujimura M, Niizuma K, Fujimura T, Furudate S, Nishijima Y, et al. Increased vascular MMP-9 in mice lacking RNF213. Neuroreport. 2014;25:1442–1446. doi: 10.1097/WNR.0000000000000289. [DOI] [PubMed] [Google Scholar]
- 16.Dai D, Lu Q, Huang Q, Yang P, Hong B, Xu Y, et al. Serum miRNA signature in Moyamoya disease. PLoS One. 2014;9:e102382. doi: 10.1371/journal.pone.0102382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Zhao S, Gong Z, Zhang J, Xu X, Liu P, Guan W, et al. Elevated serum MicroRNA let-7c in Moyamoya disease. J Stroke Cerebrovasc Dis. 2015;24:1709–1714. doi: 10.1016/j.jstrokecerebrovasdis.2015.01.041. [DOI] [PubMed] [Google Scholar]
- 18.Park YS, Jeon YJ, Lee BE, Kim TG, Choi J-U, Kim D-S, et al. Association of the miR-146aC>G, miR-196a2C>T, and miR-499A>G polymorphisms with moyamoya disease in the Korean population. Neurosci Lett. 2012;521:71–75. doi: 10.1016/j.neulet.2012.05.062. [DOI] [PubMed] [Google Scholar]
- 19.Uhlmann S, Mracsko E, Javidi E, Lamble S, Teixeira A, Hotz-Wagenblatt A, et al. Genome-wide analysis of the circulating miRNome after cerebral ischemia reveals a reperfusion-induced MicroRNA cluster. Stroke. 2017;48:762–769. doi: 10.1161/STROKEAHA.116.013942. [DOI] [PubMed] [Google Scholar]
- 20.Castillo-Fernandez JE, Spector TD, Bell JT. Epigenetics of discordant monozygotic twins: implications for disease. Genome Med. 2014;6:60. doi: 10.1186/s13073-014-0060-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Mitchell PS, Parkin RK, Kroh EM, Fritz BR, Wyman SK, Pogosova-Agadjanyan EL, et al. Circulating microRNAs as stable blood-based markers for cancer detection. Proc Natl Acad Sci U S A. 2008;105:10513–10518. doi: 10.1073/pnas.0804549105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Yamauchi T, Tada M, Houkin K, Tanaka T, Nakamura Y, Kuroda S, et al. Linkage of familial moyamoya disease (spontaneous occlusion of the circle of Willis) to chromosome 17q25. Stroke. 2000;31:930–935. doi: 10.1161/01.STR.31.4.930. [DOI] [PubMed] [Google Scholar]
- 23.Mineharu Y, Liu W, Inoue K, Matsuura N, Inoue S, Takenaka K, et al. Autosomal dominant moyamoya disease maps to chromosome 17q25.3. Neurology. 2008;70(Issue 24, Part 2):2357–2363. doi: 10.1212/01.wnl.0000291012.49986.f9. [DOI] [PubMed] [Google Scholar]
- 24.Research Committee on the Pathology and Treatment of Spontaneous Occlusion of the Circle of Willis, Health Labour Sciences Research Grant for Research on Measures for Infractable Diseases Guidelines for diagnosis and treatment of moyamoya disease (spontaneous occlusion of the circle of Willis) Neurol medico-chirurgica. 2012;52:245–266. doi: 10.2176/nmc.52.245. [DOI] [PubMed] [Google Scholar]
- 25.Houkin K, Nakayama N, Kuroda S, Nonaka T, Shonai T, Yoshimoto T. Novel magnetic resonance angiography stage grading for Moyamoya disease. Cerebrovasc Dis. 2005;20:347–354. doi: 10.1159/000087935. [DOI] [PubMed] [Google Scholar]
- 26.Vejnar CE, Zdobnov EM. miRmap: comprehensive prediction of microRNA target repression strength. Nucleic Acids Res. 2012;40:11673–11683. doi: 10.1093/nar/gks901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Hamauchi S, Shichinohe H, Houkin K. Review of past and present research on experimental models of moyamoya disease. Brain Circ. 2015;1:88. doi: 10.4103/2394-8108.166377. [DOI] [Google Scholar]
- 28.Pfaffl MW. A new mathematical model for relative quantification in real-time RT-PCR. Nucleic Acids Res. 2001;29:e45. doi: 10.1093/nar/29.9.e45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kleinloog R, Regli L, Rinkel GJE, Klijn CJM. Regional differences in incidence and patient characteristics of moyamoya disease: a systematic review. J Neurol Neurosurg Psychiatry. 2012;83:531–536. doi: 10.1136/jnnp-2011-301387. [DOI] [PubMed] [Google Scholar]
- 30.Hori S, Kashiwazaki D, Yamamoto S, Acker G, Czabanka M, Akioka N, et al. Impact of interethnic difference of collateral Angioarchitectures on prevalence of hemorrhagic stroke in Moyamoya disease. Neurosurgery. 2018; 10.1093/neuros/nyy236. [DOI] [PubMed]
- 31.Finn NA, Searles CD. Intracellular and extracellular miRNAs in regulation of angiogenesis signaling. Curr Angiogenes. 2012;4:299–307. doi: 10.2174/2211552811201040299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Hoffmann CJ, Harms U, Rex A, Szulzewsky F, Wolf SA, Grittner U, et al. Vascular signal transducer and activator of transcription-3 promotes angiogenesis and neuroplasticity long-term after stroke. Circulation. 2015;131:1772–1782. doi: 10.1161/CIRCULATIONAHA.114.013003. [DOI] [PubMed] [Google Scholar]
- 33.Saber H, Himali JJ, Beiser AS, Shoamanesh A, Pikula A, Roubenoff R, et al. Serum insulin-like growth factor 1 and the risk of ischemic stroke: the Framingham study. Stroke. 2017;48:1760–1765. doi: 10.1161/STROKEAHA.116.016563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Koide M, Ikeda K, Akakabe Y, Kitamura Y, Ueyama T, Matoba S, et al. Apoptosis regulator through modulating IAP expression (ARIA) controls the PI3K/Akt pathway in endothelial and endothelial progenitor cells. Proc Natl Acad Sci. 2011;108:9472–9477. doi: 10.1073/pnas.1101296108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Hamada K, Sasaki T, Koni PA, Natsui M, Kishimoto H, Sasaki J, et al. The PTEN/PI3K pathway governs normal vascular development and tumor angiogenesis. Genes Dev. 2005;19:2054–2065. doi: 10.1101/gad.1308805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Ohkubo K, Sakai Y, Inoue H, Akamine S, Ishizaki Y, Matsushita Y, et al. Moyamoya disease susceptibility gene RNF213 links inflammatory and angiogenic signals in endothelial cells. Sci Rep. 2015;5:13191. doi: 10.1038/srep13191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Bogaerts J, Sydes MR, Keat N, McConnell A, Benson A, Ho A, et al. Clinical trial designs for rare diseases: studies developed and discussed by the international rare cancers initiative. Eur J Cancer. 2015;51:271–281. doi: 10.1016/j.ejca.2014.10.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Materials and Methods. Details supporting the main methods in the manuscript body are provided necessary to comprehend the results. (DOCX 35 kb)
Table S1. A list of microRNAs with respective top 15 and least 15 PCA scores. A list of microRNAs with respective top 15 and least 15 PCA scores (correlation value) for each microRNA for the component 2 (Y-axis) were provided, which separated MMD and control, based on the principal component analysis for the 309 plasma-microRNAs (Please see Fig. 2b). (DOCX 14 kb)
Table S2. Number of filtered target genes and target gene symbols for each of 17 differential circulating microRNAs in MMD, predicted by microRNA Target Filter implemented in IPA® (QIAGEN) and the miRmap web interface. The target genes were filtered based on their biological function analyzed using “Bioprofiler” implemented in IPA® (QIAGEN). As there is some overlap across microRNAs with respect to their target genes, so the total number of target genes at the bottom of the list is not a simple summation of each number of target genes. (DOCX 17 kb)
Figure S1. FACS plot to confirm the purity of iPSECs. The purity of the iPSECs after 5–6 times passages was confirmed as high as 91–97% in all clones using anti-CD31 antibody with the FACS. (TIF 1011 kb)
Table S3. The 41 target genes of hsa-miR-6722-3p/328-3p that were significantly down-regulated in MMD-iPSECs. Expression log2 fold change (log2 FC), p-value, and q-value were obtained from our previous publication (Hamauchi et al. 2016 [12]). Molecule type for each gene was obtained from the IPA tool. (DOCX 19 kb)
Data Availability Statement
The data used and/or analyzed during the current study are available from the corresponding author on reasonable request. Raw data of the microarray experiments can be accessed through the National Center for Biotechnology Information Gene Expression Omnibus (NCBI GEO accession number GSE100488).