

Abstract
This review evaluated prostate cancer studies from around the world and investigated the causes of differences among them. Prostate cancer incidence and mortality rates showed significant discrepancies between countries and ethnicities. In North America as well as in other western countries, the most common cancer was found to be prostate cancer; however, it appears to be not as prevalent among men in the Middle East and North Africa. Statistics show that screening of prostate-specific antigen levels should be applied depending on ethnicity and age. Other environmental aspects such as dietary and androgenic factors are believed to have caused these differences.
Prostate cancer is one of the most frequently encountered cancers in men, and it is estimated to affect 1,618,000 men and led to 366,000 deaths globally in 2015.1 Incidence rate of prostate cancer is lower in Arab men than that in men in North American regions, where large epidemiological studies are easily conducted.2 For Arab men in Qatar during 2006, the age-standardized incidence rate was as low as 3 per 100,000,3 but in the United States, it was 147.8 per 100,000.4
Prostate cancer can occur randomly in the population, can cluster unpredictably, or could be hereditary.5,6 Low incidence of prostate cancer may be explained by low prostate-specific antigen (PSA) levels due to smaller prostate size,7 thus leading to fewer biopsies being performed and lower testosterone levels8 in races such as Arabs and Asians, compared with whites and blacks. Prostate cancer rates are increasing rapidly in most countries and in low-risk populations. Although sparse, data from Saudi Arabia have indicated that prostate cancer occurs at a lower rate in Arab populations than in populations in western countries.9
Diagnosis of prostate cancer is commonly carried out by using PSA as a biomarker as well as using age- and race-specific ranges along with the free-to-total PSA ratio and PSA velocity and density, which may all contribute to a higher incidence rate of prostate cancer. Although PSA is commonly used as tumor marker for prostate cancer, it was found to be to sensitive hence leading to overdiagnosis and overtreatment. Prostate cancer treatment may result in impotence, incontinence, or both; thus, there is a need to use specific ranges based on different factors (mainly age and ethnicity).
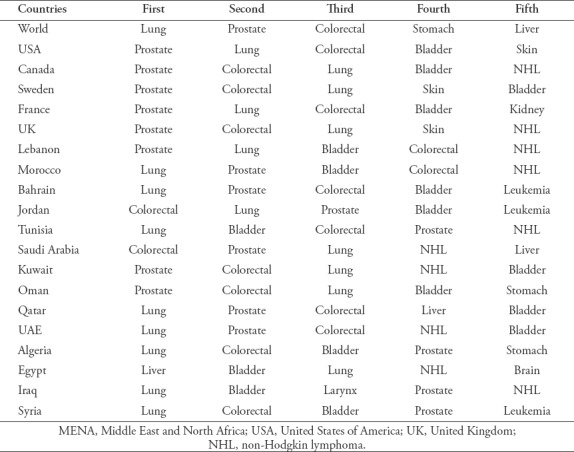
This brief review interpreted data from different studies conducted during the past 20 years that compared and evaluated prostate cancer rates in Arab men and those of other ethnicities. Differences in PSA levels required for screening, along with dietary and genetic variations of Arab men, and other potential reasons for these differences are discussed. Furthermore, the incidence rate of prostate cancer (Table 1) in the Arab communities was also reported and compared with that of lung cancer in the Middle East and North Africa (MENA) region (Table 2).
Table 1.
Prostate cancer incidence and mortality rates of Arab countries compared with worldwide rates.30
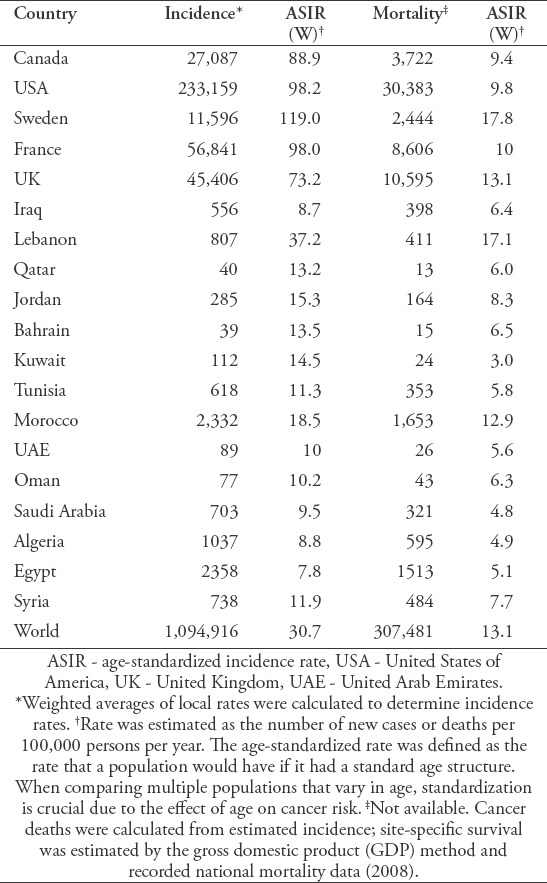
Table 2.
Five most frequent cancers in MENA compared with North America and rest of the World.31
Genetic factors
It is estimated that 25% of newly diagnosed cancers in men are prostate cancers. Middle Eastern, North African, and Asian men were found to have a lower prevalence of prostate cancer, but it is the most diagnosed cancer among Swedish men.10 Molecular differences in prostate carcinomas have not been widely explored across broad geographical regions. Nonetheless, prostate cancer is more frequent among black men and usually presents advanced-stage disease in comparison to white American men.11
Ethnic differences in genotype frequencies also exist for both SRD5A2 and CYP3A4, both of which have been previously associated with increased prostate cancer risks (black men have the highest frequency of those alleles11). The CAG repeat length differs in different populations and is related to the occurrence and evolution of prostate cancer.12,13
Dietary factors
A low-fat diet has been postulated to lead to lower serum testosterone levels.2 To establish a relationship between hormonal levels in different age groups and the risk of developing prostate cancer, extensive research work is required. Whether low rates of prostate cancer diagnoses in Arab countries will change in the future due to changes in dietary habits and other environmentally related risk factors remains to be observed.2 The Mediterranean diet has been correlated with low androstenedione, testosterone, and free testosterone levels,14 which is thought to help reduce the risk of prostate cancer.15
A low incidence of prostate cancer among the first generation of offspring of Middle Eastern immigrants has been evident in places such as Sweden,16 the Netherlands,17 and California (USA).18 However, with each new generation, the incidence gradually increases.17,19 Traditionally, it was thought that high fat consumption was positively correlated to prostate cancer, but findings in Saudi Arabia indicated that despite high saturated fat consumption, prostate cancer prevalence was still low.20
Androgenic factors
Despite the fact that prostate cancer incidence of prostate rates in Arab men are low (3-8 in 100,000 men/year), the factors responsible for it are unclear, and it has been established that prostate cancer risk and fluctuation in steroid hormone metabolism are strongly correlated. A study conducted on Omani and Kuwaiti men aged 15-80 years demonstrated that serum sex hormone-binding globulin, total testosterone, dehydroepiandrosterone sulfate, adrenal C19-steroids, and androstenedione levels were significantly lower compared with those of white men, particularly during the onset of adulthood.8 High serum levels of gender hormone-binding globulin, total testosterone, and dehydroepiandrosterone sulfate were found in Arabs diagnosed with prostate cancer, in comparison with individuals free of the disease. Results acquired from Arab men were compared with results from similarly aged white American men as well as German and Chinese men. Comparison between obtained results found no significant discrepancy between German and American men for mean serum levels of dehydroepiandrosterone sulfate. Results also indicated that there was no significant hormonal difference between Chinese and Arab men. High circulating androgens were found to be correlated with incidence of newly diagnosed prostate cancer in Arabs. The low incidence of prostate cancer among Arab men may be due to lower circulating androgens and adrenal precursors in comparison to white men.8,21
Socioeconomic factors
Lack of data related to prostate cancer in the MENA regions are due to multiple reasons. The fact that prostate tumors grow slowly and can take up to 10 or more years to become lethal makes it extremely difficult to study. Studying prostate cancer is expensive and time-consuming due to its prolonged onset. The reluctance of patients to participate in clinical trials may be a major contributor behind lack of data, especially in Arab populations.
The following are the main theories for the lower prevalence of prostate cancer in Arab countries: increasing average life expectancy; eradication of other endemic diseases; improving general health; globalization and environmental exposure; poor patient awareness about cancer screening; poor understanding of PSA use among doctors in Saudi Arabia; poor biopsy technique; poor pathology interpretation; lack of autopsy.
In 2008, a screening study was conducted in Riyadh, Saudi Arabia, which revealed that the prostate cancer incidence rate was high and that the disease was advanced. Riyadh ranked second in prostate cancer incidence in the country, with an estimated 2.5% incidence rate, of which 39.3% had positive biopsy results. From the cancer cases confirmed as prostate cancer, >17% had high Gleason scores, from which an estimated 27% were found to be metastatic and 21% presented as locally advanced cases. The stated figures indicate underreporting of prostate cancer in Saudi Arabia, hence leading to a delay in diagnosis and lack of awareness among individuals and health-care providers in terms of screening. This leads to the conclusion that large community-based studies are required to further understand prostate cancer.15
Screening for prostate cancer in the Arab World
For many years, there has been no scientific consensus regarding effective strategies to reduce the risk of prostate cancer. There are ongoing debates regarding the effectiveness of screening or the extent of potential benefits outweighing the risks.2 However, recent publications have demonstrated evidence that early detection results in reduced mortality in western populations.22 A recent review stated that men aged between 50 and 70 years should be encouraged to undergo PSA level screening.23
Screening decisions for prostate cancer are complex and require a physician with extensive experience and knowledge. It is imperative for physicians to seek continuous training and medical education so that they can perform screening procedures and ensure early detection of prostate cancer. Lack of knowledge and poor attitude regarding screening and treatment are challenges in the MENA region;24 therefore, these may be the main reasons behind the low detection of the disease.
Detection using serum PSA for Arab men
To date, serum PSA remains useful for detecting prostate cancer. Western countries have established a cutoff level of total PSA (4 ng/mL) to differentiate between benign and malignant prostatic diseases and to indicate when biopsies are needed. Generalization of cutoff values for all ages have been proven to be insufficient; hence, age-specific values should be considered for diagnosis.2 Both age and PSA were found to be positively correlated: PSA increases with increasing age increases.2 Studies have begun to determine population-specific ranges for PSA because racial variations may play a role.7
Detection programs using total PSA were found to have a high false-positive rate. False-positive results due to increased levels of total PSA occur in benign conditions (for example, benign prostatic hyperplasia [BPH]) as well as clinical and subclinical prostatitis.25 Increased total serum PSA from those conditions can potentially lead to diagnostic dilemmas for prostate cancer detection programs using serum PSA as the primary screening tool. American and European men were found have a low probability of clinically detectable prostate cancer if their total PSA is <2.5 ng/mL, as opposed to individuals with total PSA >10 ng/mL, who have a >50% chance of detecting prostate cancer.27 Despite the fact that PSA testing is the most common tool for diagnosing prostate cancer, it lacks specificity within a range of 4-10 ng/mL, leading to a diagnostic zone of only 25%.25
Discriminating prostate cancer from various benign diseases can be achieved by measuring different forms of PSA. Patients diagnosed with prostate cancer for unknown reasons were found to have lower levels of free PSA compared with those who have normal prostate or benign disease.27 Recent evidence indicates that using the free-to-total PSA ratio was found to be reliable in evaluating prostate cancer while having minimum loss of sensitivity in detection, especially in individuals having a total PSA range between 4 and 10 ng/mL. Individuals at highest risk for prostate cancer were found to have a free-to-total PSA ratio <25%; hence, complete investigations are required to confirm the disease.25
Urologists have noticed that despite low incidences of prostate cancer in the MENA regions, the disease has been on the rise. Arab men with serum total PSA >10 ng/mL were studied to conclude that the high false positive rate is due to BPH in comparison with European and American men with similar PSA levels who had a higher risk of developing the disease.25
Total PSA >10 ng/mL in Arab men may be the result of benign conditions such as BPH with prostatitis or prostate cancer. The presentation of BPH with prostatitis is accompanied by total PSA >10 ng/mL, with a gradual reduction <4 ng/mL with time. Free PSA and PSA density were not found to be effective diagnostic tools for prostate cancer. In comparison with white American and European men, PSA levels >10 ng/mL in Arabs were found to be due to BPH with prostatitis.25,26
Age-specific reference ranges of PSA in Arabs
Arabs exhibit lower prostate volumes and PSA levels in comparison to white men.7,27 Lower PSA levels in Asian men (Arabs included) are thought be due to lower prostate volumes and difference in the cellular composition of the prostate glands.7 Prostate volume and levels of serum PSA are age- and race-dependent, indicating the importance of having age-specific reference ranges for these variables, thus leading to an increase in the positive predictive value of PSA, which will result in proper estimation of prostate cancer diagnosis in individual communities.
In 2003, age- and population-specific reference ranges for PSA of Saudi men have been defined.27 Men between 40 and 89 years were found to have normal values. The mean normal PSA values based on age were the following: 40-49 years, 0.87 ng/mL; 50-59 years, 1.36 ng/mL; 60-69 years, 1.81 ng/mL; 70-79 years, 2.32 ng/mL; 80-89 years, 2.36 ng/mL, for which all age groups had >30% free PSA. Men having PSA levels <4 ng/mL were found to have unchanged free PSA percentages, of which only 16.6% had a free–to-total PSA ratio of 18%, making the upper limit of PSA in Saudi men similar to that of Korean and Chinese men. The study found that Saudi men have lower PSA values than white men. The free PSA percentage for men with PSA <4 ng/mL may therefore be used as a race-specific value for diagnosing prostate cancer.27
A 2005 study of healthy Kuwaiti and Omani men arrived at the same conclusion that Arab men have lower PSA levels and smaller prostate volumes in comparison to white men, similar to those of Chinese and Japanese men.7 Age-specific reference ranges for PSA have been determined along with the prostate volumes of men between 15 and 79 years from the previous study. The prostate volume of men >40 years were determined by conducting transrectal ultrasonography and digital rectal examination. The PSA serum ranges for each age group of Arab men were the following: 40-49 years, 0-0.9 ng/mL (prostate volume, 8-22 mL); 60-69 years, 0-2.7 ng/mL (prostate volume, 9–30 mL); 70-79 years, 0-5.5 ng/mL (prostate volume, 10-33 mL),7 thus concluding that serum PSA and prostate volume are directly proportional with age.7
Serum PSA in Arab and Asian men diagnosed with BPH with prostatitis were higher in comparison with white men. The reason for this is unknown, but one theory points to the presence of late prostatic symptoms.25,26 Kehinde et al25 reported that 17.7% of elevated PSA levels in patients were due to prostate cancer, whereas 58.6% were due to BPH and 23.7% were due to BPH with prostatitis. Similar results were found in Kuwait. Serum total PSA >10 ng/mL can lead physicians practicing in Arab and Asian countries to miss the diagnosis.25
To date, no other tumor markers have been detected to enhance the specificity or sensitivity of total or free PSA. Transurethral prostatic resection may lead to a decrease in PSA levels to normal values with or without prostatitis treatment in BPH patients. This study indicates that Arabs with total PSA >10 ng/mL do not have prostate cancer. An increase in the PSA level may indicate prostate cancer, requiring repetition of clinical and histological evaluation.25
A study of the Saudi population in 2010 compared the diagnostic utility of complexed PSA, total PSA, and their ratios with free PSA for BPH and prostate cancer. The data from this study showed few advantages with the use of complexed PSA instead of total PSA for discriminating BPH and prostate cancer.30
Age-specific PSA cutoff level for Arab men
A study supporting early diagnosis of prostate cancer investigated age-specific PSA cutoff values in Arab men. According to the findings, using lower cutoff values for PSA may frequently detect prostate cancer while it is still curable. Three reasons have been established as to why screening PSA with a lower threshold is useful in men aged 40-49 years. First, younger men have a lower incidence of BPH. Second, screening in younger men is more likely to detect localized, curable cancer. Third, younger men are less likely to have significant medical comorbidities and are more likely to undergo radical treatments such as surgery.
Prostate cancer is prevalent in 25% of men with PSA level between 4 and 10 ng/mL and also in 25% of men with PSA level <4 ng/mL. This poor specificity has led to the establishment of age-adjusted PSA level thresholds. As the difference in incidence of BPH between men younger than 60 years and older than 60 years increases (<60 years, 9%; >60 years, 17%), the screening of younger men should yield fewer false-positive results.29
A 2008 study of Egyptian men explored prostate cancer detection in patients younger than 50 years using a PSA cutoff of <4 ng/mL. Twenty-eight samples were drawn from 2 groups of men, group A (<50 years; mean age, 46 years) and group B (>50 years; mean age, 58 years). Differences in pathological findings, PSA levels, digital rectal examination findings, and body mass index between groups were measured. The mean PSA level was 1.9±1.6 ng/mL in group A and 2±1.6 ng/mL in group B, and 1.8% of the patients in group A and 10.7% of the patients in B tested positive for prostatic adenocarcinoma. Group A was found to have a higher incidence of high-grade prostatic intraepithelial neoplasia (PIN) in comparison to group B (11 versus 4 cases). Digital rectal examination had no significant association with pathological findings in either group. Body mass index was found to be correlated positively with PSA levels in group A patients, but not with those in group B. A new PSA cutoff point for younger adults is acceptable. A serum PSA level of 2 ng/mL should be endorsed as a cutoff point for screening and biopsy in asymptomatic men younger than 50 years. Young patients with low serum PSA were found to have high PIN, and this should be further studied.29
This study recommends a serum PSA level of 2 ng/mL as an accurate cutoff point for screening men younger than 50 years (to avoid missing 14.3% of positive cases with PSA 2.5 ng/mL). High-grade PIN was detected histopathologically in 19.6% of this age group, prompting the need for follow-up care for prostate cancer evaluation.29
In conclusion, prostate cancer screening remains controversial in the Arab world. However, it is clear that the incidence of this disease is increasing. As the average life expectancy increases in the Arab population, prostate cancer may start to pose a health-care problem similar to that in western countries. Hence, genetic and environmental variations from region to region should be considered when establishing clinical standards.
Acknowledgment
The project was fully financially supported by the King Saud University, Riyadh, Saudi Arabia, through the Vice Deanship of Research Chairs.
Footnotes
References
- 1.Fitzmaurice C, Allen C, Barber R. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015. JAMA Oncol. 2017;3:524. doi: 10.1001/jamaoncol.2016.5688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mosli HA. Prostate cancer in Saudi Arabia in 2002. Saudi Med J. 2003;24:573–581. [PubMed] [Google Scholar]
- 3.Bener A, Ayub H, Kakil R, Ibrahim W. Patterns of cancer incidence among the population of Qatar: a worldwide comparative study. Asian Pac J Cancer Prev. 2008;9:19–24. [PubMed] [Google Scholar]
- 4.National Cancer Institute. SEER Program. Cancer Stat Facts: Prostate. [[cited 22 March 2015]]. Available from: http://seer.cancer.gov/statfacts/html/prost.html .
- 5.Keetch DW, Humphery PA, Smith DS, Stahl D, Catalona WJ. Clinical and pathological feature of hereditary prostate cancer. J Urol. 1996;155:1841–1843. [PubMed] [Google Scholar]
- 6.McLellan DL, Norman RW. Hereditary aspects of prostate cancer. Can Med Assoc J. 1995;153:895–900. [PMC free article] [PubMed] [Google Scholar]
- 7.Kehinde EO. Age-specific reference levels of serum prostate-specific antigen and prostate volume in healthy Arab men 2005. BJU Int. 2005;96:308–312. doi: 10.1111/j.1464-410X.2005.05620.x. [DOI] [PubMed] [Google Scholar]
- 8.Kehinde EO. Do differences in age specific androgenic steroid hormone levels account for differing prostate cancer rates between Arabs and Caucasians? Int J Urol. 2006;13:354–361. doi: 10.1111/j.1442-2042.2006.01305.x. [DOI] [PubMed] [Google Scholar]
- 9.National Cancer Registry. Cancer incidence in Saudi Arabia 1997-1998 report. Riyadh (KSA): Ministry of Health; 2001. [Google Scholar]
- 10.Alyaiya AA. Proteomics-based signature for human benign prostate hyperplasia and prostate adenocarcinoma. Int J Oncol. 2011;38:1047–1057. doi: 10.3892/ijo.2011.937. [DOI] [PubMed] [Google Scholar]
- 11.Zeigler-Johnson C, Walker A, Mancke B, Spangler E, Jalloh M, McBride S, et al. Ethnic differences in the frequency of prostate cancer susceptibility alleles at SRD5A2 and CYP3A4. Hum Heredity. 2002;54:13–21. doi: 10.1159/000066695. [DOI] [PubMed] [Google Scholar]
- 12.Li J, Mercer E, Gou X, Lu YJ. Ethnical disparities of prostate cancer predisposition: genetic polymorphisms in androgen-related genes. Am J Cancer Res. 2013;3:127–151. [PMC free article] [PubMed] [Google Scholar]
- 13.Giovannucci E, Stampfer MJ, Krithivas K, Brown M, Dahl D, Brufsky A, et al. The CAG repeat within the androgen receptor gene and its relationship to prostate cancer. Proc Natl Acad Sci USA. 1997;94:3320–3323. doi: 10.1073/pnas.94.7.3320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hamalainen E, Adlercreutz H, Puska P, Pietinen P. Diet and serum sex hormones in healthy men. J Steroid Biochem. 1984;20:459–464. doi: 10.1016/0022-4731(84)90254-1. [DOI] [PubMed] [Google Scholar]
- 15.Rabah DM, Arafa MA. Prostate cancer screening in Saudi population: an explanatory trial study. Prostate Cancer Prostatic Dis. 2010;13:191–194. doi: 10.1038/pcan.2009.60. [DOI] [PubMed] [Google Scholar]
- 16.Hemminki K, Li X, Czene K. Cancer risks in first-generation immigrants to Sweden. Int J Cancer. 2002;99:218–228. doi: 10.1002/ijc.10322. [DOI] [PubMed] [Google Scholar]
- 17.Visser O, van Leeuwen FE. Cancer risk in first generation migrants in North-Holland/Flevoland, The Netherlands 1995-2004. Eur J Cancer. 2007;43:901–908. doi: 10.1016/j.ejca.2006.12.010. [DOI] [PubMed] [Google Scholar]
- 18.Nasseri K, Mills P, Allan A. Cancer incidence in the Middle Eastern population of California 1988-2004. Asian Pac J Cancer Prev. 2007;8:405–411. [PMC free article] [PubMed] [Google Scholar]
- 19.Grulich AE, McCredie M, Coates M. Cancer incidence in Asian migrants to New South Wales, Australia. Br J Cancer. 1995;71:400–408. doi: 10.1038/bjc.1995.82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Hanash K, Al-Othaimeen A, Kattan S, Lindstedt E, Al-Zahrani H. Prostatic carcinoma: a nutritional disease? Conflicting data from the Kingdom of Saudi Arabia. J Urol. 2000;164:1570–1572. [PubMed] [Google Scholar]
- 21.Kehinde EO. Prostate cancer risk: the significance of differences in age related changes in serum conjugated and unconjugated steroid hormone concentrations between Arab and Caucasian men. Int Urol Nephrol. 2006;38:33–44. doi: 10.1007/s11255-005-3619-1. [DOI] [PubMed] [Google Scholar]
- 22.Schroder FH. Prostate cancer around the world. An overview. Semin Orig Invest. 2010;28:663–667. doi: 10.1016/j.urolonc.2009.12.013. [DOI] [PubMed] [Google Scholar]
- 23.Arafa M, Rabah D. With increasing trends of prostate cancer in the Saudi Arabia and Arab world: should we start screening programs? World J Clin Oncol. 2017;8:447–449. doi: 10.5306/wjco.v8.i6.447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Arafa MA, Rabah DM, Abdel-Gawad E, Ibrahim FK. Association of physicians'knowledge and behavior with prostate cancer counseling and screening in Saudi Arabia. Saudi Med J. 2010;31:1245–1250. [PubMed] [Google Scholar]
- 25.Kehinde EO. High serum prostate-specific antigen levels in the absence of prostate cancer in Middle-Eastern men: the clinician's dilemma. BJU Int. 2003;91:618–622. doi: 10.1046/j.1464-410x.2003.04199.x. [DOI] [PubMed] [Google Scholar]
- 26.Sheikh M, Al-Saeed O, Kehinde EO, Sinan T, Anim JT, Ali Y. Utility of volume adjusted prostate specific antigen density in the diagnosis of prostate cancer in Arab men. Int Urol Nephrol. 2005;37:721–726. doi: 10.1007/s11255-005-4683-2. [DOI] [PubMed] [Google Scholar]
- 27.Kamal BA. Prostate specific antigen reference ranges in Saudi men. Saudi Med J. 2003;24:665–668. [PubMed] [Google Scholar]
- 28.Tamimi W. Complexed and total PSA in patients with benign prostatic hyperplasia and prostate cancer. Br J Biomed Sci. 2010;67:184–188. doi: 10.1080/09674845.2010.11730317. [DOI] [PubMed] [Google Scholar]
- 29.Hekal IA. The patients less than 50 years: is there a need to lower the PSA cutoff point? Prostate Cancer Prostatic Dis. 2009;12:148–151. doi: 10.1038/pcan.2008.48. [DOI] [PubMed] [Google Scholar]
- 30.IARC, WHO. Prostate Cancer: Estimated Incidence, Mortality and Prevalence Worldwide in 2012. [[Accessed 2018 March 5]]. Available from URL: http://globocan.iarc.fr/old/FactSheets/cancers/prostate-new.asp .
- 31.IARC, WHO. Prostate Cancer: Frequency Worldwide in 2012. [[Accessed 2018 March 5]]. Available from URL: http://globocan.iarc.fr/Pages/fact_sheets_population.aspx .