

Abstract
Introduction and Aims
Gender and age patterns of drinking are important in guiding country responses to harmful use of alcohol. This study undertook cross‐country analysis of drinking across gender, age groups in some high‐and middle‐income countries.
Design and Methods
Surveys of drinkers were conducted in Australia, England, Scotland, New Zealand, St Kitts and Nevis (high‐income), Thailand, South Africa, Mongolia and Vietnam (middle‐income) as part of the International Alcohol Control Study. Drinking pattern measures were high‐frequency, heavier‐typical quantity and higher‐risk drinking. Differences in the drinking patterns across age and gender groups were calculated. Logistic regression models were applied including a measure of country‐level income.
Results
Percentages of high‐frequency, heavier‐typical quantity and higher‐risk drinking were greater among men than in women in all countries. Older age was associated with drinking more frequently but smaller typical quantities especially in high‐income countries. Middle‐income countries overall showed less frequent but heavier typical quantities; however, the lower frequencies meant the percentages of higher risk drinkers were lower overall compared with high‐income countries (with the exception of South Africa).
Discussion and Conclusions
High‐frequency drinking was greater in high‐income countries, particularly in older age groups. Middle‐income countries overall showed less frequent drinking but heavier typical quantities. As alcohol use becomes more normalised as a result of the expansion of commercial alcohol it is likely frequency of drinking will increase with a likelihood of greater numbers drinking at higher risk levels.
Keywords: alcohol consumption, drinking patterns, age, gender, International Alcohol Control (IAC) study
Introduction
Alcohol consumption is a leading preventable health risk factor for the burden of disease, and in 2016 was estimated to have caused 99.2 million disability‐adjusted life years and accounted for 4.2% of total disability‐adjusted life years 1. The harmful use of alcohol disproportionately affects individuals, families and societies in different countries 2. Alcohol consumption is reportedly increasing in emerging markets and especially in low‐ and middle‐income countries, particularly among young people and women 3, 4.
Alcohol consumption varies between countries and cultures as well as individuals. A number of studies report that drinking patterns have significant influence on alcohol‐related harm at individual and aggregated levels 5, 6, 7, 8. Alcohol policies are developed with the aim of reducing harmful use of alcohol and its related health and social burden in a target population and society 2, 3, 9. Understanding patterns of alcohol use across countries and cultures is important for alcohol policy development to prevent and control alcohol‐related problems.
Individual and societal factors affecting levels of alcohol consumption have been identified including age, gender and economic development 3. The research on comparing drinking patterns across countries against these key factors is important.
Young people are more likely to engage in heavy episodic drinking than others 10. Typically, a greater proportion of total alcohol consumed by young people is consumed during heavy drinking episodes 11, 12. Studies, including some cross‐country research, have found that while alcohol consumption generally declines with age, older drinkers typically consume alcohol more frequently than younger age groups 3, 12, 13.
With respect to gender, cross‐country studies found that among drinkers, the percentages of high‐volume drinking were consistently greater in men than women, while high‐frequency drinking was greatest in the oldest age group, particularly among men 13, 14. In addition, a previous study reporting patterns of alcohol consumption from the 35 countries in 1997–2007 indicates that declines in high‐volume and heavy episodic drinking with increasing age are more typical in Europe and in English‐speaking countries 13.
Although previous studies indicate a large variation in drinking patterns among countries, there is limited formal comparative work on how country‐level economic development may be related to different types of drinking patterns.
The International Alcohol Control (IAC) Study is a new multi‐country collaborative project set up to collect comparable measures of alcohol consumption and relevant environmental factors, and to assess the impact of alcohol policies in different cultural and economic contexts on policy‐related behaviours and alcohol consumption 15. The design of the IAC study allows for follow‐up surveys and comparative research over time. Two research tools are used: surveys of drinkers to document drinking patterns and policy relevant behaviours and the Alcohol Environmental Protocol (a protocol for policy analysis). This current study uses survey data only. The IAC study was designed to allow for the inclusion of a range of countries and to date middle‐ and high‐income countries have participated. The IAC countries are largely self‐selected depending on availability of resources. Countries included in the current study are Australia, England, Mongolia, New Zealand, Scotland, South Africa, St Kitts and Nevis, Thailand and Vietnam. These countries represent a diverse range of cultures, socio‐economic contexts, alcohol policies and drinking environments (for further details on the cultural and policy contexts of countries please see Casswell et al. (2018) 16). It is the first international collaborative project to collect detailed general population survey data on alcohol consumption among drinkers using detailed beverage‐specific location based survey questions. The survey instrument allows for high coverage of alcohol available for consumption (based on sales or tax data) 17, 18, and provides comparable consumption data for different alcohol markets, including those with a sizeable proportion of informal alcohol. These new data allow for analyses by age and gender and economic development across countries, including for different consumption measures.
The purpose of this study was therefore to investigate drinking patterns by gender and age in a range of countries differing in income level.
Methods
This study obtained data from the multi‐country International Alcohol Control Policy Study. It focuses on alcohol consumption data from five high‐income countries (Australia, England, Scotland, New Zealand and St Kitts and Nevis) and four middle‐income countries (Thailand, South Africa, Mongolia and Vietnam) as defined by the World Bank 19.
Design and sampling
The study was cross‐sectional and conducted in different countries between 2011 (New Zealand) and 2016 (St Kitts and Nevis). Sampling methods were designed to obtain a random representative sample of drinkers aged 16–65 and each country utilised the sampling frame that was most appropriate in their context. Multi‐stage sampling of geographical units was used in St Kitts and Nevis, Thailand, South Africa, Mongolia and Vietnam (the latter three countries sample were sub‐national) and national stratified telephone samples were used in Australia (including cell phones), England, Scotland and New Zealand.
Interviews were conducted via computer‐assisted face‐to‐face interviewing using tablets in Mongolia, South Africa, St Kitts and Nevis, Thailand and Vietnam and over the telephone in Australia, England, Scotland and New Zealand. A screening interview established eligibility for participation in the study (drinking in the last 6 months and age 16–65 years). Eligible individuals were enumerated, and then one respondent was selected at random by the computer/tablet. In Australia, risky drinkers were oversampled, one third of abstainers and those that did not consume alcohol riskily (defined as consuming more than 50 g in a session monthly or more), this has been accounted for with weighting.
The studies were approved by ethics committees in the respective countries. Response rates varied from 16% in England, 60% in New Zealand and St Kitts and Nevis to 99% in Vietnam.
The years in which data collection was undertaken in each country are as follows: Australia (2013), England (2012/2013), Scotland (2012/2013), New Zealand (2011), St Kitts and Nevis (2014/16), Thailand (2012/13), South Africa (2014), Mongolia (2013) and Vietnam (2014).
The total sample included in the current study was 14 772 broken down as follows: Australia (n = 1792), England (n = 1712), Scotland (n = 1696), New Zealand (n = 2001), St Kitts and Nevis (n = 1307), Thailand (n = 2377), South Africa (n = 1007), Mongolia (n = 862) and Vietnam (n = 2018).
For further details on the methodology of the IAC study, please see Huckle et al. (2018) 20.
Measurement
Countries adapted the English IAC questionnaire and translated and back‐translated it into local languages (Mongolia, South Africa, Thailand, Vietnam) and piloted it before use. The questionnaire comprised various domains, including demographic factors (e.g. age and gender) and alcohol consumption.
The IAC study utilises a within‐location beverage‐specific framework and allows countries to adapt the consumption measurement framework to their context in terms of specific drinking locations. The framework asks for frequency of drinking in all locations in which drinking occurs and then typical occasion quantity in each location in the past 6 months. The IAC consumption framework asks beverage‐specific questions for each location at which participants drink. In this current analysis, a standard drink was defined as 15 mL (12 g) of alcohol. For further details on the measures and their derivation, please see Huckle et al. (2018) 20.
Frequency of drinking
Using the data on frequency of drinking in different locations over the past 6 months and quantity consumed on a typical occasion in each location, new variables were derived at the analysis stage. Frequency of drinking is the sum of all drinking occasions at all locations over the past 6 months. Three categories of drinking frequency were defined as ‘low’—up to once a month, ‘medium’—more than once a month but less than once a week and ‘high’—once a week or more. ‘High‐frequency drinking’ was defined as drinking frequency at the high category.
Typical occasion quantity
Typical occasion quantity is the weighted average across all locations (locations that are drunk at less frequently have less weight). The typical quantity was quantified in terms of mL ethanol consumed on an occasion. It was categorised into ‘low’—fewer than four drinks, ‘medium’—four to six drinks, ‘medium‐high’—more than six drinks but not more than eight drinks, and ‘high’—more than eight drinks. In some analyses, typical occasion quantity was dichotomised as ‘heavier‐typical quantity drinking’ (more than eight drinks vs. less than eight drinks).
Total consumption (volume) and drinking risk category
Total alcohol consumption in the past 6 months is a product of frequency of drinking and typical occasion quantity. Total alcohol consumed per drinker was quantified as litres of ethanol consumed in the last 6 months.
Using quantity and frequency of drinking, risk category (drinking risk) was categorised into three levels: ‘lower’—up to four drinks on an occasion or four to six drinks on an occasion less than once per week, ‘increased’—four to six drinks on an occasion at least once per week or 6+ drinks on an occasion less than once per week, and ‘high’— more than six drinks on an occasion at least once per week. ‘Higher‐risk drinking’ referred to the high category. Where participants did not provide complete data on quantity and frequency of drinking in all locations, their data were omitted.
Gender and age
To describe patterns of drinking, we divided the survey samples by gender (male and female) and age (six groups). Age ranges were grouped in six categories: ages 16–19, 20–24, 25–34, 35–44, 45–54 and 55–65 years.
Country‐level income
Country economic development was defined by country‐level income based on World Bank classification 19. The countries were categorised as high income or middle income as previously indicated in the first paragraph of methods section.
Analysis
Weighting
As one person was selected per household, unequal probability of respondent selection was corrected for. Some countries also calculated post‐stratification weights (Australia, Scotland, England and New Zealand). Australia oversampled heavy drinkers, so weights were calculated to account for this.
Outliers
For consumption data, a statistical process was used to deal with outliers whereby the right‐skewed distributions of consumption‐related variables were transformed to normalise them. The transforming function was logarithmic (for typical occasion quantity) and power function (for frequency of drinking). The transformed series was then centred and scaled by subtracting the mean and dividing by the standard deviation and the 99th percentile of respondents were then removed.
Descriptive analysis
We described average estimates of drinking frequency, typical occasion quantity and total alcohol consumption per drinker in the nine IAC countries. A bubble plot was used to display the three measures of alcohol use in a single figure.
The distribution of high‐frequency, heavier‐typical quantity and higher‐risk drinking categories were disaggregated by gender and age groups across the countries. We computed male‐to‐female (M–F) ratios to present differences in drinking patterns between men and women across the countries. Trend or direction of change in drinking patterns by age groups was also described.
Logistic regression
It is important to account for the sampling design during analysis to make sure that the standard errors are not underestimated (i.e. where modelling or statistical testing is being undertaken). This was not able to be done simply due to each of the countries in our study having different sampling designs, ranging from a simple random to a stratified multistage sample. The process used to adjust for cross‐country sampling design was based on Kaminska and Lynn (2017) 21. For a detailed description of this process, please see Huckle et al. (2018) 20.
We applied the logistic regression analysis approach to determine associations between age and gender and drinking patterns across the IAC countries. Multiple logistic regression analyses were performed to estimate odds ratios for being in the high‐frequency, heavier‐typical occasion quantity and higher‐risk drinking. A measure of country‐level income was included (high‐income vs. middle‐income). All analyses were weighted to account for the sampling design of the complex surveys using Stata's svy methods 22.
Results
Overall consumption and drinking patterns across countries
Figure 1 displays results on drinking frequency, typical occasion quantity and total consumption per drinker (volume) in the nine countries. It shows that average drinking frequency is highest in St Kitts and Nevis (124 drinking occasions in 6 months), followed by New Zealand (90 occasions), and England and Australia (83 occasions). Scotland, Thailand and Vietnam show drinking frequencies of between 64 and 79 occasions. South Africa and Mongolia show lower drinking frequencies (36–39 occasions).
Figure 1.
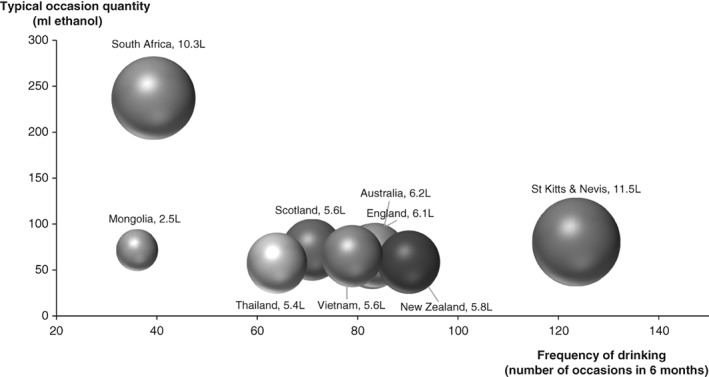
Bubble plots for alcohol consumption variables in nine International Alcohol Control study countries.
Note: The bubble plots display estimates of three alcohol consumption variables of nine International Alcohol Control study countries in terms of frequency of drinking, typical occasion quantity and total alcohol consumption per drinker. Size of bubble plots refers to total alcohol consumption per drinker (litre of ethanol). Australia's and England's estimates are very similar; their plots are almost overlapping.
For typical occasion quantity, the highest quantity is found in South Africa (237 ethanol mL), followed by St Kitts and Nevis (80 mL). Australia, England, Mongolia and Vietnam have typical quantities between 65 and 72 ethanol mL, whereas New Zealand and Thailand have slightly lower typical occasion quantities (58–59 ethanol mL) (Figure 1).
For total alcohol consumption in 6 months, St Kitts and Nevis has the highest estimate at 11.5 L of ethanol per drinker, followed by South Africa (10.3 L). Australia, England, New Zealand, Scotland, Thailand and Vietnam have estimates of total consumption between 5.6–6.1 L. The lowest estimate is 2.5 L for Mongolia (Figure 1).
Table 1 provides estimates for the three drinking patterns across the countries. Percentages of high‐frequency drinking are high in the high‐income countries (67–78%). The percentage of heavier‐typical quantity drinking (more than eight drinks on a typical occasion) is highest in South Africa (54%) and lowest in England, New Zealand and Thailand (around 10%). Apart from South Africa (highest, 37%) and Mongolia (lowest, 8%), percentages for the higher‐risk drinking (more than six drinks on an occasion at least once a week) category are between 19% and 27% in the high‐income countries and 14–19% in the middle‐income countries.
Table 1.
Summary statistics for drinking patterns by gender and age groups in nine International Alcohol Control study countries
| All | Male | Female | M–F ratio a | 16–19 years (age 1) | 20–24 years (age 2) | 25–34 years (age 3) | 35–44 years (age 4) | 45–54 years (age 5) | 55–65 years (age 6) | Age direction (Group with highest value) b | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| % High‐frequency drinking c | |||||||||||
| Australia | 71.0 | 76.5 | 65.1 | 1.2 | 43.7 | 71.4 | 76.4 | 63.6 | 76.0 | 77.2 | ↑(6) |
| England | 77.8 | 84.0 | 71.2 | 1.2 | 64.5 | 75.1 | 79.8 | 79.3 | 78.3 | 80.5 | ↑(6) |
| Scotland | 74.7 | 79.5 | 69.8 | 1.1 | 58.2 | 85.8 | 73.7 | 76.1 | 75.4 | 73.6 | ~(2) |
| New Zealand | 75.3 | 82.0 | 68.5 | 1.2 | 62.3 | 73.6 | 74.0 | 73.5 | 79.8 | 81.3 | ↑(6) |
| St Kitts & Nevis | 67.3 | 79.5 | 44.8 | 1.8 | 66.2 | 67.8 | 66.2 | 63.6 | 69.4 | 67.0 | ~(5) |
| Thailand | 41.0 | 55.7 | 21.4 | 2.6 | 22.3 | 37.9 | 42.9 | 42.9 | 42.0 | 41.4 | ∧(3,4) |
| South Africa | 49.1 | 56.0 | 36.4 | 1.5 | 15.2 | 47.7 | 48.9 | 53.1 | 59.1 | 61.2 | ↑(6) |
| Mongolia | 16.0 | 21.7 | 9.3 | 2.3 | 10.0 | 12.0 | 18.9 | 19.3 | 14.3 | 10.9 | ∧(4) |
| Vietnam | 59.3 | 63.4 | 18.9 | 3.4 | 36.4 | 51.7 | 58.7 | 62.1 | 58.1 | 59.3 | ~(4) |
| % Heavier‐typical quantity drinking d | |||||||||||
| Australia | 12.2 | 16.1 | 8.1 | 2.0 | 24.2 | 23.7 | 17.9 | 9.2 | 12.5 | 6.3 | ↓(1) |
| England | 10.0 | 14.0 | 5.8 | 2.4 | 19.5 | 11.7 | 9.7 | 11.0 | 8.5 | 5.9 | ↓(1) |
| Scotland | 13.8 | 22.4 | 4.9 | 4.6 | 19.5 | 27.9 | 16.8 | 12.8 | 11.0 | 6.0 | a↓(2) |
| New Zealand | 10.2 | 14.2 | 6.2 | 2.3 | 22.7 | 25.3 | 13.8 | 8.8 | 4.7 | 1.9 | a↓(2) |
| St Kitts & Nevis | 15.6 | 21.3 | 5.0 | 4.2 | 13.3 | 13.6 | 12.7 | 11.2 | 23.8 | 20.0 | ~(5) |
| Thailand | 10.3 | 14.5 | 4.8 | 3.0 | 10.0 | 13.9 | 15.3 | 10.9 | 10.1 | 4.8 | ∧(3) |
| South Africa | 53.6 | 60.5 | 40.6 | 1.5 | 63.6 | 54.1 | 59.2 | 54.7 | 40.3 | 45.6 | ↓(1) |
| Mongolia | 14.5 | 22.8 | 5.0 | 4.5 | 6.7 | 10.8 | 11.0 | 19.8 | 18.5 | 10.9 | ∧(3) |
| Vietnam | 13.1 | 14.2 | 1.6 | 8.8 | 18.2 | 15.5 | 22.4 | 15.2 | 10.8 | 7.3 | ∧(3) |
| % Higher‐risk drinking e | |||||||||||
| Australia | 21.4 | 28.7 | 13.6 | 2.1 | 21.5 | 33.4 | 27.2 | 21.6 | 20.2 | 18.9 | a↓(2) |
| England | 25.6 | 33.9 | 16.7 | 2.0 | 27.2 | 37.5 | 27.1 | 28.0 | 23.5 | 17.6 | a↓(2) |
| Scotland | 27.3 | 37.7 | 16.5 | 2.3 | 17.7 | 49.7 | 31.8 | 28.9 | 23.0 | 18.6 | a↓(2) |
| New Zealand | 18.7 | 25.6 | 11.7 | 2.2 | 35.1 | 41.5 | 24.6 | 14.0 | 14.2 | 6.2 | a↓(2) |
| St Kitts & Nevis | 27.4 | 35.6 | 12.3 | 2.9 | 28.0 | 23.2 | 30.3 | 20.4 | 34.0 | 26.1 | ~(5) |
| Thailand | 14.3 | 21.0 | 5.2 | 4.0 | 10.0 | 19.4 | 18.5 | 16.0 | 14.0 | 8.6 | a↓(2) |
| South Africa | 36.7 | 45.1 | 21.0 | 2.2 | 15.0 | 35.3 | 40.4 | 39.9 | 34.3 | 45.8 | ↑(6) |
| Mongolia | 7.8 | 11.9 | 3.0 | 3.9 | 6.7 | 4.8 | 9.3 | 9.4 | 7.4 | 4.7 | ~(4) |
| Vietnam | 19.3 | 21.2 | 1.1 | 19.6 | 9.1 | 20.7 | 28.8 | 22.3 | 16.8 | 13.1 | ∧(3) |
Note: The bold print means the highest value among all values by age groups. One drink equals to 15ml of ethanol. a – M‐F ratio is a ratio of male estimate/female estimate; b – numbers in the bracket refer to age‐group with the highest value age 1: 16‐19 yr, 2: 20‐24 yr, 3: 35‐44 yr, 4: 45‐54 yr, and 6: 55‐65 yr; Age direction, Monotonic: ↑ monotonic increase with age, ↓ monotonic decrease with age, a↑ or a↓ almost monotonic trend with age, Non‐monotonic: ∧ highest value at middle age, ∨ lowest value at middle age, ~ fluctuation; c – once a week or more, d – 8+ drinks per occasion, e – 6+ drinks on an occasion at least once a week
Drinking patterns by gender
Frequency of drinking in men is higher relative to women. Men have higher percentages of high‐frequency drinking in all countries, as M–F ratios greater than 1. This ratio is high in Vietnam (3.35). In general, the M–F ratio was generally observed to be greater in the middle‐income countries (Table 1).
For typical occasion quantity, percentages of heavier‐typical quantity drinking in men are higher than for women in all countries. The M–F ratio is considerably higher in Vietnam (8.8), followed by Mongolia (4.5), Scotland (4.6) and St Kitts and Nevis (4.2) (Table 1).
For the drinking risk categories, percentages of higher‐risk drinking in men are also higher than for women in all countries. The M–F ratio is very high in Vietnam (19.57) and high in Thailand (4.0) and Mongolia (3.9), all of which are middle‐income countries (Table 1).
Drinking patterns by age groups
Table 1 illustrates that higher percentages of high‐frequency drinking are found in older age groups, in Australia, England, New Zealand and South Africa, most of which are high‐income countries.
Higher percentages of heavier‐typical quantity drinking are found in the younger age groups in four high‐income countries (Australia, England, Scotland and New Zealand) and one middle‐income country (South Africa). A clear monotonic decrease with age is found in the four high‐income countries (Table 1).
For the drinking risk categories, higher percentages of higher‐risk drinking were found in the younger age groups, in particular in the four high‐income countries (Australian, England, Scotland and New Zealand) and one middle‐income country (Thailand). The opposite direction is found in South Africa. Higher percentages of higher‐risk drinkers are found among the middle‐aged groups in Vietnam (Table 1).
Higher‐risk drinking by age groups among men and women
Figure 2 shows gender‐specific higher‐risk drinking across age groups. Among men, percentage of higher‐risk drinking are highest in the second age group (20–24 years) and decline by the older age groups for four high‐income countries (Australia, England, Scotland and New Zealand). This direction is also found among women in Scotland, New Zealand and Thailand.
Figure 2.
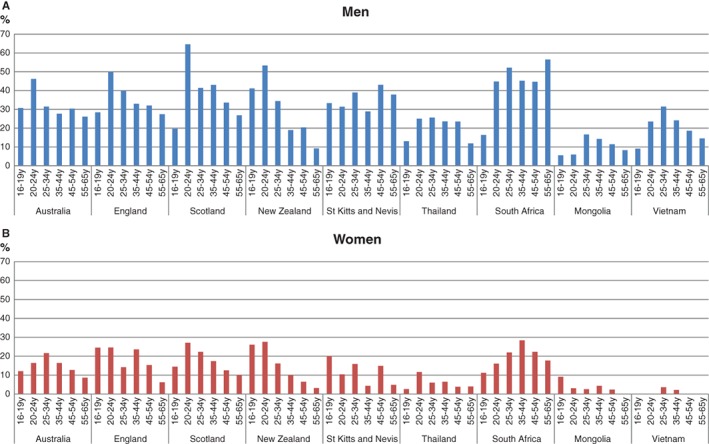
Percentages of higher‐risk drinking by age groups among men (2A) and women (2B) in nine International Alcohol Control study countries.
Note: Higher‐risk drinking is defined as more than six drinks on an occasion at least once a week. There are small numbers of female drinkers in Mongolia and Vietnam.
Associations between drinking patterns and gender, age and country‐level income
Logistic regression analysis revealed that being male is a strong predictor for the high‐frequency, heavier‐typical quantity and higher‐risk drinking categories. Age is also a significant predictor of high‐frequency drinking, with greater odds ratios in older groups compared with the youngest group. For heavier‐typical quantity drinking, middle‐and older age groups had lower odds relative to the youngest group. With respect to higher‐risk drinking, relative to the youngest age group, the young‐middle age groups had higher odds whereas the oldest group had lower odds (Table 2). Country‐level income also predicted drinking patterns—high‐income predicted high‐frequency and higher‐risk drinking, whereas middle‐income predicted heavier‐typical quantity drinking.
Table 2.
Associations between drinking patterns and gender, age and country‐income levela
| High‐frequency drinking | Heavier‐typical quantity drinking | Higher‐risk drinking | |
|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Gender | |||
| Female | 1 (reference) | 1 (reference) | 1 (reference) |
| Male | 3.05 (2.66, 3.50)*** | 2.91 (2.45, 3.46)*** | 3.22 (2.76, 3.75)*** |
| Age group | |||
| 16–19 years | 1 (reference) | 1 (reference) | 1 (reference) |
| 20–24 years | 2.21 (1.69, 2.88)*** | 1.05 (0.76, 1.45) | 1.76 (1.32, 2.35)*** |
| 25–34 years | 2.48 (1.97, 3.12)*** | 0.80 (0.60, 1.06) | 1.42 (1.10, 1.84)** |
| 34–44 years | 2.64 (2.08, 3.36)*** | 0.55 (0.40, 0.76)*** | 1.09 (0.83, 1.44) |
| 45–54 years | 2.84 (2.26, 3.56)*** | 0.45 (0.33, 0.61)*** | 0.93 (0.70, 1.22) |
| 55–65 years | 2.82 (2.17, 3.66)*** | 0.27 (0.19, 0.40)*** | 0.64 (0.46, 0.89)** |
| Country‐income level | |||
| Middle income | 1 (reference) | 1 (reference) | 1 (reference) |
| High income | 4.92 (4.02, 6.02)*** | 0.70 (0.54, 0.91)** | 1.70 (1.22, 2.37)** |
Note: *P < 0.05, **P < 0.01, ***P < 0.001.
Multiple logistic regression analyses for high‐frequency drinking (once a week or more), heavier‐typical quantity drinking (more than eight drinks per occasion) and higher‐risk drinking (more than six drinks on an occasion at least once a week).
OR, odds ratio; CI, confidence interval.
Discussion
The study purpose was to investigate drinking patterns by gender and age in a range of countries differing in income level.
Country‐level income was found to be related to risky drinking. More drinkers in the middle‐income countries reported heavier‐typical quantities with implications for intoxication related harms such as injury, violence and traffic crash. While drinkers in high‐income countries reported lower typical quantities consumed, the frequency of drinking was higher and this resulted in higher proportions of higher‐risk drinkers with the exception of South Africa, a middle‐income country. While, Tshwane district, where the IAC survey was conducted in South Africa, is mostly urban, at least 80%, and consumption is higher in urban areas 23, the high levels of heavy drinking found are still in keeping with previous data reporting high levels of consumption among drinkers in South Africa 24 and other research has identified increased availability, corporate targeting, economic development and the weak policy infrastructures for reasons for increasing consumption in this region 25, 26.
For drinking patterns by gender the current study confirms findings previous research 13, in that all drinking patterns in men were higher relative to women both when data from all countries were combined and more generally in the separate country findings, although the size of the gender ratio difference varied. These gender differences tended to be greater in the middle‐income countries for high‐frequency and higher‐risk drinking (with the exception of South Africa). The largest heavier‐typical quantity and higher‐risk gender ratios were found in Vietnam where the vast majority of drinkers in the IAC survey were males and much of the alcohol consumed was non‐commercial 27. Overall, these findings confirm differences in alcohol use between men and women which have been reported in these middle‐income countries 28, 29, 30, 31, 32, 33. It may be that female roles related to alcohol use are closer to male roles in high‐income countries 14, 34, 35. Previous studies indicate that societal level factors have influence on gender difference in alcohol use, and social welfare system, modernisation and women's position in society are strongly associated with heavy drinking particularly in women 35, 36. On the other hand, alcohol use among women is generally lower relative to men in middle‐income countries 28, 29. As women's roles change in middle‐income countries and economies expand the transnational alcohol corporations have actively marketed alcohol to women including the development of products which are targeted at women 4, 28, 30, 31. This observation is important for informing alcohol policy in middle‐income countries, to address increases in women's drinking.
For drinking patterns by age, overall high‐frequency drinking increased with increasing age; from mid‐thirties onwards there was less likelihood of very large quantities being typically consumed; higher risk drinkers were more likely to be in their 20s and 30s; however all of these relationships were more consistently found in the high‐income countries. The high‐income ‘Anglo’ countries of England, Scotland, Australia and New Zealand were characterised by about half of the young men aged 20–24 years reporting higher‐risk drinking. Higher‐risk drinking was lower among men in middle‐income countries with the exception of South Africa where it was more evenly spread across the age groups with the exception of the youngest group.
The strengths and limitations of the current study are as follows. Some advantages over previous studies included the availability of detailed consumption measures asked in the same way across countries and the inclusion of formal comparison of the effect of country‐level income on a range of drinking measures. Validation of the consumption measures used in the current study have been undertaken and it was found that the survey instrument allows for very high coverage of alcohol available for consumption (based on sales or tax data) 37, 38. One limitation was that some samples were sub‐national (South Africa, Mongolia, Vietnam). Other limitations were that different sampling designs and data collection methods (i.e. telephone vs. face to face) were used, and these factors need to be taken into account when interpreting the findings (although sampling design was adjusted for in the analysis). Response rates also varied and were low in some countries (Australia, England and Scotland). This may have affected the distribution of age and/or age by gender distributions and drinking patterns in some countries, for example, the percentages of high‐quantity drinkers in the 20–24‐ and 25–29‐year age groups in England seem low relative to the other high‐income countries. As with all surveys, some of the heaviest drinkers may have been missed.
Conclusion
Men drank more frequently, more typically consumed larger amounts and were more likely to be higher risk drinkers compared with women drinkers. Older age was associated with drinking more frequently but smaller typical quantities but this was seen more consistently in high‐income countries. Middle‐income countries overall showed less frequent and higher typical quantities; however, the lower frequencies meant the percentages of higher risk drinkers were lower overall compared with high‐income countries (with the exception of South Africa). As alcohol use becomes more normalised as a result of the expansion of commercial alcohol it is likely frequency of drinking will increase with a likelihood of greater numbers drinking at higher risk levels.
Conflict of Interest
The authors have no conflicts of interest.
Acknowledgements
The data used in this paper are from the International Alcohol Control Policy Study, led by Professor Sally Casswell. The IAC core survey questionnaire was largely developed by researchers at SHORE & Whariki Research Centre, College of Health, Massey University, New Zealand, with funding from the Health Promotion Agency, New Zealand. Further development involved collaboration between UK, Thai, Korean and New Zealand researchers. The funding sources for data sets used in this article for each country are: Mongolia—Ministry of Health and World Health Organization office in Mongolia; New Zealand—The Health Promotion Agency (formerly the Alcohol Advisory Council), and the UK Centre for Tobacco and Alcohol Studies; Thailand—International Health Policy Program, Center for Alcohol Studies, and Thai Health Promotion Foundation; England and Scotland—Medical Research Council (MRC) National Prevention Research Initiative; South Africa, St Kitts and Nevis and Vietnam—the International Development Research Centre, Canada; Australia—The Australian National Preventive Health Agency. The research reported in this publication was also supported by the South African Medical Research Council. We thank the project and field staff for their role in data collection for the survey and the data managers in each country. Finally, we express our appreciation to all the participants who gave of their time to take part in this research.
Surasak Chaiyasong PhD, Director, Taisia Huckle PhD, Senior Researcher, Anne‐Marie Mackintosh BSc Hons, Senior Researcher, Petra Meier PhD, Director, Charles D. H. Parry PhD, Director, Sarah Callinan PhD, Research Fellow, Pham Viet Cuong PhD, Director, Elena Kazantseva PhD, Researcher, Gaile Gray‐Phillip PhD, Dean, Karl Parker MSc, Statistician and Sally Casswell PhD, Director.
Reference
- 1. GBD 2016 Risk Factors Collaborators . Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990‐2016: a systematic analysis for the global burden of disease study 2016. Lancet 2017;390:1345–422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Babor T, Caetano R, Casswell S et al Alcohol: no ordinary commodity research and public policy, 2nd edn. Oxford: Oxford University Press, 2010. [Google Scholar]
- 3. World Health Organization . Global status report on alcohol and health. World Health Organization: Geneva, 2014. [Google Scholar]
- 4. Room R, Jernigan D, Carlini‐Marlatt B et al Alcohol and the development world: a public health perspective. Helsinki: Finish Fondation for Alcohol Studies, 2002. [Google Scholar]
- 5. Astudillo M, Kuntsche S, Graham K, Gmel G. The influence of drinking pattern, at individual and aggregate levels, on alcohol‐related negative consequences. Eur Addict Res 2010;16:115–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Bye EK, Rossow I. The impact of drinking pattern on alcohol‐related violence among adolescents: an international comparative analysis. Drug Alcohol Rev 2010;29:131–7. [DOI] [PubMed] [Google Scholar]
- 7. Antai D, Lopez GB, Antai J, Anthony DS. Alcohol drinking patterns and differences in alcohol‐related harm: a population‐based study of the United States. Biomed Res Int 2014;853410:25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Huckle T, Pledger M, Casswell S. Increases in typical quantities consumed and alcohol‐related problems during a decade of liberalizing alcohol policy. J Stud Alcohol Drugs 2012;73:53–62. [DOI] [PubMed] [Google Scholar]
- 9. Martineau F, Tyner E, Lorenc T, Petticrew M, Lock K. Population‐level interventions to reduce alcohol‐related harm: an overview of systematic reviews. Prev Med 2013;57:278–96. [DOI] [PubMed] [Google Scholar]
- 10. Kuntsche E, Rehm J, Gmel G. Characteristics of binge drinkers in Europe. Soc Sci Med 2004;59:113–27. [DOI] [PubMed] [Google Scholar]
- 11. Livingston M, Room R. Variations by age and sex in alcohol‐related problematic behaviour per drinking volume and heavier drinking occasion. Drug Alcohol Depend 2009;101:169–75. [DOI] [PubMed] [Google Scholar]
- 12. Chan KK, Neighbors C, Gilson M, Larimer ME, Alan Marlatt G. Epidemiological trends in drinking by age and gender: providing normative feedback to adults. Addict Behav 2007;32:967–76. [DOI] [PubMed] [Google Scholar]
- 13. Wilsnack RW, Wilsnack SC, Kristjanson AF, Vogeltanz‐Holm ND, Gmel G. Gender and alcohol consumption: patterns from the multinational GENACIS project. Addiction 2009;104:1487–500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Kerr‐Correa F, Igami TZ, Hiroce V, Tucci AM. Patterns of alcohol use between genders: a cross‐cultural evaluation. J Affect Disord 2007;102:265–75. [DOI] [PubMed] [Google Scholar]
- 15. Casswell S, Meier P, MacKintosh AM et al The International Alcohol Control (IAC) study‐evaluating the impact of alcohol policies. Alcohol Clin Exp Res 2012;36:1462–7. [DOI] [PubMed] [Google Scholar]
- 16. Casswell S, Morojele N, Williams PP et al The Alcohol Environment Protocol: A new tool for alcohol policy. Drug Alcohol Rev 2018;37:S18–S26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Casswell S, Huckle T, Wall M, Yeh LC. International alcohol control study: pricing data and hours of purchase predict heavier drinking. Alcohol Clin Exp Res 2014;38:1425–31. [DOI] [PubMed] [Google Scholar]
- 18. Livingston M, Callinan S. Underreporting in alcohol surveys: whose drinking is underestimated? J Stud Alcohol Drugs 2015;76:158–64. [PubMed] [Google Scholar]
- 19. World Bank . Country classification: World Bank list of economies [database on the Internet]. 2017. Available at: https://datahelpdesk.worldbank.org/knowledgebase/topics/19280-country-classification (accessed 10 November 2017).
- 20. Huckle T, Casswell S, Mackintosh AM et al The International Alcohol Control study: Methodology and implementation. Drug Alcohol Rev 2018;37:S10–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Kaminska O, Lynn P. Survey‐based cross‐country comparisons where countries vary in sample design: issues and solutions. J Off Stat 2017;33:123–36. [Google Scholar]
- 22. StataCorp . Stata statistical software: release 14. College Station: StataCorp LP, 2015. [Google Scholar]
- 23. National Department of Health (NDoH) , Statistics South Africa (Stats SA) , South African Medical Research Council (SAMRC) , ICF . South Africa demographic and health survey 2016: key indicators report. Pretoria and Rockville: NDoH, Stats SA, SAMRC, and ICF, 2017. [Google Scholar]
- 24. Global Information System on Alcohol and Health (GISAH) : Level of Consumption [database on the Internet]. World Health Organization, 2015 [cited 28 September 2017]. Available from: http://apps.who.int/gho/data/node.gisah.A1028?lang=en&showonly=GISAH.
- 25. Ferreira‐Borges C, Dias S, Babor T, Esser MB, Parry CD. Alcohol and public health in Africa: can we prevent alcohol‐related harm from increasing? Addiction. 2015;110:1373–9. [DOI] [PubMed] [Google Scholar]
- 26. Ferreira‐Borges C, Rehm J, Dias S, Babor T, Parry CD. The impact of alcohol consumption on African people in 2012: an analysis of burden of disease. Trop Med Int Health. 2016;21:52–60. [DOI] [PubMed] [Google Scholar]
- 27. Parry CDH, Londani M, Enkhtuya P et al Support for alcohol policies among drinkers in Mongolia, New Zealand, Peru, South Africa, St Kitts and Nevis, Thailand and Vietnam: Data from the International Alcohol Control Study. Drug Alcohol Rev 2018;37:S72–S85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Demaio AR, Dugee O, de Courten M, Bygbjerg IC, Enkhtuya P, Meyrowitsch DW. Exploring knowledge, attitudes, and practices related to alcohol in Mongolia: a national population‐based survey. BMC Public Health 2013;13:1471–2458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Lincoln M. Alcohol and drinking cultures in Vietnam: a review. Drug Alcohol Depend 2016;159:1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Parry CD. South Africa: alcohol today. Addiction 2005;100:426–9. [DOI] [PubMed] [Google Scholar]
- 31. Thamarangsi T. Thailand: alcohol today. Addiction 2006;101:783–7. [DOI] [PubMed] [Google Scholar]
- 32. Assanangkornchai S, Sam‐Angsri N, Rerngpongpan S, Lertnakorn A. Patterns of alcohol consumption in the Thai population: results of the National Household Survey of 2007. Alcohol Alcohol 2010;45:278–85. [DOI] [PubMed] [Google Scholar]
- 33. Van Bui T, Blizzard CL, Luong KN et al Alcohol consumption in Vietnam, and the use of 'standard drinks' to measure alcohol intake. Alcohol Alcohol 2016;51:186–95. [DOI] [PubMed] [Google Scholar]
- 34. Holmila M, Raitasalo K. Gender differences in drinking: why do they still exist? Addiction 2005;100:1763–9. [DOI] [PubMed] [Google Scholar]
- 35. Rahav G, Wilsnack R, Bloomfield K, Gmel G, Kuntsche S. The influence of societal level factors on men's and women's alcohol consumption and alcohol problems. Alcohol Alcohol Suppl 2006;41:i47–55. [DOI] [PubMed] [Google Scholar]
- 36. Kuntsche S, Gmel G, Knibbe RA et al Gender and cultural differences in the association between family roles, social stratification, and alcohol use: a European cross‐cultural analysis. Alcohol Alcohol Suppl 2006;41:i37–46. [DOI] [PubMed] [Google Scholar]
- 37. Casswell S, Huckle T, Pledger M. Survey data need not underestimate alcohol consumption. Alcohol Clin Exp Res 2002;26:1561–7. [DOI] [PubMed] [Google Scholar]
- 38. Livingston M, Callinan S. Under‐reporting in alcohol surveys: whose drinking is under‐estimated? J Stud Alcohol Drugs 2015;76:158–64. [PubMed] [Google Scholar]