

Abstract
Objective
To determine the long-term impact of sudden parental death on youth and pathways between bereavement and impairment.
Method
216 youths who lost a parent to suicide, accident, or sudden natural death and 172 non-bereaved youth were followed periodically for up to 7 years. The incidence and prevalence of disorder and of functional impairment, and pathways to impairment were assessed using Cox and mixed effects logistic regression and Structural Equation Modeling (SEM).
Results
Prior to parental death, bereaved youth had higher rates of psychiatric disorder, parental psychiatric disorder, and maltreatment. Even after adjustment for pre-death risk factors, bereavement was associated with an increased incidence of depression, post-traumatic stress disorder (PTSD), and functional impairment. The peak incidence of depression was in the first two years post-bereavement, with incident depression occurring mainly in those who lost a parent prior to age 12. Youth bereaved by all three causes of death showed higher rate of impairment at all timepoints. SEM found that bereavement had a direct effect on impairment, and was linked to impairment via its impact on early and later depression, and through negative life events. Child psychiatric disorder prior to parental loss also contributed to functional impairment.
Conclusion
Parental death increased the incidence of depression in offspring early in the course of bereavement. Early identification and treatment of depression in bereaved youth and augmentation of family resilience may protect against later sequelae of functional impairment.
Introduction
The loss of a parent is one of the most stressful events that a child can experience.1 There is less clarity about the short and longer-term sequelae of parental bereavement. Reports of enduring effects of parental bereavement are often based on current assessments of adults who report a history of parental death. In contrast, longitudinal studies have usually been limited to the first two years post-bereavement, so that the longer-term effects of parental bereavement and the mechanisms linking bereavement and later outcomes are not well understood.
Adults who were parentally bereaved as children report increased depressive symptoms, diminished self-confidence, educational under attainment, and dissatisfaction with their interpersonal relationships.1–3 However, these studies did not adjust for risk factors for impairment that antedated the death of the parent and are more common in bereaved families, such as parental or personal psychopathology.4,5
Longitudinal studies of parentally bereaved youth have found an increased risk for psychopathology up to 2 years after parental death, even after adjusting for pre-death risk factors.4–7 Youth who lost a parent to a natural disaster have reported long-lasting sequelae of depression and post-traumatic stress disorders (PTSD),8 although these findings may also be attributable to the effects of dislocation and loss of a home.1,8 Registry studies of parental bereavement find a peak incidence of adverse outcomes within the first two years, but also report more enduring psychological sequelae.9,10
To address the impact and mechanisms of the sequelae of parental death, we conducted a 7-year longitudinal study of youth whose parents died suddenly and demographically similar non-bereaved controls. We posited, as per extant theoretical models,1 that the loss of a parent increased the risk for psychiatric disorder and functional impairment in children through three inter-related pathways: (1) children of parents who die prematurely are already at higher risk than their non-bereaved peers due to pre-existing vulnerability prior to the death, namely, personal and family history of psychopathology and exposure to adversity; (2) parental loss decreases family resources that protect children from the effects of other negative events, due to functional impairment and psychiatric disorder in the surviving parent; and (3) as a result of (1) and (2), youth develop maladaptive coping styles and experience an increased risk of new-onset psychopathology that in turn results in functional impairment over time.
In previous reports, we found deceased parents, who were middle-aged and as such died prematurely, had higher rates of psychiatric disorders compared to controls.4 Parentally-bereaved youth had an increased incidence of depression and PTSD 9 months after parental death, even controlling for pre-death risk factors.4 Bereaved offspring had a higher rate of depression nearly 2 years post-death, mediated by higher rates of incident depression 9 months after the loss; enduring depression was more common in those bereaved offspring who had a previous history of depression, increased exposure to negative life events, and had had lost a mother rather than a father.6 Five years post-death, bereaved offspring showed attenuated developmental competence in work, career planning, and relationships, mediated by family climate and functional impairment in both the surviving parent and the child.11 Herein, we report on a 7-year follow-up of this cohort to determine transient and enduring sequelae of parental bereavement compared to controls, inquiring about: (1) the peak incidence and subsequent course of depression, PTSD, and other conditions; (2) the incidence and course of functional impairment; and (3) the pathways by which bereavement leads to enduring impairment.
Method
Participant recruitment
Adults who died by suicide, accident, or sudden natural death and had at least one biological child between the ages of 7-18 were identified through the medical examiner’s reports (45.1%) or via newspaper reports (54.9%). The parental death needed to have occurred within 24 hours of the initial incident, and families with multiple deaths or injuries were excluded. Of those who were eligible, 71% consented to participate.
Living, non-bereaved parents were recruited by random-digit dialing or by newspaper advertisements and one of the parents was frequency-matched to the deceased parents by neighborhood, age, and gender, with a participation rate of 55%. Control offspring could not have had a death in a first- or second-degree relative within the past two years.
This study was approved by the University of Pittsburgh Institutional Review Board. All participants in the study gave written consent or assent.
Assessments
Participants were interviewed at 9, 21, 33, 62, and 84 months after the death by experienced clinical interviewers, with interviews for offspring and parents conducted blind to one another. Retrospective assessment was used to determine if the offspring’s and surviving parent’s disorders had their onset before or after parental death. For non-bereaved offspring and their parents, “new-onset disorder” was defined as having occurred within 9 months of the baseline assessment. The equivalent of “pre-death psychiatric disorders” in the non-bereaved offspring and parents was defined as disorders that occurred at least 9 months before the baseline assessment.
Socioeconomic status was assessed using Hollingshead’s scale at intake, and household income at each subsequent assessment.12 The Schedule for Affective Disorders and Schizophrenia for School-Age Children – Present and Lifetime Version13 and the Structured Clinical Interview for DSM-IV Axis I Disorders14 were used for the diagnostic assessment of youth and adults, respectively. Deceased parents’ lifetime disorders were assessed by psychological autopsy.15 Personality disorders in adult participants were assessed with the Structured Interview for DSM–IV Personality Disorders.16 The Longitudinal Interview for Follow-Up Evaluations was used to document the course of disorders in offspring.17 Functional impairment was assessed using the Global Assessment Scale (GAS) for children and adults.18,19 The distribution for the GAS was highly skewed (Shapiro-Wilk W=0.92, p<.001) and as such we used impairment as a dichotomous outcome with a score <70 corresponding to impairment in school, peers, or family domains. High inter-rater reliability was maintained for the assessment of psychiatric diagnoses (κ‘s=0.74-0.85, N=107) and impairment (inter-class correlation=0.92, 95% CI 0.90-0.93, N=734). Additional assessments for youth and adults for symptomatology, suicidal ideation, aggression, history of maltreatment, life events, coping, social support and family climate are listed in eTable 1.20–35
Data analyses
The incidence of disorders was compared between bereaved and control offspring using Kaplan-Meier survival analysis. Cox proportional hazard models were used to assess the effects of bereavement on incident disorders after controlling for demographic variables and pre-death risk variables. Pre-death risk variables were child and parental psychiatric disorder, and history of physical or sexual abuse that antedated the death. These variables differentiated between bereaved and non-bereaved samples and were related to post-bereavement incident disorder. We tested for interactions of bereavement with demographic and pre-death risk variables, and subsequently conducted stratified analyses when interactions were significant. When the proportional hazards assumption was not met, a time-varying covariate that was an interaction between bereavement and survival time was included. The prevalence of disorders at each timepoint, which includes disorders present since the previous assessment was also compared between bereaved and non-bereaved offspring using the chi-square statistic or Fisher’s exact test. To examine changes in the prevalence of outcomes over time, we used mixed effects logistic regression, adjusting for pre-death risk variables.
For statistical analyses with missing data, we applied multiple imputations by chained equations (MICE). Results using the original and imputed data set were similar, so only the latter are reported in this paper. Analyses were conducted using STATA version 12.1 IC (Stata Corp, College Station, TX.).
Structural Equation Modeling (SEM) in Mplus 8.036 was used to examine the direct and indirect effects of bereavement on impairment 7 years after bereavement. Logistic regression was employed to identify the variables at baseline and follow-up timepoints associated with impairment at 7 years to be included in SEM. We reduced the longitudinal data for the middle 3 timepoints after the baseline assessment by averaging across these three timepoints.
When different measures were used in youth and adults to assess the same domain, scores were z-transformed. To adjust for the effects of having multiple participants from the same family, all multivariate analyses included a term for clustering. Six bereaved and seven controls experienced the death of a family member or close relationship during the study. The findings were the same including or excluding them, so we report the results on the full sample.
Results
Sample description (See Table 1)
Table 1.
Demographic, Clinical and Psychological Characteristics at Intake by Bereavement Status
| Total | Non-Bereaved | Bereaved | Test | df | P | ||||
|---|---|---|---|---|---|---|---|---|---|
| Offspring No. | 388 | 172 | 216 | ||||||
| Mean | SD | Mean | SD | Mean | SD | ||||
| Demographics | |||||||||
| Age at time of parent death (years)* | 12.0 | 3.0 | 12.0 | 2.8 | 12.0 | 3.1 | t=−0.05 | 386 | 0.96 |
| N | % | N | % | N | % | ||||
| Female Sex | 188 | 48.5 | 84 | 48.8 | 104 | 48.1 | χ2=0.02 | 1 | 0.89 |
| White Race | 311 | 80.2 | 144 | 83.7 | 167 | 77.3 | χ2=2.47 | 1 | 0.12 |
| History of Psychiatric Disorders Prior to Death** | |||||||||
| Depression Diagnosis | 42 | 10.9 | 14 | 8.2 | 28 | 13.0 | χ2=2.30 | 1 | 0.13 |
| Bipolar Disorder Diagnosis | 3 | 0.8 | 0 | 0.0 | 3 | 1.4 | Fisher’s | – | 0.26 |
| Anxiety Diagnosis | 33 | 8.5 | 12 | 7.0 | 21 | 9.7 | χ2=0.90 | 1 | 0.34 |
| Post-Traumatic Stress Disorder Diagnosis | 4 | 1.0 | 1 | 0.6 | 3 | 1.4 | Fisher’s | – | 0.63 |
| Attention Deficit Hyperactivity Disorder Diagnosis |
56 | 14.6 | 19 | 11.2 | 37 | 17.2 | χ2=2.78 | 1 | 0.10 |
| Behavior Disorder Diagnosis | 21 | 5.5 | 6 | 3.5 | 15 | 7.0 | χ2=2.19 | 1 | 0.14 |
| Alcohol/Substance Abuse Diagnosis | 4 | 1.0 | 2 | 1.2 | 2 | 0.9 | Fisher’s | – | >0.99 |
| Any Psychiatric History | 111 | 28.8 | 39 | 22.9 | 72 | 33.5 | χ2=5.15 | 1 | 0.02 |
| Physical/Sexual Abuse | 21 | 5.4 | 3 | 1.7 | 18 | 8.3 | χ2=8.12 | 1 | 0.004 |
| Psychiatric Disorders at Baseline | |||||||||
| Depression Diagnosis | 45 | 11.6 | 7 | 4.1 | 38 | 17.6 | χ2=17.08 | 1 | <0.001 |
| Bipolar Disorder Diagnosis | 8 | 2.1 | 2 | 1.2 | 6 | 2.8 | Fisher’s | – | 0.31 |
| Anxiety Diagnosis | 41 | 10.6 | 14 | 8.1 | 27 | 12.5 | χ2=1.93 | 1 | 0.17 |
| Post-Traumatic Stress Disorder Diagnosis | 18 | 4.6 | 0 | 0.0 | 18 | 8.3 | χ2=15.03 | 1 | <0.001 |
| Attention Deficit Hyperactivity Disorder Diagnosis |
53 |
13.7 |
19 |
11.1 |
34 |
15.7 |
χ2=1.79 |
1 |
0.18 |
| Behavior Disorder Diagnosis | 18 | 4.6 | 6 | 3.5 | 12 | 5.6 | χ2=0.92 | 1 | 0.34 |
| Alcohol/Substance Abuse Diagnosis | 2 | 0.5 | 1 | 0.6 | 1 | 0.5 | Fisher’s | – | >0.99 |
| Any Psychiatric History | 116 | 29.9 | 33 | 19.2 | 83 | 38.4 | χ2=16.91 | 1 | <0.001 |
| Mean | SD | Mean | SD | Mean | SD | ||||
| Functioning | 78.6 | 11.8 | 82.2 | 10.1 | 75.7 | 12.2 | t=5.72 | 384.6 | <0.001 |
| Self-Reported Clinical Measures | |||||||||
| Depression z-score | 0.23 | 1.09 | −0.04 | 0.94 | 0.48 | 1.16 | t=−4.64 | 349.5 | <0.001 |
| Anxiety z-score | 0.25 | 1.05 | 0.13 | 0.98 | 0.36 | 1.10 | t=−2.09 | 355.8 | 0.04 |
| Suicidal Ideation | 21.5 | 11.4 | 19.7 | 9.9 | 23.0 | 12.41 | t=−2.75 | 345.8 | 0.01 |
| Impulsive Aggression | 69.6 | 22.4 | 66.6 | 20.4 | 72.2 | 23.9 | t=−2.38 | 354 | 0.02 |
| Post-Traumatic Stress Disorder | 2.98 | 5.86 | 0.47 | 2.22 | 5.72 | 7.23 | z=−11.46 | – | <0.001 |
| Negative Coping Strategies z-score | 0.16 | 1.00 | 0.16 | 0.98 | 0.15 | 1.02 | T=0.12 | 336 | 0.91 |
| Family Climate | 52.7 | 8.9 | 53.8 | 8.3 | 51.7 | 9.3 | t=2.22 | 343 | 0.03 |
| Intercurrent Life Events z-score | 0.82 | 1.15 | 0.55 | 1.00 | 1.03 | 1.21 | t=−4.29 | 383.5 | <0.001 |
| Social Support z-score | −0.05 | 1.02 | 0.11 | 1.00 | −0.18 | 1.02 | t=2.70 | 353 | 0.01 |
| Surviving Caretaking Adult | |||||||||
| No. | 240 | 99 | 141 | ||||||
| M | SD | M | SD | M | SD | ||||
| Demographics | |||||||||
| Age | 43.3 | 7.7 | 42.4 | 6.3 | 43.8 | 8.4 | t=−1.37 | 226 | 0.17 |
| Socio-economic Status | 43.5 | 12.4 | 45.8 | 10.7 | 42.1 | 13.2 | t=1.81 | 154 | 0.07 |
| N | % | N | % | N | % | ||||
| Female Sex | 191 | 81.3 | 75 | 75.8 | 120 | 85.1 | χ2=3.37 | 1 | 0.07 |
| White Race | 203 | 84.6 | 86 | 86.9 | 117 | 83.0 | χ2=0.67 | 1 | 0.41 |
| Spouse or significant other of the deceased | 173 | 75.9 | 80 | 92.0 | 93 | 66.0 | χ2=19.87 | 1 | <0.001 |
| History of Psychiatric Disorders Prior to Death** | |||||||||
| Depression Diagnosis | 99 | 41.4 | 31 | 31.6 | 68 | 48.2 | χ2=6.56 | 1 | 0.01 |
| Bipolar Disorder Diagnosis | 7 | 2.9 | 1 | 1.0 | 6 | 4.3 | Fisher’s | 1 | 0.25 |
| Psychosis Diagnosis | 1 | 0.4 | 1 | 1.0 | 0 | 0.0 | Fisher’s | – | 0.41 |
| Anxiety Diagnosis | 61 | 25.4 | 15 | 15.2 | 46 | 32.6 | χ2=9.37 | 1 | 0.002 |
| Post-Traumatic Stress Disorder Diagnosis | 25 | 10.4 | 9 | 9.1 | 16 | 11.3 | χ2=0.32 | 1 | 0.57 |
| Alcohol/Substance Abuse Diagnosis | 66 | 27.8 | 28 | 28.3 | 38 | 27.5 | χ2=0.02 | 1 | 0.90 |
| Personality Disorder Diagnosis | 8 | 3.3 | 2 | 2.0 | 6 | 4.3 | Fisher’s | – | 0.48 |
| Any Psychiatric History | 150 | 63 | 51 | 52.0 | 99 | 70.7 | χ2=8.63 | 1 | 0.003 |
| Mean | SD | Mean | SD | Mean | SD | ||||
| Current Functioning | 76.8 | 12.2 | 82.0 | 9.2 | 73.6 | 12.7 | t=5.78 | 219.2 | <0.001 |
| Deceased Parent No. | 241 | 98 | 143 | ||||||
| Demographics | |||||||||
| M | SD | M | SD | M | SD | ||||
| Age | 43.9 | 7.7 | 43.4 | 7.0 | 44.3 | 8.2 | t=−0.86 | 239 | 0.39 |
| Socio-economic Status | 43.3 | 13.4 | 46.6 | 11.4 | 41.0 | 14.3 | t=2.67 | 150.02 | 0.01 |
| N | % | N | % | N | % | ||||
| Male Sex | 186 | 77.5 | 74 | 76.3 | 112 | 78.3 | χ2=0.14 | 1 | 0.71 |
| White Race | 199 | 82.9 | 84 | 86.6 | 115 | 80.4 | χ2=1.56 | 1 | 0.21 |
| History of Psychiatric Disorders Prior to Death** | |||||||||
| Depression Diagnosis | 93 | 39.1 | 31 | 32.3 | 62 | 43.7 | χ2=3.11 | 1 | 0.08 |
| Bipolar Disorder Diagnosis | 18 | 7.5 | 2 | 2.0 | 16 | 11.2 | χ2=7.04 | 1 | 0.01 |
| Psychosis Diagnosis | 3 | 1.3 | 0 | 0.0 | 3 | 2.1 | Fisher’s | – | 0.28 |
| Anxiety Diagnosis | 56 | 23.6 | 25 | 26.0 | 31 | 22.0 | χ2=0.52 | 1 | 0.47 |
| PTSD Diagnosis | 23 | 9.6 | 13 | 13.4 | 10 | 7.0 | χ2=2.74 | 1 | 0.10 |
| Alcohol/Substance Abuse Diagnosis | 131 | 54.4 | 43 | 43.9 | 88 | 61.5 | χ2=7.31 | 1 | 0.01 |
| Personality Disorder Diagnosis | 39 | 16.2 | 4 | 4.1 | 35 | 24.5 | χ2=17.83 | 1 | <0.001 |
| Any Psychiatric History | 177 | 73.8 | 66 | 68.0 | 111 | 77.6 | χ2=2.74 | 1 | 0.10 |
Age at time of parental death for bereaved and age at 9 months prior to baseline assessment for non-bereaved;
History of psychiatric disorders prior to death in the bereaved group and lifetime history of psychiatric disorders that occurred prior to 9 months from the baseline assessment in the non-bereaved group.
Participants were 216 offspring from 143 families bereaved by suicide, accident, or sudden natural death, and 172 non-bereaved offspring from 98 families who were 18 years or younger at the time of the parent’s death.
The deceased parents were middle-aged, predominantly male, white, and had died from suicide (N=50), accident (N=35), or sudden natural death (N=58). The causes of sudden natural death were myocardial infarction (n=23), other cardiac conditions (n=21), pneumonia (n=3), and others (n=11) (aneurysm, blood clot, cancer, complications from gastric bypass surgery, diabetes mellitus, infection, stroke). Those bereaved families recruited via medical examiners were less likely to be bereaved by sudden natural death (32.8% vs. 54.7%, χ21=6.34; p=0.01), and to be white (71.7% vs. 86.3%, χ21=4.36; p=0.04), more likely for the surviving parent to have had a history of depression (78.9% vs. 47.6%, χ21=4.18, p=0.04), and more likely for offspring to have been physically or sexually abused prior to the death (23.1% vs. 3.4%, Fisher’s Exact Test, p=0.04).
Deceased parents, compared to their living counterparts, had higher lifetime rates of bipolar (11.2% vs. 2.0%, χ21=7.04, p=0.01), alcohol/substance (61.5% vs. 43.9%, χ21=7.31, p=0.01) and personality disorders (24.5% vs. 4.1%, χ21=17.83; p<0.001). The surviving caretaking adults were middle-aged and predominantly female (81.3%), and compared to their non-bereaved peers, had higher pre-death rates of lifetime depression (48.2% vs. 31.6%, χ21=6.56; p=0.01) and anxiety disorders (32.6% vs. 15.2%, χ21=9.37; p=0.002).
The 68% of offspring who completed the 7-year assessment who completed this assessment were less likely to have been bereaved (60.2% vs. 76.7%, χ21=11.97; p=0.001), black or Hispanic (13.4% vs. 33.3%, χ21=21.34; p<0.001), and to have had a parent with a history of bipolar disorder (3.4% vs. 16.7%, χ21=20.88; p<0.001) (eTable 2), although the median duration of follow-up was similar between bereaved and non-bereaved offspring (6.6 vs. 6.4 years, Wilcoxon rank-sum test χ21=3.10; p=0.08).
Incidence
Bereaved, compared to non-bereaved offspring showed an increased incidence of depression (Incidence Rate Ratio=2.08, 95% Confidence Interval [CI]: 1.45, 3.03), during the first 2 years post-bereavement (Incidence Rate Ratio=3.13, 95% Confidence Interval: 1.89, 5.40), but not thereafter (Incidence Rate Ratio =1.24, 95% Confidence Interval: 0.70, 2.20). Bereavement increased the incidence of depression, even after adjusting for pre-death risk variables (Hazard Ratio=2.55, 95% Confidence Interval: 1.50, 4.33) (See eTable 3 Model 3a). For incident depression, there was a significant interaction between bereavement and the child’s age at the time of parental death (Hazard Ratio=0.85, 95% Confidence Interval: 0.75, 0.97) (See eTable 3 Model 3b). The adjusted Hazard Ratio for incident depression was increased in offspring who lost a parent prior to age 12 (Hazard Ratio=4.92, 95% Confidence Interval 2.04, 11.87), but not in those who lost a parent during adolescence (Hazard Ratio=1.15, 95% Confidence Interval 0.69, 1.90) (see eTable 3 Models 3c and 3d, and Figure 1). Relative to controls, there was a significantly increased incidence of depression in offspring whose parents died by suicide (Hazard Ratio=2.26, 95% CI: 1.39-3.66), and by sudden natural death (Hazard Ratio=2.19, 95% CI: 1.26-3.83), but not in offspring bereaved by accidental death (Hazard Ratio=1.59, 95% Confidence Interval: 0.88, 2.85).
Figure 1.
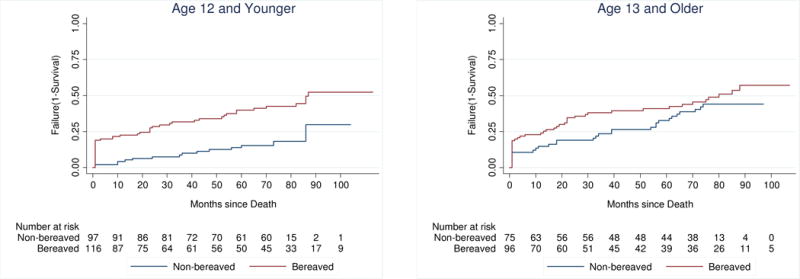
Kaplan-Meier Curves for Incident Depression by Offspring’s Age at Parent’s Death
Bereaved offspring showed an increased incidence of PTSD (Incidence Rate Ratio=7.27, 95% Confidence Interval: 2.58, 28.29) (See Figure 2), which was increased in the first 2 years after the loss (Incidence Rate Ratio=10.41, 95% Confidence Interval: 2.57, 91.10), with a non-significant trend thereafter (Incidence Rate Ratio=4.14, 95% Confidence Interval: 0.86, 39.34). Bereavement increased the incidence of PTSD, even after adjusting for pre-death risk variables (adjusted Hazard Ratio=5.66, 95% Confidence Interval: 1.95, 16.40) (See eTable 4). Relative to controls, those bereaved by suicide (Hazard Ratio=2.25, 95% Confidence Interval: 1.41-3.57) and sudden natural death (Hazard Ratio=2.18, 95% Confidence Interval: 1.25, 3.79) showed elevated hazard ratios, but offspring bereaved by accidental death did not (Hazard Ratio=1.62, 95% Confidence Interval: 0.90, 2.92).
Figure 2.
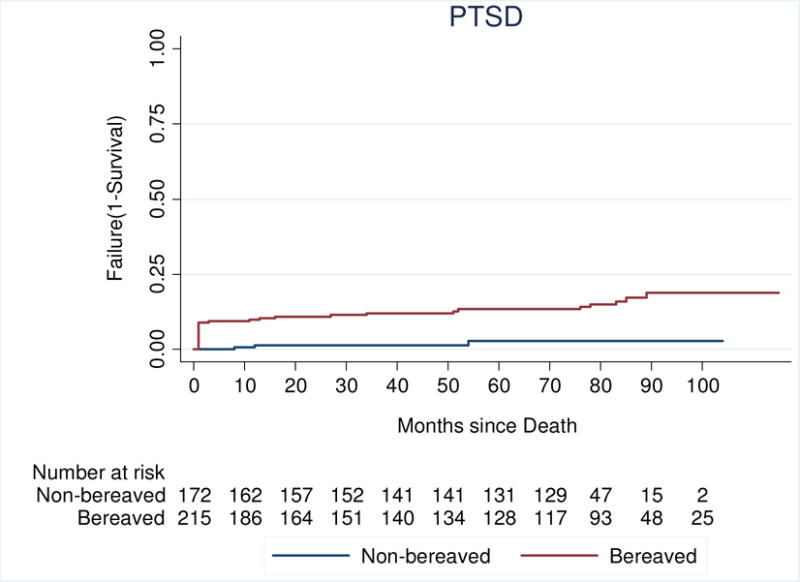
Kaplan-Meier Curves for Incident PTSD
Bereaved offspring showed a higher incidence of clinically significant suicidal ideation (defined as a Suicidal Ideation Questionnaire score ≥31; Incidence Rate Ratio=1.89, 95% Confidence Interval: 1.20, 3.03) (see Figure 3). Bereavement showed a trend towards increased ideation in both the first 24 months (Incidence Rate Ratio=1.72, 95% Confidence Interval: 0.96, 3.19), and thereafter (Incidence Rate Ratio=2.18, 95% Confidence Interval: 1.04, 4.92). The effect of bereavement on ideation became non-significant after controlling for pre-death risk variables (See eTable 5).
Figure 3.

Kaplan-Meier Curves for Incident Clinically Significant Suicidal Ideation
There were no significant effects of bereavement on the incidence of anxiety (Hazard Ratio=1.44, 95% Confidence Interval: 0.86, 2.40), alcohol and drug abuse (Hazard Ratio=0.97, 95% Confidence Interval: 0.55, 1.69), bipolar disorder (Hazard Ratio=1.34, 95% Confidence Interval: 0.45, 3.99), or behavioral disorders (conduct disorder, oppositional defiant disorder) (Hazard Ratio=1.02, 95% Confidence Interval: 0.48, 2.15).
Prevalence
The prevalence of psychiatric disorders and suicidal ideation were compared between bereaved and non-bereaved offspring at each time point (Figure 4). While bereaved offspring showed an increased prevalence of depression at early time points, mixed effects logistic regression showed that over time, the rates of depression in the bereaved and non-bereaved offspring converged (bereavement by time interaction, Odds Ratio=0.62, 95% Confidence Interval: 0.48, 0.81, p<0.001, see eTable 6). The prevalence of clinically significant suicidal ideation was elevated in bereaved offspring at four out of five timepoints, including the 7 years assessment, but the increased prevalence in bereaved offspring was accounted for by greater loading of pre-death risk variables. In contradiction to earlier findings, the sex of the deceased parent did not affect the prevalence of depression or other disorders at 7 years (p’s>0.27).4
Figure 4.
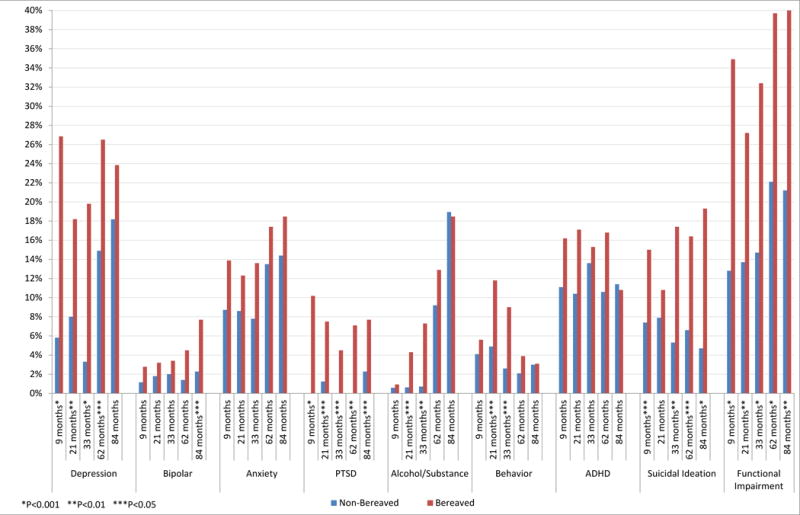
Prevalence of Disorders and Impairment in Bereaved and non-Bereaved Youth between Assessment Points
Incidence and course of impairment
Bereaved, compared to non-bereaved offspring had an increased incidence of impairment (Incidence Rate Ratio=2.93, 95% Confidence Interval: 2.10, 4.14), even after adjusting for demographic and pre-death risk variables (Hazard Ratio=2.07, 95% Confidence Interval: 1.43, 2.99) (Table 2 and eFigure 1). Incident bereavement-related impairment was increased over the first two years (Incidence Rate Ratio=2.63, 95% Confidence Interval: 1.72, 4.13), as well as thereafter (Incidence Rate Ratio=2.56, 95% Confidence Interval: 1.47, 4.61), and was increased in all three types of parental death: (suicide: Hazard Ratio=1.69, 95% Confidence Interval: 1.05, 2.74; accident: Hazard Ratio=1.73, 95% Confidence Interval: 1.10, 2.72; sudden natural death: Hazard Ratio=2.71, 95% Confidence Interval: 1.78, 4.14). Mixed effects logistic regression showed that the prevalence of impairment was consistently increased in bereaved offspring (Odds Ratio=6.60, 95% Confidence Interval: 2.66-16.32; p<0.001), with no change in this relationship over time (non-significant bereavement by time interaction, p=0.23).
Table 2.
Incident Impaired Level of Functioning by Bereavement Status after Controlling for Covariates
| Hazard Ratio | 95% Confidence Interval |
t | P | |
|---|---|---|---|---|
| Bereavement | 2.07 | 1.43, 2.99 | 3.89 | <0.001 |
| Age at Parent’s Death | 0.95 | 0.90, 0.99 | −2.19 | 0.03 |
| Female Sex | 1.34 | 0.98, 1.82 | 1.85 | 0.06 |
| White Race | 0.59 | 0.40, 0.88 | −2.57 | 0.01 |
| Socio-economic Status | 0.99 | 0.98, 1.01 | −0.94 | 0.35 |
| History of Psychiatric Disorder (offspring) | 4.02 | 2.86, 5.66 | 7.97 | <0.001 |
| History of Psychiatric Disorder (parent) | 1.17 | 0.71, 1.94 | 0.62 | 0.54 |
| Physical/Sexual Abuse | 1.48 | 0.93, 2.36 | 1.64 | 0.10 |
Pathways for the relationship between bereavement and impairment
Logistic regression identified the most parsimonious set of variables at baseline and the average score at the next three time points associated with impairment at 7 years (see eTable 7), which were used to fit a Structural Equation Model (See Figure 5).
Figure 5.
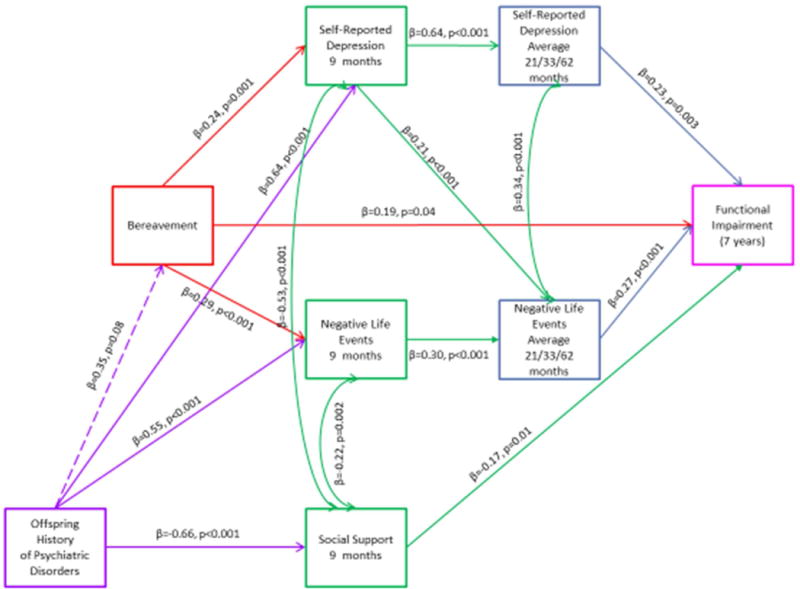
Path Analysis of Functional Impairment (Average of Intermediate Time Points)
There was a significant direct effect of bereavement on impairment (standardized coefficient [β]=0.19, standard error=0.09, p=0.04). The indirect effects of bereavement on impairment were mediated by: (1) self-reported depression at 9 months, and the average of self-reported depression over the next 3 time points (β=0.04, standard error=0.02, p=0.02); (2) negative life events at 9 months and the average over the next 3 time points (β=0.03 standard error=0.01, p=0.02); and (3) self-reported depression at 9 months, and the average of negative life events over the next 3 time points (β=0.02, standard error=0.01, p=0.03). A history of pre-death child psychiatric disorder was more common in bereaved offspring, and showed indirect pathways to impairment via its impact on self-reported depression (β=0.11, standard error=0.04, p=0.01), social support (β=0.13, standard error=0.06, p=0.02), negative life events (β=0.05, standard error=0.02, p=0.02), as well as through self-reported depression at 9 months and the average negative life events over the next 3 time points (β=0.04, standard error=0.02, p=0.01). This model showed a good fit to the data (Test of model fit: χ210=12.61, P=0.25; Comparative Fit Index=0.994; Tucker-Lewis Index=0.970; Weighted Root Mean Square Residual=0.37; Root Mean Square Error of Approximation=0.03, 90% CI: 0-0.08).
Discussion
In this 7-year controlled follow-up study, parentally-bereaved offspring showed an increased incidence of depression and PTSD. The increased incidence of depression occurred mainly in the first two years after parental death and in youth whose parents died when they were younger than age 12. Bereavement had a direct effect on impairment and was linked to impairment through its impact on earlier depression and continued depression in offspring at subsequent timepoints, and via its impact on negative life events. Pre-death psychiatric disorder in offspring was also related to impairment via its effects on social support, negative life events, and depression.
This study has several unique strengths. Both parents and children were carefully assessed for factors antecedent and subsequent to the death. Psychiatric disorder was also assessed in the deceased parent. The 7-year follow-up is considerably longer than most comparable longitudinal studies, and the multiple time points provide a detailed view of the unfolding sequelae of bereavement over time.1,5,7 The sample of youth bereaved by suicide and accidents are likely representative, given their high acceptance rate and demographic similarities to accidents and suicides in the region. Limitations include sample size, which while large for a longitudinal study, precludes a definitive assessment of the impact of differing causes of parental death. It is difficult to determine the representativeness of the cases of sudden natural death because they were not routinely referred to medical examiners. While those cases obtained via advertising had lower family loading for psychopathology and abuse, the effects of bereavement appeared to be similar regardless of referral source.
Our finding of an increased incidence of depression early in the course of bereavement is consistent with other studies, as is the result that younger children are more vulnerable to the negative sequelae of parental bereavement.9,10 The incidence pattern for PTSD was more ambiguous, but was consistent with other work showing a long-lasting vulnerability to incident PTSD after a traumatic event.37
The loss of a parent conveyed an early and enduring negative impact on offspring’s functioning, in part mediated by the onset of depression beginning early in the course of bereavement. The deleterious impact of early depression on later functioning occurred despite the convergence of rates of depression in the bereaved and non-bereaved offspring over time, with similar findings in prevention trials showing long-term functional sequelae of early-onset depression.38
There were increased rates of clinically significant suicidal ideation at nearly all timepoints in the bereaved vs. non-bereaved offspring, consistent with other reports findings that parental bereavement was associated with an increased risk for suicidal behavior.9,10 While it appears that antecedent risk factors associated with bereavement, rather than bereavement per se increased the risk of suicidal ideation in bereaved youth, clinicians should be aware that individuals parentally bereaved youth are at increased risk for clinically significant suicidal ideation.
These findings serve as a reminder that parents with psychiatric disorder are at increased risk for premature death.4 Better identification and treatment of parental psychiatric disorder, and attendance to the increased comorbid medical problems associated with mood disorders, such as cardiovascular disease, could help to prevent premature death in parents and hence protect families from the sequelae of parental bereavement.39
These findings partially support the conceptual model outlined in the introduction of the paper, in which pre-death risk factors, post-bereavement child disorder, and erosion of familial social support contribute to enduring impairment, along with the impact of negative life events. While offspring coping was related to impairment in univariate analyses, this variable did not survive logistic regression and hence did not play a role in our path analysis. Our model was influenced by that developed for The Family Bereavement Program (FBP), a preventive intervention for families that have lost a parent. In their model, parental bereavement negatively impacted children’s adaptive coping and the surviving parents’ ability to provide consistent discipline and maintain a positive relationship with the child.1,40 FBP offers parallel group sessions for children that teaches optimal coping responses and for parents to promote consistent discipline, augmenting parent-child relationships, and encouraging, as appropriate, children’s expression of grief.40 Youth whose families were assigned to FBP experienced both fewer events and a diminished impact of negative life events when they occurred.40 FBP protected bereaved children from negative sequelae via the promotion of adaptive coping and through the augmentation of the parent-child relationship.1,40
This study supports improved detection and management of parental psychiatric disorder and comorbid medical conditions in order to prevent the sequelae of parental bereavement. These findings also highlight the importance of careful monitoring, early identification and treatment of psychiatric disorder in bereaved children and the surviving parent, assessment of family psychiatric and environmental risk factors, and augmentation of family resilience through promotion of positive parenting. These steps in early identification and intervention can attenuate the impact of parental loss and help these youths to become functional adults, despite the burden of bereavement.
Supplementary Material
β’s are standardized coefficients. Model controls for age, sex, and race
Test of model fit: χ210=12.61, P=0.25. Comparative Fit Index [CFI]=0.994. Tucker-Lewis Index [TLI]=0.970. Weighted Root Mean Square Residual [WRMR]=0.37. Root Mean Square Error of Approximation [RMSEA]=0.03, 90% CI: 0-0.08.
The indirect effects of bereavement were mediated via:
Self-reported depression at 9 months and the average self-reported depression (21/33/62 months): β=0.04, SE=0.02, p=0.02
Self-reported depression at 9 months and the average negative life events (21/33/62 months): β=0.02, SE=0.01, p=0.03
Negative life events at 9 months and the average negative life events (21/33/62 months): β=0.03, SE=0.01, p=0.02
The indirect effects of offspring history of psychiatric disorder were mediated via:
Social support at 9 months: β=0.13, SE=0.06, p=0.02
Self-reported depression at 9 months and the average self-reported depression (21/33/62 months): β=0.11, SE=0.04, p=0.01
Self-reported depression at 9 months and the average negative life events (21/33/62 months): β=0.04, SE=0.02, p=0.01
Negative life events at 9 months and the average negative life events (21/33/62 months): β=0.05, SE=0.02, p=0.02
Acknowledgments
We gratefully acknowledge John T. Chen, PhD, for his statistical assistance, and the editorial assistance of Mr. Joseph Park. Most importantly, we express our gratitude to our participants, who made this study possible.
Funding/Support
This study was supported by grants MH065368 (Brent) and MH018951 (Pham) from the National Institute of Mental Health, a Young Investigator Award from the American Foundation for Suicide Prevention (Melhem), and the University of Pittsburgh Clinical Scientist Training Program from the Clinical and Translation Science Institute grant UL1TR001857 (Pham).
Footnotes
Financial Disclosure
Dr. Brent receives royalties from Guilford Press, has or will receive royalties from the electronic self-rated version of the C-SSRS from eResearch Technology, Inc., is on the editorial board of UpToDate, and is a reviewer for Healthwise and a consultant for McKeeson. No other disclosures were reported.
References
- 1.Luecken LJ, Roubinov DS. Pathways to lifespan health following childhood parental death. Soc Personal Psychol Compass. 2012;6(3):243–257. doi: 10.1111/j.1751-9004.2011.00422.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mack KY. Childhood family disruptions and adult well-being: The differential effects of divorce and parental death. Death Stud. 2001;25(5):419–443. doi: 10.1080/074811801750257527. [DOI] [PubMed] [Google Scholar]
- 3.Cas AG, Frankenberg E, Suriastini W, Thomas D. The impact of parental death on child well-being: Evidence from the Indian Ocean tsunami. Demography. 2014;51(2):437–457. doi: 10.1007/s13524-014-0279-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Melhem NM, Walker M, Moritz G, Brent DA. Antecedents and sequelae of sudden parental death in offspring and surviving caregivers. Arch Pediatr Adolesc Med. 2008;162(5):403–410. doi: 10.1001/archpedi.162.5.403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kaplow JB, Saunders J, Angold A, Costello EJ. Psychiatric symptoms in bereaved versus nonbereaved youth and young adults: A longitudinal epidemiological study. J Am Acad Child Adolesc Psychiatry. 2010;49(11):1145–1154. doi: 10.1016/j.jaac.2010.08.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Brent D, Melhem N, Donohoe MB, Walker M. The incidence and course of depression in bereaved youth 21 months after the loss of a parent to suicide, accident, or sudden natural death. Am J Psychiatry. 2009;166(7):786–794. doi: 10.1176/appi.ajp.2009.08081244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Cerel J, Fristad MA, Verducci J, Weller RA, Weller EB. Childhood bereavement: Psychopathology in the 2 years postparental death. J Am Acad Child Adolesc Psychiatry. 2006;45(6):681–690. doi: 10.1097/01.chi.0000215327.58799.05. [DOI] [PubMed] [Google Scholar]
- 8.Goenjian AK, Walling D, Steinberg AM, Roussos A, Goenjian HA, Pynoos RS. Depression and PTSD symptoms among bereaved adolescents 6(1/2) years after the 1988 Spitak earthquake. J Affect Disord. 2009;112(1–3):81–84. doi: 10.1016/j.jad.2008.04.006. [DOI] [PubMed] [Google Scholar]
- 9.Berg L, Rostila M, Hjern A. Parental death during childhood and depression in young adults - a national cohort study. J Child Psychol Psychiatry. 2016;57(9):1092–1098. doi: 10.1111/jcpp.12560. [DOI] [PubMed] [Google Scholar]
- 10.Wilcox HC, Kuramoto SJ, Lichtenstein P, Langstrom N, Brent DA, Runeson B. Psychiatric morbidity, violent crime, and suicide among children and adolescents exposed to parental death. J Am Acad Child Adolesc Psychiatry. 2010;49(5):514–523. doi: 10.1097/00004583-201005000-00012. quiz 530. [DOI] [PubMed] [Google Scholar]
- 11.Brent DA, Melhem NM, Masten AS, Porta G, Payne MW. Longitudinal effects of parental bereavement on adolescent developmental competence. J Clin Child Adolesc Psychol. 2012;41(6):778–791. doi: 10.1080/15374416.2012.717871. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hollingshead A. Four Factor Index of Social Status. New Haven, CT: Yale University; 1975. [Google Scholar]
- 13.Kaufman J, Birmaher B, Brent D, Rao U, Flynn C, Moreci P, Williamson D, Ryan N. Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL): Initial reliability and validity data. J Am Acad Child Adolesc Psychiatry. 1997;36(7):980–988. doi: 10.1097/00004583-199707000-00021. [DOI] [PubMed] [Google Scholar]
- 14.First M, Spitzer R, Gibbon M, Williams J, Benjamin L. Structured Clinical Interview for DSM-IV Axis I Disorders: Patient Edition (SCID) New York: Biometrics Research Department: New York State Psychiatric Institute; 2002. [Google Scholar]
- 15.Hawton K, Appleby L, Platt S, Foster T, Cooper J, Malmberg A, Simkin S. The psychological autopsy approach to studying suicide: A review of methodological issues. J Affect Disord. 1998;50(2–3):269–276. doi: 10.1016/s0165-0327(98)00033-0. [DOI] [PubMed] [Google Scholar]
- 16.First MB, Benjamin LS, Gibbon M, Spitzer RL, Williams JB. Structured clinical interview for DSM-IV Axis II personality disorders. Washington, DC: American Psychiatric Press; 1997. [Google Scholar]
- 17.Keller MB, Lavori PW, Friedman B, Nielsen E, Endicott J, McDonald-Scott P, Andreasen NC. The Longitudinal Interval Follow-up Evaluation. A comprehensive method for assessing outcome in prospective longitudinal studies. Arch Gen Psychiatry. 1987;44(6):540–548. doi: 10.1001/archpsyc.1987.01800180050009. [DOI] [PubMed] [Google Scholar]
- 18.Shaffer D, Gould MS, Brasic J, Ambrosini P, Fisher P, Bird H, Aluwahlia S. A Children’s Global Assessment Scale (CGAS) Arch Gen Psychiatry. 1983;40(11):1228–1231. doi: 10.1001/archpsyc.1983.01790100074010. [DOI] [PubMed] [Google Scholar]
- 19.Endicott J, Spitzer RL, Fleiss JL, Cohen J. The Global Assessment Scale. A procedure for measuring overall severity of psychiatric disturbance. Arch Gen Psychiatry. 1976;33(6):766–771. doi: 10.1001/archpsyc.1976.01770060086012. [DOI] [PubMed] [Google Scholar]
- 20.Foa EB, Johnson KM, Feeny NC, Treadwell KR. The Child PTSD Symptom Scale: A preliminary examination of its psychometric properties. J Clin Child Psychol. 2001;30(3):376–384. doi: 10.1207/S15374424JCCP3003_9. [DOI] [PubMed] [Google Scholar]
- 21.Foa EB, Riggs DS, Dancu CV, Rothbaum BO. Reliability and validity of a brief instrument for assessing post-traumatic stress disorder. Journal of traumatic stress. 1993;6(4):459–473. [Google Scholar]
- 22.Birmaher B, Khetarpal S, Brent D, Cully M, Balach L, Kaufman J, Neer SM. The Screen for Child Anxiety Related Emotional Disorders (SCARED): Scale construction and psychometric characteristics. J Am Acad Child Adolesc Psychiatry. 1997;36(4):545–553. doi: 10.1097/00004583-199704000-00018. [DOI] [PubMed] [Google Scholar]
- 23.Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuring clinical anxiety: Psychometric properties. J Consult Clin Psychol. 1988;56(6):893–897. doi: 10.1037//0022-006x.56.6.893. [DOI] [PubMed] [Google Scholar]
- 24.Angold A, Costello EJ, Messer SC, Pickles A. Development of a short questionnaire for use in epidemiological studies of depression in children and adolescents. Int J Methods Psychiatr Res. 1995;5(4):237–249. [Google Scholar]
- 25.Beck AT, Steer RA, Carbin MG. Psychometric properties of the Beck Depression Inventory: Twenty-five years of evaluation. J Consult Clin Psychol. 1988;8(1):893–897. doi: 10.1037//0022-006x.56.6.893. [DOI] [PubMed] [Google Scholar]
- 26.Reynolds WM, Mazza JJ. Assessment of suicidal ideation in inner-city children and young adolescents: Reliability and validity of the Suicidal Ideation Questionnaire-JR. School Psychology Review. 1999;28(1):17. [Google Scholar]
- 27.Buss AH, Perry M. The Aggression Questionnaire. J Pers Soc Psychol. 1992;63(3):452. doi: 10.1037//0022-3514.63.3.452. [DOI] [PubMed] [Google Scholar]
- 28.Chaffin M, Wherry JN, Newlin C, Crutchfield A, Dykman R. The Abuse Dimensions Inventory: Initial data on a research measure of abuse severity. J Interpers Violence. 1997;12(4):569–589. [Google Scholar]
- 29.Brand AH, Johnson JH. Note on reliability of the Life Events Checklist. Psychol Rep. 1982;50:1274. [Google Scholar]
- 30.Lewinsohn PM, Rohde P, Seeley JR, Fischer SA. Age and depression: Unique and shared effects. Psychol Aging. 1991;6(2):247–260. doi: 10.1037//0882-7974.6.2.247. [DOI] [PubMed] [Google Scholar]
- 31.Spirito A, Stark LJ, Williams C. Development of a brief coping checklist for use with pediatric populations. J Pediatr Psychol. 1988;13(4):555–574. doi: 10.1093/jpepsy/13.4.555. [DOI] [PubMed] [Google Scholar]
- 32.Lazarus RS. Coping theory and research: past, present, and future. Psychosom Med. 1993;55(3):234–247. doi: 10.1097/00006842-199305000-00002. [DOI] [PubMed] [Google Scholar]
- 33.Dubow EF, Ullman DG. Assessing social support in elementary school children: The survey of children’s social support. J Clin Child Psychol. 1989;18(1):52–64. [Google Scholar]
- 34.Zimet GD, Dahlem NW, Zimet SG, Farley GK. The Multidimensional Scale of Perceived Social Support. J Pers Assess. 1988;52(1):30–41. doi: 10.1080/00223891.1990.9674095. [DOI] [PubMed] [Google Scholar]
- 35.Olson D, Portner J, Lavee Y. Family Adaptability and Cohesion Evaluation Scales (FACES-II) Minneapolis: University of Minnesota Press; 1985. [Google Scholar]
- 36.Muthén L, Muthén B. Mplus User’s Guide. 8th. Los Angeles, CA: Muthén & Muthén;; 1998–2017. [Google Scholar]
- 37.Meyers JL, Lowe SR, Eaton NR, Krueger R, Grant BF, Hasin D. Childhood maltreatment, 9/11 exposure, and latent dimensions of psychopathology: A test of stress sensitization. J Psychiatr Res. 2015;68:337–345. doi: 10.1016/j.jpsychires.2015.05.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Brent DA, Brunwasser SM, Hollon SD, Weersing VR, Clarke GN, Dickerson JF, Beardslee WR, Gladstone TR, Porta G, Lynch FL, Iyengar S, Garber J. Effect of a cognitive-behavioral prevention program on depression 6 years after implementation among at-risk adolescents: A randomized clinical trial. JAMA Psychiatry. 2015;72(11):1110–1118. doi: 10.1001/jamapsychiatry.2015.1559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Seligman F, Nemeroff CB. The interface of depression and cardiovascular disease: therapeutic implications. Ann N Y Acad Sci. 2015;1345:25–35. doi: 10.1111/nyas.12738. [DOI] [PubMed] [Google Scholar]
- 40.Sandler IN, Wolchik SA, Ayers TS, Tein JY, Luecken L. Family Bereavement Program (FBP) approach to promoting resilience following the death of a parent. Fam Sci. 2013;4(1) doi: 10.1080/19424620.2013.821763. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.