

Abstract
Erectile dysfunction (ED) has negative effects on quality of life. The first line of oral medication for this condition is phosphodiesterase type 5 inhibitors (PDE5I) including Tadalafil. Ocular complications associated with Tadalafil are rare and usually occurred in participant with known risk factors. In this report, we describe and review the related literature of development of nonarteritic anterior ischemic optic neuropathy -associated Tadalafil. A healthy nonsmoking 42-year-old male with a history of ED presented with acute onset of an inferior visual field defect on the right eye. Automated perimetry showed inferior altitudinal loss in the affected eye. The administration of Tadalafil was discontinued as a potential causative agent for this condition. During follow-up, neither improvement signs nor symptoms revealed.
KEYWORDS: Anterior ischemic optic neuropathy, erectile dysfunction, Tadalafil
INTRODUCTION
Erectile dysfunction (ED) has negative effects on quality of life. The first line of oral medication for this condition is phosphodiesterase type 5 inhibitors (PDE5I) including sildenafil citrate, Tadalafil, vardenafil hydrochloride, and avanafil.[1]
In 2003, Tadalafil was approved by US Food and Drug Administration (FDA) as third ED prescription drug pill (after sildenafil and vardenafil).[1,2]
In 2005, in the postmarketing setting, had been found that Tadalafil was associated with vision impairment related to nonarteritic anterior ischemic optic neuropathy (NAION) in certain patients taking these drugs.[3,4,5]
Some of these patients had underlying anatomic or vascular risk factors for the development of NAION unrelated to PDE5I use including low cup-to-disc ratio, more than 50 years old, diabetes, hypertension, coronary artery disease, hyperlipidemia, nocturnal hypotension, and smoking.[3,4] Although FDA concluded that they were not able to draw a cause and effect relationship, given these patients underlying vascular risk factors or anatomical defects,[2] the fact that this event occurs in a similar population to those who do not take these medicines, may be questionable sine, some of patients with sing and symptom of NAION had not any documented risk factor.[6]
In this report, we describe a NAION associated with Tadalafil in a healthy 48-year-old male without any risk factor and review the related literature. The emphasis of this report is consideration of Tadalafil as one of the differential diagnoses of NAION.
CASE REPORT
A healthy nonsmoking 42-year-old male with a history of ED presented with acute onset of an inferior visual field defect on the right eye that failed to resolve during 2 days. Past medical histories were no notable for any medical conditions include diabetes mellitus and hyperlipidemia. He had not any risk factor for cardiovascular diseases. The drug history was negative except Tadalafil (20 mg two times weekly) before participated in sexual intercourse for the treatment of ED since 8 years ago.
The visual field defect was happened within 3 h after the use of the last dose of medication.
General physical examination and review of the systems had normal finding and there were no symptoms or signs of temporal arteritis. Blood pressure measured 120/70 mmHg.
On ophthalmologic examination, his uncorrected visual acuity was 7/10 in the right eye and 3/10 in the left eye and best-corrected visual acuity was 8/10 in the right eye (OD; +0.75) and 7/10 in the left eye (OS; +2.75/−1.25 × 102). There was a right relative afferent pupil defect. Anterior segment examination revealed no significant abnormalities except mild cataract in both eyes. His intraocular pressure was normal for both eyes.
Dilated fundus examination revealed swelling of the right disc with a normal cup-to-disc ratio and a faint disc hemorrhage consistent with ischemic optic neuropathy [Figure 1]. The remainder of the examination results and also the fundus in left eye were normal. Automated perimetry (Swedish Interactive Threshold Algorithm-Fast) was normal in the left eye and showed inferior altitudinal loss in the right eye [Figure 2].
Figure 1.
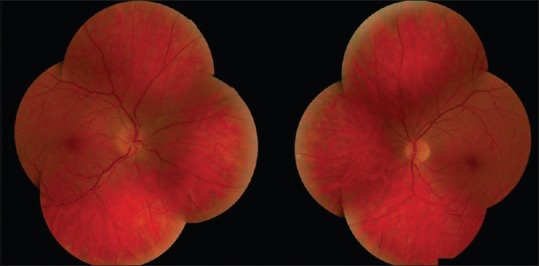
Fundus photograph. Blurring of the optic disk margin from edema with peripapillary hemorrhages in the right eye and normal optic disc in the left eye
Figure 2.
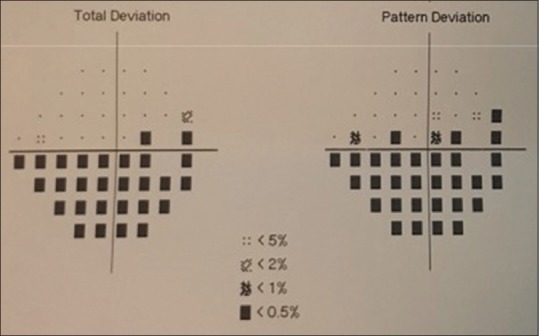
Humphrey visual field test showing inferior altitudinal loss in the right eye
Initial laboratory examinations include kidney and liver function tests, lipid profile, C-reactive protein, and echocardiography yielded normal results. Erythrocyte sedimentation rate was normal (20 mm). Based on the clinical and paraclinical evidence, the diagnosis of NAION-associated Tadalafil was made. Therefore, the patient was advised to avoid Tadalafil.
A 10-week follow-up revealed neither improvement signs nor symptoms.
DISCUSSION
Possible pathophysiological cause for the development of NAION included impaired blood supply of optic disk and anatomical disturbance of optic disk. Blood supply of optic disk arises from short posterior ciliary arteries, which branched to smaller vessels. These small vascular braches feed the laminar and prelaminar portion of the optic disk. Occlusion of these vessels can result in NAION.[6]
Regarding anatomical disturbance of optic disk, a small cup-to-disk ratio known as “Disk at risk” and crowed nerve fiber bundles at the margin of disk can be associated with the development of NAION.[4,5,6]
The point that makes our case very impressive was no underlying anatomic or vascular risk factors. Hence, these statements can support from clinical association between NAION and Tadalafil. The mechanism of action of Tadalafil in treatment of ED is related to cyclic guanosine monophosphate (cGMP).[7] During sexual activity, nitric oxide (NO) released from cavernous nerves. This NO stimulates guanylate cyclase enzyme formed cGMP. cGMP relaxes smooth muscle vessel that increased blood flow into corpus cavernosum and subsequent penile erection is happen.[1,7]
PDE5 degenerates cGMP and is naturally found in the corpus cavernosum. PDE5Is selectively inhibit this enzyme and the high levels of cGMP remain in corpus cavernosum, so improvement in erection function is achieved.[7]
In our case, we used the Naranjo criteria[8] to evaluate the probability of NAION-associated Tadalafil.
Our case had a causality score of 7 based on the above criteria (possible adverse drug reaction). This score was not higher because two reasons, first no re-administration was performed due to the important ophthalmological sequel and second permanent effect of AION on visual field, so there are no improvements occur when the drug discontinued.
There are some cases of NAION after PDE5I consumption that most of these cases associated with sildenafil and only limited cases of NAION-associated Tadalafil were reported. Since 2005 until April 2017, we found only four published cases[4,5,9,10] of NAION-associated Tadalafil none of which presented <4 h without risk factor [Table 1].
Table 1.
Clinical characteristics of previous reported patients with nonarteritic anterior ischemic optic neuropathy-associated Tadalafil use
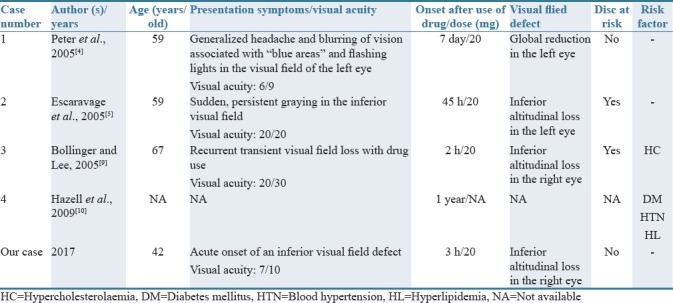
The mean age of these patients was 56.75 years (range: 42–67). Doses varied from 20 mg. Loss of visual acuity and decreased visual field occurred between 2 h and 7 days after oral dosing. Two patients had a known risk factor for the development of NOIAN.
In contrast the other case, the presentation of adverse effect in our case was rapid.
Although, generally, consumption of Tadalafil at night and following nocturnal hypotension increases the risk of NOIAN, the symptom can occur more rapidly.
Hypotension during night can cause optic nerve ischemia by reducing the optic disk blood supply below to crucial level. This theory can be as important systemic factor association between PDE5I and NAION.[3,4,5]
In the previous study showed that people with a history of unilateral NAION or crowed optic disk on funduscopic examination in one eye, sildenafil could increase the risk of development of ischemic optic neuropathy in the fellow eye.[3]
Such as this recommendation should be considered in patients who use Tadalafil.
Although sildenafil and vardenafil inhibit PDE in the eye, more than Tadalafil, Tadalafil is not seemed absolute safe drug from aspects of ophthalmology.[10]
We thereby suggest the possible rapid onset of irreversible and unpredictable NAION without any risk factor during the use of Tadalafil.
The absence of resolution of NAION after discontinuation of Tadalafil in our patient suggests an irreversible and serious adverse effect that is better that ophthalmologist consulting is done before starting for patients because the best solution for the prevention of this effect is avoidance, especially in high-risk patients.
In conclusion, NAION-associated Tadalafil should be considered as a differential diagnosis any acute visual field defect without documented cause.
AUTHORS' CONTRIBUTION
AD, MM and MP designed the study and were responsible for the overall case management. MA, AA and MP prepared the manuscript. AD and MM conducting the study and revising the draft. All authors approved the final version of the manuscript, and agreed for all aspects of the work.
Declaration of patient's consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Gresser U, Gleiter CH. Erectile dysfunction: Comparison of efficacy and side effects of the PDE-5 inhibitors sildenafil, vardenafil and tadalafil – Review of the literature. Eur J Med Res. 2002;7:435–46. [PubMed] [Google Scholar]
- 2.FDA updates labeling for erectile dysfunction drugs. FDA Consum. 2005;39:3. [PubMed] [Google Scholar]
- 3.Laties AM. Vision disorders and phosphodiesterase type 5 inhibitors: A review of the evidence to date. Drug Saf. 2009;32:1–8. doi: 10.2165/00002018-200932010-00001. [DOI] [PubMed] [Google Scholar]
- 4.Peter NM, Singh MV, Fox PD. Tadalafil-associated anterior ischaemic optic neuropathy. Eye (Lond) 2005;19:715–7. doi: 10.1038/sj.eye.6701614. [DOI] [PubMed] [Google Scholar]
- 5.Escaravage GK, Jr, Wright JD, Jr, Givre SJ. Tadalafil associated with anterior ischemic optic neuropathy. Arch Ophthalmol. 2005;123:399–400. doi: 10.1001/archopht.123.3.399. [DOI] [PubMed] [Google Scholar]
- 6.Miller NR, Arnold AC. Current concepts in the diagnosis, pathogenesis and management of nonarteritic anterior ischaemic optic neuropathy. Eye (Lond) 2015;29:65–79. doi: 10.1038/eye.2014.144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Eltony SA, Abdelhameed SY. Effect of chronic administration of sildenafil citrate (Viagra) on the histology of the retina and optic nerve of adult male rat. Tissue Cell. 2017;49:323–35. doi: 10.1016/j.tice.2017.01.006. [DOI] [PubMed] [Google Scholar]
- 8.Naranjo CA, Busto U, Sellers EM, Sandor P, Ruiz I, Roberts EA, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30:239–45. doi: 10.1038/clpt.1981.154. [DOI] [PubMed] [Google Scholar]
- 9.Bollinger K, Lee MS. Recurrent visual field defect and ischemic optic neuropathy associated with tadalafil rechallenge. Arch Ophthalmol. 2005;123:400–1. doi: 10.1001/archopht.123.3.400. [DOI] [PubMed] [Google Scholar]
- 10.Hazell L, Cornelius V, Wilton LV, Shakir SA. The safety profile of tadalafil as prescribed in general practice in England: Results from a prescription-event monitoring study involving 16 129 patients. BJU Int. 2009;103:506–14. doi: 10.1111/j.1464-410X.2008.08000.x. [DOI] [PubMed] [Google Scholar]