

Abstract
Clinical decision-making may have a role in racial and ethnic disparities in healthcare but has not been evaluated systematically. The purpose of this study was to synthesize qualitative studies that explore various aspects of how a patient’s African-American race or Hispanic ethnicity may factor into physician clinical decision-making. Using Ovid MEDLINE, Embase, and Cochrane Library, we identified 13 manuscripts that met inclusion criteria of usage of qualitative methods, addressed U.S. physician clinical decision-making factors when caring for African-American, Hispanic, or Caucasian patients, and published between 2000 and 2017. We derived 6 fundamental themes that detail the role of patient race and ethnicity on physician decision-making, including: importance of race, patient-level issues, system-level issues, bias and racism, patient values, and communication. In conclusion, a nonhierarchical system of intertwining themes influenced clinical decision-making among racial and ethnic minority patients. Future study should systematically intervene upon each theme in order to promote equitable clinical decision-making among diverse racial/ethnic patients.
Keywords: clinical decision-making, healthcare disparities, minority health, bias
INTRODUCTION
The clinical decision-making process is complex.[1, 2] Guidelines exist to help clinicians make evidence-based decisions.[3, 4] Although there are clinical scenarios in which clinical decision-making should be clear (e.g. Class I guideline indication or Class III guideline indication), there are many areas of medicine that do not fall into clear decision categories and are much more vague. Race or ethnicity is rarely an indication for change in clinical care. Yet, notable differences in clinical decision-making process exist among racial or ethnic minority patients.[3, 5]
Understanding differences in provider clinical decision-making by race and ethnicity is a necessary first step in creating equity in healthcare. Multiple studies of health care providers have demonstrated negative implicit bias towards racial and ethnic minority patients, particularly African-Americans and Hispanics, [6–9] and some have concluded that racial or ethnic bias may contribute to health disparities.[10, 11] However, other studies suggest that a negative bias towards minorities is not associated with inequitable decision-making.[12, 13] Several qualitative studies have explored the relationship between physician decision-making and patient race or ethnicity,[14, 15] but there has been no robust synthesis of qualitative studies of physician decision-making across race and ethnicity.
A qualitative meta-synthesis is an ideal approach for critically evaluating qualitative data that explore physician clinical decision-making. Thus, the objective of this study was to rigorously evaluate and synthesize qualitative studies that explore factors related to contemporary physician clinical decision-making for African-American and Hispanic patients over the past two decades. Increasing awareness and understanding of the clinical decision-making process will contribute to the design and evaluation of future interventions that aim to create equity in healthcare.
METHODS
This study used the Enhanced Transparency in Reporting the Synthesis of Qualitative Research (ENTREQ) to understand physician approaches to clinical decision-making among racial/ethnic minorities.[16] A systematic literature search was conducted using the Preferred Reporting Items for Systematic reviews and Meta-analyses (PRISMA).[17] The Letts Criteria was performed for quality appraisal of qualitative studies.[18] The Thomas and Harden approach was used for thematic synthesis.[19]
Search Strategy
Inclusion criteria for this meta-synthesis included contemporary qualitative studies, published in 2000 or later, that address physician perceptions of providing clinical care to African-American or Hispanic patients in the U.S. Studies were excluded if they were non-qualitative studies, focused on other races/ethnicities, or focused only on patient rather than physician perceptions. When a manuscript included a combination of physician, nurse, medical student, and patient perspectives, only physician results were included for analysis. A professional librarian (L.H.) searched Ovid MEDLINE, Embase, and the Cochrane Library to identify qualitative studies addressing the factors related to physician clinical decision-making for African-Americans and Hispanics. We limited the search to U.S. studies with an emphasis on African-American or Hispanic patients since they represent the largest racial and ethnic groups in the U.S. and have the highest proportion of healthcare disparities.[20] The search strategy for each database included the following concepts: physicians, ethnicity, healthcare treatment, and qualitative studies. Multiple subject headings and text word terms were included to describe these concepts. The search was limited to English-language studies, and the years 2000 to present, in order to address contemporary care. The search is complete through April 3, 2017. The PRISMA search strategy is in the Supplement (Supplemental Tables Search Strategy).[17] All manuscript titles and abstracts identified in the initial search were reviewed for inclusion criteria by the primary investigator (K.B.) (Figure). An additional manuscript was identified outside of the professional librarian search using Google search and was added to this study.
Quality Appraisal
The Letts “Guidelines for Critical Review Form: Qualitative Studies” provides one of the most comprehensive appraisals of qualitative studies.[18] Letts Criteria has precision in the assessment of rigor through 1) credibility: trustworthiness of the analysis, 2) transferability: generalizability, 3) dependability: consistency of data often achieved with an audit trail, and 4) confirmability: bias reduction of the researcher by seeking external opinions of the data.[18] All manuscripts meeting inclusion criteria were appraised with the Letts Criteria by the primary investigator (K.B.), and a random sample was reappraised by study team member (D.K.) for efficacy (Table 1). Manuscripts were evaluated and reported across 8 key domains: study purpose, literature, study design, sampling, data collection, data analyses, overall rigor, and conclusions/implications.[18] All manuscripts met most Letts criteria and were deemed appropriate for inclusion. However, most studies did not evaluate for saturation of themes due to limits in reaching target number of racial and ethnic minority participants. The majority of the studies were also lacking researcher relationship to participants, and researcher assumptions and biases. Although many studies were missing transferability and dependability, overall rigor was appropriately met for the majority of studies through analytic rigor, credibility, and confirmability.
Table 1.
Letts et al. Critical Review of Literature
| #1 [22] | #2 [23] | #3 [24] | #4 [25] | #5 [26] | #6 [27] | #7 [28] | #8 [29] | #9 [30] | #10 [31] | #11 [14] | #12 [15] | #13 [32] | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study Purpose | Was the purpose and/or research question stated clearly? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Literature | Was relevant background literature reviewed? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Study Design | Was a theoretical perspective identified? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Sampling | Was the process of purposeful selection described? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Was sampling done until redundancy/saturation in data was reached? | No | No | No | No | Yes | No | No | Yes | No | Yes | No | No | No | |
| Was informed consent obtained? | Yes | Yes | Yes | -- | Yes | -- | Yes | -- | Yes | Yes | Yes | Yes | Yes | |
| Data Collection | Were the participants described clearly and completely? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Were the roles of the researcher and relationship with participants described? | No | Yes | No | No | No | No | No | No | No | No | No | No | No | |
| Were assumptions and biases of researchers identified? | No | Yes | No | No | No | No | No | No | No | No | No | No | No | |
| Was procedural rigor used? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | |
| Data Analyses | Analytic Rigor: Were data analyses inductive? | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Analytic Rigor: Were findings consistent and reflective of data? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | |
| Auditability: Was there a decision trail? | No | Yes | No | No | No | Yes | No | Yes | Yes | No | Yes | No | No | |
| Auditability: Were the processes of analyzing data described adequately? | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | |
| Theoretical Connections: Did a meaningful picture of the phenomenon emerge? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | |
| Rigor | Was there evidence of credibility? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Was there evidence of transferability? | Yes | No | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | |
| Was there evidence of dependability? | No | No | No | No | No | Yes | No | No | Yes | Yes | Yes | Yes | Yes | |
| Was there evidence of confirmability? | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | |
| Conclusions/Implications | Were conclusions appropriate given study findings? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Did findings contribute to theory development and future practice? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
Meta-synthesis
Meta-synthesis has an interpretative rather than aggregating intent, in contrast to meta-analysis of quantitative studies.[21] Qualitative data are useful for providing a snapshot of one person’s interpretation of an event or phenomenon. By bringing together many different interpretations, conclusions are strengthened by discovering common themes and differences, and by building new interpretations of the topic of interest.[21] Thus, a thematic synthesis was used based upon the Thomas and Harden approach.[19] Manuscripts were summarized with study aim, study design, methods, participant descriptions, and summary of findings by the primary investigator (K.B.) (Table 2). All primary quotes from each manuscript underwent iterative line-by-line coding for thematic analysis with an inductive approach by the primary investigator (K.B.), and study team (H.L., D.K.). Theory was derived from the data rather than pre-existing theories being applied to the data. Additional iterations were characterized into derived themes and subthemes over the course of several weeks. Concordance was achieved through majority agreement of the study team. Credibility and confirmability were obtained through triangulation with the initial study team (K.B., J.J., H.L., D.K., U.S.) and expert co-authors. An audit trail of theme derivations was maintained throughout the study. The final derived themes exhibited overlap but were further characterized by exemplar quotes and written description (Table 3). Exemplar quotes best displayed the derived themes and subthemes. The physician’s self-identified race and ethnicity, sex, and city of practice were included when available to provide further insight into quotes.
Table 2.
Study Descriptions
| Author, Date | Study Aim | Study Design | Methods | Participants | Summary of Findings | Derived Themes* |
|---|---|---|---|---|---|---|
| #1. Bonham et al., 2009 [22] | To provide physicians attitudes towards race, genetics, and clinical medicine | Qualitative descriptive | Focus groups | 50 Caucasian internists and 40 African-American internists | 1) Both race groups agreed that race is important but there were differences regarding the importance of race. 2) They were reticent to make connections among race, genetics, and disease, and believed genetics had a limited role in explaining racial differences in health. 3) There was enthusiasm about the future of genomic medicine | Importance of Race, Patient-level Issues |
| #2. Braun et al., 2010 [23] | To describe perceptions guiding physicians’ end of life decision-making and explore the relationship between physicians’ race and ethnicity and decision-making | Grounded theory | Focus groups | 11 Caucasian, 8 African-American, 7 Hispanic internists and subspecialists | Physicians agreed about the following themes irrespective of physician race and ethnicity: 1) role of the physician, 2) response to “unreasonable” requests, 3) organizational factors, and 4) physician training with end of life care. Physician racial/ethnic differences included: 1) reduce burden of surrogate decision-making, 2) responding to “do everything”, 3) influence of physician-patient racial/ethnic concordance/discordance, 4) cultural differences in truth-telling, and 5) spirituality | Patient Values, Communication |
| #3. Clark-Hitt et al, 2010 [24] | To explain racial disparities from perceptions of physicians and nurses | Grounded theory | Semi-Structured interviews | 13 Caucasian, 3 Asian, 2 African-American physicians and 8 Caucasian nurses | African-Americans receive unequal care to Caucasians because of: 1) worse access to care, 2) physician bias, 3) African-American patients’ perceived shortcomings, and 4) Caucasian patients’ demands | Patient-level Issues, Bias & Racism |
| #4. Frank et al., 2010 [25] | To explore physician use of race based therapies | Qualitative descriptive | Focus groups | 50 Caucasian, 40 African-American physicians | 1) Some physicians supported race-based therapies since this could encourage compliance and promote healthy behaviors. 2) Physicians thought that the effectiveness of some medications varied across race and perhaps genetic level and 3) were concerned that patients were not receiving therapy secondary to race. 4) Race-based medicine like BiDIL was developed primarily for commercial interests. | Importance of Race |
| #5. Goodman et al., 2006 [26] | To examine barriers and facilitators of colorectal cancer screening among Mid-Atlantic Latinos | Qualitative descriptive | Structured interviews | 27 physicians and 70 Latino patients | The physicians perceived the following barriers: primary care site characteristics, knowledge deficits of physicians and patients, cost, attitudes, ordering priorities, language, procedural issues, pain, discrimination, and immigrant status. | Patient-level Issues, System-level Issues, Bias & Racism, Patient Values, Communication |
| #6. Johansson et al., 2011 [27] | To provide physician and nurse perception of impact of race on patient care and professional careers | Qualitative descriptive | Focus groups | 7 physicians (African-American and Hispanic) and 6 nurses (African-American and Hispanic) | Racism and prejudice was present at 3 levels: 1) healthcare system to patient, 2) provider to patient, and 3) provider to provider. Communication and culture was important among patients who preferred racially concordant care providers. Racism and prejudice was also experienced during careers | Patient-level Issues, Bias & Racism, Communication |
| #7. Mott-Coles et al., 2014 [28] | To address how healthcare providers approach cultural beliefs of African-American and Latina women | Qualitative descriptive | Structured interviews | 3 physicians, 9 nurses, and 2 technicians | Similar approaches for care were provided to patients irrespective of race and ethnicity/culture. However, participants felt that culturally sensitive care was also provided. | Patient Values, Communication |
| #8. Nunez-Smith et al., 2008 [29] | To provide physician perspectives on race | Qualitative descriptive | Structured interviews | 25 physicians of African descent | 1) Perceived race-related healthcare experiences shape view of healthcare and professional identities prior to formal medical training. 2) Protecting race/ethnic minority patients from discrimination is a top priority. 3) Physicians rely on external support systems for race-related issues rather than the healthcare system. 4) Physicians perceive differences between interpretations of potentially offensive race-related experiences and non-minority colleagues. 5) Physicians are uncomfortable voicing race-related issues at work. | Bias & Racism |
| #9. Owsley et al., 2006 [30] | To identify perceived barriers to eye care among older African-Americans and ophthalmologists and optometrists | Qualitative descriptive | Focus groups | 35 eye care providers (physicians and optometrists) and 119 African-American patients | 1) Barriers identified by patients included: transportation, trust. communication, and cost. Patient comments were predominantly positive regarding attitudes about eye care. 2) Barriers identified by providers included: transportation, cost, trust, and insurance. Provider comments were predominantly negative regarding frustration with African-American patients. | Patient-level Issues, Patient Values, Communication |
| #10. Park et al., 2005 [31] | To explore perceptions of resident physicians’ abilities to provide quality care to diverse population | Grounded theory | Focus groups and Structured interviews | 33 Caucasian, 7 African-American, 6 Hispanic, 14 Asian, 8 other medical residents | Cross-cultural care is important to residents and institutions, but formal training is not provided and should be provided. Coping behaviors instead of skills are used with diverse patient groups. | Importance of Race, Communication |
| #11. Plaisime et al., 2016 [14] | To explore providers’ experiences with race and African-American men | Grounded theory | Semi-structured interviews | 9 physicians, 2 nurses, 5 medical students (10 African-American and 6 Caucasian) | Racism was identified in 2 themes: 1) bias against African-American men; fear and discomfort with African-American men, and 2) cognitive dissonance. | Bias & Racism |
| #12. Snipes et al., 2011 [15] | To determine if race is medically relevant | Qualitative descriptive | Focus groups | 40 African-American and 50 Caucasian physicians | Differences in relevance of race by race of MD: 1) African-Americans thought race was a factor for choosing treatment options like aggressive therapy and found importance in understanding the patient’s views (alternative medicine, preferences, cultural beliefs). 2) Few Caucasians thought race was an important part of medical history and thought that all patients should be treated aggressively regardless of race | Importance of Race, Patient-level Issues, Communication |
| #13. Ward et al., 2010 [32] | To determine how resident physicians view barriers to colorectal cancer screening among African-American patients and to compare perceptions with the literature | Mixed methods | Structured interviews | 14 Caucasian, 9 Asian, 4 African-American, 3 other upper level resident physicians | Resident physicians believed awareness of colorectal cancer was low among African-Americans. Perceived barriers included: lack of knowledge, fear, personal circumstance, procedure related concerns. Residents desired increased education, public awareness, and easier scheduling in order to improve screening of African-Americans. Residents did not recognize key perceptions of barriers faced by African-American patients described in the literature. | Patient-level Issues, Patient Values |
Derived themes are based upon available quotes published within the manuscripts and are further described in Table 3.
Table 3.
Themes Surrounding the Influence of Race in Physician Decision-Making
| Derived Themes/Subthemes | Study Theme Primary Paper (table 1 reference# page number) | Exemplar Quotes (table 1 reference# page number) |
|---|---|---|
| I. Importance of Race | ||
| Discomfort discussing race | Race is poorly defined (1p4), Race is a sensitive issue (1p6) | “But you still have to be careful. I mean if you tell somebody too many negatives about their ‘race’ or something like that, they might take it the wrong way. (Philadelphia, Caucasian)” (1p6) |
| Definition of race | Race is poorly defined (1p4 and 5), Race is one of many factors (1p6), Reticent about race and genetics (1p6 and 7), Skepticism about race and therapy (4p386), Implications of race and therapy (4p387), Market BiDil (4p387), Race is not the future of medicine (4p387), Value of cross-cultural care (10p877), Mentors and evaluation (10p878), Race is unimportant (12p5) | “Race is a social construct. It’s useful. It’s very useful, given the historic context; I would not let anybody not refer to me as a black woman. However, I actually do believe that there’s no biological basis for that… (Atlanta, African-American)” (1p5) “So, genetics plays a huge role in all this. But my objection is that I don’t think race is as useful a categorizing tool because the correlations aren’t so good. There’s been a lot of bleeding over between groups, through intermarriage and travel and so forth. And it’s just not as exact as we would like it to be. (Atlanta, Caucasian)” (1p6 and7) |
| Race matters in medicine | Race is poorly defined (1p4 and 5), Race is relevant (1p5 and 6), Support of race based medicine (4p386), Opposition of race based medicine (4p386), Weak link between race and medicine (4p386), Stereotyping (10p877), Beliefs (10p877), Race is unimportant (12p5), Race is important (12p5 and 6) | “You know you’re going to suspect certain diseases more commonly in women than in men and you’re going to treat young maybe different than old. There are so many different factors. To me race is just one of the many of them. (Baltimore, Caucasian)” (1p6) “African Americans…have four times greater risk of end-stage renal disease than the general white population…So, to me that means that you’re dealing with an African American who’s at risk, and one of the important drugs for African Americans would be ace inhibitors. Use what you want, but make sure an ace inhibitor is there, because of the risk that they carry. (Philadelphia, African-American focus group)” (4p386) |
| Genetics improve care | Positive feeling for personalized medicine (1p7 and 8), Genetics supercede race (1p8), Race is defined by genetics (4p386), Compliance with race based medicine (4p386), Genetics for drug response (4p386) | “I think with the identification of the human gene (sic) with the human genome project, that’s going to be huge for the future, because then you will actually will be able to tailor make medications based on a genetic profile. And make it just more personalized irregardless of what your race may or may not be. I think that is where, hopefully, we’re headed in the future… (Baltimore, African-American)” (1p8) |
| II. Patient-level Issues | ||
| Accessibility/insurance | Access to care (9p2799, 3p393 and 394, 5p258), Socioeconomic status and race (1p6, 13p306), enetics do not explain disparities (1p7), Validity of disparities research (3p395), Site characteristics (5p258), Physician practice and settings (6p52) | “When I think about resources and what we do know about health disparities, access to care, testing and being able to get the appropriate medication, education and support systems in place, that’s something that we know, that’s something that’s in front of us. (Baltimore, African-American)” (1p6) “I think there is a portion of it that’s genetics but particularly with things like cancer, I’m going to say that I think most of it is probably environmental in access to care and treatment differences. I don’t think the majority of the difference is accounted for by genetics. I think more of it can be accounted for in that people may not have access to a physician or wait to go to a physician or when they get there it takes them longer to be diagnosed and then longer to be treated. (Atlanta, African-American)” (1p7) |
| Patient liability | Perceived shortcomings (3p390 and 391), Priorities (5p258), Attitudes (5p258), Medical Information is most important (12p4) | “… this is my impression, that the African Americans have tended not to want to go to see the urologist while the Caucasian patients have been willing to go. [The Caucasian patients] said, “Sure, I’ll go talk to him.” Actually, really they are interested and going and talking with the specialist. … (male, Caucasian) (3p391) |
| Patient demands | Caucasian patient demands (3p391 and 392), Trust (6p52), Lack of knowledge of colorectal cancer (13p306), Lack of awareness (13p306) | “White people, especially White middle-class people have a sense of entitlement, especially when it comes to health care. And they’ll demand what they want, and they [doctors] think that people of minority status who are not accustomed to receiving whatever they want are probably less likely to be as demanding. (male, Caucasian)” (3p391 and 392) |
| Immigrant | Immigrant (5p258) | “No data from prior country on medical history” (5p258) |
| Multiple comorbidities | Immigrant (5p257), Personal/social circumstances (13p306) | “They come here to the hospital with serious illnesses. They don’t come here to be screened.” (13p306) |
| III. System-level Issues | ||
| Site issues | Site characteristics (5p258) | “Organizational accessibility of clinics as a barrier” (5p258) |
| Physician knowledge issues | Site characteristics (5p258), Knowledge (5p258) | “Test indications and sensitivity; confusion between colorectal cancer and prostate cancer among men or between the pelvic exam and fecal occult blood test among women” (5p258) |
| IV. Bias & Racism | ||
| Bias | Provider bias (3p393), Discrimination (5p258), Protecting minority patients (8p1473), Disparity in treatment (6p52), Two-tiered medical system (6p52), Perception of African-American males (11p4), Biased care (11p5) | “You wonder if it is because we as humans want people who look like us to get the care that we would want. You know that there’s somehow a better identification of, “This could be my grandfather, this could be my dad, or this could be.” Whereas someone who is Black or Native American, or Somali, I just don’t quite, I don’t walk in their shoes as easily. And, you know, who knows? Is there a hard wiring there? I don’t know. I’d like to believe that there isn’t. (male, Caucasian)” (3p393) “Two patients with … exactly the same symptoms and the Black patient was given …less than the White patient.” (6p52) “Well, I regret to say [that Black males are] not met with great fairness. I think that the medical establishment by and large is hierarchal, conservative, fearful, and not ready to relinquish its power. - (Caucasian male)” (11p4) |
| V. Patient Values | ||
| Trust | Trust (9p2799), Reaction to diagnosis (7p446), Site characteristics (5p258), Patient and physician concordance/discordance (2p6 and 7) | “not trusting doctor leads to noncompliance,” (9p2799) |
| Spiritual beliefs | Faith and spirituality (9p2799, 2p7) | “I feel quite comfortable to talk about spirituality. I use spirituality a lot- most of my black patients are spiritual, we discuss limitations on what we can do, and that they keep in perspective what God sees as healing versus what he doesn’t – that we can sometimes not do everything. It allows them to bring out their hopes, and I never try to squash anyone’s hopes, but I do give them some reality and then say ‘Now it’s up to God’.” (2p7) |
| Fear of procedures | Fear of outcomes (13p306), Fear of procedures (13p306) | “Fear of the unknown. The thinking is ‘I’m fine. Why go looking for something that may alter my life?’” (13p306) |
| VI. Communication | ||
| Culture | Communication (9p2799, 6p52), Acculturation (7p446), Family (7p446), Education (7p446), Facilitation (5p259), Skills for cultural barriers (10p877) | “An African-American physician growing up around African-Americans, is comfortable around African-Americans. ‘That’s familiarity.’” (6p52) |
| Language | Knowledge (5p258), Language (5p258), Literacy and language (10p877), Diversity (6p52) | “Be careful with your interpretation of what you think they’re telling you. And with how well you think that they’re understanding your point. … So make sure that you have the patients actually say it back to you.” (10p877) |
| Negotiation | Skills negotiation (10p878), Race is important (12p6), Unreasonable requests (2p4) | “In your case report we started the conversation with, I think we all agreed that that patient was a walking time bomb. For me the interesting question may or may not be related to race – it’s why did she walk into the office at that point and still have no treatment. So, one of my goals is always to try to understand what motivates people – you know, their paradigm of their own health. And that may or may not be a race-related issue. (Los Angeles Focus Group, Caucasian)” (12p6) |
RESULTS
Among 579 manuscripts identified with the initial search strategy, 86 were duplicates. The primary investigator (K.B.) reviewed 493 manuscript titles and abstracts for inclusion criteria; 481 manuscripts were excluded (patient perceptions only n=186, review n=23, non-U.S. study n=78, non-qualitative study n=143, not involve race n=4, off topic n=40, non-physician n=3, other race and ethnicity n=4). An additional manuscript not found during the professional search was identified during literature search and added for a final total of 13 manuscripts representing 518 physicians (Figure 1, [14, 15, 22–32]).
Figure 1. Flowchart.

Manuscripts meeting inclusion criteria were identified among 3 research databases.
Among the final 13 manuscripts, 6 derived themes addressed factors related to physician clinical decision-making for African-American and Hispanic patients. Derived themes included the importance of race, patient-level issues, system-level issues, bias and racism, patient values, and communication (Table 3). The themes were further characterized by 18 subthemes exploring reasons for differential clinical decision-making among African-American and Hispanic patients. The themes were not hierarchical in relationship but rather an interrelated system of themes that appeared to potentiate each other (Figure 2).
Figure 2. Factors Contributing To Racial/Ethnic Differences In Patient Care.
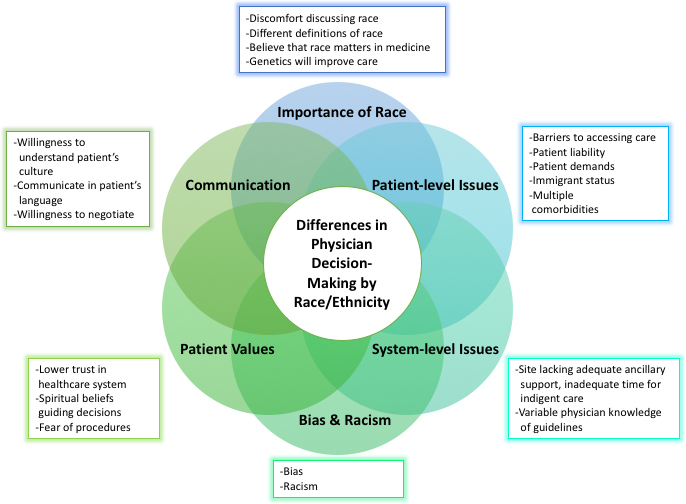
Physician Decision-Making Schematic of derived themes and subthemes
I. Importance of Race
Physicians had different perspectives on the importance of race in clinical decision-making. There was support and disapproval for explicitly using race in clinical decision-making. Subthemes included discomfort discussing race with patients, differing opinions regarding the definition of race, affirmation that race matters in medicine and should be used to guide decision-making, and believing that genetics may improve care of racial and ethnic minorities. However, physician perspectives differed by physician race.
A Caucasian physician described difficulty in using race to make clinical decisions since this physician was unclear of the appropriate way to define race.
“Plus there’s no certain line about what race is. I mean what percentage of a particular race do you have to be to be that race. Do you have a reflectometer to measure the skin color? What does it mean? (Baltimore, Caucasian)” (reference 1 page 4, 1p4)
An African-American physician described that race matters but chose not to describe race in clinical settings due to the potential improper treatment of patients based upon labeling of race and ethnicity.
“… but I think that there are some real historical implications of race as it relates to health status of African Americans. The issue of race was used to separate African Americans and European Americans on wards. Your race identified where you would go, and what level of care you received…One of the reasons I don’t take race is because historically, I have a huge problem with how it has been used. And, I’m not sure what that marker will mean in, as I put it on the chart as it, as that chart flies through here and there. (Detroit, African-American)” (1p5)
II. Patient-level Issues
Physicians attributed racial and ethnic differences in clinical decision-making to common patient-level issues that were assumed to be associated with race. Subthemes included addressing barriers of accessibility like insurance, patient liability for outcomes, patient demands varying by race and ethnicity, immigrant status changing the ability to provide clinical care, and multiple comorbidities of racial and ethnic minorities impacting patient outcomes.
One Caucasian physician shared how she had not sent her racial/ethnic minority patients to see specialists when indicated because the patients were underinsured.
“So it’s really hard to get a lot of specialists. And they will be upset if you refer someone that really doesn’t need to be referred to see medical assistance patients. Because they’re not going to get reimbursed for it at all. And they don’t want to be seeing something that the primary care provider could have taken care of. Whereas … someone who’s educated, working, has good insurance, they want … probably specialist because their insurance is going to pay for it. So that’s a disparity. (female, Caucasian)” (3p393)
Another Caucasian physician described that racial/ethnic minority patients were less adherent to medical regimens. Therefore, she was less likely to send her patients to specialists.
“… if a physician feels the patient isn’t very compliant with the regimen they’ve recommended, then they might be less likely to send them to a specialist … if they’re not even following up with the treatment I recommend, why bother to send them to another physician, who’s going to recommend, to evaluate this problem when they’re not even taking care of their hypertension in the first place? (female, Caucasian)” (3p390)
III. System-level Issues
Physicians described system-level issues that factored into the clinical decision-making process for racial and ethnic minority patients. Subthemes included site issues and physician knowledge issues related to caring for racial and ethnic minority patients.
In a clinic serving a predominantly minority population, physicians described inadequate support of the healthcare clinic and lack of guidelines as a reason for disparities in this population.
“Insufficient primary care clinic infrastructure (personnel, space, data support etc) as a barrier” (5p258)
“No guidelines, or clinic policies concerning colorectal cancer in clinics as a barrier” (5p258)
IV. Bias & Racism
Physicians from both Caucasian and African-American races described bias and racism as reasons for differences in clinical decision-making of racial and ethnic minority patients. Specifically, they believed that minority patients were subject to negative bias and racism. An African-American physician described an unconscious racism example he has witnessed from Caucasian physicians towards African-American patients.
“… the physician is empathizing more for the White patient because he has more of a connection with him. … Most doctors who are very good doctors, and otherwise nice people, are simply doing less for the Black patient because they have this unconscious racism. I guess it’s kind of hard to swallow, but you almost don’t want to accept it. (male, African-American)” (3p393)
A Caucasian physician described an example of bias or racism towards African-American patients leading to differences in clinical care.
“I’ve had … [Black] patients who I think have not been offered procedures because of either where they were economically or where they were assumed to be economically because of their race… I had a patient who clearly needed to be catheterized for their presentation and it was suggested that we do medical management. And I remember talking to the cardiologist and just saying that I didn’t understand why we’re doing this … As soon as we started talking, he said, “oh well, of course, we’ll cath him.” And so, like that, it changed… [I] certainly have enough anecdotal experience to think that people are probably [being] treated differently based on race. - (male, Caucasian)” (11p5)
V. Patient Values
Physicians attribute differences in clinical decision-making to variable patient values demonstrated in racial and ethnic minority patients. Subthemes included lower levels of trust in the healthcare system among minority patients related to historical disservice, spiritual beliefs guiding minority patient decisions, and minorities’ fear of procedures.
Physicians below described positive and negative experiences discussing religion with their racial and ethnic minority patients.
“Blacks tend to be, uh, very religious individuals and so, if you’re not a religious person yourself, if you really don’t have that, the faith, and, really talk about God, - it’s hard to get their trust,-that’s why doctors who are not religious or don’t show it may have it harder to gain black patients’ trust.” (2p6)
“The Hispanic physician groups had the most diverse responses to the question about religious beliefs, ranging from not mentioning faith or religion at all because it could be interpreted as ‘too intrusive’ to asking everyone about religious beliefs because they had experienced patients who “stopped stressing out when you talk to them about God” and that it restored patients’ hope.” (2p7)
VI. Communication
Differences in communication were thought to contribute to differences in clinical decision-making for racial and ethnic minority patients. Subthemes included expressing willingness to understand a patient’s culture, communication through the patient’s language, and willingness to negotiate with the patient to achieve care goals.
One physician shared the importance of inquiring about the individual racial/ethnic minority patient’s culture in order to improve the physician-patient relationship.
“I think the biggest one is to not be afraid of the fact that you’re going to hurt their feelings by asking them, “What cultural things do you think I should know about you to help me care for you better?” (10p877)
A physician described how he maintained a relationship with his Hispanic patient by negotiating treatment with both guideline based allopathic medicine and complementary alternative medicine.
“I have a patient who is Hispanic who really doesn’t want to come to terms with his diagnosis of diabetes. He’s a young guy and he’s trying all kinds of herbs, and I had to put aside my scientific thinking to come to an agreement with him that he could do that as long as he also monitored his blood sugar.” (10p878)
DISCUSSION
In this meta-synthesis of contemporary qualitative studies, physicians from diverse backgrounds believed that a patient’s race and ethnicity factored into the clinical decision-making process for healthcare. We derived six key themes factoring into the clinical decision-making process, including: importance of race, patient-level issues, system-level issues, bias and racism, patient values, and communication. Many of the subthemes implied negative perspectives towards racial and ethnic minorities. Overall, the themes were not hierarchical rather an interrelated system of issues that potentiate each other. This study moves the racial and ethnic disparities field forward by openly asking how race and ethnicity impact clinical decision-making. Compared to quantitative studies, this meta-synthesis was able to demonstrate the interrelated system of factors that contribute to racial and ethnic differences in care. This study provides an informed guide of factors that must be targeted in order to achieve equity in clinical decision-making among diverse racial and ethnic populations.
Our results support quantitative findings that suggest the physician clinical decision-making process is influenced by patient race and ethnicity.[3, 33] Clinical decisions are not being made on purely objective medical information.[3, 33] The Institute of Medicine’s Unequal Treatment Report identified variability in provider clinical decision-making based upon race and ethnicity, which resulted in healthcare disparities.[34] In a quantitative study of 164 medical students, when an African-American female patient and a Caucasian male patient actor both enacted the same symptoms of angina, medical students were more likely to believe that the Caucasian patient had true angina, especially when the medical students were also of Caucasian race.[35] Similarly in a quantitative survey study, 720 physicians randomized to clinical vignettes with patients of different races perceived known life-saving treatments to be less appropriate in racial minorities.[36] In another survey study, 284 nephrologists felt that renal transplants would be less effective in improving survival in African-Americans than in Caucasians, and believed that African-Americans were offered transplants less often due to patient preferences rather than physician bias.[37]
A multi-targeted approach is needed to reduce racial/ethnic differences in physician clinical decision-making. Both theoretical and evidence-based methods are available for each of the six derived themes of this meta-synthesis. First, there are differing viewpoints on the importance of race during a physician-patient interaction, including what race means and how it should be used. This can be addressed with physician cultural education during training and practicing years, which has been associated with improved patient outcomes.[34, 38–40] Cultural training includes training in perspective-taking, seeking common group identities, teaching skepticism with race-based differences in care, increasing awareness of structural racism and inequality.[38, 41] Second, patient-level issues related to socioeconomic position occur more frequently in racial/ethnic minorities.[42, 43] Usage of a social worker or community liaison has assisted with meeting patient specific needs.[40, 44–47] Also treating the patient as an individual rather than as a collective group of people may reduce racial/ethnic disparities in care.[39, 48, 49] Third, healthcare system-level issues must be addressed. Decreasing stressors that increase a physician’s cognitive load (i.e. large patient cohort, short period of time to see patients, dysfunctional computer system) and evaluating for systematic differences in healthcare delivery have been associated with more equitable care.[48, 50] Fourth, bias and racism exist from individual levels through societal infrastructure.[48] Multiple approaches associated with reduction in bias and racism in the patient-physician interaction include: promoting intergroup relationships and egalitarian views,[38, 50, 51] perspective shifting education that may alter bias,[52] providing bias education and training,[38, 49, 53] increasing objectivity through guidelines-based care,[34, 50, 54] and an emerging method that implements reflective group decision-making.[55] Fifth, patient’s values should be considered. Similar to the approach for patient-level issues, each patient’s care should be individualized rather than generalized to racial/ethnic stereotypes.[39, 48, 49] Sixth, communication should be a focus for reducing racial/ethnic disparities. This requires an improved perspective on marginalized patient groups and willingness to identify ways to communicate in the patient’s language.[38, 56] In summary, because of the interrelated themes, eradicating a single factor or theme would not inhibit the system of racial/ethnic health inequality. Multiple simultaneous interventions are indicated for each theme.
Several limitations of this work should be considered. First, the primary data for each study were not accessible. Analyses are based upon the selected data that were published in each manuscript, which is an inherent limitation to meta-syntheses. However, most of the selected manuscripts included substantial quotes that would allow for consistent thematic assessment. Second, the clinical decision-making process for healthcare is a shared pathway between physicians and patients. The patient perspective is not provided in this meta-synthesis. We chose to focus on the clinician perspectives since numerous qualitative studies have evaluated the perspective of racial and ethnic minority patients. Third, most studies did not denote evaluation for saturation during thematic analysis nor did researchers identify relationships to participants. Although this may result in response bias, the consistency of themes across multiple studies suggests appropriate sampling and precise results. Lastly, this meta-synthesis focuses on African-American and Hispanic minority patients since they have well-documented health disparities.[20] Results may not be generalizable to other racial and ethnic minorities. However, approaches for providing equitable objective healthcare may be useful for all racial and ethnic groups and may extend to other intersections with race and ethnicity like sex, socioeconomic position, and creed.
CONCLUSION
In this qualitative meta-synthesis of physician perceptions, we found that physicians perceive that a patient’s race and ethnicity factored into the physician clinical decision-making process, predominantly in a negative way. Themes were nonhierarchical, interrelated, and potentiating. The themes included understanding the importance of race, patient-level issues, system-level issues, bias and racism, patient values, and communication. Future steps in developing health equity among racial and ethnic minority patients should include application of multi-targeted interventions for each factor simultaneously. A structured institutional strategy to implement new interventions will require buy-in from hospital administrators, healthcare providers, trainees, and community stakeholders.
Supplementary Material
Acknowledgments
Funding: Dr. Breathett received support from the American Heart Association (AHA) Strategically Focused Research Network (#16SFRN29640000), the National Institute of Health (NIH) L60 MD010857, the University of Colorado Department of Medicine, Health Services Research Development Grant Award, and the University of Arizona Health Sciences, Strategic Priorities Faculty Initiative Grant. Dr. Jones received support from the Agency for Healthcare Research and Quality (K08HS024569). Dr. Peterson discloses grant funding from the AHA. Otherwise there are no disclosures.
Footnotes
COMPLIANCE WITH ETHICAL STANDARDS:
Conflict of Interest: None
Ethical approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent: Not applicable. This was a retrospective study of previously published publicly available manuscripts.
References
- 1.Cassel CK, Guest JA. Choosing Wisely: Helping Physicians and Patients Make Smart Decisions About Their Care. JAMA. 2012;307:1801–1802. doi: 10.1001/jama.2012.476. [DOI] [PubMed] [Google Scholar]
- 2.Bate L, Hutchinson A, Underhill J, Maskrey N. How clinical decisions are made. Br J Clin Pharmacol. 2012;74:614–620. doi: 10.1111/j.1365-2125.2012.04366.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hajjaj F, Salek M, Basra M, Finlay A. Non-clinical influences on clinical decision-making: a major challenge to evidence-based practice. J R Soc Med. 2010;103:178–187. doi: 10.1258/jrsm.2010.100104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ross JS. Promoting Evidence-Based High-Value Health Care. JAMA Intern Med. 2015;175:1564–1564. doi: 10.1001/jamainternmed.2015.3543. [DOI] [PubMed] [Google Scholar]
- 5.Chapman EN, Kaatz A, Carnes M. Physicians and Implicit Bias: How Doctors May Unwittingly Perpetuate Health Care Disparities. J Gen Intern Med. 2013;28:1504–1510. doi: 10.1007/s11606-013-2441-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Blair IV, Steiner JF, Fairclough DL, et al. Clinicians’ Implicit Ethnic/Racial Bias and Perceptions of Care Among Black and Latino Patients. Ann Fam Med. 2013;11:43–52. doi: 10.1370/afm.1442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sabin J, Nosek BA, Greenwald A, Rivara FP. Physicians’ implicit and explicit attitudes about race by MD race, ethnicity, and gender. J Health Care Poor Underserved. 2009;20:896–913. doi: 10.1353/hpu.0.0185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Cooper LA, Roter DL, Carson KA, et al. The associations of clinicians’ implicit attitudes about race with medical visit communication and patient ratings of interpersonal care. Am J Public Health. 2012;102:979–987. doi: 10.2105/AJPH.2011.300558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Johnson TJ, Winger DG, Hickey RW, et al. A comparison of physician implicit racial bias towards adults versus children. Acad Pediatr. 2016 doi: 10.1016/j.acap.2016.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Blair IV, Steiner JF, Havranek EP. Unconscious (Implicit) Bias and Health Disparities: Where Do We Go from Here? Perm J. 2011;15:71–78. doi: 10.7812/tpp/11.979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Balsa AI, McGuire TG. Prejudice, clinical uncertainty and stereotyping as sources of health disparities. J Health Econ. 2003;22:89–116. doi: 10.1016/s0167-6296(02)00098-x. [DOI] [PubMed] [Google Scholar]
- 12.Haider AH, Sexton J, Sriram N, et al. Association of Unconscious Race and Social Class Bias With Vignette-Based Clinical Assessments by Medical Students. JAMA. 2011;306:942–951. doi: 10.1001/jama.2011.1248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Haider AH, Schneider EB, Sriram N, et al. Unconscious race and social class bias among acute care surgical clinicians and clinical treatment decisions. JAMA Surg. 2015;150:457–464. doi: 10.1001/jamasurg.2014.4038. [DOI] [PubMed] [Google Scholar]
- 14.Plaisime MV, Malebranche DJ, Davis AL, Taylor JA. Healthcare Providers’ Formative Experiences with Race and Black Male Patients in Urban Hospital Environments. J Racial Ethn Health Disparities. 2016 doi: 10.1007/s40615-016-0317-x. [DOI] [PubMed] [Google Scholar]
- 15.Snipes SA, Sellers SL, Tafawa AO, et al. Is race medically relevant? A qualitative study of physicians’ attitudes about the role of race in treatment decision-making. BMC Health Serv Res. 2011;11:183. doi: 10.1186/1472-6963-11-183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Tong A, Flemming K, McInnes E, et al. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med Res Methodol. 2012;12:181. doi: 10.1186/1471-2288-12-181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097. doi: 10.1371/journal.pmed.1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Letts L, Wilkins S, Law M, et al. Guidelines for critical review form: Qualitative studies (Version 2.0) McMaster University Occupational Therapy Evidence-Based Practice Research Group; 2007. https://www.canchild.ca/system/tenon/assets/attachments/000/000/360/original/qualguide.pdf. [Google Scholar]
- 19.Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008;8:45. doi: 10.1186/1471-2288-8-45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Disparities in Healthcare Quality Among Racial and Ethnic Minority Groups. [Accessed 3 May 2017];AHRQ Archive. https://archive.ahrq.gov/research/findings/nhqrdr/nhqrdr10/minority.html.
- 21.Walsh D, Downe S. Meta-synthesis method for qualitative research: a literature review. J Adv Nurs. 2005;50:204–211. doi: 10.1111/j.1365-2648.2005.03380.x. [DOI] [PubMed] [Google Scholar]
- 22.Bonham VL, Sellers SL, Gallagher TH, et al. Physicians’ attitudes towards race, genetics and clinical medicine. Genet Med Off J Am Coll Med Genet. 2009;11:279–286. doi: 10.1097/GIM.0b013e318195aaf4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Braun UK, Ford ME, Beyth RJ, McCullough LB. THE PHYSICIAN’S PROFESSIONAL ROLE IN END-OF-LIFE DECISION MAKING: VOICES OF RACIALLY AND ETHNICALLY DIVERSE PHYSICIANS. Patient Educ Couns. 2010;80:3–9. doi: 10.1016/j.pec.2009.10.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Clark-Hitt R, Malat J, Burgess D, Friedemann-Sanchez G. Doctors’ and nurses’ explanations for racial disparities in medical treatment. J Health Care Poor Underserved. 2010;21:386–400. doi: 10.1353/hpu.0.0275. [DOI] [PubMed] [Google Scholar]
- 25.Frank D, Gallagher TH, Sellers SL, et al. Primary care physicians’ attitudes regarding race-based therapies. J Gen Intern Med. 2010;25:384–389. doi: 10.1007/s11606-009-1190-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Goodman MJ, Ogdie A, Kanamori MJ, et al. Barriers and facilitators of colorectal cancer screening among Mid-Atlantic Latinos: focus group findings. Ethn Dis. 2006;16:255–261. [PubMed] [Google Scholar]
- 27.Johansson P, Jones DE, Watkins CC, et al. Physicians’ and nurses’ experiences of the influence of race and ethnicity on the quality of healthcare provided to minority patients, and on their own professional careers. J Natl Black Nurses Assoc JNBNA. 2011;22:43–56. [PubMed] [Google Scholar]
- 28.Mott-Coles S. Patients’ Cultural Beliefs in Patient-Provider Communication With African American Women and Latinas Diagnosed With Breast Cancer. Clin J Oncol Nurs. 2014;18:443–448. doi: 10.1188/14.CJON.443-448. [DOI] [PubMed] [Google Scholar]
- 29.Nunez-Smith M, Curry LA, Berg D, et al. Healthcare workplace conversations on race and the perspectives of physicians of African descent. J Gen Intern Med. 2008;23:1471–1476. doi: 10.1007/s11606-008-0709-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Owsley C, McGwin G, Scilley K, et al. Perceived barriers to care and attitudes about vision and eye care: focus groups with older African Americans and eye care providers. Invest Ophthalmol Vis Sci. 2006;47:2797–2802. doi: 10.1167/iovs.06-0107. [DOI] [PubMed] [Google Scholar]
- 31.Park ER, Betancourt JR, Kim MK, et al. Mixed messages: residents’ experiences learning cross-cultural care. Acad Med J Assoc Am Med Coll. 2005;80:874–880. doi: 10.1097/00001888-200509000-00019. [DOI] [PubMed] [Google Scholar]
- 32.Ward SH, Parameswaran L, Bass SB, et al. Resident physicians’ perceptions of barriers and facilitators to colorectal cancer screening for African Americans. J Natl Med Assoc. 2010;102:303–311. doi: 10.1016/s0027-9684(15)30602-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Garcia-Retamero R, Galesic M. On defensive decision making: how doctors make decisions for their patients. Health Expect Int J Public Particip Health Care Health Policy. 2014;17:664–669. doi: 10.1111/j.1369-7625.2012.00791.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Smedley B, Stith A, Nelson A. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care (with CD) Institute of Medicine; 2003. [PubMed] [Google Scholar]
- 35.Rathore SS, Lenert LA, Weinfurt KP, et al. The effects of patient sex and race on medical students’ ratings of quality of life. Am J Med. 2000;108:561–566. doi: 10.1016/s0002-9343(00)00352-1. [DOI] [PubMed] [Google Scholar]
- 36.Schulman KA, Berlin JA, Harless W, et al. The effect of race and sex on physicians’ recommendations for cardiac catheterization. N Engl J Med. 1999;340:618–626. doi: 10.1056/NEJM199902253400806. [DOI] [PubMed] [Google Scholar]
- 37.Ayanian JZ, Cleary PD, Keogh JH, et al. Physicians’ beliefs about racial differences in referral for renal transplantation. Am J Kidney Dis Off J Natl Kidney Found. 2004;43:350–357. doi: 10.1053/j.ajkd.2003.10.022. [DOI] [PubMed] [Google Scholar]
- 38.Zestcott CA, Blair IV, Stone J. Examining the Presence, Consequences, and Reduction of Implicit Bias in Health Care: A Narrative Review. Group Process Intergroup Relat GPIR. 2016;19:528–542. doi: 10.1177/1368430216642029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Anderson MR, Moscou S, Fulchon C, Neuspiel DR. The role of race in the clinical presentation. Fam Med. 2001;33:430–434. [PubMed] [Google Scholar]
- 40.Quiñones AR, O’Neil M, Saha S, et al. Interventions to Improve Minority Health Care and Reduce Racial and Ethnic Disparities. Department of Veterans Affairs (US); Washington (DC): 2011. [PubMed] [Google Scholar]
- 41.Metzl JM, Roberts DE. Structural Competency Meets Structural Racism: Race, Politics, and the Structure of Medical Knowledge. Virtual Mentor. 2014;16:674. doi: 10.1001/virtualmentor.2014.16.9.spec1-1409. [DOI] [PubMed] [Google Scholar]
- 42.McMorrow S, Long SK, Kenney GM, Anderson N. Uninsurance Disparities Have Narrowed For Black And Hispanic Adults Under The Affordable Care Act. Health Aff Proj Hope. 2015;34:1774–1778. doi: 10.1377/hlthaff.2015.0757. [DOI] [PubMed] [Google Scholar]
- 43.Breathett K, D’Amico R, Adesanya TMA, et al. Patient Perceptions on Facilitating Follow-Up After Heart Failure Hospitalization. Circ Heart Fail. 2017;10 doi: 10.1161/CIRCHEARTFAILURE.117.004099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Two Feathers J, Kieffer EC, Palmisano G, et al. Racial and Ethnic Approaches to Community Health (REACH) Detroit Partnership: Improving Diabetes-Related Outcomes Among African American and Latino Adults. Am J Public Health. 2005;95:1552–1560. doi: 10.2105/AJPH.2005.066134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Thomas KL, Shah BR, Elliot-Bynum S, et al. Check it, change it: a community-based, multifaceted intervention to improve blood pressure control. Circ Cardiovasc Qual Outcomes. 2014;7:828–834. doi: 10.1161/CIRCOUTCOMES.114.001039. [DOI] [PubMed] [Google Scholar]
- 46.Verhagen I, Steunenberg B, de Wit NJ, Ros WJ. Community health worker interventions to improve access to health care services for older adults from ethnic minorities: a systematic review. BMC Health Serv Res. 2014;14 doi: 10.1186/s12913-014-0497-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Viswanathan M, Kraschnewski JL, Nishikawa B, et al. Outcomes and costs of community health worker interventions: a systematic review. Med Care. 2010;48:792–808. doi: 10.1097/MLR.0b013e3181e35b51. [DOI] [PubMed] [Google Scholar]
- 48.Feagin J, Bennefield Z. Systemic racism and U.S. health care. Soc Sci Med 1982. 2014;103:7–14. doi: 10.1016/j.socscimed.2013.09.006. [DOI] [PubMed] [Google Scholar]
- 49. [Accessed 27 Nov 2017];Implicit Bias Review. http://kirwaninstitute.osu.edu/researchandstrategicinitiatives/implicit-bias-review/
- 50.van Ryn M, Burgess DJ, Dovidio JF, et al. THE IMPACT OF RACISM ON CLINICIAN COGNITION, BEHAVIOR, AND CLINICAL DECISION MAKING. Bois Rev Soc Sci Res Race. 2011;8:199–218. doi: 10.1017/S1742058X11000191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Kawakami K, Phills CE, Steele JR, Dovidio JF. (Close) distance makes the heart grow fonder:Improving implicit racial attitudes and interracial interactions through approach behaviors. J Pers Soc Psychol. 2007;92:957–971. doi: 10.1037/0022-3514.92.6.957. [DOI] [PubMed] [Google Scholar]
- 52.Kubota JT, Banaji MR, Phelps EA. The neuroscience of race. Nat Neurosci. 2012;15:940. doi: 10.1038/nn.3136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Rudman LA, Ashmore RD, Gary ML. “Unlearning” automatic biases: The malleability of implicit prejudice and stereotypes. J Pers Soc Psychol. 2001;81:856–868. doi: 10.1037/0022-3514.81.5.856. [DOI] [PubMed] [Google Scholar]
- 54.Helping courts address implicit bias: Resources for education. National Center for State Courts; [Accessed 4 Oct 2016]. http://www.ncsc.org/ibeducation. [Google Scholar]
- 55.de Groot E, Endedijk M, Jaarsma D, et al. Development of critically reflective dialogues in communities of health professionals. Adv Health Sci Educ Theory Pract. 2013;18:627–643. doi: 10.1007/s10459-012-9403-y. [DOI] [PubMed] [Google Scholar]
- 56.Hardeman RR, Medina EM, Kozhimannil KB. Dismantling Structural Racism, Supporting Black Lives and Achieving Health Equity: Our Role. N Engl J Med. 2016;375:2113–2115. doi: 10.1056/NEJMp1609535. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.