

ABSTRACT
Increasing numbers of international students require Japanese universities to provide mental health support as one of their primary responsibilities. The problem with the provision of such support is that the stigma of mental disorder causes many individuals to avoid seeking help. We aim to clarify the association between stigma and mental illness to develop anti-stigma education. We performed a cross-sectional observational study. The target population comprised international students enrolled in a Japanese university. Online questionnaires were used to assess self-stigma, perceived stigma, recognized knowledge of schizophrenia and depression, gender, country and region, general mental health status, parents’ income, non-clinical and clinical help-seeking attitudes, and Japanese and English language ability. Logistic regression model was used to estimate odds ratios (ORs) for self-stigma and perceived stigma after adjusting for the above factors. A total of 119 students were invited to participate, 61 (51.3%) of whom were enrolled. Students with good knowledge of depression/schizophrenia did not indicate more severe self-stigma compared with those without such knowledge. Students with good knowledge of schizophrenia indicated more severe perceived stigma compared with those without such knowledge (OR 3.78 [95% confidence intervals; CI, 1.21-11.78]). Students with good knowledge of depression indicated less severe perceived stigma compared with those without such knowledge (OR 0.31 [95% CI, 0.10–0.94]). In this study, among international students, higher perceived stigma was associated with knowledge of schizophrenia and lower knowledge of depression.
Key Words: stigma, young adult, mental health, culture, education
INTRODUCTION
The number of foreign students studying in Japan is increasing rapidly under the nation’s globalization policy. Some international students suffer from mental disorders, such as adjustment disorder, depression, and acute psychosis, due to acculturation difficulties including culture gaps.1-3) Problems stemming from these mental disorders require urgent attention so that international students can obtain early mental health support.4) However, there is a stigma associated with mental illness that leads to delay in help seeking behaviors.5-7) Goffman discussed how the stigma of mental illness could be invisible.8) ; that is, the stigma could blemish an individual’s character through mental manifestations. Previous research suggested that the stigma of mental illness is associated with individual attributes; more specifically, males are stigmatized more severely than females, and younger people more so than elderly people.9,10) Additionally, the stigma of mental illness is affected by individual background factors such as one’s social, economic, and educational status.11) Stigma is considered to be related to mental health well-being. Some previous research suggests that public stigma or perceived public stigma are associated with depression.6,12) Their research suggest that social acceptance of people with mental health problems negatively correlated with national suicide rates in 25 European countries, and that the levels of stigma vary among different countries.13) However, another global study found no such differences.14) Thus, there has as yet not been sufficient into global differences in levels of stigma.
Goffman explained that a language of relationships, rather than attributes, is really needed to understand stigma.8) In other words, stigma has been defined in terms of relationships, and should be treated as such.15) The impact of stigma is twofold as it includes negative beliefs about a group or the self.16) Personal stigma involving negative belief about the self is divided into three groups: 1) Self-stigma, 2) Experienced stigma, and 3) Perceived stigma.15) Experienced stigma mainly means experiences of discrimination. Self-stigma refers to what one thinks about mental disorders. Perceived stigma refers to one’s thoughts about how society views mental disorders. However, the differences between self-stigma and perceived stigma have not been made clear.
As yet, no study has mainly focused primarily on stigma among international students after considering possible confounding factors. Here, we address stigma to develop proper anti-stigma education program. In this investigation, we aim to clarify what factors are associated with self-stigma and perceived stigma among international students.
MATERIALS AND METHODS
Study Design
We conducted a cross-sectional study administered via questionnaires at a single institution.
Study Participants
The target population comprised all newly entered international students registered at a certain University in Japan for the 2014 autumn semester.
Questionnaire Survey
All questionnaires were presented in English, because it is an international language. The questionnaire contained items about the students’ attributes, such as age, gender, nationality/region, department affiliation, and parental income. In addition, we assessed how often international students visited the International Student Mobility Division or used the advisory services provided in the International Center. The International Student Mobility Division supports international students’ daily and school lives, while the advisory services provide students opportunities for health consultation with multiple doctors. This information was introduced by the university upon the admission of the international students. Actual usage of the services provided by the International Student Mobility Division reflected the international students’ support-seeking behaviors towards non-clinical issues, whereas their actual usage of advisory service reflects their support-seeking behavior towards clinical issues. Furthermore, we considered language ability in terms of acculturation and language fluency.17) Questions about Japanese and English language abilities were based on the Common European Framework of Reference for Languages.
To assess self-stigma, we used the Self-Stigma of Mental Illness Scale-Short Form (SSMIS-SF) consisting of 10 items; for example, “Seeking psychological help would make me feel less intelligent.”18) To assess perceived stigma, we used the Link Stigma Scale; this scale consists of 12 items, for example, “Most people believe that a person who has been in a mental hospital is just as intelligent as the average person.”19,20) We adopted the 6-item Kessler Psychological Distress Scale (K6) to measure general mental health.21) The K6 is both multiculturally appropriate. We inquired about knowledge of mental illness, specifically, schizophrenia and depression. This self-report questionnaire uses a 4-point rating scale, The SSMIS-SF, Link Stigma Scale, and K6 are standardized measures that are freely available for use without permission.
Statistical Analysis
We established self-stigma and perceived stigma as primary outcomes; accordingly, these were the dependent variables in the analysis. On the other hand, we identified additional factors to use as independent variables to calculate their associations with the primary outcomes. For each of the stigma scales, participants were divided into two categories based on scored above or below pre-determined cutoff scores. Cutoff scores were also used to create dichotomous categories for most of the independent variables, apart from global regions and countries. Therefore, we performed logistic regression model to estimate the odds ratios (ORs) and their 95% confidence intervals (CIs).
Previous research measured SSMIS-SF scores, and found means of 34.0, 26.2, and 32.5, respectively, on the scales that ranged from 10–50 points.22) We determined a cut-off score of 30 points based on these references. Regarding the Link Stigma Scale score, the cut-off of 32 points on a scale with a ranging from 12–48 points was used to divide participants into 2 groups according to a previous distribution for this scale.23) We classified Asia into three regions of China, the Republic of Korea, and other Asian countries based on the international students’ mother countries. Regarding the K6, 14 points ranging from 6–30 points was used to divide participants into 2 groups based on the optimal cut-off points.24) Language ability was divided into 2 groups based on the achievement of “Independent User” status, and the other variables were divided into 2 groups as well.
We determined the following order of analysis. First, we tested the relationship between self-stigma and perceived stigma. If the stigma scales were significantly related, both variables would be submitted together into the same analysis models. Then, we used analysis of covariance to assess self-stigma and perceived stigma among the global regions and countries. Finally, other variables would be submitted into the analysis models to adjust for the following confounding factors: gender, country and region, knowledge of each mental illness, mental health status, economic status, non-clinical and clinical help-seeking attitude, and Japanese and English language ability.
Analyses were performed using Stata 14.2 software (Stata Corporation, College Station, Tex., USA). All tests of significance were 2-tailed, and p values < 0.05 were considered statistically significant. This investigation was approved by the Ethics Committee of the Kyoto University Graduate School of Medicine (E2265).
RESULTS
A total of 119 newly admitted students for the 2014 autumn semester were invited to participate. These are the details of the programs: 52 students from the International Education Program, 26 from the General Exchange Program, 19 from the Japanese Studies Program, 15 from the Intensive Japanese Language Course for the Monbukagakusho Scholarship, and 7 from the Japan-Korea Joint Program (Science and Engineering). Of these, 61 (51.3%) were enrolled in this study (Table 1).
Table 1.
Characteristics of participants
| Total number | 61 | |
| Males | 21 (34.4) | |
| Age (years old as of April 1, 2014) | Average (Standard Deviation) | 23.4 (4.1) |
| Country or region | European Union | 19 (31.1) |
| China | 18 (29.5) | |
| Republic of Korea | 9 (14.8) | |
| The Other Asian regions | 6 (9.8) | |
| The Middle and South America regions | 3 (4.9) | |
| The North America regions | 2 (3.3) | |
| The Oceania regions | 2 (3.3) | |
| Others | 2 (3.3) | |
| Status | International Education Program student | 21 (34.4) |
| Japanese Studies Program student | 13 (21.3) | |
| Research student/Auditing student | 9 (14.8) | |
| General Exchange Program student | 6 (9.8) | |
| Undergraduate student | 4 (6.6) | |
| Short-Term International student | 4 (6.6) | |
| Others | 4 (6.6) | |
| Academic affiliation | International Center | 23 (37.7) |
| Integrated Human Studies, Human and Environmental Studies | 16 (26.2) | |
| Letters | 4 (6.6) | |
| Economics | 3 (4.9) | |
| Science | 3 (4.9) | |
| Engineering | 3 (4.9) | |
| Education | 2 (3.3) | |
| Pharmaceutical Science | 1 (1.6) | |
| Asian and African Areas Studies | 1 (1.6) |
Values are expressed in numbers (percentage except Standard Deviation).
On the other hand, 58 newly admitted students did not participate in this study. These are their native regions: European Union 22 (18.5%), China 8 (6.7%), Republic of Korea 10 (8.4%), Other Asian regions 8 (6.7%), Central and South American regions 2 (1.7%), North American regions 8 (6.7%), Oceania 0 (0%), and Others 0 (0%). A detailed summary of the self-stigma descriptive statistics is as follows: observation number 57; mean score 28.4 (Standard Division: SD = 3.10); maximum/minimum score = 35 / 19. A detailed summary of the perceived stigma descriptive statistics is as follows: observation number 56; mean score 31.0 (SD = 2.28); maximum/minimum score = 37 / 24. We described a simple scatter plot between self-stigma score and perceived stigma score (Fig. 1). The correlation between perceived self-stigma score and self-stigma score was not significant (r = 0.024).
Fig. 1.
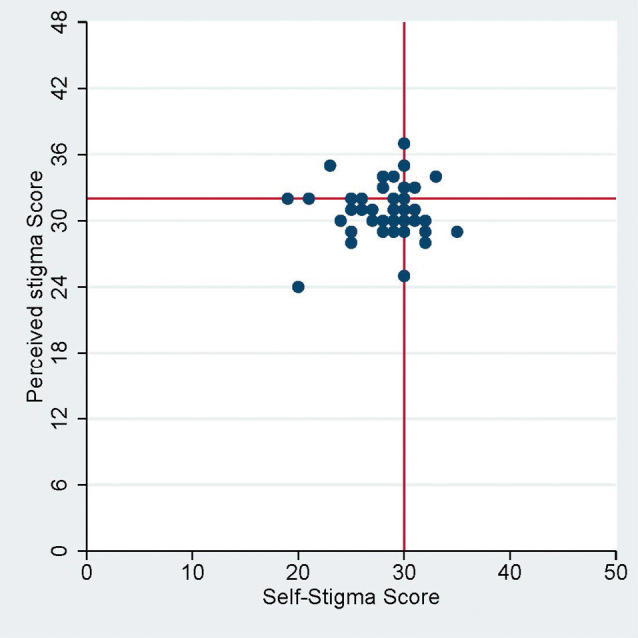
Scatter plot of self-stigma scores and perceived stigma scores
Cut-off score set at 30 points for the SSMIS-SF and 32 points for the Link stigma scale.
We illustrated the plots for the self-stigma and perceived stigma score among the global regions and individual countries (Fig. 2 and 3). There were no significant differences among regions and countries in either self-stigma or perceived stigma (p = 0.30, and p = 0.25, respectively).
Fig. 2.
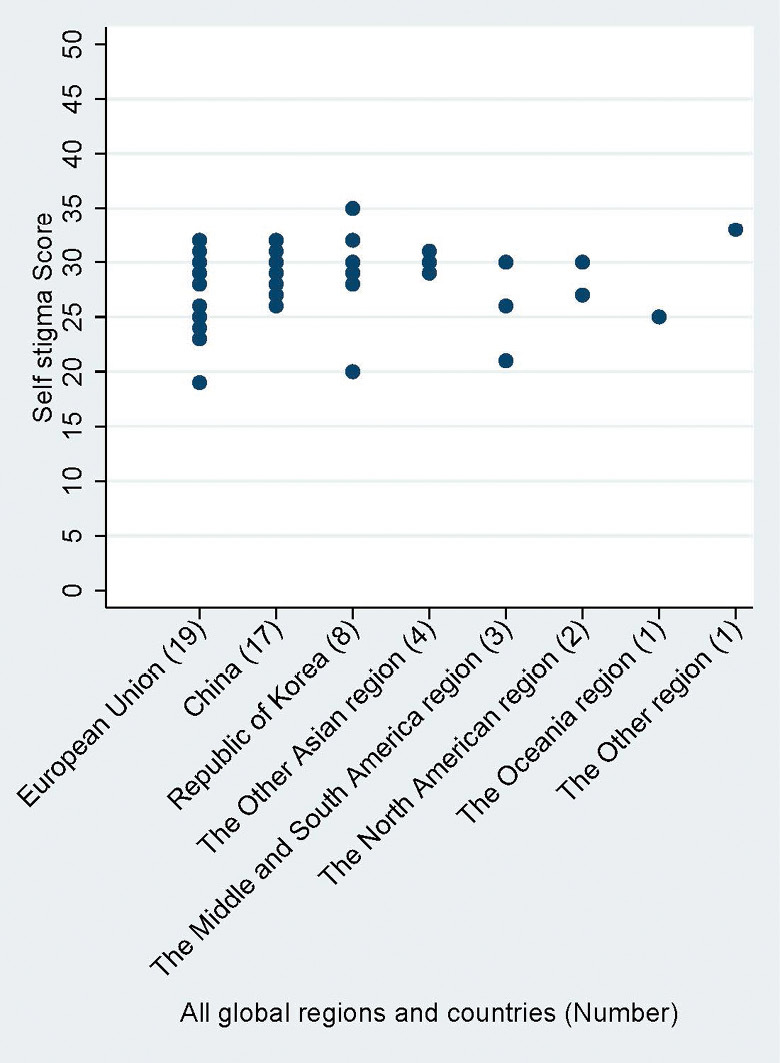
Self-stigma for all global regions and countries
Fig. 3.
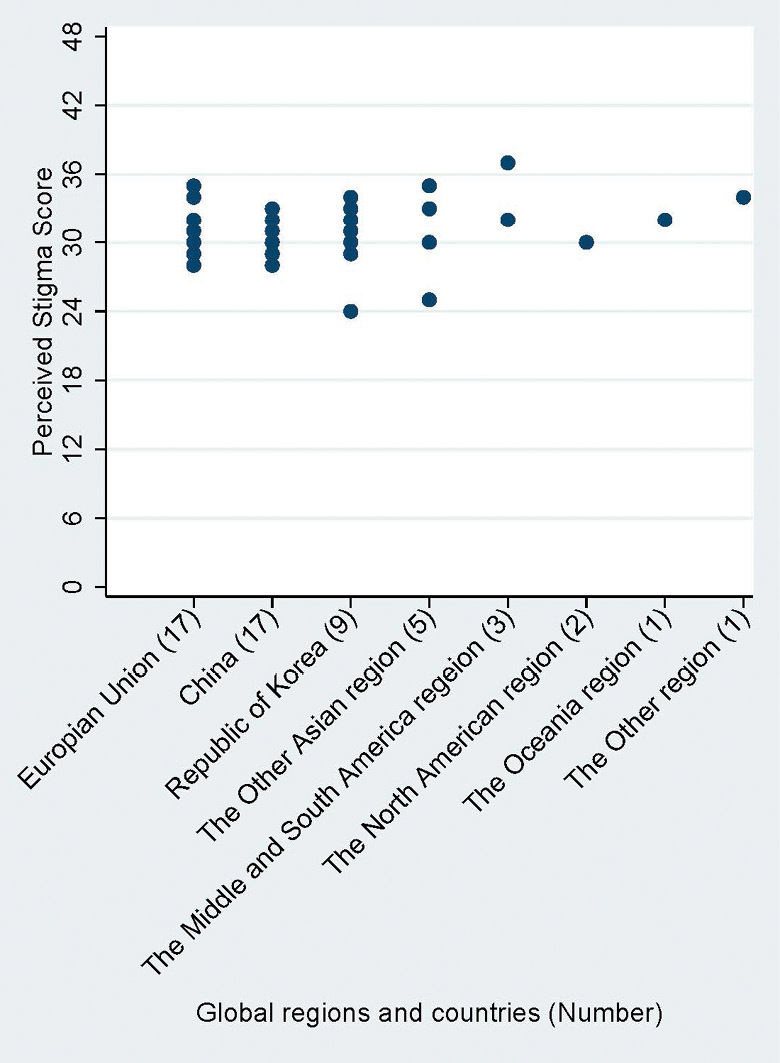
Perceived stigma for all global regions and countries
We illustrated the K6 score distribution of with a bar chart (Fig. 4). A detailed summary of these descriptive statistics as follows: observation number 60; mean score 10.9 (SD = 3.43); maximum/minimum score = 21 / 6. Individuals with a K6 score of 14 or more were said to have mental health risks; these people normally represent 10% of the general population. In this study, 18.3% (11 / 60) of the sample scored over this threshold.
Fig. 4.
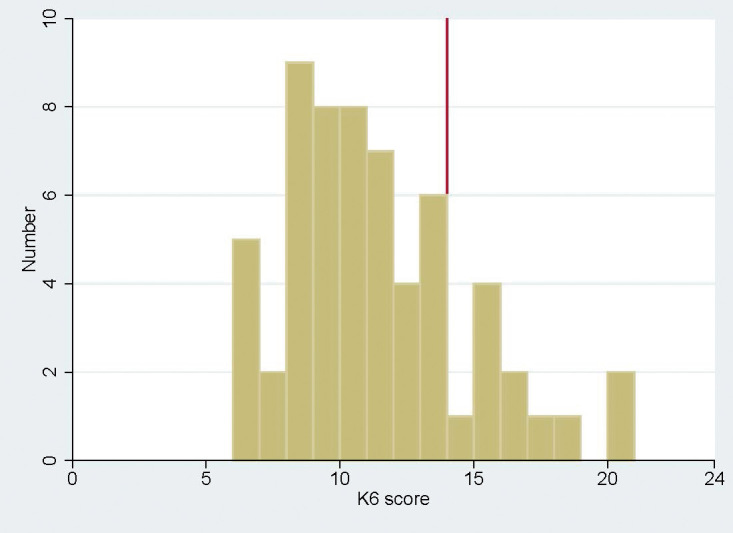
Distribution of K6 scores
Cut-off score set at 14 points.
Factors associated with self-stigma are shown in Table 2. Students having good knowledge of either schizophrenia or depression did not have more severe self-stigma (OR 1.05 [95% CI, 0.37–3.00], and OR 1.27 [95% CI, 0.44–3.71], respectively). Additionally, none of the other factors was associated with either more severe perceived or self-stigma. Factors associated with perceived stigma are shown in Table 3. Students having good knowledge of schizophrenia had significantly more severe perceived stigma compared with students not having such knowledge (OR 3.78 [95% CI, 1.21–11.78]). However, students having good knowledge of depression had significantly less severe perceived stigma (OR 0.31 [95% CI, 0.10–0.94]).
Table 2.
Factors associated with higher self-stigma
| The group with higher self-stigma score (more than 30, n = 24) (%) | The group with lower self-stigma score (less than 30, n = 33) (%) | Crude odds ratio (95%CI) (n = 57) | Adjusted odds ratio (95%CI) (n = 55) | |
|---|---|---|---|---|
| Having knowledge of schizophrenia (over 4 grades†) | grade4; 3 (33.3),
grade3; 7 (50.0), grade2; 8 (44.4), grade1; 6 (37.5) |
grade4; 6 (66.7),
grade3; 7 (50.0), grade2; 10 (55.6), grade1; 10 (62.5) |
1.02 (0.61–1.69) | 1.05 (0.37–3.00) |
| Having knowledge of depression (over 4 grades†) | grade4; 9 (50.0),
grade3; 6 (35.3), grade2; 4 (36.4), grade1; 5 (45.5) |
grade4; 9 (50.0),
grade3; 11 (64.7), grade2; 7 (63.6), grade1; 6 (54.6) |
1.08 (0.67–1.75) | 1.27 (0.44–3.71) |
| Gender (males or not) | 16 (66.7) | 20 (60.6) | 0.77 (0.26–2.31) | 1.03 (0.26–4.07) |
| Country and region (Asia or not) | 16 (66.7) | 15 (45.5) | 2.40 (0.81–7.14) | 2.05 (0.54–7.81) |
| Higher K6 score (more than 14) | 5 (20.8) | 4 (n=32) (12.5) | 1.84 (0.44–7.76)
(n=56) |
2.23 (0.25–19.71) |
| The annual income of parents or guardians in the home country (more than moderate) | 18 (75.0) | 21 (n=32) (63.6) | 1.57 (0.48–5.10)
(n=56) |
1.60 (0.44–5.86) |
| I often use the International Center or the International Student Mobility Division. (once a week or more) | 10 (41.7) | 11 (33.3) | 1.43 (0.48–4.24) | 1.69 (0.424–6.51) |
| In the future, I want to make use of the advisory services in health concerns. | 6 (25.0) | 10 (30.3) | 0.77 (0.23–2.51) | 0.15 (0.415–2.83) |
| Language ability in Japanese (Independent user or further) | 14 (58.3) | 21 (63.6) | 0.38 (0.08–1.78) | 0.67 (0.18–2.44) |
| Language ability in English (Independent user or further) | 19 (86.0) | 30 (90.9) | 0.80 (0.27–2.35) | 0.39 (0.06–2.71) |
As a result of adjusting all displayed factors for each other by multivariate logistic regression analysis, each factor indicates an independent value for the adjusted odds ratio.
†grade4; Know well, grade3; Know a little, grade2; Don’t know very much, and grade1; Not at all.
Table 3.
Factors associated with higher perceived stigma
| The group with higher perceived stigma score (more than 32, n = 23) (%) | The group with lower perceived stigma score (less than 32, n = 33) (%) | Crude odds ratio (95%CI) (n = 55) | Adjusted odds ratio (95%CI) (n = 55) | |
|---|---|---|---|---|
| Having knowledge of schizophrenia (over 4 grades†) | grade4; 3 (42.9),
grade3; 8 (53.3), grade2; 7 (38.9), grade1; 5 (31.2) |
grade4; 4 (57.1),
grade3; 7 (46.7), grade2; 11 (61.1), grade1; 11 (68.8) |
1.31 (0.77–2.25) | 3.78 (1.21–11.78)* |
| Having knowledge of depression (over 4 grades†) | grade4; 5 (31.2),
grade3; 8 (47.1), grade2; 6 (50.0), grade1; 4 (36.4) |
grade4; 11 (68.8),
grade3; 9 (52.9), grade2; 6 (50.0), grade1; 7 (63.6) |
0.90 (0.55–1.48) | 0.31 (0.10– 0.94)* |
| Gender (males or not) | 14 (60.9) | 24 (72.7) | 1.71 (0.55–5.33) | 1.01 (0.24–4.29) |
| Country and region (Asia or not) | 11 (47.8) | 21 (63.6) | 0.52 (0.18–1.55) | 0.44 (0.11–1.81) |
| Higher K6 score (more than 14) | 4 (17.4) | 6 (n = 32) (18.8) | 2.25 (0.25–20.1) | 3.34 (0.49–22.82) |
| The annual income of parents or guardians in the home country (more than moderate) | 15 (65.2) | 24 (72.7) | 0.70 (0.22–2.22) | 0.95 (0.26–3.41) |
| I often use the International Center or the International Student Mobility Division (once a week or more) | 9 (39.1) | 14 (42.4) | 0.87 (0.29–2.58) | 0.95 (0.26–3.41) |
| In the future, I want to make use of the advisory services in health concerns. | 6 (26.1) | 11 (33.3) | 0.71 (0.22–2.29) | 0.63 (0.14–2.78) |
| Language ability in Japanese (Independent User or further) | 14 (60.9) | 20 (60.6) | 1.28 (0.33–5.00) | 1.25 (0.34– 4.65) |
| Language ability in English (Independent User or further) | 19 (82.6) | 26 (78.8) | 1.01 (0.34–3.01) | 1.98 (0.31–12.50) |
As a result of adjusting all displayed factors for each other by multivariate logistic regression analysis, each factor indicates an independent value for the adjusted odds ratio.
*p < 0.05.
†grade4; Know well, grade3; Know a little, grade2; Don’t know very much, and grade1; Not at all.
DISCUSSION
The results of this investigation clarified associations between perceived stigma and knowledge of each mental disease among international students. From these results, it is possible to describe the correlations among two kinds of stigma, global regions and individual countries, and mental health status, as is detailed below.
Correlation between Self-stigma and Perceived Stigma
The results suggested no significant correlation between self-stigma and perceived stigma, which was in contrast to results from a previous study.7) We speculate that this investigation, which used the same questionnaire, may have changed the subject of their survey of self-stigma and perceived stigma. As such, this result might not correlate with individual questionnaires responses for each stigma.
Self-stigma and perceived stigma did not significantly differ among the global regions and individual countries. Previous sporadic research controversially suggested different levels of mental illness stigma among several countries.25–28) On the other hand, global surveys of 20 or more countries have not shown significant differences.13,14) Our survey was also conducted on a vast global scale; therefore, it is not surprising that we achieved similar results.
The Risk of Mental Health for International Students
The K6 score results suggest that international students did not have complete mental health well-being. With the K6 cut off point of 14 or higher, it is assumed that approximately 10% of the general population experience mental health risks. We suggest that the proportion is higher among international students (18.3%; see Fig. 4). This might be because the new international students were tired and anxious just after their arrival in Japan. On the other hand, there was no association between both stigma and mental health status. A previous randomized control trial of anti-stigma education resulted in no improvement in K10 scores after anti-stigma education with e-learning.29) Accordingly, mental health status may affect stigma later. We previously interviewed local students before arrival who participated in an international exchange program; we found that they were noticeably exhausted.30) This exhaustion may enhance mental health risk for international students. Therefore, we suggest mental health screening by physicians before participation in a study abroad programs.30) Furthermore, we recommend anti-stigma education focused on increasing knowledge of mental illnesses.
Association between Stigma and Knowledge of Mental Illness
Self-stigma might not be affected after knowledge of either schizophrenia or depression is acquired. However, perceived stigma might increase after knowledge of schizophrenia is acquired. Additionally, perceived stigma might decrease after knowledge of depression is acquired. Many people can better understand symptoms of depression. In contrast, many people have difficulty understanding symptoms of schizophrenia. This is because they are aware of the danger and unpredictability of schizophrenia compared to depression.31) Some previous research suggested that the perceived stigma of schizophrenia is more severe than that of depression.32,33) Furthermore, the stigma of schizophrenia is enhanced when causative biological factors are clarified.34-37) In other words, increased psychiatric awareness increases the severity of the perceived stigma of schizophrenia.32)
Anti-stigma Education
Our results suggest that anti-stigma education has great difficulty in reducing the perceived stigma of schizophrenia. Previous research involving a meta-analysis of randomized controlled trials supports this finding.38) To solve this dilemma, we suggest an improvement in education centered on mental health literacy, showing that mental stress that can promote the onset of schizophrenia. We also believe it necessary to increase knowledge of depression to prevent it. Thus, we recommend a more thorough examination of international students before they enroll in the academic program to provide greater enlightenment concerning their unique cases. To this end, we aim to launch an anti-stigma education campaign.
Study Limitations
As with any study, some limitations must be acknowledged. First, the population of our study has three problems from the viewpoint of internal validity. A cross-sectional observational study cannot reveal causal relationships. The findings of this study reveal only associations between perceived stigma of schizophrenia or depression and having knowledge of schizophrenia or depression, respectively. Therefore, the results of this study may be contaminated with selection bias because of country and regional differences, especially concerning China and the North American regions, between participants and non-participants. We also have subjective problems with another aspect of internal validity. Response biases might distort the self-administered questionnaire results as a result of subjective impressions, especially, concerning the questionnaire assessing knowledge of schizophrenia and depression. Perhaps, subjective recognition of these illnesses might only indicate a broad interest in them.39-42)
Second, there is a problem in terms of external validity. This study may not be representative of all international students in Japan. For instance, Chinese students make up the greatest numbers of international students in the country: At the university, 895 out of the 1,887 international students (47.4%) in October 2014 (data not shown) were Chinese, while overall in Japan, 94,399 out of 184,155 international students (51.3%) in May 2014 were Chinese.39) In our survey, however, only 18 of the 61 students (29.5%) were Chinese.43)
Conclusion
Despite its several limitations, the findings of our current study still point coherently to the following conclusion: among international students, higher perceived stigma is associated with higher knowledge of schizophrenia and lower knowledge of depression.
CONFLICT OF INTEREST
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
ACKNOWLEDGEMENTS
We would like to thank Professor Toshiya Murai, and Assistant Professor Hisaya Kawagishi of Department of Psychiatry Kyoto University Graduate School of Medicine; Honorary Professor Mariko Mori of Kyoto University; Professor Junko Kawai, and Associate Professor Taro Iemoto of Kyoto University Institute for Liberal Arts and Sciences, the Education Center for Japanese Language and Culture; and Contract Senior Lecturer Yuki Sasaki of the Center for Global Partnerships and Education, Okayama University for setting up research fields. Sincere gratitude must also be given to Professor Takashi Kawamura of Kyoto University Health Services for providing us with helpful advice.
This work was supported by JSPS KAKENHI [Grant-in-Aid for Scientific Research on Innovative Areas] Grant Number JP17H05925 and JSPS KAKENHI [Grant-in-Aid for Scientific Research (C)] Grant Number JP15K01650.
REFERENCES
- 1).Kawagishi H, Takeuchi J, Sakagami Y. High-risk factors for abandoning exchange programs midway: a case series. Campus Health, 2015; 52: 113–118. [Article in Japanese]
- 2).Stewart L, Leggat PA. Culture shock and travelers. J Travel Med, 1998; 5: 84–88. [PMID: 9772322] [Retrieved April 13, 2017.] Available from: http://onlinelibrary.wiley.com/doi/10.1111/j.1708-8305.1998.tb00469.x/epdf. [DOI] [PubMed]
- 3).Sam DL, Eide R. Survey of mental health of foreign students. Scand J Psychol, 1991; 32: 22–30. [PMID: 2047794] [DOI] [PubMed]
- 4).Sakagami Y, Uwatoko T, Takeuchi J. Mental health issues in international students at Kyoto University: A retrospective cohort study. Journal of International Student Advisors and Educators, 2014; 17: 7–18. [Retrieved April 13, 2017.] Available from: http://coisan.org/journal/archives/journal017.pdf.
- 5).Mojtabai R. Mental illness stigma and willingness to seek mental health care in the European Union. Soc Psychiatry Psychiatr Epidemiol, 2010; 45: 705–712. [PMID: 19680588] [DOI] [PubMed]
- 6).Yap MB, Reavley NJ, Jorm AF. Associations between stigma and help-seeking intentions and beliefs: findings from an Australian national survey of young people. Psychiatry Res, 2013; 210: 1154–1160. [http://dx.doi.org/10.1016/j.psychres.2013.08.029] [PMID: 24011848]. [DOI] [PubMed]
- 7).Eisenberg D, Downs MF, Golberstein E, Zivin K. Stigma and help seeking for mental health among college students. Med Care Res Rev, 2009; 66: 522–541. [PMID: 19454625] [DOI] [PubMed]
- 8).Goffman E. Stigma: Notes on the Management of Spoiled Identity. 1963, Middlesex: Penguin Books, Harmondsworth.
- 9).Holzinger A, Floris F, Schomerus G, Carta MG, Angermeyer MC. Gender differences in public beliefs and attitudes about mental disorder in western countries: a systematic review of population studies. Epidemiol Psychiatr Sci, 2012; 21: 73–85. [PMID: 22670415] [DOI] [PubMed]
- 10).Stuart H, Patten SB, Koller M, Modgill G, Liinamaa T. Stigma in Canada: results from a rapid response survey. Can J Psychiatry, 2014; 59: S27–33. [PMID: 25565699] [Retrieved April 13, 2017.] Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4213749/. [DOI] [PMC free article] [PubMed]
- 11).von dem Knesebeck O, Mnich E, Daubmann A, Wegscheider K, Angermeyer MC, Lambert M, et al. Socioeconomic status and beliefs about depression, schizophrenia and eating disorders. Soc Psychiatry Psychiatr Epidemiol, 2013; 48: 775–782. [PMID: 23052428] [DOI] [PubMed]
- 12).Pyne JM, Kuc EJ, Schroeder PJ, Fortney JC, Edlund M, Sullivan G. Relationship between perceived stigma and depression severity. J Nerv Ment Dis, 2004; 192: 278–283. [DOI] [PubMed]
- 13).Schomerus G, Evans-Lacko S, Rüsch N, Mojtabai R, Angermeyer MC, Thornicroft G. Collective levels of stigma and national suicide rates in 25 European countries. Epidemiol Psychiatr Sci, 2015; 24: 166–171. [http://dx.doi.org/10.1017/S2045796014000109] [PMID: 24576648] [DOI] [PMC free article] [PubMed]
- 14).Thornicroft G, Brohan E, Rose D, Sartorius N, Leese M; INDIGO Study Group. Global pattern of experienced and anticipated discrimination against people with schizophrenia: a cross-sectional survey. Lancet, 2009; 373: 408–415. [http://dx.doi.org/10.1016/S0140-6736(08)61817-6] [PMID: 19162314] [DOI] [PubMed]
- 15).Corrigan PW, Watson AC. Understanding the impact of stigma on people with mental illness. World Psychiatry, 2002; 1: 16–20. [PMID: 16946807] [Retrieved April 13, 2017.] Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1489832/. [PMC free article] [PubMed]
- 16).Brohan E, Slade M, Clement S, Thornicroft G. Experiences of mental illness stigma, prejudice and discrimination: a review of measures. BMC Health Serv Res, 2010; 10: 80. [PMID: 20338040] [Retrieved April 13, 2017.] Available from: http://bmchealthservres.biomedcentral.com/articles/10.1186/1472-6963-10-80. [DOI] [PMC free article] [PubMed]
- 17).Ward C, Bochner S, Furnham A. The psychology of culture shock. Second Edition. 2015, Taylor & Francis Group, Philadelphia.
- 18).Corrigan PW, Michaels PJ, Vega E, Gause M, Watson AC, Rüsch N. Self-stigma of mental illness scale–short form: reliability and validity. J Psychiatry Research, 2012; 199: 65–69. [http://dx.doi.org/10.1016/j.psychres.2012.04.009] [PMID: 22578819] [DOI] [PMC free article] [PubMed]
- 19).Link BG, Phelan JC, Bresnahan M, Stueve A, Pescosolido BA. Public conceptions of mental illness: labels, causes, dangerousness, and social distance. Am J Public Health, 1999; 89: 1328–1333. [DOI] [PMC free article] [PubMed]
- 20).Shimotsu S. Reliability and validity of the Link’s Devaluation-Discrimination Scale. Japanese Journal of Psychiatric Treatment, 2006; 21: 521–528. [Article in Japanese]
- 21).Kessler RC, Barker PR, Colpe LJ, Epstein JF, Gfroerer JC, Hiripi E, et al. Screening for serious mental illness in the general population. Arch Gen Psychiatry, 2003; 60: 184–189. [DOI] [PubMed]
- 22).Corrigan PW, Michaels PJ, Vega E, Gause M, Watson AC, Rüsch N. Self-stigma of mental illness scale--short form: reliability and validity. J Psychiatr Res, 2012; 199: 65–69. [http://dx.doi.org/10.1016/j.psychres.2012.04.009] [PMID: 22578819] [DOI] [PMC free article] [PubMed]
- 23).Shimotsu S, Sakamoto S. Attitudes toward mental disorders, stigma, Devaluation-Discrimination Scale. Seishin Igaku, 2010; 39: 114–120. [Article in Japanese]
- 24).Cornelius BL, Groothoff JW, van der Klink JJ, Brouwer S. The performance of the K10, K6 and GHQ-12 to screen for present state DSM-IV disorders among disability claimants. BMC Public Health, 2013; 13: 128. [PMID: 23402478] [DOI] [PMC free article] [PubMed]
- 25).Haraguchi K, Maeda M, Mei YX, Uchimura N. Stigma associated with schizophrenia: cultural comparison of social distance in Japan and China. Psychiatry Clin Neurosci, 2009; 63: 153–160. [PMID: 19335384] [DOI] [PubMed]
- 26).Jorm AF, Kitchener BA, Fischer JA, Cvetkovski S. Mental health first aid training by e-learning: a randomized controlled trial. Aust N Z J Psychiatry, 2010; 44: 1072–1081. [PMID: 21070103] [DOI] [PubMed]
- 27).Angermeyer MC, Buyantugs L, Kenzine DV, Matschinger H. Effects of labelling on public attitudes towards people with schizophrenia: are there cultural differences? Acta Psychiatr Scand, 2004; 109: 420–425. [PMID: 15117286] [DOI] [PubMed]
- 28).Kurumatani T, Ukawa K, Kawaguchi Y, Miyata S, Suzuki M, Ide H, et al. Teachers’ knowledge, beliefs and attitudes concerning schizophrenia- a cross-cultural approach in Japan and Taiwan. Soc Psychiatry Psychiatr Epidemiol, 2004; 39: 402–429. [PMID: 26811110] [DOI] [PubMed]
- 29).Jorm AF, Kitchener BA, Fischer JA, Cvetkovski S. Mental health first aid training by e-learning: a randomized controlled trial. Aust N Z J Psychiatry, 2010; 44: 1072–1081. [PMID: 21070103] [DOI] [PubMed]
- 30).Takeuchi J, Kawagishi H, Minoshima T, Sakagami Y. Identification of students at high risk for mental health problems before participation in short-term study abroad programs; a case series. Campus Health, 2014; 51: 217–221. [Article in Japanese]
- 31).Angermeyer MC, Beck M, Matschinger H. Determinants of the public’s preference for social distance from people with schizophrenia. Can J Psychiatry, 2003; 48: 663–668. [DOI] [PubMed]
- 32).Angermeyer MC, Matschinger H, Schomerus G. Attitudes towards psychiatric treatment and people with mental illness: changes over two decades. Br J Psychiatry, 2013; 203: 146–151. [PMID: 23787060] [DOI] [PubMed]
- 33).Reavley NJ, Jorm AF. Young people’s stigmatizing attitudes towards people with mental disorders: findings from an Australian national survey. Aust N Z J Psychiatry, 2011; 45: 1033–1039. [PMID: 21942780] [DOI] [PubMed]
- 34).Angermeyer MC, Daubmann A, Wegscheider K, Mnich E, Schomerus G, Knesebeck OV. The relationship between biogenetic attributions and desire for social distance from persons with schizophrenia and major depression revisited. Epidemiol Psychiatr Sci, 2015; 24: 335–341. [PMID: 24786227] [DOI] [PMC free article] [PubMed]
- 35).Kvaale EP, Gottdiener WH, Haslam N. Biogenetic explanations and stigma: a meta-analytic review of associations among laypeople. Soc Sci Med, 2013; 96: 95–103. [PMID: 24034956] [DOI] [PubMed]
- 36).Kvaale EP, Haslam N, Gottdiener WH. The ‘side effects’ of medicalization: a meta-analytic review of how biogenetic explanations affect stigma. Clin Psychol Rev, 2013; 33: 782–794. [PMID: 23831861] [DOI] [PubMed]
- 37).Angermeyer MC, Holzinger A, Carta MG, Schomerus G. Biogenetic explanations and public acceptance of mental illness: systematic review of population studies. Br J Psychiatry, 2011; 199: 367–372. [PMID: 22045945] [DOI] [PubMed]
- 38).Griffiths KM, Carron-Arthur B, Parsons A, Reid R. Effectiveness of programs for reducing the stigma associated with mental disorders. A meta-analysis of randomized controlled trials. World Psychiatry, 2014; 13: 161–175. [PMID: 25855820] [DOI] [PMC free article] [PubMed]
- 39).Yamaguchi S, Wu SI, Biswas M, Yate M, Aoki Y, Barley EA, et al. Effects of short-term interventions to reduce mental health-related stigma in university or college students: a systematic review. J Nerv Ment Dis, 2013; 201: 490–503. [PMID: 23719324] [DOI] [PubMed]
- 40).Dyduch A, Grzywa A. Stigma and related factors basing on mental illness stigma. Pol Merkur Lekarski, 2009; 26: 263–267. [Article in Polish] [PubMed]
- 41).Baumann A, Zäske H, Decker P, et al. Changes in the public’s social distance toward individuals with schizophrenia in six German cities. Results of representative pre- and postinterventional telephone surveys from 2001 to 2004. Nervenarzt, 2007; 78: 787–788, 790–795. [Article in German] [DOI] [PubMed]
- 42).Gaebel W, Zäske H, Baumann AE, et al. Evaluation of the German WPA “program against stigma and discrimination because of schizophrenia--Open the Doors”: results from representative telephone surveys before and after three years of antistigma interventions. Schizophr Res, 2008; 98: 184–193. [http://dx.doi.org/10.1016/j.schres.2007.09.013] [PMID: 17961985] [DOI] [PubMed]
- 43).Independent Administrative Institution Japan Student Services Organization. Result of an Annual survey of International Students in Japan 2014 [Online]. [Retrieved April 13, 2017.] Available from: http://www.jasso.go.jp/statistics/intl_student/data14_e.html.