

Abstract
Background:
Recent evidences showed that outdoor air pollution had significant influence on cognitive functioning of adults. However, little is known regarding the association of indoor air pollution with cognitive dysfunction. Hence, the current study was done to assess the association between indoor air pollution and cognitive impairment among adults in rural Puducherry.
Methodology:
A community-based cross-sectional study was done among 295 adults residing in rural field practice area of tertiary care institute in Puducherry during February and March 2018. Information regarding sociodemographic profile and household was collected using pretested semi-structured questionnaire. Mini-Mental State Examination was done to assess cognitive function. We calculated adjusted prevalence ratios (aPR) to identify the factors associated with cognitive impairment.
Results:
Among 295 participants, 173 (58.6) were in 30–59 years; 154 (52.2%) were female; and 59 (20.0%) were exposed to indoor air pollution. Prevalence of cognitive impairment in the general population was 11.9% (95% confidence interval [CI]: 8.7–16.1). Prevalence of cognitive impairment among those who were exposed to indoor air pollution was 27.1% (95% CI: 17.4–39.6). Individuals exposed to indoor air pollution (aPR = 2.18, P = 0.003) were found to have two times more chance of having cognitive impairment.
Conclusion:
About one-fourth of the participants were exposed to indoor air pollution, out of which more than one-fourth was found to have cognitive impairment which is twice that of the general population. Hence, prevention of exposure to indoor air pollution needs to be done through increased availability to cleaner fuels for household usage.
KEYWORDS: Cognition, dementia, indoor air pollution
INTRODUCTION
The World Health Organization (WHO) has reported that dementia will become an epidemic in the near future because of growing elderly population, especially in developing countries.[1] This demands an early action to identify the persons at risk of dementia and prevent the disease from occurring or treat the affected persons accordingly. Cognitive impairment is the transitional phase between normal aging process and dementia. Hence, screening for cognitive impairment will help in recognizing the persons at risk of dementia and take corrective measures immediately. However, there is limited evidence available regarding the burden of impairment and determining risk factors, especially among low- and middle-income countries like India.[2] Understanding the environmental and social factors responsible for cognitive impairment is important given the increasing elderly population keep on increasing globally.
One of the environmental factors which is less studied but found to have significant influence on cognitive function is exposure to air pollutants. Studies around the world have reported that the exposure to high amounts of air pollution can negatively impact the cognitive functioning of the adults.[3,4,5,6,7,8] Several mechanisms have been proposed for the possible explanation on link between air pollution and cognitive dysfunction. Neurological mechanisms like inflammation of brain in response to particulate matter exposure and cardiovascular mechanisms are also proposed. However, clear mechanisms have not been established yet.[9,10,11,12] Previous studies on link between the cognitive decline and air pollution has reported that exposure to pollutants most commonly affects specific domains such as verbal learning, attention, logical and short-term memory, and executive functioning. However, severe effects were reported with long-term exposure to air pollutants.[3,6,13]
However, most of the studies were focussed on outdoor air pollutants from traffic or industries such as sulfur-dioxide, nitrogen oxide, and carbon monoxide, particulate matter and its relationship with cognitive impairment. Less is known regarding the association between indoor air pollution and cognitive dysfunction. Almost all the studies on outdoor air pollution and cognitive dysfunction have reported a significant association.[3,4,5,6,7,8] Hence, for the current study, we have hypothesized that there could be an association between indoor air pollution and cognitive dysfunction. The WHO has reported that indoor air pollution poses serious health risk for almost 3 billion people who cook and use biomass fuels and coals for household purpose.[14] Globally, indoor air pollution contributed to about 4.3 million deaths almost all in low- and middle-income countries. In India, it is found to be the second leading cause of premature mortality.[14]
According to the National Family Health Survey-IV, about 56.2% of households in India do not have access to clean fuel, contributing to indoor air pollution. Hence, more focus needs to be given on indoor air pollution and its association with cognitive impairment, especially among rural areas, who rely on biomass fuels in their households. Despite the higher burden of indoor air pollution in India, very little research has examined the influence of indoor air pollution on cognitive impairment in India. Hence, to assess this impact, the current study was done to find the association between indoor air pollution and cognitive impairment among the adults residing in the selected villages of rural Puducherry, South India.
METHODOLOGY
A community-based cross-sectional study was carried out in the Rural Health Center (RHC) of a tertiary care institute which caters to a population of around 10000 in the villages of Ramanathapuram, Thondamanatham, Pillaiyarkuppam, and Thuthipet. The study was conducted during the months of February and March 2018. Individuals belonging to age group of 30 years and above were included in the study as it is difficult to detect the impact of air pollution and cognitive dysfunction among younger adults.
The sample size was calculated by OpenEpi v 3.01 (v 3.01 updated on 2013, USA) using anticipated proportion of cognitive impairment 25% among adults living in households with indoor air pollution; confidence interval (CI) of 95%, and absolute precision of 5%, the sample size was calculated to be 289. However, we covered 295 individuals.
Primary sampling unit was households. Numbers of households needed from each of the four villages were calculated using proportionate sampling after which; systematic random sampling was employed to select the households from the villages. Individual belonging to the age group of 30 years and above were the study units. The study participants were chosen from eligible individuals available in the selected households during the house visit. KISH technique was applied to select one eligible individual from the households when there were multiple eligible persons in the household. Households which were locked even after three visits were excluded from the study.
Four training doctors posted in RHC were chosen as data collectors. They were sensitized regarding the objectives of the study, confidentiality of information, participant's right, and informed consent, and were also trained to administer the questionnaire to the individuals. Postgraduate students posted in the same RHC supervised the data collection procedure by reviewing all questionnaires at the end of each day to ensure completion of data collection forms as well as addressed any issue faced by the data collectors.
The purpose of the study and procedure involved in the study was explained to the individuals before administration of the questionnaire. Individuals were also assured regarding confidentiality of the information and data collection was started after obtaining informed consent. The interview consisted of three sections: the first section consisted of sociodemographic characteristics; the second section comprised household details such as type of house, type of fuel used for cooking, place of cooking, and type of fuel used for cooking. Use of fuel for cooking was seen by direct observation; the third section consisted of Mini-Mental State Examination (MMSE) to determine the mild cognitive impairment among study participants.
Definition of exposure to indoor air pollution depends on the type of fuel used in the household. Several evidences have shown that the use and toxic effects of kerosene and biomass fuels are the major factors responsible for indoor air pollution in the households, especially in rural areas.[15,16,17] Hence, households using biomass or kerosene as fuel for cooking within house were defined as exposed group. Households using liquefied petroleum gas (LPG) as fuel for cooking were considered as nonexposed group.
The MMSE is a short, easily administered 11-item scale which screens for cognitive dysfunction. Internal consistency of the questionnaire was reported to be 0.82.[18] MMSE had been standardized for our research by forward translation, expert panel back translation, pretesting and cognitive interviewing and concluded with the preparation of final version. Based on the scores obtained, they were classified into normal (score 25–30) and mild cognitive impairment (score <25). Each test took around 5–10 min.
Data were entered into Epidata v 3.01 software (Manufactured by Epidata association on the year 1999 in Denmark) and analysis was done using SPSS version 19.0. Continuous variables were summarized as mean (standard deviation [SD]). Prevalence of cognitive impairment among exposed and nonexposed groups was summarized as proportion with 95% CI. Bivariate analysis (Chi-square test/Fisher's exact test) was used to find the association of cognitive impairment with indoor air pollution and other household and sociodemographic characteristics. Determinants of cognitive impairment (Independent effects) were identified using multivariable analysis (log-binomial regression), considering cognitive impairment as dependent variable and age category, occupation, and indoor pollution as explanatory variables. Unadjusted and Adjusted Prevalence Ratio (aPR) ratio with 95% CI was calculated. P < 0.05 was considered statistically significant.
RESULTS
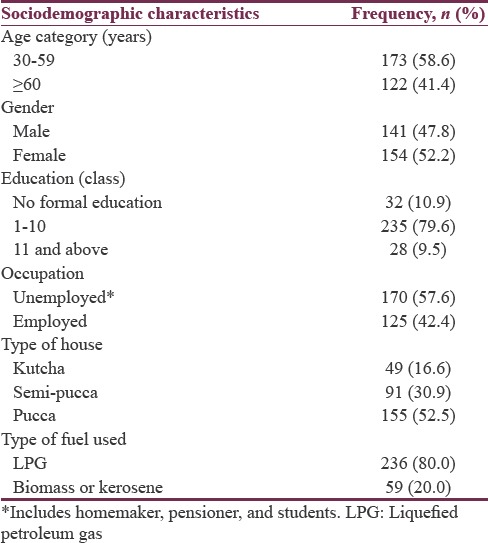
A total of 295 individuals were approached for screening of cognitive impairment and presence of indoor air pollution. None of the individuals refused to participate in the study (response rate 100%). The mean (SD) age of study participants were 53.4 (15.4) years. Table 1 depicts sociodemographic characteristics of the study participants. A total of 173 (58.6) were in 30–59 years; 154 (52.2%) were female; 235 (79.6%) were educated from class 1–10; 170 (57.6%) were unemployed; 155 (52.5%) were residing in pucca house, and 236 (80.0%) were using LPG for cooking purposes. Usage of firewood and kerosene for cooking within house was considered as presence of indoor pollution. The overall prevalence of individuals exposed to indoor air pollution was found to be 20%.
Table 1.
Sociodemographic characteristics of the study participants residing in the selected villages of rural Puducherry, (n=295)
The overall prevalence of cognitive impairment in the study population was 11.9% (95% CI: 8.7–16.1). Prevalence of cognitive impairment within the group who were suffering from indoor air pollution was 27.1% (95% CI: 17.4–39.6).
Table 2 represents the factors associated with cognitive impairment among adults residing in a rural area of Puducherry, South India. Individuals of age more than or equal to 60 years (PR = 4.79, P < 0.001) were found to have nearly five times more chance of having cognitive impairment when compared to individuals of 30–59 years. Males had greater cognitive impairment when compared to females (PR = 1.17, P = 0.64). Unemployed participants had more than two times (PR = 2.48, P = 0.002) higher risk of having cognitive impairment when compared to participants who are employed. Participants exposed to indoor air pollution (PR = 3.37, P < 0.001) were found to have three times more chance of having cognitive impairment when compared to the nonexposed participants.
Table 2.
Factors associated with cognitive impairment among adults residing in a rural area of Puducherry, South India (n=295)
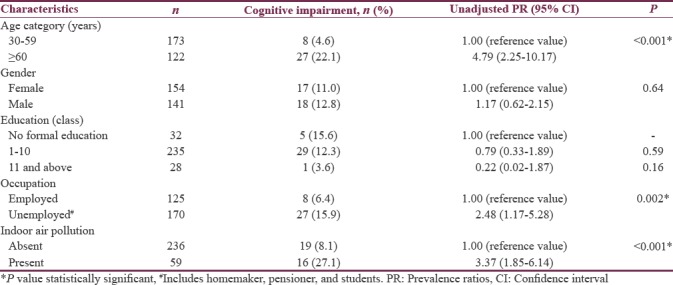
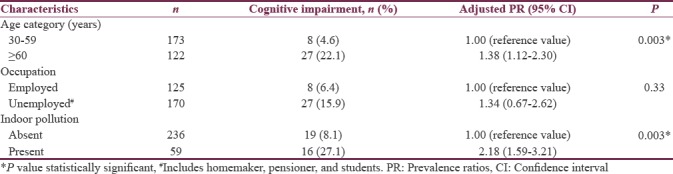
Table 3 illustrates multivariable logistic regression analysis for factors associated with cognitive impairment among adults residing in the rural area of Puducherry. For the regression analysis, age category, occupation, and presence of indoor air pollution variables were considered for model. Even though the effect size was reduced in all the factors after adjusted analysis, a significant association was retained. Individuals of age ≥60 years (aPR = 1.38, P = 0.003) and unemployed (aPR = 1.34, P = 0.33) were found to have 1.3 times more chance of having cognitive impairment when compared to individuals of 30–59 years and individuals who were employed, respectively, even after adjusting for indoor air pollution. Even though effect of indoor air pollution has reduced after adding other variables in the model, still the individuals exposed to indoor air pollution (aPR = 2.18, P = 0.003) had more than two times higher risk of having cognitive impairment when compared to the nonexposed population.
Table 3.
Multivariable logistic regression analysis for factors associated with cognitive impairment among adults residing in rural area of Puducherry (n=295)
DISCUSSION
This was a community-based cross-sectional analytical study conducted among adults aged ≥30 years in rural areas of Puducherry to assess the association between indoor air pollution and cognitive function. Prevalence of cognitive impairment among the total study participants was 11.9%. About one-fifth (20%) of the study participants were exposed to indoor air pollution. Out of which, more than one-fourth (27.1%) were found to have cognitive impairment, while <10% in nonexposed group had cognitive impairment. Age category, occupation, and indoor air pollution were found to be the predictors of cognitive impairment. Indoor air pollution was found to have positive association with cognitive impairment even after adjusting for other confounding variables such as age category and occupation.
Large-scale population study in India showed the prevalence of mild cognitive impairment to be around 4.6%.[11] Studies around India among elderly population showed the prevalence of cognitive impairment ranging from 3.5% to 7.7%.[19,20] The current study reported the prevalence among the people exposed to indoor air pollution to be 27.1% which is clearly in excess of general population and elderly. On adjusted analysis, exposure to indoor pollution has more than twice the risk of developing cognitive impairment when compared to general population. Similar findings were found in a study done in Mexico which reported positive association between exposure to indoor air pollution and cognitive dysfunction.[21] This implies that people exposed to indoor air pollution are at more risk of having cognitive dysfunction even when compared to other vulnerable population like elderly. Indoor air pollution is already proven to be significant risk factor for respiratory and cardiovascular diseases.[22] However, lesser research has been done on its influence on cognitive function. Considering the burden of indoor air pollution in the rural areas and significant association found in the recent studies, more research is required to find out the possible mechanisms involved and focus on developing appropriate strategies to tackle it.
Other factors such as age category and occupation were also found to be independently associated with cognitive impairment. Similar findings were found in most of the studies conducted around the world as well as in India. Age category is an established determinant of decline in cognitive function over the years. However, influence of occupation on cognitive impairment and air pollution is not explored in detail in most of the studies. The current study found that the participants who were unemployed had more chance of developing cognitive impairment. A possible reason for this association can be people who are unemployed tend to spend more time in home which can increase their risk of having cognitive dysfunction when compared to employed peoples.
This is one of a kind study in India assessing the association of exposure to air pollution and cognitive dysfunction among adults in the rural population. The current study adds to the literature on negative impact of indoor air pollution on cognitive functioning. Another major strength of the study is the community-based nature which makes the generalizability better. Higher response rate (100%), direct observation for assessment of indoor air pollution and use of validated scale adds to the strength of the study.
However, the study has certain limitations. Our study involved indirect measures for assessing the indoor air quality to find the association with cognitive function. Hence, further studies need to be done using direct measures for assessment of air quality in the rural households to determine the association with impairment in cognition. Furthermore, we could not explore the possible mechanisms through which the indoor air pollutants can affect the cognitive function. Hence, further longitudinal research might help in studying the mechanism involved in exposure to indoor air pollution and development of cognitive dysfunction in greater detail.
Exposure to indoor air pollution can be significantly reduced by increasing the access to cleaner fuel sources like LPG. This can help in reducing the impact on cardiovascular diseases, chronic respiratory disease, and neurological conditions like dementia. The current study also showed the significant influence of indoor air pollution on cognitive function. However, reducing the exposure to indoor air pollutants will be challenging in rural population where biomass fuels are still the main source for cooking purposes.
Government of India has even introduced a scheme “Pradhan Mantri Ujjwala Yojana” in 2016 which aims to provide cash incentives for LPG gas connections to women belonging to below poverty line families. More awareness needs to be generated regarding the scheme to reduce the indoor air pollution significantly across the rural population. Further public health efforts such as expansion and improvement of the programs will help in improving the health status of people living in rural households. In addition, further research needs to be done in larger scale throughout the country to study the possible mechanisms for the influence of indoor air pollution on cognitive function, especially in rural areas, where biomass fuels usage is common.
CONCLUSION
About 20% of the study participants were using biomass fuels for cooking purposes and were exposed to indoor air pollution. Among them, 27% were found to have cognitive impairment which is twice more than the general population who were not exposed to indoor air pollution. Hence, the prevention of exposure to indoor air pollution, especially among the rural population, needs to be done through increased accessibility and availability to cleaner fuels such as LPG for household usage. Further longitudinal research might help in understanding the mechanism through which indoor air pollution act on cognitive function.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.World Health Organization. Dementia. WHO; [Last accessed on 2018 Apr 07]. Available from: http://www.who.int/mediacentre/factsheets/fs362/en/ [Google Scholar]
- 2.Das SK, Pal S, Ghosal MK. Dementia: Indian scenario. Neurol India. 2012;60:618–24. doi: 10.4103/0028-3886.105197. [DOI] [PubMed] [Google Scholar]
- 3.Oudin A, Forsberg B, Adolfsson AN, Lind N, Modig L, Nordin M, et al. Traffic-related air pollution and dementia incidence in Northern Sweden: A longitudinal study. Environ Health Perspect. 2016;124:306–12. doi: 10.1289/ehp.1408322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Weuve J, Puett RC, Schwartz J, Yanosky JD, Laden F, Grodstein F, et al. Exposure to particulate air pollution and cognitive decline in older women. Arch Intern Med. 2012;172:219–27. doi: 10.1001/archinternmed.2011.683. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ailshire JA, Crimmins EM. Fine particulate matter air pollution and cognitive function among older US adults. Am J Epidemiol. 2014;180:359–66. doi: 10.1093/aje/kwu155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gatto NM, Henderson VW, Hodis HN, St John JA, Lurmann F, Chen JC, et al. Components of air pollution and cognitive function in middle-aged and older adults in Los Angeles. Neurotoxicology. 2014;40:1–7. doi: 10.1016/j.neuro.2013.09.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ranft U, Schikowski T, Sugiri D, Krutmann J, Krämer U. Long-term exposure to traffic-related particulate matter impairs cognitive function in the elderly. Environ Res. 2009;109:1004–11. doi: 10.1016/j.envres.2009.08.003. [DOI] [PubMed] [Google Scholar]
- 8.Tonne C, Elbaz A, Beevers S, Singh-Manoux A. Traffic-related air pollution in relation to cognitive function in older adults. Epidemiology. 2014;25:674–81. doi: 10.1097/EDE.0000000000000144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Campbell A, Oldham M, Becaria A, Bondy SC, Meacher D, Sioutas C, et al. Particulate matter in polluted air may increase biomarkers of inflammation in mouse brain. Neurotoxicology. 2005;26:133–40. doi: 10.1016/j.neuro.2004.08.003. [DOI] [PubMed] [Google Scholar]
- 10.Levesque S, Taetzsch T, Lull ME, Kodavanti U, Stadler K, Wagner A, et al. Diesel exhaust activates and primes microglia: Air pollution, neuroinflammation, and regulation of dopaminergic neurotoxicity. Environ Health Perspect. 2011;119:1149–55. doi: 10.1289/ehp.1002986. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Morgan TE, Davis DA, Iwata N, Tanner JA, Snyder D, Ning Z, et al. Glutamatergic neurons in rodent models respond to nanoscale particulate urban air pollutants in vivo and in vitro . Environ Health Perspect. 2011;119:1003–9. doi: 10.1289/ehp.1002973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Calderón-Garcidueñas L, Azzarelli B, Acuna H, Garcia R, Gambling TM, Osnaya N, et al. Air pollution and brain damage. Toxicol Pathol. 2002;30:373–89. doi: 10.1080/01926230252929954. [DOI] [PubMed] [Google Scholar]
- 13.Chen JC, Schwartz J. Neurobehavioral effects of ambient air pollution on cognitive performance in US adults. Neurotoxicology. 2009;30:231–9. doi: 10.1016/j.neuro.2008.12.011. [DOI] [PubMed] [Google Scholar]
- 14.World Health Organization. WHO Methods and Data Sources for Global Burden of Disease Estimates 2000-2015. WHO; [Last accessed on 2018 Apr 07]. Available from: http://www.who.int/healthinfo/global_burden_disease/GlobalDALYmethods_2000_2015 . [Google Scholar]
- 15.Fullerton DG, Bruce N, Gordon SB. Indoor air pollution from biomass fuel smoke is a major health concern in the developing world. Trans R Soc Trop Med Hyg. 2008;102:843–51. doi: 10.1016/j.trstmh.2008.05.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Chakraborty D, Mondal NK, Datta JK. Indoor pollution from solid biomass fuel and rural health damage: A micro-environmental study in rural area of Burdwan, West Bengal. Int J Sustain Built Environ. 2014;3:262–71. [Google Scholar]
- 17.Lam NL, Smith KR, Gauthier A, Bates MN. Kerosene: A review of household uses and their hazards in low- and middle-income countries. J Toxicol Environ Health B Crit Rev. 2012;15:396–432. doi: 10.1080/10937404.2012.710134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Khullar S, Kaur G, Dhillon H, Sharma R, Mehta K, Singh M, et al. The prevalence and predictors of cognitive impairment in type 2 diabetic population of Punjab, India. J Soc Health Diab. 2017;5:47–53. [Google Scholar]
- 19.Sosa AL, Albanese E, Stephan BC, Dewey M, Acosta D, Ferri CP, et al. Prevalence, distribution, and impact of mild cognitive impairment in Latin America, China, and India: A 10/66 population-based study. PLoS Med. 2012;9:e1001170. doi: 10.1371/journal.pmed.1001170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Sharma D, Mazta SR, Parashar A. Prevalence of cognitive impairment and related factors among elderly: A population based study. J Dr NTR Univ Health Sci. 2013;2:171–6. [Google Scholar]
- 21.Saenz JL, Wong R, Ailshire JA. Indoor air pollution and cognitive function among older Mexican adults. J Epidemiol Community Health. 2018;72:21–6. doi: 10.1136/jech-2017-209704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.World Health Organization. Dementia. WHO; [Last accessed on 2018 May 22]. Available from: http://www.who.int/phe/health_topics/outdoorair/databases/FINAL_HAP_AAP_BoD_24March2014 . [Google Scholar]