

Abstract
The authors present the case study of a 35-year informatics-based single subspecialty practice for the management of patients with chronic thyroid disease. This extensive experience provides a paradigm for the organization of longitudinal medical information by integrating individual patient care with clinical research and education. The kernel of the process is a set of worksheets easily completed by the physician during the patient encounter. It is a structured medical record that has been computerized since 1972, enabling analysis of different groups of patients to answer questions about chronic conditions and the effects of therapeutic interventions. The recording process and resulting studies severe as an important vehicle for medical education about the nuances of clinical practice. The authors suggest ways in which computerized medical records can become an integral part of medical practice, rather than a luxury or novelty.
Science is built up with facts as a house with stones.
But a collection of facts is no more a science than a heap of stones is a house.
—Jules Henri Poincaré, 1908
Patient care is still very much an art even as the foundations of medicine become increasingly scientific.1,2 Understanding how clinical information is transformed into clinical knowledge comes from experience in careful observation and assimilation of patient and process data—in short, from an informatics-centered approach to medical practice. This paper describes a 35-year experiment in developing the informatics tools for a chronic (thyroid) disease clinic. Essential to these efforts was the evolving design of a set of patient worksheets that permit efficient capture of patient data with minimal intrusion into the patient-practitioner encounter.3,4,5,6 The worksheets summarize patient data and clinical impressions of nurse and physician practitioners, making it easy to generate a computer-based or electronic medical record (EMR) with the longitudinal information essential to the follow-up of patients with a chronic disease. Within a well-defined subspecialty we have faced and largely solved a major problem still recognized as basic to the success of the EMR—that is, the need to efficiently capture physician data in coded form.7
Our thyroid patient database has grown since 1960 to contain over 15,000 patients referred for possible thyroid disease. We have followed subgroups of these patients for up to 35 years, a total of about 120,000 patient visits. Initially stored on punched cards, the data were placed on-line in 1972 on a mainframe computer for interactive access, and transferred to a PC-based system in 1987. The systematic organization of clinical information has, since its inception, played an invaluable role in carrying out clinical research projects, developing reporting and decision support software, and providing the materials for continuing medical education. This integration of patient care, clinical research, and medical education—catalyzed by the informatics-based approach to clinical practice—is illustrated by numerous examples in this paper. In describing the evolution of our information processes, we demonstrate their influence on the design of other specialty reporting systems, changes in the process of nurse-practitioner care, the discovery of clinical patterns from the database, the formulation and testing of hypotheses about thyroid disease, and the analysis of cost-effective strategies for screening and long-term chronic disease patient management. Our system can be viewed as a paradigm for a flexible practitioner-driven model of clinical information management processes that has withstood the test of time. We outline some positive and negative lessons learned about the role of technology in such processes, and the potential for similar schemes and systems to amplify the capabilities of practitioners as we move towards more outcome-directed and cost-limited practices in medicine. We maintain that success comes from choosing a level of technology that matches the information needs of a clinical practice, rather than adopting whatever current technology has to offer regardless of the clinical needs.
Foundations for an Informatics-centered Practice
When establishing a Department of Nuclear Medicine at the Straub Clinic in Honolulu in 1960, one of us (Dr. Nordyke) also began a specialized thyroid clinic patterned after a similar one at the Los Angeles Veterans Administration Radioisotope Service, which had been developed over the preceding four years by Dr. Nordyke in cooperation with the Service Chief, Dr. William Blahd. During the pre-1960 period a worksheet was developed for recording patient history, physical examination, laboratory studies, clinical impression, final diagnosis, treatment, and disposition/follow-up. The motivation for doing this was twofold: to keep a systematic and consistent record of patient information for follow-up care, and to lay the foundation for clinical research studies. While conventional, these reasons at the time (and even now) were not enough to motivate most clinicians to develop a structured medical record, even though the value of thyroid follow-up recording was well recognized.8 For us, additional incentives were the type of circumscribed specialty practice that thyroid problems present and the perceived standardization and repetition of tasks that it usually involves. Being eager to find the most effective and efficient way to conduct and control a growing thyroid practice led to continuous upgrading of the thyroid worksheet.
The Thyroid Worksheet
The primary documents for patient data recording are a printed worksheet and a time-oriented follow-up sheet, shown in their current versions in Figures ▶,▶ and ▶. The illustrated worksheets are the culmination of six major and several minor changes from 1960 to 1990 and have been unchanged since 1990. Worksheets are taken into the examining room by the nurse practitioner or physician and do not intrude on the normal way of practice or relationship with the patient.4,6 The organization of the sheets essentially follows the routine of the physician and covers demographic information; problem (chief complaint); history regarding thyroid disease; medications; history and physical findings demonstrated to have diagnostic significance for thyroid disease, emphasizing function (hyperthyroidism and hypothyroidism) and anatomy (eyes, details of thyroid gland); results of diagnostic procedures such as Achilles reflex time (ART), scan, fine-needle aspiration, and laboratory tests; clinical impression by nurse practitioner and physician separately prior to information from procedures; treatment; follow-up; and comment.
Figure 1A.
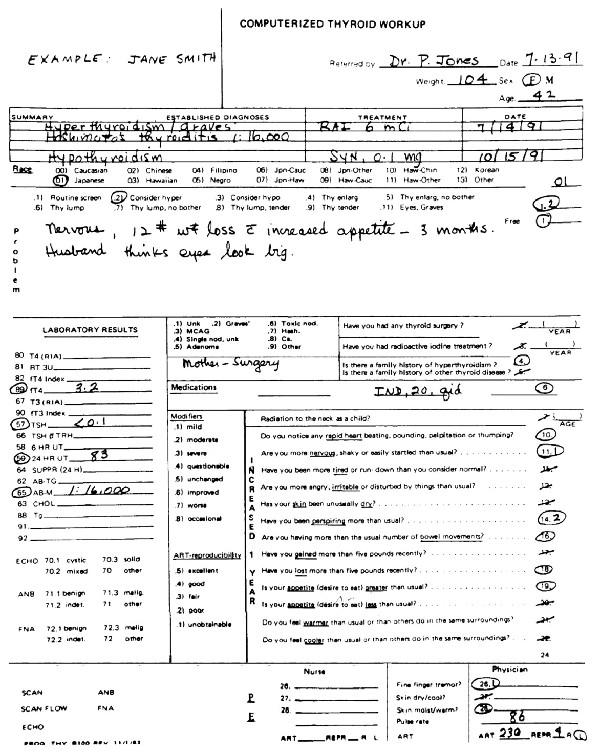
Computerized Thyroid Workup. This printed worksheet is used as the primary document to record information in our practice.
Figure 1B.
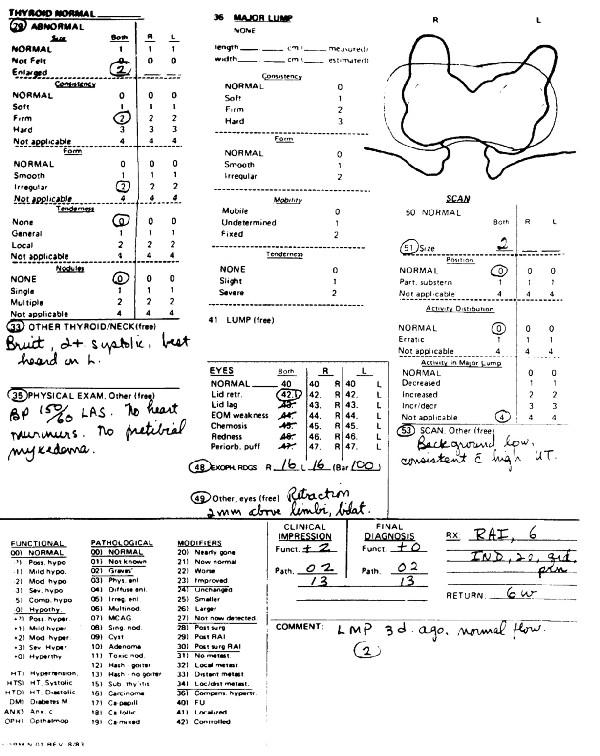
, Continuation of the printed worksheet. Notice the many opportunities to insert free language.
Figure 2.

Thyroid Follow-up Visit. The physician takes this follow-up flowsheet and the printed worksheets into the examining room.
Special Characteristics
The special characteristics of these worksheets are shorthand notations, completeness, flexibility, and time-oriented follow-up. Shorthand notations are quick and easy to use, and they simplify data capture by computer (Figures ▶,▶ and ▶). Examples are a line through a number if the item is negative, a circle if positive, and a modifier if needed. Modifier definitions are listed on Figure ▶,▶ for easy reference. In our example, a 28-year-old woman was referred for possible hyperthyroidism. She had a sister with Graves' disease, was taking Inderal and birth-control pills, and complained of increasing rapid heart beating, slight nervousness, fatigue, moderate perspiration, increased number of bowel movements, a 12-pound weight loss with increased appetite, and severe heat intolerance. Physical examination revealed a slight fine finger tremor, and skin that was slightly warm and moist. The thyroid gland was enlarged two times and was firm, irregular, nontender, and without nodules. There was mild retraction of the left upper lid above the limbus. Clinical impression and final diagnosis for function and pathology are required at each visit. Codes and modifiers for this purpose are defined on ▶. In the illustration, the coding for additional diagnoses may be added on the lines below the coded diagnoses in free language. Comparison of clinical impression and final diagnosis provides continuous fine tuning of diagnostic acumen.
Completeness is illustrated in the areas of the thyroid gland as a whole, a major lump in the gland, eye examination, and scan. For example, if the gland feels normal, a check is made in the space for “Thyroid normal.” If any abnormality is felt, statements must be made about the gland's size (both lobes or right and left), consistency (normal, soft, firm, hard), form (normal, smooth, irregular), tenderness (none, general, local), and nodules (none, single, multiple). If a nodule is found, it must be categorized by length, width, consistency, form, mobility, and tenderness. A similar approach is taken for the eye examination and scan.
Flexibility is illustrated by the ability to insert free language at any point in the worksheet. It is used routinely in the “Problem” and “Comment” positions and at every point where “Other” is stated (e.g., items 33, 35, 41, 49, and 53).
Time-oriented longitudinal recording is shown in ▶. Six patient visits are available on each sheet, three on each side, and an unlimited number of sheets can be added for each patient. All numbers and modifiers in the follow-up sheets are identical in meaning to those in the primary worksheets, but the free language areas tend to be more freely used. The compact layout allows for easy single-visit cross-sectional information and, simultaneously, for longitudinal comparison of changes over time for symptoms, signs, laboratory tests, clinical impressions, diagnostic status, medications, and comment. An especially valuable aspect of this record format is the ability to rapidly gauge the progress of the patient in both function and anatomy of the thyroid gland (changes in symptoms and signs, size of goiter or nodule, laboratory test results, etc.).
The most evident immediate advantage of the flow-chart has been the rapid review of patient status regardless of years of follow-up. Our experience corresponds with that of Fries,9 who studied the time it took to thumb through a standard chart compared with a flowchart similar to ours. The time for each case was reduced from seven to two minutes. Beyond easily tracking the course of individual patients over many years, the most evident long-term advantage of the flowchart is the ability to group patients for clinical research and education purposes.
Reporting System
The information from the worksheets (both coded and free language) is entered into the computer by an aide. From these data, a computer-generated report is produced for the patient's chart within a few minutes. The data are stored for administrative control, research, and self-education. The report placed in the chart itself is the basis for exchanging information with other practitioners involved in the management of the case.
As can be seen from the example shown in ▶, after listing the patient identifiers and visit-specific information, the report reproduces the physician's description of the patient's problem followed by family history related to thyroid disease. Each category of findings is underlined, and relevant terms are listed in compressed form. Significant negative findings—e.g., the lack of heart murmur or pretibial myxedema, and the absence of tenderness and nodules on thyroid gland examination—are included automatically. Definitions of observations and measurements are given sparingly but in a way that will reduce questions from referring practitioners. For instance, lid retraction in millimeters above the limbus is noted, the degree of reproducibility of reflex time measurement is graded, and normal ranges for tests are given.
Figure 3.

The typed report generated by the computer from the coded and free language data keyed in from the worksheet and flowsheet. The report is ready within a few minutes and can be put into the patient's chart immediately.
The comment section of the report includes both free text and text composed by rule-driven software that draws on recorded data from other parts of the report. Other parts are triggered by coded notations on the worksheet (e.g., the number 2 in the worksheet comment section in ▶). The report comment section is intended primarily to give the referring physician a summary of recommendations and actions taken at the thyroid clinic beyond the immediate treatment listed above it, and has proven to be a most useful reminder for patient follow-up. On the report shown in ▶, the main points discussed with the patient about the iodine 131 (131I) treatment are listed, followed by related recommendations for changes in the patient's lifestyle and expectations about likely patterns of improvement in thyroid condition and expected side effects.
Evolution of the Thyroid Worksheet
The original version of the worksheet, developed and refined through the 1960s, consisted of three pages. It was geared to the initial visit of a patient and to the identical recording of data from subsequent visits onto the same sheet. A noticeable difference between this worksheet and the present one was its orientation toward the entry of data onto computer cards and the concomitant exclusive use of numerical codes. One result was a rigid set of coding values for specific history, symptom, and sign data split into disjoint categories. Another was that much space was wasted (noticeably in the reporting of laboratory test results) on data that was frequently not obtained.
In terms of structure, data about history and symptoms appeared on the first page of the worksheet, physical examination results on the second, and laboratory test results—together with impressions and follow-up information on the third. Dates were truncated to month and year because of coding constraints, and dosages for prescribed therapies were not listed.
Despite some of these limitations, the 1960s worksheet proved remarkably effective in capturing most of the data needed for patient follow-up and for clinical studies that were carried out on subsets of them10 using the data-processing techniques of the time, which were mostly confined to sorting and simple statistical distribution graphing of data.
Substantial changes to the worksheets were introduced in the early 1970s by structuring information in response to clinical experience. These changes were also influenced by the intensification of studies on the database of cases accumulated over the previous decade and the development of pattern recognition and statistical decision-making programs from these data.11
The worksheet as revised in 1971 provided more opportunity for free text entry to characterize the patient's problem, because choosing a single code for the chief complaint that brought the patient to the clinic had proved inadequate in many cases. In addition, the form showed the reason for the visit, which begins the connection between process and patient information. The most noticeable difference from the 1960s worksheet, however, was the greater compartmentalization of the data by history, physical exam, and laboratory data. There were also changes in the coding of the laboratory data, reflecting simplification of the expected results that were significant for the assessment of thyroid function. New laboratory data, such as the antithyroid antibodies (THT), later replaced by anti-microsomal antibodies, was also added to the form. Results of palpation of the gland now differentiated between the left and right lobes, and other signs, such as those involving the feeling of the skin, now combined the diagnostically important categories of “warm and moist” for hyperthyroidism and “dry and cool” for hypothyroidism, which were definitely confirmed by statistical analysis of the previous 10 years' data. Incorporation of probabilities for the clinical impression reflected the development of a decision-support module based on Bayesian probability calculations.11
Two subsequent revisions of the sheet, in 1972 and 1973, led to increased compartmentalization of data layout, the paring down of some comments sections, and the discarding of Bayesian probabilities for the physical exam results, which were not found to be useful to the practitioner actually performing the examination. The limitations of this “black box” probabilistic approach to decision support helped motivate the development of more knowledge-intensive and more explanatory models for consultation programs in a variety of specialties including thyroid disease.12,13
Other changes at this time involved summarizing laboratory tests and bringing them to the first page of the form, where they could be used for both ordering tests and recording the results. This highlighted the increasing importance of the “objective” laboratory test component of the thyroid practice. For physical examination of the thyroid gland a separate data item was recorded for the major lump and its characterization, and thyroid size was recorded separately for the right lobe and left lobe unless the data were similar for both. This summarized refinement of data is a major indication of how experience with the worksheet affected clinical practice in a systematic way, and how it affected clinical research in the objective determination and definition of signs and symptoms.
An important development reflecting the first formal sharing of practice between nurse practitioner and physician was the incorporation of a section for the nurse's record of physical exam results side-by-side with the physician's. In addition, more structure was provided for the summary at the top of the form by listing problems, diagnoses, treatments, and dates.
The late 1970s and the 1980s saw further restructuring of the worksheets, with simplifications or deletions of findings that proved not to be useful in practice and with the addition of new laboratory tests, such as the sensitive thyrotropin (TSH) and various thyroid scan results. Some changes were also made to the longitudinal record in the selection of items to be followed and in the display of critical information on impression, medications, and major test results to facilitate rapid overview of the patient's present status in relation to that at previous visits. In this way the forms evolved to the current version.
Thyroid Database
Data collected from thyroid worksheets was stored during the 1960s on punched cards for processing on mainframe IBM computers. From this format a database was first created for retrospective analysis of data gathered between 1960 and 1970, by pattern recognition and Bayesian probability models.11 From 1971 to 1983 the data were held online on an HP3000 computer system from a commercial vendor. The data at this point covered 11,053 initial patient visits and 8922 follow-up visits. Of the latter, 3083 were from the 1960-71 period and 5839 were from 1971-83. Data were then transferred to a DBASEIII system on IBM PCs and subsequently stored on diskettes because of cost considerations.
A study carried out in 1975 showed that thyroid function screening by a Licensed Practical Nurse (LPN) could lead to significantly lowered costs for detection of hyperthyroid and hypothyroid conditions. The screening focused on reflex time, pulse, and signs of cool/dry or warm/moist skin, increased appetite or weight loss, nervousness, fatigue, and whether there had been previous thyroid surgery or radioiodine treatment. The system used Bayesian predictive probability estimates to suggest whether a secondary thyroid screen was needed. Various protocols were devised using different combinations of LPN effort and computer, thyroxine (T4) laboratory test results and computer, LPN effort plus laboratory and computer, and physician effort plus computer to determine tradeoffs in their sensitivity and specificity. Our studies showed that with T4 test results and computer support, thyroid function screening was not affected when an LPN performed the screening instead of a thyroid specialist. Without the test results and computer support, the LPN tended to be more specific and the physician more sensitive in the interpretation of data. Cost studies showed that considerable savings were realized by having the LPN take the initial history and perform a selected physical examination, with the thyroid consultant reviewing these and making the clinical decisions.
Consequences of Applying an Informatics Approach to the Thyroid Clinic
As shown by the evolution of the worksheets, their design required refinement from time to time on the basis of what worked and what didn't in the clinic, but the overall structure remained stable over considerable periods of time. The worksheet-centered approach has produced obvious advantages for our practice: The handling of patient information is smooth, efficient, and reproducible, and the information itself is easily retrievable when needed for future care, or administrative, research and educational purposes.
Clinical Research
We have carried out scores of research projects, from recurrent testing of sensitivities and specificities of items on the worksheet (thus continually updating worksheet information) to a multi-year prospective analysis of the optimal 131I dose for eliminating hyperthyroidism. The following list is a sampling of questions that have been answered from our own practice:
Is the Achilles reflex time a useful sign of hyperthyroidism as well as hypothyroidism? (Yes. It has excellent sensitivity and specificity compared with other signs of thyroid dysfunction.)14
Is there a correlation between goiter size and degree of hyperthyroidism? (Yes. The correlation is positive but weak.)15
Can second-generation TSH be used as a first-line test to detect hypothyroidism? (Yes.)16,17
Can second-generation TSH be used as a first-line screen for both hyperthyroidism and hypothyroidism? (Yes.)18
What is the most cost-effective sequence of TSH and free T4 for general use in a hospital laboratory? (It is TSH followed, if abnormal, by free T4).18
What is the optimal starting dose of 1-thyroxine (T4) and the follow-up time intervals in recent onset hypothyroidism occurring after 131I treatment of hyperthyroidism? (The mean final dose of T4 was 0.103 mg/day; for 24 of 52 consecutive patients, the dose was 0.1 mg/day. The follow-up time interval between dosage changes was four to six weeks.)19
What is the optimal 131I dosage for a single-dose cure of hyperthyroidism? (The optimal dose was 10 mCi. Cure was directly related to dose, from 70% cure at 5 mCi to 87% cure at 10 mCi.)20
Is the single dose cure rate affected by immediate post-131I treatment of hyperthyroidism with antithyroid drugs? (Yes. There is about a 25% reduction in the one-year cure rate at the 10-mCi 131I treatment level when this is done.)*
How do the signs and symptoms of hyperthyroidism change with age? (There is little change until after the fifth decade, when signs and symptoms begin to decrease slowly.)14
What are the clinical characteristics of painful subacute thyroiditis in Hawaii? (They are 69% bilateral, female:male ratio 6.7:1, spontaneous remission within two to four months.)21
Is it cost-effective to use both antithyroglobulin antibodies and antimicrosomal (antithyroid peroxidase) antibodies for detection of Hashimoto's thyroiditis? (Little is lost by using only antimicrosomal antibodies, which saves about half the cost of laboratory testing.)22
Patient Care and Management
The long-term worksheet-based informatics approach to practice has had as strong an effect on patient care and management as it has on clinical research. Besides the immediate effect on thyroid practice, it has provided a basis for quality and cost studies for thyroid testing protocols and has encouraged reproducibility studies for clinical measurements and tests. The approach has also had a major influence on the development of other chronic disease clinics and multi-specialty clinics and on the Nuclear Medicine Reporting System. In the 1960s and 1970s it was directly related to the pioneering work on multiphasic screening at the Straub Clinic, which was developed in collaboration with Dr. Fred I. Gilbert, Jr.23,24
Other Chronic Disease Clinics
Based on the results of the thyroid clinic worksheets and protocols, clinics for other chronic diseases and specialty practices—including gout, hypertension, family planning, Parkinson's disease, acne, neck-back problems, diabetes, anorectal complaints, and cancer chemotherapy—were established. The different clinics had a variety of modes of operation, from nurse-managed practices in which a nurse had major control of patient management with backup by the physician, to those like the thyroid clinic, where an LPN acted in a supportive capacity under the immediate direction of a physician in charge. They also had different records of success. The ones that worked best were those concerned with gout (under nurse-managed care there were fewer hospitalizations per year for problems related to gout than under complete physician care),25 neck-back problems, hypertension, thyroid disease, and anorectal complaints. (A trained proctoscopic technician carried out about 2000 proctoscopic examinations annually from 1972 to 197525 in a protocol that has been fused with multiphasic health testing and continues to the present.) The informatics-based clinics led to significant cost-effective gains in health care delivery in the 1970s.
Nuclear Medicine Reporting Systems
The success of the first three versions of the thyroid worksheet encouraged us in 1973-74 to design a set of 12 worksheets for summarizing information from studies carried out at the Nuclear Medicine Department at Straub.5 The functions we covered included imaging for lung, brain, myocardial infarction, liver and biliary tract, thyroid, tumors and inflammation, left ventricular ejection fraction and wall motion, gastric emptying, hepatic artery catheter placement, and gastrointestinal bleeding localization. ▶ shows the worksheet for the liver/spleen scan as an example. The worksheet is divided into patient identifier information, reason for test, areas measured, technician description of the imaging process, and specific details of results. The report ends with summary impressions by the nuclear medicine specialist. Once completed, aides would quickly enter the results into the computer for rapid report generation. An example of the report generated for a liver/spleen scan is shown in ▶.
Figure 4.

Liver/Spleen Scan. This is the printed worksheet for a liver/spleen scan report.
Figure 5.

The typed report generated by computer from the liver/spleen scan worksheet.
The reason for developing this system was the dissatisfaction of practitioners in having to dictate 300 to 400 often repetitive reports of the specified types each month. This led to delays in transmitting information to referring physicians. About a third of the studies were usually normal, which required the circling of a single letter by the nuclear medicine specialist; another third required minimal specific characterization of results in less than a minute of practitioner time; and the final third required more time. The overall increase in efficiency for the two-thirds with minimal reporting is considerable. Referring physicians have test reports in their patients' records within the day, leading to more timely and appropriate patient care. The sheets, like those for the thyroid clinic, included considerable free text capabilities for most items. When the worksheet method of the Nuclear Medicine Reporting System was compared with medical transcription of the same information, cost savings were found to be 79 cents per report.4 This reporting system has been in continuous use, with periodic improvements, from the mid-1970s to the present. Physicians using the system perceive major gains from its use: The time needed to produce typed reports is markedly reduced, standardization and completeness of reports is improved, and typed reports can be ready for signature within a few minutes without a trained medical transcriptionist.6
Automated Multiphasic Health Testing System
Automated multiphasic health testing (AMHT) at the Straub Clinic (the Health Appraisal Center) is a direct offshoot of the chronic disease worksheets and protocols described above. It was started as an off-line facility in 1967 and was placed on-line in 1971.24 About 40 patients are examined daily. The system was designed to provide a base-line examination and health analysis. It used patient-computer interaction for history-taking; technicians for obtaining physiologic function data and laboratory and radiologic information; specially trained nurses for reviewing the history, doing the complete physical examination, and developing problem lists; and a computer to provide a history with flagged abnormalities, a summary, and a partial problem list with suggested analysis. After all information was available, the AMHT physician reviewed it, checked the patient for abnormal findings, and provided a computerized summary statement that was given to the referring physician. This remained automated from 1971 to 1986, when a new administration continued the services without use of the computer. During its computerized operation, many quality control and research projects were carried out for the entire Straub Clinic.
Discussion
When we started this work in 1960, the interaction between physician and patient seemed the best and most natural point for identifying areas of patient care that needed improvement and finding ways to improve them. At that time (and even now), most of the information collected by the physician was discarded; it was not organized to allow retrieval and analysis. To a large extent, medical practice is information handling.26 Much of the information comes from the experience of others, but one's own practice is a rich and often overlooked source. Records have always been the weak link. Unless records are well organized and retrievable, observations of the processes and outcomes of groups of patients are so cumbersome that the busy practicing physician rarely undertakes them.
Despite many advances in computing over the past three decades, the computer has rarely been used at the physician-patient interface.26,27 It has been used instead mostly for administrative and financial purposes, the recording needs of which are often quite different and frequently at variance with those of clinical practice and research.28
This is unfortunate, since possibilities to continuously improve the professional aspects of patient care are largely concentrated at the physician-patient interface. This interface is the final common pathway where ancillary data come together, where the physician's knowledge and skills are applied, where unique elements of each practice are best known, where specific needs and goals are established by physician and patient together, where the needs for further research and education are discovered, and where outcome performance is finally evaluated. It is, therefore, unfortunate that the computer has been used almost exclusively for peripheral chores and rarely where it has the greatest chance of improving the quality of patient care.
Reasons for this state of affairs are many and complex. Even recently, it has been recognized that “no data entry problem is more challenging than that of acquiring data obtained from conversation with and examination of the patient.”29 Furthermore, computerizing patient data has highlighted the problems in organizing such data. A major difficulty lies in the tradeoff between the need for flexible and expressive descriptions of patient findings best captured by free text, and the need for well-defined codes to categorize the findings best captured by standardized coding systems.7 When we started our work, there was no standard coding for thyroid data. Even today, despite considerable advances in the formulation of medical coding schemes, nomenclatures and controlled vocabularies,30,31 and minimum data sets,32 many enhancements are needed to increase their clinical usefulness.33 The importance of longitudinal EMRs is widely recognized,34 especially for chronic diseases,35 but the actual formulation of standards for clinical informatics is still ongoing.33,34
The alternative of free text entry requires reasonably flexible and accurate natural language understanding, which still poses many open scientific questions and technologic challenges, even when restricted and simplified for medical reporting.36
As illustrated previously, we have developed a mix of coded and free text entry that works clinically: It supports the flow of physician-patient interaction while providing enough coding of specialty data needed for follow-up care and clinical studies. It took us about 25 years to establish the most appropriate mix of coded and free text input and so balance the needs for flexible yet retrievable information recording in our single subspecialty of thyroid disease. From a 35-year perspective, however, we can conclude that the overall structure of our medical records remained relatively stable, and has been more the subject of gradual evolutionary refinement rather than revolutionary change. This might be attributed to our having operated in a circumscribed medical subspecialty, where clinical problem definitions and knowledge have improved gradually without major changes in their scientific foundations. Moreover, medical thinking about the management of chronic disease, such as thyroid dysfunction, has seen an equally gradual evolution, with improved testing procedures and refinements in treatment rather than wholesale changes in prior practice. In this sense, the stability in the structure of the information needed for practice can be seen as something expected, as it reflects the nature of evolution in the clinical field.
What we learned in the period from 1960 to the mid-1970's was:
The sensitivity/specificity tradeoffs for all the signs, symptoms, and test results included in the original and some updated versions of the thyroid record;
The effects of combining various data items in the questionnaire based on their statistical prediction power;
The comparative advantages of the nurse-practitioner versus the physician in recording patient histories and performing physical examinations, and their performance tradeoffs with and without computer decision support;
How to organize the best and most compressed version of the medical record for initial visits, and the advantages of a longitudinal summary record for follow-up management; and
The value of automatically generating reports by computer for the referring physician and for inclusion in the patient's medical record.
In the two decades that have followed, only minor improvements have been required in the design of the record—in its layout and organization; in the location of items in the longitudinal record to make trends in patient data, impression, and treatment more apparent; and in compression of the record for ease of handling. In many ways we can view our work as a successful “niche adaptation” of an EMR.
From a technologic perspective, our work points to a number of lessons:
Clinical research was invaluably helped by early computer coding of clinical data elements. In no other way could we have a 35-year database for the studies.
Computer analysis of the data in the thyroid database, once organized and “cleaned,” proved to be the basis for statistical studies that were essential for determining the aggregation of signs and symptoms that made further data recording most efficient.
Ongoing computer analysis of patient data sets proved essential in developing protocols for shared care with nurse-practitioner and physician interaction.
Computer-generated report systems for thyroid and other clinics proved to be of lasting value in health care management for health appraisal, chronic disease follow-up, and sharing of information with referring physicians, as well as for administrative assessment of efficiencies and effectiveness of practice protocols and processes.
Introducing decision support for the practicing physician in the early 1970s proved unnecessary. It was an interesting exercise in confirming clinical judgment, but proved to be a distraction for clinical practice in the longer term.
Using the same Bayesian decision support in the mid-1970s for the nurse-practitioner proved to be of academic value only, since in a single subspecialty practice the nurse's decisions were always reviewed by the physician anyway.
On-line storage of cases in the 1970s and early 1980s proved to be unnecessarily costly and not essential for automated report generation, which was the greatest source of clinical added value of the computer system. Once the follow-up forms had been devised, new data could be added on a per-visit basis with no reference to prior visit information. Initial visit and time-oriented analyses could be performed off-line from the database in longitudinal studies. This supports the contention that “avoiding obsolescence will require a progressive separation of the application from the underlying database.”37
Administrative cost and insurance information was always separate from the clinical information. The clinic or hospital administration never saw the need to merge the two and would not provide funding to do so, despite cost-effectiveness studies of patient care demonstrating the potential of the clinical database for bringing about efficiencies in health care.25 This experience is consistent with that of most other early developers of computer-based medical records,38 until recent changes due to managed care and greater expectations of outcomes research and evidence-based medicine.
Conclusions
We can conclude that the development of specialty EMRs that are effective for both clinical research and improved standards of practice needs to be a longterm endeavor—of responding to new data and improving clinical knowledge in response to lessons that can be best learned from a computer-based database of cases. We can also conclude that the informatics needs of a practice come from organizing data and knowledge as it is naturally driven by clinical practice and research problems, not by the technology. Technologic opportunities should not be missed, to be sure, but they are often expensive and not immediately useful. The possibility of disconnecting on-line reporting from off-line database analysis proved to be an important lesson in a period of limited and costly computing resources. Likewise, the introduction of clinical decision support should be carefully matched to the needs of practitioners, avoiding the merely confirmatory and striving for value-added information, like that provided by the automated reports generated by our systems.
Our experience over the last three decades suggests that using a simple paper worksheet as input to a desktop PC with a commercially available database program provides an expanded overview of a practice that enhances continuous quality improvement, clinical research, and continuing professional education. Continuous quality improvement at the professional level is not easy to define or to distinguish from clinical research. It extends across a spectrum that assures the follow-up of ill patients, monitors the reproducibility of laboratory tests, answers small and large questions about patient care, and keeps track of costs, processes and outcomes of alternative procedures or treatments.
Clinical research is best known for randomized, controlled trials that often take years to conclude and that apply to only a small fraction of clinical problems.39,40 Published series on any subject are often not directly applicable to one's own practice because of differences in procedures, techniques, training, and abilities.39,41 It is less well recognized that answers to a multitude of small questions can be found quickly in a local database but not in a medical literature search. Many seemingly trivial operational issues become very important in terms of cost, patient satisfaction and sometimes, major outcomes of care.42 Relman43 writes “... unless we systematically collect and analyze the results of our clinical experience, we will never know enough to make discriminating choices.” More specifically, we need to study patients who have common diseases in order to improve diagnosis and management, and we also need detailed long-term studies of the evolution of chronic diseases.44 The continuously updated personal databank provides an informational power otherwise unavailable for these purposes.
Continuing education fuses indistinguishably with continuous quality improvement and clinical research. Questions arise, answers are found, and knowledge moves up to a new level. If answers are generated from our own practices, they are more likely to translate into operational changes than if they are obtained from a literature review. We agree with Houle45 that the most fruitful education derives from continually monitoring one's own work, making judgments about success or failure, and altering performance accordingly. Such monitoring will not occur without personally developed data banks, but so far computer technology has not greatly influenced continuing medical education.46 It has only been used sporadically to link education to practice.
Excellent large computerized patient record systems have been developed.38,47 Efforts to standardize and extend the electronic medical record are being encouraged and supported by federal agencies and private organizations, and the Computer-Based Medical Record Institute recommended by the Institute of Medicine48 was founded to promote development of a nationwide network of EMRs. In time, large and small EMRs, linked together internally and externally, should become widely available.
In the meantime, and to prepare for this, our simpler approach can be used in almost any practice. Our fundamental plea is that computerized records become an integral part of medical practice rather than a luxury or a novelty,49 and that physicians use methods that foster systematic learning from their own clinical experiences. For now, any physician willing to spend the time and thought needed for preliminary planning can develop a personally tailored, relatively in-expensive computerized record system. The effort will be repaid by easier observation of cost, process, and outcomes, leading to a higher level of patient care. As computer networking and data interoperability standards mature, physicians will be further repaid by being able to pool their efforts with those of their colleagues in ways that can only enhance their expertise and knowledge further.
Acknowledgments
The authors thank Lynn Madanay, MD, Guy Mussen, MS, Ann Harada, MPH, Cynthia Soraoka, MSW, MBA, and Katherine Fleury, MT (ASCP), MBA, for their help with this project over many years. They thank Christine W. Kulikowski for critical comments and help in editing the manuscript. They acknowledge their gratitude to the late Fred I. Gilbert, Jr., MD, without whose encouragement, support and collaboration much of this research would not have been possible.
This work was supported in part by the Pacific Health Research Institute, the Straub Foundation, and the George F. Straub Trust.
Dr. Nordyke died in August 1997, shortly after this paper was accepted for publication.
Footnotes
Our unpublished data.
References
- 1.Van Bemmel JH. Medical informatics, art or science? Methods Inf Med. 1996;35: 157-72. [PubMed] [Google Scholar]
- 2.Kulikowski CA. The scope of medical informatics as art and science. Methods Inf Med. 1996;35: 185-8. [PubMed] [Google Scholar]
- 3.Nordyke RA. Experiences with a protocol for thyroid disorders. In: Kallstrom, Yarnall (eds). Advances in Patient Care. 1975; 125.
- 4.Nordyke RA, Gilbert FI Jr, Mussen GA. Semi-automated reporting system for a nuclear medicine department. Proc Am Assoc Med Sys. 1982; 183-7.
- 5.Gilbert FI Jr, Nordyke RA, Higgins MP, Raney JD, Smith CJ. A computer-assisted hospital and outpatient information system for patients served by Straub Clinic and Hospital, Inc. Straub Foundation Proceedings. 1985;50: 5-7. [Google Scholar]
- 6.Nordyke RA, Gilbert FI Jr. Using the computer in the doctor's office to enhance the quality of patient care. Straub Foundation Proceedings. 1990;55(2): 17-21. [Google Scholar]
- 7.McDonald CJ. The barriers to electronic medical record systems and how to overcome them. J Am Med Inform Assoc. 1997;4: 213-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Falkenberg M, Nilsson OR, Rosenqvist U. Value of thyroid follow-up registers. Scand J Prim Health Care. 1987;5: 181-5. [DOI] [PubMed] [Google Scholar]
- 9.Fries JF. Time-oriented patient records and a computer data bank. JAMA. 1972;222: 1536-42. [PubMed] [Google Scholar]
- 10.Nordyke RA. Long-term follow-up of patients treated for thyrotoxicosis using the Achilles' reflex time. Hormones. 1970;1: 36-45. [DOI] [PubMed] [Google Scholar]
- 11.Nordyke RA, Kulikowski CA, Kulikowski CW. A comparison of methods for the automated diagnosis of thyroid dysfunction. Comput Biomed Res. 1971;4: 374-89. [DOI] [PubMed] [Google Scholar]
- 12.Weiss SM, Kulikowski CA, Safir A, Amarel A. A model-based method for computer-aided medical decision-making. Artif Intel. 1978;11: 145-62. [Google Scholar]
- 13.Kulikowski CA, Weiss SM. Representation of expert knowledge for consultation: the CASNET and EXPERT projects. In: Szolovits P. (ed). Artificial Intelligence in Medicine. AAAS Selected Symposia Series. Boulder, CO: Westview Press, 1982;2: 21-55. [Google Scholar]
- 14.Nordyke RA, Gilbert FI Jr, Harada ASM. Graves' disease: influence of age on clinical findings. Arch Intern Med. 1988; 148: 626-31. [DOI] [PubMed] [Google Scholar]
- 15.Nordyke RA, Gilbert FI Jr, Harada ASM. Correlation between goiter size and the degree of hyperthyroidism in Graves' disease. Straub Foundation Proceedings. 1986;51: 16-8. [Google Scholar]
- 16.Nordyke RA, Gilbert FI Jr, Miyamoto L. Laboratory monitoring of primary hypothyroidism: use of a newer, more sensitive TSH assay. Postgrad Med. 1986;80(4): 145-9. [DOI] [PubMed] [Google Scholar]
- 17.Nordyke RA, Gilbert FI Jr. Management of primary hypothyroidism. Compr Ther. 1990;16(7): 28-32. [PubMed] [Google Scholar]
- 18.Nordyke RA, Reppun T, Madanay L, Woods J, Goldstein AP, Miyamoto L. Alternative sequences of TSH and FT4 for routine thyroid function testing: quality and cost. Arch Intern Med. 1997; in press. [DOI] [PubMed]
- 19.Nordyke RA, Gilbert FI Jr. Treatment of hypothyroidism: dose and follow-up intervals. Straub Foundation Proceedings. 1990;55(3): 35-6. [Google Scholar]
- 20.Nordyke RA, Gilbert FI Jr. Optimal iodine-131 dose for eliminating hyperthyroidism in Graves' disease. J Nucl Med. 1991;32: 411-6. [PubMed] [Google Scholar]
- 21.Nordyke RA, Gilbert FI Jr. Painful subacute thyroiditis in Hawaii. West J Med. 1991;155: 61-3. [PMC free article] [PubMed] [Google Scholar]
- 22.Nordyke RA, Gilbert FI Jr, Miyamoto LA, Fleury KA. The superiority of antimicrosomal over antithyroglobulin antibodies for detecting Hashimoto's thyroiditis. Arch Intern Med. 1993;153: 862-5. [PubMed] [Google Scholar]
- 23.Gilbert FI Jr, Nordyke RA. Periodic examination of the apparently well individual. Digest 7th Int Conf Med Biol Eng. Stockholm, Sweden. 1967; 178.
- 24.Gilbert FI Jr, Nordyke RA. Automated multiphasic health testing in multispecialty group practice. Prev Med. 1973;1: 261-5. [DOI] [PubMed] [Google Scholar]
- 25.Nordyke RA, Gilbert FI Jr. Share-care clinics. In: Changing Health Care Team. Seattle, WA: Medical Communications Services Association. 1976; 27-31.
- 26.Levison D. Information, computers, and clinical practice. JAMA. 1983;249: 607-9. [PubMed] [Google Scholar]
- 27.McDonald CJ, Tierney WM. Computer-stored medical records. JAMA. 1988;259: 3433-40. [PubMed] [Google Scholar]
- 28.Jollis JG, Ancukiewicz M, DeLong ER, Pryor DB, Mulhbaier MH, Mark DB. Discordance of databases designed for claims payment versus clinical information systems. Ann Intern Med. 1993;119: 844-50. [DOI] [PubMed] [Google Scholar]
- 29.Levy AH, Lawrance DP. Data acquisition and the computer-based patient record. In: Ball MJ, Collen MF (eds). Aspects of the Computer-based Patient Record. New York: Springer-Verlag. 1992;125: 139. [Google Scholar]
- 30.Cote R, Rothwell DJ, eds. Systematized Nomenclature of Medicine (3rd ed). Chicago, IL: College of American Pathologists. 1992.
- 31.Unified Medical Language System. Bethesda, MD: National Library of Medicine.
- 32.Renner AL, Swart JC. Patient core standard for longitudinal health/medicine. Comput Nurs. 1997;15: S7-S13. [PubMed] [Google Scholar]
- 33.McCormick K, Renner AL, Mayes R, Regan J, Greenberg M. The federal and private sector roles in the development of minimum data sets and core health elements. Comput Nurs. 1997;15: S23-S32. [PubMed] [Google Scholar]
- 34.Gabrielli ER. Longitudinal electronic patient records: a challenge of our time. Comput Nurs. 1997;15: S48-S52. [PubMed] [Google Scholar]
- 35.Shortliffe EH, Tang P, Detmer D. Patient records and computers. Ann Intern Med. 1991;115: 979-81. [DOI] [PubMed] [Google Scholar]
- 36.Evans DA, Cimino JJ, Hersh WR, Huff SM, Bell DS. Toward a medical-concept representation language. J Am Med Inform Assoc. 1994;1: 207-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Stead WW, Wiederhold G, Gardner R, Hammond WE, Margolies D. Database systems for computer-based patient records. In: Ball MJ, Collen MF (eds). Aspects of the computer-based patient record. New York: Springer-Verlag. 1992; 83-98.
- 38.Pryor AT. Current state of computer-based patient record systems. In: Ball MJ, Collen MF (eds). Aspects of the computer-based patient record. New York: Springer-Verlag. 1992; 69-93.
- 39.Greenfield S, The state of outcome research: are we on target? N Engl J Med. 1989;320: 1142-3. [DOI] [PubMed] [Google Scholar]
- 40.Jencks SF. Quality assurance. JAMA 1990;263: 2679-80. [PubMed] [Google Scholar]
- 41.Brook RH, Park RE, Chassin MR, Kosecoff J, Keesey J, Solomon DH. Carotid endarectomy for elderly patients: predicting complications. Ann Intern Med. 1990;113: 747-53. [DOI] [PubMed] [Google Scholar]
- 42.Sandrick K. New quality systems have broad impact on physicians, clarify cause of problem. ACP Observer. 1991; April: 1-19.
- 43.Relman A. Reforming the health care system. Group Practice J. 1991;40(1): 18-20. [Google Scholar]
- 44.Griner PF, Huth E. Research in general internal medicine. Ann Intern Med. 1982;96: 518-9. [DOI] [PubMed] [Google Scholar]
- 45.Houle CO. Continuing Learning in the Professions. San Francisco, CA: Jossey-Bass. 1980; 208-9.
- 46.Manning PR, Petit DW. The past, present and future of continuing medical education. Achievements and opportunities, computers and re-certification. JAMA. 1987;258(24): 3542-6. [PubMed] [Google Scholar]
- 47.Barnett O. Computers in medicine. JAMA. 1990;263(19): 2631-3. [PubMed] [Google Scholar]
- 48.Dick RS, Steen EB (eds). The Computer-based Patient Record: An Essential Technology for Health Care. Washington, DC: National Academy Press. 1991; 132-52. [PubMed]
- 49.Krasner JB. Computer and medical practice: an auspicious union. In: Nash DB (ed): Future Practice Alternatives in Medicine. New York: Igaku-Shoin. 1987.