

Abstract
Objectives
Open gingival embrasures leading to appearance of black triangles which apart from being unesthetic contribute towards food retention, adversely affecting the health of the periodontium. Correction of such papillary deformities is extremely challenging, which requires an in depth knowledge about the interproximal geometry for the appropriate management of interdental papilla. So, the present study was aimed to determine the proximal contact areas of maxillary anterior teeth and their influence on the interdental papilla.
Materials and methods
In 200 periodontally healthy patients equally divided into 21–40 years (Group I) and 41–60 years (Group II) of age group amounting to a total of 1400 interdental papillae in maxillary anterior teeth were examined to compute the apicocoronal Proximal contact area (PCA), Proximal contact area proportion (PCAP), and dimensions between alveolar crest and apical contact point (D1) to assess their influence on presence or absence of interdental papilla.
Results
The PCA dimensions were maximum for Central incisor-Central incisor measuring about 3.90 ± 0.93 mm and 3.97 ± 0.90 mm for Group I males and females respectively and 3.86 ± 1.22 mm and 3.63 ± 1.14 mm for males and female patients in Group II respectively. There was a gradual reduction till Canine-Premolar. Similar trend was followed in PCAP and D1. Consistently more dimensions of D1 were observed in Group II as compared to Group I which influenced the presence of papilla which was predominantly found in Group I patients amongst both the sexes.
Conclusion
There was a gradual decrease in the PCA and PCAP in the distal direction anteroposteriorly from maxillary central incisors to first premolars on either sides. The younger age group of both the sexes exhibit greater presence of interdental papilla owing to the lesser D1 dimensions as compared to the older patients.
Keywords: Interdental papilla, Proximal contact, Esthetic
1. Introduction
The presence of intact interdental papilla, one of the constituents of healthy gingiva, is of prime importance which needs to be considered for diagnosis and treatment of periodontal and restorative anomalies (Kolte et al., 2014, Murphy, 1996). The clinicians have been striving not only to restore the loss of function but also to achieve a pleasing esthetics especially in the anterior sextant which satisfies the aspiration of the patients to bear a beautiful smile.
Open gingival embrasures, leading to appearance of black triangle, are potentially attributed to multifactorial etiology. This includes dimensional changes in the interdental papilla during teeth alignment, alveolar bone destruction, gingival recession, length of embrasures, crown shapes and interproximal contact position (Cardaropoli and Re, 2005). Apart from being unesthetic the black triangles also contribute towards food retention, adversely affecting the health of the periodontium. Correction of such papillary deformities is extremely challenging, which requires profound knowledge of the interproximal geometry and an interdisciplinary team approach for an appropriate management of interdental papilla and gingival embrasure form. Several clinical and radiographic trials have elaborated on the influence of interproximal distance between roots (Cho et al., 2006) crown height and relative bone length (Kolte et al., 2016a, Kolte et al., 2016b) distance of contact point to the crest of alveolar bone (Tarnow et al., 1992) and other such factors on the presence or absence of interdental papilla.
Current literature identifies the location of contact point in an apicoincisal direction for anterior maxillary teeth and the term contact point and contact area have been used interchangeably to describe the same (Ash, 1993, Krauss, 1991). The relevance of contact point lies in the fact that it defines the gingival embrasure and this is supposed to have an impact on the height of the interdental papilla (Martegani et al., 2007, Chu et al., 2009a, Chu et al., 2009b) and the incisal embrasure. True point contact needs to be differentiated from proximal contact areas as the former appear when contacting surfaces exhibit perfect curvatures and are commonly observed in young patients, while the latter appear in anterior dentition amongst the adults. Periodontal and restorative procedures directed towards restoring the white and pink proportions in the anterior sextants need to identify contact points or areas with differing locations and dimensions. With the prevailing differences in perception of dental esthetics, efforts need to be made to establish common standards to guide the clinicians.
The concept of connector space or zone as defined by Morley and Eubank (2001) is a longer and broader area than a contact point or area usually 2 mm × 2 mm in dimensions. This concept was further elaborated in relationship to the connector zone for maxillary anterior teeth as a percentage of maxillary central incisor crown height referred to as the 50-40-30 rule (Morley, 2000) This rule is a preliminary effort in describing the visual perception of the contact area but lacks supporting quantitative research.
Considering the lack of understanding owing to limited investigations in the literature with regards to location and the apico-incisal dimensions of proximal contact areas, this study was planned to determine the proximal contact areas of maxillary anterior teeth and their influence on the interdental papilla.
2. Materials and methods
The study population comprised of 200 periodontally healthy patients, randomly selected from those visiting the Department of Periodontics and Implantology of our Institute. These patients were equally divided into two groups based on their age as:
Group I: Periodontally healthy patients with age range from 21 to 40 years and
Group II: Periodontally healthy patients with age range from 41 to 60 years.
The male and female patients were equal in numbers in both the groups and were recruited between June 2015 to August 2016. All the patients were informed about the nature of the study and their written consent was obtained. The study protocol was approved from the Institutional Ethics Committee and confirmed with the Helsinki Declaration. Inclusion criteria for the study population was patients with fully erupted maxillary anterior teeth possessing tight proximal contacts and healthy gingiva with Plaque index (Sillness and Loe, 1964) and Gingival index (Loe and Silness, 1963) score of 0–1. Patients with a history of mucogingival surgery, periodontal pathologic conditions, trauma or congenital defects, multiple diastema, currently undergoing orthodontic treatment and possessing crowns or prosthetic restorations were excluded. The patients were taken up for phase I therapy involving instructions in oral hygiene and scaling and root planing to ensure complete elimination of inflammation, if any, that was present. Two weeks later, a detailed examination was conducted which confirmed the absence of inflammation and then study models were prepared for all the patients with alginate impressions using irreversible hydrocolloid material (Septodont, Marieflex) which were disinfected and then immediately poured with stone (Neelkanth, Stone Plaster). Measurements of a total 1400 interdental sites of maxillary anterior teeth from first premolar to the contra lateral first premolar were measured with a digital caliper (Workzone, Digital Caliper 6 in./150 mm LCD display, Shandong, China) and 2.5× optical loupes. The measurements included crown length and width (Chu et al., 2009a, Chu et al., 2009b), proximal contact area (Stappert et al., 2010) crown width/length ratio and interdental papilla estimation which was done with visual examination after isolation and drying of the interdental area (see Fig. 1, Fig. 2). Papilla was considered to be present when it filled the entire interproximal space up to the contact point and absent when it did not completely fill the interproximal space, leading to appearance of black triangle. Proximal contact area (PCA) in an apicoincisal direction was considered from the apical most point of contact area to the coronal most incisal point. The proximal contact area proportion (PCAP) was calculated through mathematical equation which yielded the percentage ratio.
Fig. 1.
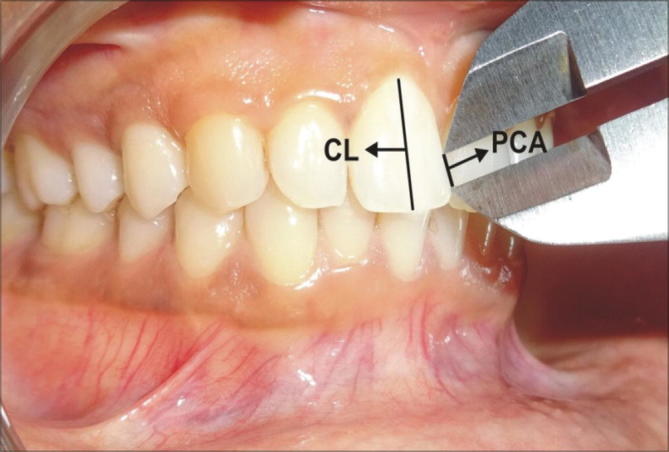
Healthy gingiva having tight interproximal contacts between maxillary anterior teeth showing Proximal contact area (PCA), Crown length (CL).
Fig. 2.

Clinical Measurement of Proximal contact area with the digital calliper Proximal contact area (PCA) Crown length (CL).
The distance from bone crest to contact point (D1) in each interdental area was assessed radiographically (Digora Optime RVG software) using the paralleling technique. The clinical parameters recorded included Plaque index (PI), Gingival index (GI) and assessment of interdental papilla. All the clinical parameters were recorded by the first examiner (RK) and study model measurements were done by second examiner (PB), who were calibrated by repeating respective measurements in a pilot study.
3. Statistical analysis
Continuous variables (PCA, PCAP and D1) were presented as Mean ± SD. Categorical variables were expressed in actual numbers and percentages. Continuous variables were compared between 4 groups by performing oneway ANOVA. Multiple comparison was carried out to compare difference between any 2 groups by performing Bonferroni-t test. For comparing these variables between Group I and Group II by performing independent t-test. Categorical variable were compared by performing Pearson’s chi square test. P < 0.05 was considered as statistical significance. Statistical software STATA Version 14.0 was used for data analysis.
4. Results
The descriptive values of mean PCA, PCAP, D1 and the presence of papilla in each maxillary anterior interdental area are presented in Table 1. The mean PCA dimensions were found to be maximum between central incisors (CI/CI) which then gradually reduced between central incisor-lateral incisor (CI/LI), lateral incisor-canine (LI/CA) and the least were found with canine-premolar (CA/PM). The mean PCA for males and females between central incisors (CI/CI) was 3.90 ± 0.93 mm and 3.97 ± 0.90 mm in Group I, while it was 3.86 ± 1.22 mm and 3.63 ± 1.14 mm for males and female patients in Group II respectively. The least PCA dimensions were found between PM/CA where the mean values were 1.98 ± 0.58 mm and 1.81 ± 0.55 mm for males and female patients in Group I while it was 1.92 ± 0.64 mm and 1.82 ± 0.59 mm for males and female patients in Group II respectively. On the contra lateral side, the PCA dimensions of CA/PM for males and females were 2.24 ± 0.54 mm and 1.99 ± 0.59 mm in Group I and 2.20 ± 0.61 mm and 2.07 ± 0.59 mm for males and females in Group II respectively.
Table 1.
Descriptive statistics for PCA, PCAP, D1 and papilla presence between maxillary anterior teeth.
| Interdental area | Group | PCA | PCAP | D1 | Papilla present |
|---|---|---|---|---|---|
| PM/CA (14/13) | Group I/M | 1.98 ± 0.58 | 25.58 ± 7.73 | 4.5 ± 0.55 | 49(98%) |
| Group I/F | 1.81 ± 0.55 | 25.84 ± 6.94 | 4.33 ± 0.71 | 48(96%) | |
| Group II/M | 1.92 ± 0.64 | 23.83 ± 7.21 | 4.92 ± 0.92 | 24(48%) | |
| Group II/F | 1.82 ± 0.59 | 25.66 ± 7.14 | 4.46 ± 0.66 | 13(26%) | |
| CA/LI (13/12) | Group I/M | 2.32 ± 0.70 | 24.93 ± 6.74 | 4.44 ± 0.86 | 49(98%) |
| Group I/F | 2.25 ± 0.59 | 26.69 ± 8.03 | 4.41 ± 0.65 | 48(96%) | |
| Group II/M | 2.48 ± 0.85 | 25.87 ± 8.88 | 4.96 ± 1.22 | 24(48%) | |
| Group II/F | 2.26 ± 0.65 | 26.85 ± 8.28 | 4.44 ± 0.59 | 13(26%) | |
| LI/CI (12/11) | Group I/M | 5.31 ± 0.62 | 38.70 ± 6.80 | 4.71 ± 0.99 | 37(74%) |
| Group I/F | 3.19 ± 0.82 | 41.36 ± 10.40 | 4.6 ± 0.78 | 42(84%) | |
| Group II/M | 3.35 ± 0.82 | 38.79 ± 0.64 | 5.25 ± 1.20 | 23(46%) | |
| Group II/F | 3.13 ± 0.88 | 39.52 ± 10.22 | 4.64 ± 0.80 | 16(32%) | |
| CI/CI (11/21) | Group I/M | 3.90 ± 0.93 | 38.40 ± 8.50 | 5.06 ± 1.01 | 39(78%) |
| Group I/F | 3.97 ± 0.90 | 42.36 ± 9.59 | 4.87 ± 0.77 | 41(82%) | |
| Group II/M | 3.86 ± 1.22 | 38.06 ± 10.65 | 5.58 ± 1.03 | 24(48%) | |
| Group II/F | 3.63 ± 1.14 | 36.82 ± 10.56 | 5.42 ± 0.82 | 16(32%) | |
| CI/LI (21/22) | Group I/M | 3.44 ± 0.64 | 39.94 ± 7.95 | 4.47 ± 0.83 | 44(88%) |
| Group I/F | 3.05 ± 0.3 | 39.26 ± 12.69 | 4.36 ± 0.69 | 43(86%) | |
| Group II/M | 3.39 ± 0.83 | 38.50 ± 7.44 | 5.41 ± 1.16 | 23(46%) | |
| Group II/F | 3.37 ± 1.25 | 39.19 ± 12.74 | 5.21 ± 0.94 | 13(26%) | |
| LI/CA (22/23) | Group I/M | 2.57 ± 0.62 | 26.80 ± 6.12 | 4.44 ± 0.57 | 47(94%) |
| Group I/F | 2.48 ± 0.58 | 29.45 ± 9.44 | 4.3 ± 0.61 | 47(94%) | |
| Group II/M | 2.67 ± 0.67 | 27.15 ± 5.78 | 4.94 ± 0.85 | 23(46%) | |
| Group II/F | 2.65 ± 0.67 | 28.69 ± 7.27 | 4.98 ± 0.78 | 15(30%) | |
| CA/PM (23/24) | Group I/M | 2.24 ± 0.54 | 28.3 ± 6.51 | 4.46 ± 0.57 | 47(94%) |
| Group I/F | 1.99 ± 0.59 | 28.90 ± 10.32 | 4.35 ± 0.57 | 46(92%) | |
| Group II/M | 2.20 ± 0.61 | 27.34 ± 6.15 | 4.82 ± 0.73 | 23(46%) | |
| Group II/F | 2.07 ± 0.59 | 26.95 ± 6.35 | 4.87 ± 0.68 | 15(30%) | |
PCA = Proximal contact area, PCAP = Proximal contact area proportion, D1 = Distance from bone crest to apical contact point.
The PCAP and D1 followed a similar trend and was found to be more with CI/CI, LI/CI and CI/LI which later on decreased from mesial to distal sites in the maxillary anterior dentition bilaterally. This gradual decrease in D1 from midline to laterally is reflected in the presence of papilla in the interdental area which is inversely related to D1 especially in Group I patients both males and females.
The descriptive statistics of mean PCA, PCAP and D1 are presented in Table 2, according to age groups. There is consistently more D1 dimensions in Group II as compared to Group I in each of interdental sites and these differences were found to be statistically significant for PM/CA, CA/LI and LI/CI while the difference was highly significant with CI/CI, CI/LI, LI/CA and CA/PM (p < 0.0001).
Table 2.
Descriptive statistics comparing PCA, PCAP and D1 between Group I and Group II.
| Interdental area | Group | PCA | PCAP | D1 |
|---|---|---|---|---|
| PM/CA (14/13) | Group I M/F | 1.89 ± 0.57 | 25.71 ± 7.31 | 4.41 ± 0.64 |
| Group II M/F | 1.87 ± 0.62 | 24.75 ± 7.20 | 4.69 ± 0.64 | |
| p-value | 0.02(0.7830), NS | 0.95(0.3519), NS | 0.27(0.0107), S | |
| CA/LI (13/12) | Group I M/F | 2.29 ± 0.65 | 25.81 ± 7.43 | 4.42 ± 0.60 |
| Group II M/F | 2.37 ± 0.45 | 26.34 ± 8.76 | 4.74 ± 0.80 | |
| p-value | 0.08(0.3906), NS | 0.55(0.6269), NS | 0.27(0.0189), S | |
| LI/CI (12/11) | Group I M/F | 3.25 ± 0.73 | 40.13 ± 8.83 | 4.65 ± 0.89 |
| Group II M/F | 3.24 ± 0.86 | 39.16 ± 9.42 | 4.94 ± 1.06 | |
| p-value | 0.008(0.9421), NS | 0.97(0.4506), NS | 0.29(0.0380), S | |
| CI/CI (11/21) | Group I M/F | 3.94 ± 0.91 | 40.52 ± 9.26 | 4.96 ± 0.90 |
| Group II M/F | 3.74 ± 1.18 | 37.44 ± 10.57 | 5.50 ± 0.93 | |
| p-value | 0.1924, NS | 0.0298, S | 0.0001, HS | |
| CI/LI (21/22) | Group I M/F | 3.25 ± 0.71 | 39.60 ± 10.54 | 4.41 ± 0.76 |
| Group II M/F | 3.38 ± 1.05 | 38.84 ± 10.39 | 5.31 ± 1.06 | |
| p-value | 0.2901, NS | 0.6087, NS | <0.0001, HS | |
| LI/CA (22/23) | Group I M/F | 2.52 ± 0.60 | 28.12 ± 8.03 | 4.37 ± 0.59 |
| Group II M/F | 2.66 ± 0.67 | 27.92 ± 6.58 | 4.96 ± 0.86 | |
| p-value | 0.1274, NS | 0.8440, NS | <0.0001, HS | |
| CA/PM (23/24) | Group I M/F | 2.11 ± 0.58 | 28.61 ± 8.59 | 4.40 ± 0.65 |
| Group II M/F | 2.13 ± 0.60 | 27.14 ± 6.22 | 4.84 ± 0.78 | |
| p-value | 0.016(0.8448), NS | 1.46(0.1677), NS | 0.44(<0.0001), HS | |
PCA = Proximal contact area, PCAP = Proximal contact area proportion, D1 = Distance of bone crest to apical contact point, NS = Non-significant, S = Significant, HS = Highly significant.
5. Discussion
In search of definitive guidelines for attaining esthetics in relation to the proportionate existence of white and pink components, several clinical trials have been reported in the literature pertaining to PCA locations (de Castro et al., 2006, Sarver, 2004). In the present clinical trial, it was observed that PCA dimension for CI/CI was the maximum amongst the anterior dentition, both in males and females of both the age groups and as the measurements were recorded distally on either sides, there was a gradual reduction. This indicates that the proximal contact area reduces as we move distally from the midline in the maxillary dentition. These findings are similar to those obtained by Stappert et al. (2010), but the authors did not comment about age and gender variability due to the limited and unspecified study population. In our study, it was revealed that for all the interproximal contact areas the dimensions of PCA were more in males as compared to the females. This could be attributed to the squarish crown morphology found predominantly in males while triangular or tapered squarish one in females (Kolte et al., 2016a, Kolte et al., 2016b, Gobbato et al., 2012). Also it was revealed in Group I patients that with the decrease in PCA, there was an increase in the presence of papilla, however this inverse relationship was not observed in Group II patients. This could be probably because there was a greater increase in the alveolar crest to apical contact point distance with Group II patients. These findings suggest an inverse relationship between PCA and presence of papilla especially in younger age group.
With regards to PCAP, it has been established that numerically a percentage of 40-30-20-20 existed with mean individual tooth height dimensions for anterior maxillary teeth (Stappert et al., 2010). The results of our study clearly are not in agreement to this observation, because of the fact that we obtained higher values of PCAP for LI/CI and CA/PM on either sides. This difference in the PCAP values in our study appears to be more reasonable as we had equal gender distribution along with well accounted age grouping in the study population. Also there is always an influence of the population examined in different studies.
It was also noted that D1 was comparatively more for CI/CI, while there was an extremely gradual reduction on the distal interproximal areas. This has been aptly reflected in the presence of interdental papilla, the percentage of which was more with the reduction in D1 dimensions. These findings are similar to the ones reported in previous studies (Kolte et al., 2016a, Kolte et al., 2016b, Tarnow et al., 1992) where it has been mentioned that presence of interdental papilla is strongly and inversely proportional to the vertical dimensions between alveolar crest and contact point. An interesting feature of our study is the fact that in majority of the patients belonging to younger age group all the interproximal areas revealed presence of interdental papilla, when compared to the older patients, thus indicating a strong association with age. It is also evident that the gingival papilla in between CI/CI and CI/LI on either sides is extremely sensitive and demonstrates a greater frequency of papillary recession as compared to the other interproximal sites. These being the most prominent sites in the esthetic zone, they pose even more challenges for the clinician in restoring the papillary component.
6. Conclusion
Within the limits of our study, it can be inferred that, it is more appropriate to recognise PCA’s instead of the proximal contact points, while planning for any periodontal or restorative procedures in the maxillary anterior sextants. There is a gradual decrease in the PCA and PCAP in the distal direction anteroposteriorly from maxillary central incisors to first premolars on either sides. D1 dimensions were observed to be consistently more in Group II indicating the age variability which inturn influenced the presence of interdental papilla. The younger age group of both the genders exhibited greater presence of interdental papilla as compared to the older patients. Further investigations in different populations are desired to formulate universal guidelines for restoring esthetics in maxillary anterior teeth in a clinical and/or laboratory setting.
Authors’ contributions
The authors contributed in the following way:
Dr. Abhay Kolte: Concept and design of the study, literature search, data analysis and manuscript preparation as well as editing.
Dr. Rajashri Kolte: Design, definition of intellectual content, literature search, clinical studies, data analysis, manuscript preparation as well as editing.
Dr. Pranjali Bawankar: Definition of intellectual content, literature search, clinical studies, experimental studies and data acquisition.
Acknowledgments
Acknowledgments
None.
Funding
Not applicable.
Competing interests
The authors declare no competing interests with regards to the authorship and/or publication of this article.
Ethics approval
Institutional ethical committee Reference Number: IEC/VSPMDCRC/11/2016.
Footnotes
Peer review under responsibility of King Saud University.
References
- Ash M.M. Physiologic form of teeth and periodontium. In: Ash M.M., Nelson S., editors. Wheelers Dental anatomy, Physiology and Occlusion. WB Saunders; Philadelphia: 1993. pp. 102–127. [Google Scholar]
- Cardaropoli D., Re S. Interdental papilla augmentation procedure following orthodontic treatment in a periodontal patient. J. Periodontol. 2005;76:655–661. doi: 10.1902/jop.2005.76.4.655. [DOI] [PubMed] [Google Scholar]
- Chu S.J., Tan J.H., Stappert C.F., Tarnow D.P. Gingival zenith positions and levels of the maxillary anterior dentition. J. Esthet. Restor. Dent. 2009;21:113–120. doi: 10.1111/j.1708-8240.2009.00242.x. [DOI] [PubMed] [Google Scholar]
- Chu S.J., Tarnow D.P., Tan J.H., Stappert C.F. Papilla proportions in the maxillary anterior dentition. Int. J. Periodont. Restorat. Dent. 2009;29:385–393. [PubMed] [Google Scholar]
- de Castro M.V., Santos N.C., Ricardo L.H. Assessment of the “golden proportion” in agreeable smiles. Quintessence Int. 2006;37:597–604. [PubMed] [Google Scholar]
- Gobbato L., Tsukiyama T., Levi P.A., Jr, Griffin T.J., Weisgold A.S. Analysis of the shapes of maxillary central incisors in a Causcasian population. Int. J. Periodont. Restorat. Dent. 2012;32:69–78. [PubMed] [Google Scholar]
- Cho Hae-Sung, Jang Hyum-Seon, Kim Dong-Kie, Park Joo-Cheol, Kim Heung-Joong, Choi Seong-Ho. The effect of interproximal distances between roots on the existence of interdental papillae according to the distances from the contact point to the alveolar crest. J. Periodontol. 2006;77:1651–1657. doi: 10.1902/jop.2006.060023. [DOI] [PubMed] [Google Scholar]
- Kolte A., Kolte R., Bodhare G. Association between the central papilla and embrasure crown morphology in different gingival biotypes – a cross sectional study. Int. J. Esthet. Dent. 2016;11:550–564. [PubMed] [Google Scholar]
- Kolte A.P., Kolte R.A., Mishra P.R. Dimensional influence of interproximal areas on existences of interdental papillae. J. Periodontol. 2014;85:795–801. doi: 10.1902/jop.2013.130361. [DOI] [PubMed] [Google Scholar]
- Kolte A.P., Kolte R.A., Pajnigara N.G., Pajnigara N.G. A clinical and radiographic assessment of positional variations of gingival papilla and its proportions. Int. J. Periodont. Restorat. Dent. 2016;36:213–218. doi: 10.11607/prd.2464. [DOI] [PubMed] [Google Scholar]
- Krauss B.S. Mosby; St. Louis: 1991. Dental Anatomy and Occlusion. [Google Scholar]
- Loe H., Silness J. Periodontal disease in pregnancy. I. Prevalence and severity. Acta Odontol. Scand. 1963;21:533–551. doi: 10.3109/00016356309011240. [DOI] [PubMed] [Google Scholar]
- Martegani P., Silvestri M., Mascarello F., Scipioni T., Ghezzi C., Rota C. Morphometric study of the interproximal unit in the estheic region to correlate anatomic variables affecting the aspects of soft tissue embrasure space. J. Periodontol. 2007;78:2260–2265. doi: 10.1902/jop.2007.060517. [DOI] [PubMed] [Google Scholar]
- Morley J. A multidisciplinary approach to complex esthetic restoration with diagnostic planning. Pract. Periodont. Aesthet. Dent. 2000;12:575–577. [PubMed] [Google Scholar]
- Morley J., Eubank J. Macroesthetic elements of smile design. J. Am. Dent. Assoc. 2001;132:39–45. doi: 10.14219/jada.archive.2001.0023. [DOI] [PubMed] [Google Scholar]
- Murphy K.G. International tissue maintenance in GTR procedures: description of a surgical technique and 1-year reentry result. Int. J. Periodont. Resorat. Dent. 1996;16:463–477. [PubMed] [Google Scholar]
- Sarver D.M. Principles of cosmetic dentistry in orthodontics: Part 1. Shape and proportionality of anterior teeth. Am. J. Orthod. Dentofacial Orthop. 2004;126:749–753. doi: 10.1016/j.ajodo.2004.07.034. [DOI] [PubMed] [Google Scholar]
- Sillness J., Loe H. Periodontal disease in pregnancy. II. Correlation between oral hygiene and periodontal condition. Acta Odontol. Scand. 1964;22:121–135. doi: 10.3109/00016356408993968. [DOI] [PubMed] [Google Scholar]
- Stappert C.F., Tarnow D.P., Chu S.J. Proximal contact areas of the maxillary anterior dentition. Int. J. Periodont. Restorat. Dent. 2010;30:471–477. [PubMed] [Google Scholar]
- Tarnow D.P., Magner A.W., Fletcher P. The effect of the distance from the contact point to the crest of bone on the presence or absence of the interproximal dental papilla. J. Periodontol. 1992;63:995–996. doi: 10.1902/jop.1992.63.12.995. [DOI] [PubMed] [Google Scholar]