

Abstract
Objective
To examine how point-of-sale (POS) display bans, tobacco retailer density, and tobacco retailer proximity were associated with smoking cessation and relapse in a cohort of smokers in Canada, where provincial POS bans were implemented differentially over time from 2004 to 2010.
Methods
Data from the 2005 to 2011 administrations of the International Tobacco Control (ITC) Canada Survey, a nationally representative cohort of adult smokers, were linked via residential geocoding with tobacco retailer data to derive for each smoker a measure of retailer density and proximity. An indicator variable identified whether the smoker’s province banned POS displays at the time of the interview. Outcomes included: cessation for at least one month at follow-up among smokers from the previous wave and relapse at follow-up among smokers who had quit at the previous wave. Logistic generalized estimating equation models were used to determine the relationship between living in a province with a POS display ban, tobacco retailer density, and tobacco retailer proximity with cessation (n=4388) and relapse (n=866).
Results
Provincial POS display bans were not associated with cessation. In adjusted models, POS display bans were associated with lower odds of relapse, which strengthened after adjusting for retailer density and proximity, although results were not statistically significant (OR 0.66, 95% CI 0.41, 1.07, P-value=0.089). Neither tobacco retailer density nor proximity was associated with cessation or relapse.
Conclusions
Banning POS retail displays shows promise as an additional tool to prevent relapse, although these results need to be confirmed in larger longitudinal studies.
INTRODUCTION
As traditional tobacco marketing channels have been prohibited, tobacco companies have transitioned their marketing resources from mass media (e.g., television, billboards) to point-of-sale (POS) in tobacco retail shops (e.g., interior and exterior ads, extensive price promotions and discounts, product displays).[1–3] In addition to POS marketing, the density and proximity of tobacco retailers to residential areas are critical for making tobacco easily available.[4] Marketing exposures and tobacco availability (i.e., density and residential proximity to tobacco retailer) have been found to impede smoking cessation.[5–9] However, the independent effects of POS marketing and retail availability on cessation and relapse have not been examined rigorously.
The Transtheoretical Model of Health Behavior Change suggests two key smoking cessation stages beyond making a quit attempt (Action) that are relevant to POS marketing exposures: staying off of cigarettes (Maintenance) and returning to smoking (Relapse).[10] The effects of tobacco marketing likely vary across stages. Tobacco marketing at POS can serve as smoking cues, which increase cravings and smoking behavior.[11–13] Environmental cues to smoke appear to have a greater impact on intermittent smokers than daily smokers,[14] which may have corollaries with former smokers in the Maintenance stage: once quit, former smokers may respond more strongly to environmental cues, such as tobacco marketing at POS, than addicted smokers who continue smoking for nicotine. If so, cues from tobacco marketing at POS may play a stronger role for cessation or relapse than for making a quit attempt initially. Indeed, prior quantitative [5, 8] studies are suggestive of these ideas, finding that sensitivity and exposure to POS marketing were associated with lower odds of cessation, but exposure to POS marketing was not associated with quit attempts.[8] The quantitative findings are further supported by qualitative work showing that POS marketing made cessation more difficult, and relapse more likely, due to temptation and increased cravings.[6]
Little is known about the role of tobacco availability on cessation and relapse. One study in Texas found that closer residential proximity to tobacco retailers, though not tobacco retailer density, was associated with lower odds of cessation,[7] while a similar study in England found no relationship between tobacco retail density or proximity with cessation.[15] Another US study found that greater distance from a tobacco retailer was associated with higher 30-day abstinence, and greater density was associated with lower abstinence, but only in high poverty areas; results were null in low poverty areas.[16] Greater density and closer proximity were both associated with lower cessation among men, but not women, who smoked moderately or heavily at baseline in a Finnish study; however, proximity was associated with lower probability of cessation among women who were light smokers at baseline.[9] Another Finnish study found that decreased proximity was associated with increased quitting but not with relapse.[17] In Canada, retail density was associated with greater odds of making a quit attempt but not relapse, and proximity was not associated with either quit attempts or relapse.[18] These mixed results suggest a need for larger, longitudinal studies that are better positioned to discriminate between the effects of retail density and proximity, including when also accounting for POS displays.
Most studies investigating the effects of POS marketing on adult smokers are limited to non-representative samples or qualitative inquiries.[5, 6, 8, 19–22] Furthermore, none of these studies disentangle the influence of POS marketing from tobacco availability on smoking behavior outcomes. One way to separate out these different effects is by looking across geographic areas with disparate POS display policies. Canada offers such an opportunity, as provinces and territories implemented POS display bans differentially over time between 2004 and 2010.[23] Although Canada had previously banned POS marketing,[24] the new provincial laws banned the display of tobacco products. In the present study involving a nationally representative cohort of Canadian adult smokers, we took advantage of the set of natural experiments across different provinces to examine variation in POS display bans, and data on likely tobacco retailers to measure tobacco availability (i.e., density and residential proximity to tobacco retailer). We hypothesized that living in a province with a POS display ban would be associated with greater cessation and lower probability of relapse. We also hypothesized that higher tobacco availability would be associated with lower cessation and higher probability of relapse.
METHODS
Study Setting
Between 2004 and 2010, all ten Canadian provinces implemented bans of retail displays of tobacco products, albeit differentially over time.[23] Bans were implemented in Manitoba, Saskatchewan, and Prince Edward Island prior to the beginning of our study period in October 2006; in Nova Scotia in March 2007; in British Columbia, Ontario, Quebec, and Alberta between March and July 2008 (corresponding to a period between study waves); in New Brunswick in January 2009; and in Newfoundland and Labrador in January 2010 (Figure 1).
Figure 1.
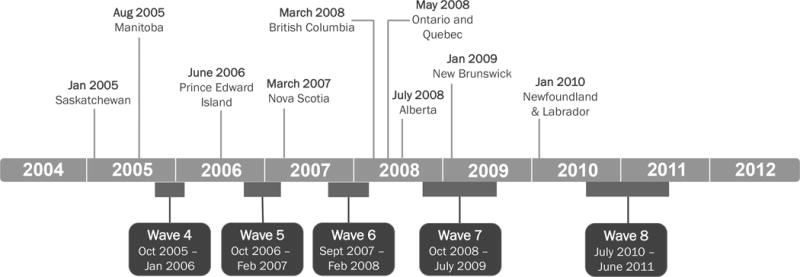
Timeline for Canada ITC data collection and timing of POS display ban implementation by province.
Population
We analyzed data from the International Tobacco Control (ITC) Canada Survey, a population-based, longitudinal survey of a nationally representative sample of 2000 adult smokers,[25] using data from four survey waves spanning 4.5 years: Wave 5 (October 2006 to February 2007), Wave 6 (September 2007 to February 2008), Wave 7 (October 2008 to July 2009), and Wave 8 (July 2010 to April 2011). From an initial sample size of 3105 individuals (n=8027 observations), we excluded participants without information on province (n=76 participants, n=112 observations) and those from Prince Edward Island (n=16 participants, n=36 observations) due to the small sample and the need to adjust for tobacco control environment by province. After these exclusions, we had a total of 7879 observations from 3013 participants. We further excluded observations for missing tobacco retail exposure data (n=228 participants, n=1105 observations) and covariates (n=7 participants, n=25 observations). After exclusion criteria were applied, we divided the dataset into two analytic samples for each outcome of interest: cessation (n=4388 observations, 2024 individuals) and relapse (n=866 observations, 448 individuals). The analytic samples were defined based on respondents smoking status at times t and t+1. Specifically, the cessation sample consisted of respondents who were smokers at time t, whereas the relapse sample included respondents who had quit smoking for at least 30 days at time t.
Measures
Smoking cessation and relapse
Two dependent variables were evaluated: smoking cessation and relapse. A smoker was considered to have achieved cessation if he/she was smoking at the previous wave, but had quit for at least one month, and was still quit at the time of being surveyed. A person who had quit smoking at the last survey wave and was back to smoking at the present wave was considered to have relapsed.
POS ban on tobacco products
To assess exposure to the provincial POS ban policy, participants were assigned an indicator variable with “Yes” representing a ban in their province before their interview date, and “No” representing no ban.
Tobacco retailer density and proximity
The Canadian retailer data were obtained from Enhanced Points of Interest database from Desktop Mapping Technologies Inc (DMTI-EPOI),[26] which has been used in prior research on tobacco retail density around Canadian schools,[27] and is the most complete database of retailers over time. Grocery stores, gasoline service stations, and tobacco stores and stands were coded as tobacco retailers in all provinces.[28–31] In a sensitivity analysis, we also included drug stores and liquor stores as tobacco retailers for provinces that sold tobacco through those locations. They were not included in the main analysis, as these types of stores are less likely to sell cigarettes, few ITC participants report purchasing cigarettes from these venues (analysis not shown), and only British Columbia allowed sales in liquor stores. The DMTI-EPOI database is updated annually, thus data from 2007 to 2010 were used in this study, corresponding to the dates of the ITC surveys analyzed.
We calculated tobacco retailer density and proximity relative to study participants’ residential addresses. Participants’ street addresses (92.5% of sample) or postal codes (assigned to postal code centroids; 7.5%) from the ITC Canada data were geocoded using DMTI’s street network and postal code locations, or ArcGIS’s online North America Geocode Service 10.0 if the first method did not work. Tobacco retailer density was calculated as the number of tobacco retailers within a 1 km radius from a participant’s residence using ARCGIS’s proximity tools. We used a 1 km radius rather than the commonly used 500m due to the low population density in Canada, especially in rural areas and small towns. Tobacco retailer proximity was the measurement of the closest tobacco retailer (i.e., grocery store, gasoline service station, or tobacco store or stand) to a participant’s residence, calculated using Euclidean distance via ARCGIS’s proximity tools, measured in km.
Covariates
Covariates included in the models were age, sex, education, income, province, and cigarette prices. Education was categorized as: high school, some post-secondary education, completed university (referent). Annual income level in Canadian dollars (CAD) was categorized as: under $29,999; $30,000-59,999; $60,000-74,999; $75,000-99,999; $100,000 and over (referent); refused/don’t know. Cigarette prices measured the average cigarette price (per 200 cigarettes) for each province for each survey year.[32] Additionally, provincial indicators were used to adjust for the tobacco control environment in each province over time. We also adjusted for quit attempts in the cessation models, defined as a smoker making an attempt to stop smoking since the previous wave. We did not adjust for survey year due to collinearity with the POS ban indicator variable (Spearman’s correlation: ρ=0.81 cessation sample, ρ=0.85 relapse sample).
Statistical Analysis
We calculated unweighted descriptive statistics for all variables of interest for each analytic sample at each survey wave. Generalized estimating equation (GEE) logistic regression models accounted for the within-person correlation over time and modeled the relationship between POS display bans, tobacco retailer density, and tobacco retailer proximity with smoking cessation variables. To evaluate these relationships, we estimated seven models for each of the outcomes studied (i.e., cessation and relapse), measuring exposure in the same wave as the outcome. First, we modeled the crude association for each exposure and outcome, and then adjusted for covariates. Finally, we modeled all three exposure variables simultaneously in a fully adjusted model. Models 1, 3, and 5 examined the crude association between each exposure (i.e., POS display ban, retailer density, retailer proximity) and the outcome variable. Models 2, 4, and 6 included covariates (i.e., age, sex, education, income, province, cigarette price, quit attempts in the cessation models). Model 7 examined all three exposure variables (i.e., POS ban, density, proximity) with cessation and relapse, adjusting for covariates. All GEE analyses were conducted in SAS 9.3 and accounted for the complex survey design by incorporating strata and weights that were constructed to be representative of the population.
We conducted multiple sensitivity analyses. First, we included drug stores and liquor stores in our calculations of tobacco retail density and proximity. Second, because of the uncertainty with geocoding rural versus urban addresses, we conducted an analysis excluding rural participants. We also adjusted for heaviness of smoking index (HSI) from the prior wave in the cessation analysis and examined time-in-sample for cessation and relapse models. Finally, we examined whether adjusting for self-reported exposure to workplace, restaurant, and bar smoke-free policies affected the results from both cessation and relapse models.
RESULTS
The mean age of study participants was between 47 and 53 years, and 56 to 63% of participants were male, depending on wave and analytic sample (Table 1). Among smokers from the previous wave, 7 to 9% of respondents had quit for at least a month at follow-up (cessation sample). Between 17% and 21% of participants had relapsed at follow-up among those who had quit at the previous wave in the relapse sample. Large increases in provincial POS display bans were seen between waves 6 and 7, from 7 to 11% of people in the sample to approximately 96% experiencing the bans, with variation by analytic sample. On average, there were 7 to 9 tobacco retailers within a 1 km radius of participants’ homes, and the distance to the nearest tobacco retailer ranged between 1.04 and 2.17 km.
Table 1.
Selected sample characteristics, International Tobacco Control Policy (ITC) Canada Survey, 2006-2011
| Cessation* | Relapse† | |||||||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| Variables | Wave 5 n=1129 |
Wave 6 n=1119 |
Wave 7 n=1165 |
Wave 8 n=975 |
Wave 5 n=185 |
Wave 6 n=209 |
Wave 7 n=214 |
Wave 8 n=258 |
| Age, mean (SD) | 47.52 (12.89) | 48.79 (12.96) | 49.93 (12.30) | 52.56 (11.72) | 47.08 (13.52) | 48.37 (13.30) | 50.50 (13.76) | 51.43 (13.35) |
| Sex, % | ||||||||
| Male | 58.02 | 57.91 | 56.14 | 55.69 | 63.24 | 59.33 | 61.21 | 60.08 |
| Female | 41.98 | 42.09 | 43.86 | 44.31 | 36.76 | 40.67 | 38.79 | 39.92 |
| Income, % | ||||||||
| under $29,999 | 25.24 | 24.93 | 23.69 | 23.90 | 18.92 | 20.1 | 17.29 | 18.6 |
| $30,000-$59,999 | 35.08 | 35.84 | 35.79 | 34.36 | 34.05 | 32.54 | 34.58 | 33.33 |
| $60,000-74,999 | 11.78 | 11.35 | 10.73 | 10.77 | 14.59 | 15.79 | 13.08 | 13.18 |
| $75,000-99,999 | 9.39 | 10.55 | 10.99 | 11.08 | 14.05 | 10.53 | 13.55 | 13.57 |
| $100,000 and over | 11.6 | 10.81 | 12.02 | 11.18 | 11.89 | 14.83 | 12.15 | 13.57 |
| Don’t know/missing | 6.91 | 6.52 | 6.78 | 8.72 | 6.49 | 6.22 | 9.35 | 7.75 |
| Education, % | ||||||||
| Grade school, some HS, HS completed | 43.31 | 44.33 | 41.37 | 42.56 | 36.22 | 34.45 | 37.85 | 34.5 |
| Tech/trade school/community college, some university | 39.24 | 37.27 | 39.31 | 38.05 | 43.24 | 46.89 | 41.12 | 43.41 |
| Completed university, post-graduate | 17.45 | 18.41 | 19.31 | 19.38 | 20.54 | 18.66 | 21.03 | 22.09 |
| Province, % | ||||||||
| Newfoundland and Labrador (NL) | 2.13 | 1.97 | 1.8 | 2.05 | 2.16 | 0.96 | 2.8 | 1.55 |
| Nova Scotia (NS) | 3.63 | 3.75 | 5.06 | 4.41 | 3.78 | 3.83 | 2.8 | 3.1 |
| New Brunswick (NB) | 1.59 | 2.32 | 2.23 | 2.77 | 1.62 | 2.39 | 3.27 | 3.88 |
| Quebec (QC) | 23.56 | 24.58 | 24.46 | 23.18 | 26.49 | 26.32 | 22.9 | 27.91 |
| Ontario (ON) | 38.62 | 39.05 | 39.48 | 39.79 | 44.32 | 44.02 | 42.06 | 39.53 |
| Manitoba (MB) | 3.72 | 3.75 | 4.21 | 4.00 | 0.54 | 0.96 | 1.40 | 3.88 |
| Saskatchewan (SK) | 4.07 | 3.49 | 3.86 | 3.49 | 2.16 | 1.91 | 2.34 | 2.33 |
| Alberta (AB) | 9.12 | 9.03 | 8.58 | 8.21 | 7.03 | 7.18 | 9.35 | 7.75 |
| British Columbia (BC) | 13.55 | 12.06 | 10.3 | 12.10 | 11.89 | 12.44 | 13.08 | 10.08 |
| Quit attempts, % | ||||||||
| Yes | ||||||||
| No | ||||||||
| Cessation, % | ||||||||
| quit | 7.79 | 8.22 | 8.93 | 7.18 | ||||
| back to smoking | 92.21 | 91.78 | 91.07 | 92.82 | ||||
| Relapse, % | ||||||||
| back to smoking | 21.08 | 19.62 | 16.82 | 20.93 | ||||
| still quit | 78.92 | 80.38 | 83.18 | 79.07 | ||||
| Provincial POS bans, % | ||||||||
| Yes | 7.79 | 10.99 | 96.57 | 100.0 | 2.70 | 6.70 | 95.79 | 100.0 |
| No | 92.21 | 89.01 | 3.43 | 0.0 | 97.30 | 93.30 | 4.21 | 0.0 |
| Number of retailers /1 km | 8.23 (0.4) | 8.82 (0.4) | 7.5 (0.3) | 8.06 (0.4) | 8.57 (0.9) | 8.19 (0.8) | 6.58 (0.7) | 7.17 (0.6) |
| Distance to retailer (km), mean (SD) | 1.80 (0.2) | 1.04 (0.1) | 1.43 (0.2) | 1.04 (0.1) | 1.61 (0.4) | 1.31 (0.3) | 2.17 (0.8) | 1.44 (0.3) |
The cessation sample consisted of respondents who were smokers at time t (n=4388 observations).
The relapse sample included respondents who had quit smoking for at least 30 days at time t (n=866 observations).
In the cessation sample, there was no significant difference in the weighted percentage of people who quit when comparing those exposed to POS display bans or not (7.7% versus 8.5%, respectively, chi-square P-value 0.343). In adjusted GEE models, none of the exposure variables (POS display bans, retail density, proximity) was associated with cessation (Table 2).
Table 2.
Odds ratios for cessation associated with POS display ban, tobacco retail density, and tobacco retail distance, International Tobacco Control Policy (ITC) Canada Survey, 2006–2011
| Model 1* | Model 2† | Model 3* | Model 4† | Model 5* | Model 6† | Model 7† | |
|---|---|---|---|---|---|---|---|
|
| |||||||
| Cessation‡ n=4388 OR (95% CI) | |||||||
| POS ban | 0.90 (0.69, 1.18) |
0.92 (0.66, 1.29) |
0.92 (0.66, 1.30) |
||||
| Tobacco retailer density/1km | 1.00 (0.99, 1.01) |
1.00 (0.99, 1.01) |
1.00 (0.99, 1.01) |
||||
| Distance to nearest retailer (km) | 1.00 (0.97, 1.02) |
1.01 (0.97, 1.06) |
1.01 (0.97, 1.06) |
||||
Bivariate models.
Models adjusted for age, sex, income, education, province, provincial cigarette price, quit attempts.
The cessation sample consisted of respondents who were smokers at time t.
There was no significant difference in the weighted percentage of quitters who relapsed based on whether they lived in a province with a POS display ban (17.2% exposed versus 18.9% unexposed, chi-square P-value 0.506). Nevertheless, after adjustment for covariates (Table 3, Model 2) and further adjustment for retail density and proximity (Model 7), living in a province with a POS ban was associated with lower odds of relapse, although the results were not statistically significant (Model 2: OR 0.68, 95% CI 0.42, 1.09; P-value 0.1114; Model 7: OR 0.66, 95% CI 0.41, 1.07; P-value 0.0894). Neither tobacco retail density nor tobacco retail proximity was associated with relapse in adjusted models (Model 4 for density, Model 6 for proximity).
Table 3.
Odds ratios for relapsing associated with POS display ban, tobacco retail density, and tobacco retail distance, International Tobacco Control Policy and Evaluation Project, Canada 2006–2011
| Relapse‡ n=866 OR (95% CI) | |||||||
|---|---|---|---|---|---|---|---|
|
| |||||||
| Model 1* | Model 2† | Model 3* | Model 4† | Model 5* | Model 6† | Model 7† | |
| POS ban | 0.89 (0.58, 1.36) |
0.68 (0.42, 1.09) |
0.66 (0.41, 1.07) |
||||
| Tobacco retailer density /1km | 0.99 (0.97, 1.01) |
0.99 (0.97, 1.01) |
0.99 (0.97, 1.01) |
||||
| Distance to nearest retailer (km) | 0.96 (0.90, 1.03) |
0.95 (0.88, 1.03) |
0.94 (0.85, 1.04) |
||||
Bivariate models.
Models adjusted for age, sex, income, education, province, provincial cigarette price.
The relapse sample included respondents who had quit smoking for at least 30 days at time t.
Regarding the sensitivity analyses, results showed similar point estimates and statistical significance for results from models that assessed (1) including drug stores and liquor stores and (2) after adjusting for HSI from the previous wave for cessation. In the sensitivity analyses excluding rural participants, point estimates were similar for cessation and relapse, but the confidence interval was slightly wider for the POS ban estimate in the relapse sample (Model 7: OR 0.66, 95% CI 0.39, 1.11), likely due to the change in sample size (n=735 in sensitivity analysis versus n=866 in original). Time-in-sample was collinear with the POS exposure variable for the cessation and relapse models (Spearman’s correlation: ρ=0.72 and ρ=0.78, respectively), so models were not re-estimated. Finally, when adjusting for self-reported work, restaurant, and bar smoke-free policies, point estimates were similar, and none of the coefficients for the smoke-free variables were statistically significant correlates of cessation or relapse. The sample size was reduced when including these additional variables (i.e., from n=866 to n=744 for the relapse sample). As a consequence, the confidence interval widened for the POS ban variable (Model 7: OR 0.65, 95% CI 0.37, 1.15).
DISCUSSION
We used data from a population-based, longitudinal survey of adult smokers in Canada to evaluate how living in a province with a POS display ban, tobacco retailer density, and tobacco retailer proximity are associated with smoking cessation and relapse. Living in a province with a POS display ban was associated with lower odds of relapse, although the results were not statistically significant (p=0.089). This finding was consistent with the idea that eliminating exposure to smoking cues such as tobacco POS displays may be particularly salient for the Relapse stage. We observed no associations between the POS bans and cessation, despite our hypothesis that the absence of POS retail displays is important at the Maintenance stage. Neither tobacco retailer density nor proximity was associated with cessation or relapse.
There are many potential reasons why we did not see stronger associations between POS bans and cessation or relapse. It is possible that POS bans have a small impact on cessation and relapse due to the study context. At the time of this study, Canada already had a strong tobacco control regulatory environment, including bans on tobacco advertising (i.e., tv/radio, billboards, newspaper/magazines), price promotions, and other promotions (i.e., online, direct mail).[24] The absence of synergy between POS displays and other marketing at POS (e.g., advertising, promotional strategies) may mean that POS bans in a study context like Canada could limit the impact of a display ban. Another possibility is that during the study period, implementation of other local polices may have had a greater influence on cessation and relapse, although we adjusted for cigarette price by province for each wave, and also for province to account for differences in the overall policy environments. In addition, there was little investment in anti-smoking media campaigns during the study period, and all provinces had implemented quitlines prior to 2006,[33] indicating that these factors are unlikely to account for our results. Moreover, the additional sensitivity analysis adjusting for self-reported smoke-free policies yielded substantially similar results. Finally, coefficients for POS bans were in the anticipated direction for relapse (exposure to bans associated with lower odds of relapse), although we may have been underpowered to detect statistically significant associations for what we expected to be relatively small effects.
To the best of our knowledge, no previous work has investigated the impact of POS display bans on smoking cessation behaviors. However, several studies that looked at the association between POS marketing and smoking cessation generally found that greater exposure to POS marketing made smokers less likely to quit.[5, 6, 8] Our trend results for POS bans associated with lower odds of relapse (P-value=0.0894, Model 7) are consistent with these prior studies, as former smokers would have been exposed to less marketing in the form of product displays.
In the current study, higher tobacco retailer density was not associated with cessation or relapse. Only five previous longitudinal studies have investigated density and cessation behaviors, with mixed results. In Finland, greater density was associated with less quitting among moderate/heavy smoking men,[9] although the same study found no relationship between density and quitting for men who were light smokers nor for female smokers,[9] and studies in the US and England likewise found no relationship.[7, 15] Another US study, though, found that greater density was associated with lower 30-day abstinence in high poverty, but not low poverty, areas.[16] A Canadian study found that higher density was not associated with relapse.[18] Our results are consistent with the some findings from previous studies since we found no association between density and cessation, and also observed no association between density and relapse, as in the Canadian study.
The current study also found no relationship between distance from the nearest tobacco retailer and cessation or relapse. Of the previous longitudinal studies examining distance and cessation, US and Finnish studies found that greater distance was associated with an increase in cessation,[7, 9, 16, 17] although one US study only found this relationship in high poverty, and not in low poverty, areas,[16] and one Finnish study only found this among moderate/heavy male smokers, and not among men who were light smokers or female smokers (where the opposite relationship was found for light smokers).[9] However, English and Canadian studies found no relationship between distance and cessation.[15, 18] Regarding relapse, two longitudinal studies had previously examined the relationship between distance and relapse, and found no relationship.[17, 18] Our results are consistent with null findings for quitting from England and Canada and among specific groups in Finland and the US, and null findings for relapse from Finland and Canada. Future research should consider examining other measures of distance, such as having at least one retailer within a given radius,[18] roadway distance, travel time, or living at extreme distances from the nearest retailer, and relation of these measures to workplace or activity space.
Strengths and limitations
To the best of our knowledge, this is the first study to evaluate the potential effects of POS display bans on cessation and relapse, and also the first to tease apart how POS display bans and tobacco retailer availability (i.e., density and proximity) may independently influence smoking cessation outcomes. Nevertheless, our study has several important limitations. Other aspects of the tobacco control environment may have confounded our results. To address this, we adjusted for cigarette price at the provincial level and included an indicator for province to account for potential differences across the policy environment. Although we did not examine differences in anti-smoking ads or quit support across provinces, there was little investment in media campaigns during the study period and all provinces had quitlines prior to 2006.[33] Moreover, our sensitivity analysis including self-reported indicators of smoke-free policies showed substantially similar results, and none of the coefficients on the smoke-free variables was associated with cessation or relapse, which is consistent with prior work showing that the relationship between smoke-free policies and cessation behaviors is not strong.[34–37] We measured policy implementation, not compliance. However, previous studies in Canada suggest excellent compliance with policy implementation.[38] It is possible that tobacco retailer density and proximity were measured with error due to the use of DMTI-EPOI data rather than direct observations of the retailer environment, although we specifically chose retailers based on their likelihood of selling tobacco, and sensitivity analyses with additional types of retailers that may sell tobacco yielded similar results. In addition, our measurement focused on availability around the home, which does not account for the places people work, or travel to, frequently. Hence, other methods that capture exposure data in real time, such as ecological momentary assessments, [39, 40] may be necessary to study density and proximity. We measured distance using Euclidean distance rather than roadway network, and so do not have actual travel distance or travel times. In practice, Euclidean distance and roadway networks have been shown to be highly correlated,[41] reducing the likelihood of measurement error. We also do not account for availability of contraband tobacco or access to a vehicle, which may alter the effect of the distance measures. Furthermore, tobacco availability and POS policy implementation may vary by geographical location (i.e., rural vs. urban areas). However, the sensitivity analysis that excluded all participants that resided in rural areas found similar results for all models. Attrition may be another potential source of bias since 27.8%, 24.3%, and 25.6% of participants were lost to follow-up from waves 5 to 6, waves 6 to 7, and waves 7 and 8, respectively. Nevertheless, there were no significant differences between the socio-demographic covariates (i.e., age, sex, education, income), exposure variables (POS bans, tobacco retailer density and proximity), or the outcome variables (cessation, relapse) in the study sample and among participants who were lost to follow-up, with a few exceptions: tobacco retailer density (among participants lost to follow up from waves 6 to 7 and waves 7 to 8) and sex (among participants lost to follow up from waves 7 to 8).
Conclusions
We found that exposure to provincial POS display bans was associated with lower odds of relapse (albeit not statistically significant), but was not associated with cessation. Tobacco retailer density and proximity did not influence cessation or relapse. Even in a context where POS advertising is banned, a POS display ban shows promise as an additional tool to prevent relapse, although results need to be confirmed in larger longitudinal studies. POS display bans may contribute to the ongoing denormalization of smoking, reducing the prompt to smoke that POS displays cause when viewed by those who are attempting to quit or have already quit.
What is already known on this subject
No previous study has examined the effect of point-of-sale (POS) display bans on smoking cessation or relapse, nor tried to disentangle the effects of POS display from POS retail availability.
The few studies examining POS marketing indicate that it impedes cessation.
Results are mixed and limited for understanding how tobacco retailer density and proximity affect smoking cessation.
What this paper adds
This paper examined the relationship between POS display bans and smoking cessation and relapse in Canada, where bans were implemented differentially across provinces over time.
Our results suggest that POS display bans may help prevent relapse. Neither tobacco retailer density nor proximity were associated with cessation or relapse.
Acknowledgments
Funding
This work was supported by a pilot project to NLF from the American Cancer Society Institutional Research Grant to the University of South Carolina College of Pharmacy. Major funders of the ITC Canada Survey Waves 5-8: US National Cancer Institute (P50 CA111236, R01 CA100362), Canadian Institutes of Health Research (MOP-79551, MOP-115016, FDN-148477). Additional support was provided to Geoffrey T. Fong from a Senior Investigator Award from the Ontario Institute for Cancer Research and a Prevention Scientist Award from the Canadian Cancer Society Research Institute. None of the sponsors played any direct role in the design or conduct of the study; the collection, management, analysis or interpretation of the data; in the preparation of the manuscript, or in the decision to submit the manuscript for publication.
Footnotes
Competing Interests
The authors declare they have no competing interests.
Contributorship statement
NLF and JFT conceptualized the study. GM conducted the geographic analyses. PL, NLF, and Y-HW conducted the statistical analyses. NLF and JWH supervised the statistical analyses. PL and NLF drafted the manuscript. All authors contributed to the study design, interpretation of results, and final revision of the manuscript.
References
- 1.Henriksen L. Comprehensive tobacco marketing restrictions: promotion, packaging, price and place. Tob Control. 2012;21(2):147–153. doi: 10.1136/tobaccocontrol-2011-050416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Harper T. Why the tobacco industry fears point of sale display bans. Tob Control. 2006;15(3):270–271. doi: 10.1136/tc.2006.015875. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wakefield MA, Terry-McElrath YM, Chaloupka FJ, et al. Tobacco industry marketing at point of purchase after the 1998 MSA billboard advertising ban. Am J Public Health. 2002;92(6):937–940. doi: 10.2105/ajph.92.6.937. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Pearce J, Barnett R, Moon G. Sociospatial inequalities in health-related behaviours: Pathways linking place and smoking. Prog Hum Geog. 2012;36(1):3–24. [Google Scholar]
- 5.Germain D, McCarthy M, Wakefield M. Smoker sensitivity to retail tobacco displays and quitting: a cohort study. Addiction. 2010;105(1):159–163. doi: 10.1111/j.1360-0443.2009.02714.x. [DOI] [PubMed] [Google Scholar]
- 6.Hoek J, Gifford H, Pirikahu G, et al. How do tobacco retail displays affect cessation attempts? Findings from a qualitative study. Tob Control. 2010;19(4):334–337. doi: 10.1136/tc.2009.031203. [DOI] [PubMed] [Google Scholar]
- 7.Reitzel LR, Cromley EK, Li YS, et al. The Effect of Tobacco Outlet Density and Proximity on Smoking Cessation. Am J Public Health. 2011;101(2):315–320. doi: 10.2105/AJPH.2010.191676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Siahpush M, Shaikh RA, Smith D, et al. The Association of Exposure to Point-of-Sale Tobacco Marketing with Quit Attempt and Quit Success: Results from a Prospective Study of Smokers in the United States. Int J Env Res Pub He. 2016;13(2) doi: 10.3390/ijerph13020203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Halonen JI, Kivimaki M, Kouvonen A, et al. Proximity to a tobacco store and smoking cessation: a cohort study. Tob Control. 2014;23(2):146–151. doi: 10.1136/tobaccocontrol-2012-050726. [DOI] [PubMed] [Google Scholar]
- 10.Prochaska JO, Velicer WF. The transtheoretical model of health behavior change. Am J Health Promot. 1997;12(1):38–48. doi: 10.4278/0890-1171-12.1.38. [DOI] [PubMed] [Google Scholar]
- 11.Carpenter MJ, Saladin ME, LaRowe SD, et al. Craving, Cue Reactivity, and Stimulus Control Among Early-Stage Young Smokers: Effects of Smoking Intensity and Gender. Nicotine & Tobacco Research. 2014;16(2):208–215. doi: 10.1093/ntr/ntt147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Shiffman S, Dunbar M, Kirchner T, et al. Smoker Reactivity to Cues: Effects on Craving and on Smoking Behavior. J Abnorm Psychol. 2013;122(1):264–280. doi: 10.1037/a0028339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Conklin CA, Vella EJ, Joyce CJ, et al. Examining the Relationship Between Cue-Induced Craving and Actual Smoking. Exp Clin Psychopharm. 2015;23(2):90–96. doi: 10.1037/a0038826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Shiffman S, Dunbar MS, Li XX, et al. Smoking Patterns and Stimulus Control in Intermittent and Daily Smokers. Plos One. 2014;9(3) doi: 10.1371/journal.pone.0089911. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Han T, Alexander M, Niggebrugge A, et al. Impact of tobacco outlet density and proximity on smoking cessation: A longitudinal observational study in two English cities. Health & place. 2014;27:45–50. doi: 10.1016/j.healthplace.2014.01.008. [DOI] [PubMed] [Google Scholar]
- 16.Cantrell J, Anesetti-Rothermel A, Pearson JL, et al. The impact of the tobacco retail outlet environment on adult cessation and differences by neighborhood poverty. Addiction. 2015;110(1):152–161. doi: 10.1111/add.12718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Pulakka A, Halonen JI, Kawachi I, et al. Association Between Distance From Home to Tobacco Outlet and Smoking Cessation and Relapse. Jama Intern Med. 2016;176(10):1512–1519. doi: 10.1001/jamainternmed.2016.4535. [DOI] [PubMed] [Google Scholar]
- 18.Chaiton MO, Mecredy G, Cohen J. Tobacco retail availability and risk of relapse among smokers who make a quit attempt: a population-based cohort study. Tob Control. doi: 10.1136/tobaccocontrol-2016-053490. Published Online First 21 April 2017. [DOI] [PubMed] [Google Scholar]
- 19.Burton S, Clark L, Jackson K. The association between seeing retail displays of tobacco and tobacco smoking and purchase: findings from a diary-style survey. Addiction. 2012;107(1):169–175. doi: 10.1111/j.1360-0443.2011.03584.x. [DOI] [PubMed] [Google Scholar]
- 20.Carter OB, Mills BW, Donovan RJ. The effect of retail cigarette pack displays on unplanned purchases: results from immediate postpurchase interviews. Tob Control. 2009;18(3):218–221. doi: 10.1136/tc.2008.027870. [DOI] [PubMed] [Google Scholar]
- 21.Wakefield M, Germain D, Henriksen L. The effect of retail cigarette pack displays on impulse purchase. Addiction. 2008;103(2):322–328. doi: 10.1111/j.1360-0443.2007.02062.x. [DOI] [PubMed] [Google Scholar]
- 22.Clattenburg EJ, Elf JL, Apelberg BJ. Unplanned cigarette purchases and tobacco point of sale advertising: a potential barrier to smoking cessation. Tob Control. 2013;22(6):376–381. doi: 10.1136/tobaccocontrol-2012-050427. [DOI] [PubMed] [Google Scholar]
- 23.Li L, Borland R, Fong GT, et al. Impact of point-of-sale tobacco display bans: findings from the International Tobacco Control Four Country Survey. Health Educ Res. 2013;28(5):898–910. doi: 10.1093/her/cyt058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Kasza KA, Hyland AJ, Brown A, et al. The Effectiveness of Tobacco Marketing Regulations on Reducing Smokers’ Exposure to Advertising and Promotion: Findings from the International Tobacco Control (ITC) Four Country Survey. Int J Env Res Pub He. 2011;8(2):321–340. doi: 10.3390/ijerph8020321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Thompson ME, Fong GT, Hammond D, et al. Methods of the International Tobacco Control (ITC) four country survey. Tobacco Control. 2006;15(suppl 3):iii12–iii18. doi: 10.1136/tc.2005.013870. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Waterloo Uo. DMTI CanMap enhanced points of interest (EPOI) Canada: University of Waterloo; 2015. [Google Scholar]
- 27.Chan WC, Leatherdale ST. Tobacco retailer density surrounding schools and youth smoking behaviour: a multi-level analysis. Tobacco induced diseases. 2011;9(1):9. doi: 10.1186/1617-9625-9-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Ontario Tobacco Research Unit. The Tobacco Control Environment: Ontario and Beyond. 1. Vol. 14. Toronto, ON: Ontario Tobacco Research Unit; 2008. Prohibition of Tobacco Sales in Specific Places: Monitoring Update. (Special Reports: Monitoring and Evaluation Series, 2007–2008). [Google Scholar]
- 29.Ontario Tobacco Research Unit. The Tobacco Control Environment: Ontario and Beyond. 1. Vol. 13. Toronto, ON: Ontario Tobacco Research Unit; 2007. Fact Sheet 1.2: Prohibition of Tobacco Sales in Specific Places. (Special Reports: Monitoring and Evaluation Series, 2006–2007). [Google Scholar]
- 30.Ontario Tobacco Research Unit. The Tobacco Control Environment: Ontario and Beyond Monitoring and Evaluation Series. 1. Vol. 15. Toronto, ON: Ontario Tobacco Research Unit; 2009. Prohibition of Tobacco Sales in Specific Places: Monitoring Update. [Google Scholar]
- 31.Ontario Tobacco Research Unit. The Tobacco Control Environment: Ontario and Beyond Monitoring and Evaluation Series. 1. Vol. 16. Toronto, ON: Ontario Tobacco Research Unit; 2010. Prohibition of Tobacco Sales in Specific Places: Monitoring Update. [Google Scholar]
- 32.Reid JL, Hammond D. Tobacco use in Canada: patterns and trends Supplement: Tobacco Control Policies in Canada ed. Waterloo, ON: Propel Centre for Population Health Impact, University of Waterloo; 2015. [Google Scholar]
- 33.Project ITC. ITC Canada National Report: Findings from the Wave 1 to 8 Surveys (2002–2011) Waterloo, Ontario Canada: University of Waterloo; 2013. [Google Scholar]
- 34.Albers AB, Siegel M, Cheng DM, et al. Effect of smoking regulations in local restaurants on smokers’ anti-smoking attitudes and quitting behaviours. Tob Control. 2007;16(2):101–106. doi: 10.1136/tc.2006.017426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Federico B, Mackenbach JP, Eikemo TA, et al. Impact of the 2005 smoke-free policy in Italy on prevalence, cessation and intensity of smoking in the overall population and by educational group. Addiction. 2012;107(9):1677–1686. doi: 10.1111/j.1360-0443.2012.03853.x. [DOI] [PubMed] [Google Scholar]
- 36.Hyland A, Hassan LM, Higbee C, et al. The impact of smokefree legislation in Scotland: results from the Scottish ITC: Scotland/UK longitudinal surveys. European journal of public health. 2009;19(2):198–205. doi: 10.1093/eurpub/ckn141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Nagelhout GE, Willemsen MC, de Vries H. The population impact of smoke-free workplace and hospitality industry legislation on smoking behaviour. Findings from a national population survey. Addiction. 2011;106(4):816–823. doi: 10.1111/j.1360-0443.2010.03247.x. [DOI] [PubMed] [Google Scholar]
- 38.Cohen JE, Planinac L, Lavack A, et al. Changes in Retail Tobacco Promotions in a Cohort of Stores Before, During, and After a Tobacco Product Display Ban. Am J Public Health. 2011;101(10):1879–1881. doi: 10.2105/AJPH.2011.300172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Ferguson SG, Shiffman S. Using the Methods of Ecological Momentary Assessment in Substance Dependence Research-Smoking Cessation as a Case Study. Subst Use Misuse. 2011;46(1):87–95. doi: 10.3109/10826084.2011.521399. [DOI] [PubMed] [Google Scholar]
- 40.Kirchner TR, Cantrell J, Anesetti-Rothermel A, et al. Geospatial Exposure to Point-of-Sale Tobacco Real-Time Craving and Smoking-Cessation Outcomes. Am J Prev Med. 2013;45(4):379–385. doi: 10.1016/j.amepre.2013.05.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Boscoe FP, Henry KA, Zdeb MS. A Nationwide Comparison of Driving Distance Versus Straight-Line Distance to Hospitals. Prof Geogr. 2012;64(2):188–196. doi: 10.1080/00330124.2011.583586. [DOI] [PMC free article] [PubMed] [Google Scholar]