

Abstract
Study Design:
Narrative review and expert recommendation.
Objectives:
To establish treatment recommendations for atlas fractures based on the knowledge of the experts of the Spine Section of the German Society for Orthopaedics and Trauma.
Methods:
Neither high-level evidence studies comparing conservative and operative management nor studies matching different operative treatment strategies exist. This recommendation summarizes the knowledge of the experts of the Spine Section of the German Society for Orthopaedics and Trauma with regard to the treatment of atlas fractures.
Results:
Most atlas fractures are the result of compression forces. A valuable morphological classification system has been described by Gehweiler. For an adequate diagnosis, a computed tomography is mandatory. To distinguish between stable and unstable type 3 injuries, it is necessary to evaluate the integrity of the transverse atlantal ligament (TAL) with magnetic resonance imaging and to classify the TAL lesions. The majority of atlas fractures are stable and will be successfully managed conservatively. Unstable atlas fractures (type 3b and sagittal split type 4 fractures) should be treated by surgical stabilization. Unstable atlas fractures (type 3b) with a midsubstance ligamentous disruption or severely dislocated ligamentous bony avulsions of the TAL can successfully be treated by a C1/2 fusion. Unstable atlas fractures (type 3b) with a moderately dislocated ligamentous bony avulsion of the TAL and sagittal split type 4 fractures may be treated by atlas osteosynthesis only.
Conclusions:
Whereas the majority of atlas fractures can be managed conservatively, in specific fracture patterns surgical treatment strategies have become the standard of care.
Keywords: atlas, C1, instability, fracture, transverse atlantal ligament (TAL), surgery, atlas osteosynthesis, C1/2 fusion, cervical spine, injury, axial compression
Introduction
Atlas (C1) fractures represent about 25% of all craniocervical injuries and 2% to 13% of all cervical spine injuries.1 Concomitant fractures of the cervical spine are common, for example, odontoid fractures occur in approximately 40% to 44% of all cases combined with atlas fractures.
Neither high-level evidence studies comparing conservative and operative management nor studies matching different operative treatment strategies exist. Hence, the following recommendations for the treatment of atlas fractures primarily rely on the experiences of the participating spinal surgeons2,3 of the Spine Section of the German Society for Orthopaedics and Trauma (DGOU). The DGOU was founded in 2008. Its inauguration resulted from a merger of the German Society for Orthopedics and Orthopedic Surgery founded in 1901 and the German Society for Trauma Surgery founded in 1922. The DGOU is the largest surgical society in Germany with more than 10 000 members including more than 50 scientific subgroups representing all subspecialties of orthopedic and trauma surgery like the spine section. The German Society for Orthopaedics and Trauma has a specific expertise and is the organization defining treatment standards and guidelines in orthopedic and trauma surgery in Germany. Typically these recommendations are developed by applying the AWMF (the Working Group of the Scientific Medical Organizations in Germany) rules. Currently, more than 200 orthopedic and trauma guidelines according to AWMF standards are published and actively applied in Germany.
The recommendation presented here are considering the current literature and refer to the diagnostics and treatment of acute traumatic atlas injuries of otherwise healthy skeletally mature patients with normal bone quality.
Clinical Presentation
Patients suffering from a traumatic fracture of the atlas typically complain of pain in the upper cervical spine.4 Muscle tenderness, muscle spasms, and pain-related decreased motion of the upper cervical spine, especially with rotation, are common. Rarely, the patient may present with torticollis or a “cock-robin” deformity from a C1 fracture. A neurological deficit due to a spinal cord injury linked to an atlas fracture is very rare,5 but has been described (eg, “Collet-Sicard syndrome”6). Additionally, symptoms associated with a hypoperfusion of the basilar supply territory like nausea, vomiting, tinnitus, impaired vision, and drop attacks are possible due to a potential vertebral artery lesion or posttraumatic thrombosis.
The differential diagnosis includes predominantly congenital anomalies like hypoplasia of the anterior and posterior atlas arch, bipartite atlas, or posttraumatic nonunion.
Biomechanical Considerations
The anatomy of the atlas with the superior articular facet inclined in a mediocaudal direction while the inferior articular facet is orientated in a mediocranial direction translates axial loads to the occiput into a distraction of the lateral masses of the atlas. If tension forces exceed the stability of the bony or ligamentous atlas structures, the atlas ring fractures and/or the transverse atlantal ligament (TAL) ruptures. The predominant locations of these fractures are the weakest points of the atlas that corresponds to the attachment points of the anterior/posterior arch or the TAL with the lateral mass.
Sköld7 identified in an autopsy study that forehead injuries associated with extension typically resulted in posterior arch fractures, while anterior and posterior ring injuries were associated with axial compression due to an impact on the vertex. Lateral impacts often resulted in lateral mass and anterior arch fractures. Additionally, Panjabi et al8 demonstrated that isolated TAL lesions, bony avulsions as well as midsubstance ruptures, are possible even without bony disruption of the atlas ring. Oda et al9 showed that a low-velocity trauma often is associated with lateral mass fractures, while a high-velocity trauma typically resulted in burst fractures of the atlas ring.
Diagnostic Imaging Algorithm
Although cervical spine X-rays remain the first-line diagnostic tool, nondisplaced atlas fractures might often be overlooked. In dislocated atlas burst fractures, the open mouth anterior-posterior X-ray (odontoid view) might show a uni- or bilateral “overhang” of the C1 lateral mass over the C2 superior articular process. According to the “rule of Spence,” this overhang might indicate instability.10 To measure instability, the distance between the overhanging lateral border of C1 and the lateral border of C2 should be evaluated. If the dislocation is bilateral, both values should be summarized. If the overhang of C1 exceeds 6.9 mm, instability is present. However, it was proposed by Heller et al11 that this value should be adjusted to 8.1 mm due to radiographic magnification factors.
To evaluate the integrity of the atlas ring in detail and to classify a potential atlas fracture, computed tomography (CT) is always necessary. Especially the axial CT slices should carefully be reviewed to detect a bony avulsion of the TAL as a criterion for a potential instability. If a dislocation of the C1 lateral mass is obvious and the CT was unable to detect a bony avulsion of the transverse ligament, magnetic resonance imaging (MRI) is recommended to evaluate TAL integrity.12 This is important to distinguish between stable atlas burst fractures with an intact TAL and unstable burst fractures with a ruptured TAL.
Today, the “rule of Spence” has been shown to be inaccurate for assessing the integrity of the TAL. Studies have reported only little correlation between bony displacement of atlas fractures on CT scans and TAL stability. Instead, MRI should be applied for evaluating the TAL. Dickman et al12 also demonstrated that 60% of patients with a TAL rupture would not have meet the “rule of Spence” criteria for a TAL injury. An additional criteria for instability is the widening of the anterior atlanto-dental interval to more than 3 mm in functional lateral X-rays,13 because it indicates translational atlantoaxial instability.
Trauma to the upper cervical spine might also compromise many vascular structures. However, the vertebral artery is most at risk, especially in lesions of the transverse process and in lateral mass fractures involving the foramen of the vertebral artery. Especially in these cases an angio-CT or an angio-MRI has to be performed to exclude lesions of the vertebral artery.14
Classification
There are several classification systems for atlas fractures available. In clinical studies, the 3 most commonly used are the Jefferson classification4 followed by the Landells classification15 and the Gehweiler classification.16 While the Jefferson classification is commonly used in America and Asia, the Gehweiler classification is widely applied in Europe. Hence, it is the preferred classification system of the Spine Section of the DGOU.
Gehweiler16 divided atlas fractures in 5 subgroups (Figure 1). A type 1 atlas fracture is an isolated fracture of the anterior arch (corresponding to Jefferson 1), while a type 2 atlas fracture is an isolated, predominately bilateral, fracture of the posterior atlas ring (corresponding to Jefferson 2). The combined injury of the anterior and posterior arch of the atlas, the “classic Jefferson-fracture,” corresponds to a Gehweiler 3 fracture (corresponding to Jefferson 3). Important is the distinction between stable and unstable injuries. In stable injuries the TAL is intact (type 3a). If these fractures are associated with a lesion of the TAL, they are classified as unstable (type 3b).3 The type 4 fractures are fractures of the lateral mass (corresponding to Jefferson 4). Type 5 fractures are isolated fractures of the C1 transverse process (not corresponding to a Jefferson type).
Figure 1.
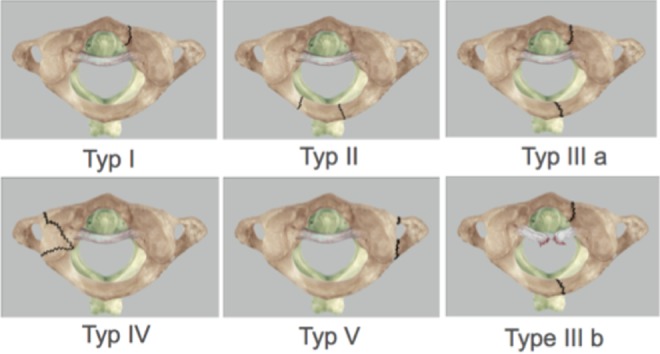
Classification of atlas fractures according to Gehweiler et al.16
The integrity of the TAL is important for atlas stability. Dickman et al17 presented a classification that distinguishes between an intraligamentous rupture and a bony avulsion of the ligament. The intraligamentous rupture (type 1) involves a central lesion (type 1a), while a lesion close to the lateral mass is referred to as a type 1b injury. The bony avulsion of the TAL from the lateral mass (type 2) can be differentiated into an isolated bony avulsion (type 2a) and a bony avulsion associated with a fracture of the lateral mass (type 2b). Another important factor is the degree of separation or dislocation of the bony avulsion fragment from the lateral mass, because it defines the surgical treatment options.
Therapeutic Algorithm (Figure 3)
Figure 3.

Treatment algorithm for management of atlas fractures of the Spine Section of the German Society for Orthopaedics and Trauma.
Figure 2.
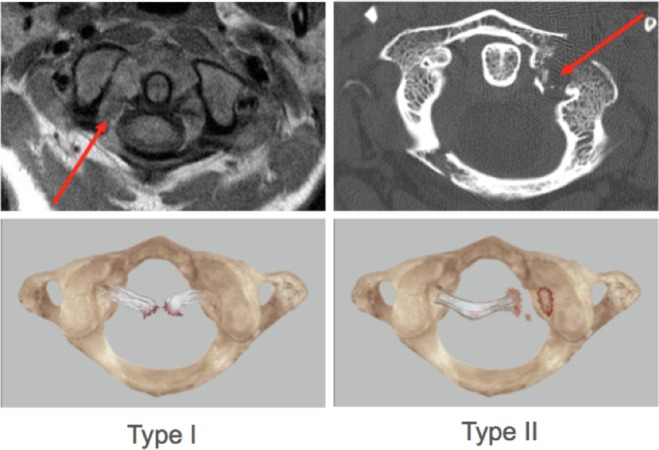
Classification of the TAL injuries according to Dickman et al.17 For a detailed description of the fracture patterns see the main text.
The treatment of C1 fractures remains controversial and is influenced by the presence of concomitant cervical spine injuries. To date, no internationally accepted treatment standards are available. The therapeutic algorithm presented in this review is focused on isolated atlas fractures in adults and is based on the Gehweiler classification. It summarizes the recommendations of the experts of the Spine Section of the DGOU.
While conservative treatment is the method of choice in most cases, widely accepted surgical indications are atlas factures associated with atlanto-occipital instability, an intraligamentous rupture of the TAL, and any “unstable” atlas fracture. Instability was defined by Hein et al18 as a fracture of the anterior and posterior arches of the atlas associated with a rupture of the TAL and an incongruence of the atlanto-occipital and the atlanto-axial joints.
Gehweiler Types 1, 2, and 5 Fractures
Atlas fracture types 1, 2, and 5 according to Gehweiler are stable lesions. These fractures can be treated with cervical spine immobilization for 6 weeks by a hard cervical collar. In type 5 fractures a vertebral artery lesion has to be excluded by angio-CT or angio-MRI.
Gehweiler Type 3 Fractures
In stable atlas fractures, type 3a according to Gehweiler, a conservative therapy in a hard collar (eg, Philadelphia collar) is recommended. However, these patients should be carefully followed regarding further dislocation, nonunion, and/or signs for atlantoaxial instability.
For unstable type 3b fractures with minimal displaced bony avulsion of the TAL (type Dickman II), a direct osteosynthesis of the atlas or halo-traction for 6 to 12 weeks is recommended, because it can be assumed that the minimally displaced bony avulsion fragment heals to the lateral mass after atlas ring fixation creating a stable atlantoaxial complex. Although Halo traction is generally possible, nowadays more surgeons prefer the surgical management of these type 3b lesions with regard to the potential discomfort, higher complication rates, and possible nonunions under halo-traction treatment. Postoperatively cervical spine flexion should be limited by a hard collar to avoid secondary dislocation of the minimal displaced bony TAL avulsion.
An isolated atlas osteosynthesis is not recommended in type 3b fractures with severe dislocated bony avulsion of the TAL (type Dickman II), because it cannot be assumed that the severely displaced bony avulsion fragment heals to the lateral mass, ultimately resulting in an unstable atlantoaxial complex. In these cases an atlantoaxial fusion is currently the treatment of choice.
For unstable type 3b fractures with intraligamentous TAL rupture (type Dickman I), an atlantoaxial fusion is also recommended due to the presumed unlikelihood of ligamentous healing potentially resulting in posttraumatic translational atlantoaxial instability. However, several more recent studies support the opinion that if full restoration of the atlas vertebra’s height by reducing the traumatic displacement, and bony healing, are achieved by isolated atlas osteosynthesis, the TAL rupture’s importance for developing atlanto-axial instability seems to be less relevant.19
If a fusion C1-2 is thought to be unavoidable, depending on the anatomical situation and the ability of intraoperative reduction, a posterior atlantoaxial fusion according to Grob and Magerl20 or Melcher and Harms21 are viable treatment options.
Gehweiler Type 4 Fractures
Most of the type 4 fractures are minimal displaced and can be treated conservatively in a hard cervical collar. In case of extended bony involvement with fracture lines compromising vertebral artery foramen, a vertebral artery lesion has to be excluded. In the rare case of a primary or secondary significant dislocation of the fractured lateral mass, resulting in either incongruence of the atlanto-occipital and atlantoaxial joint or in local scoliotic deformity, a reduction under traction and retention for 6 to 12 weeks in a halo-fixator is recommended. Early axial traction leads in most cases to an anatomical lateral mass realignment by ligamentotaxis. However, after initial reduction and after 3, 6, and 12 weeks under halo-traction, a CT evaluation is necessary to confirm an accurate realignment and to assure fracture healing. In case of inadequate initial reduction under halo-traction or early re-dislocation, surgery is indicated in order to maintain reduction. In these cases typically an occipito-atlantal stabilization is required. Due to the potential challenges in achieving a good screw fixation within the fractured lateral mass of C1 and the affection of the atlantoaxial and atlanto-occipital joint, a temporary occipito-cervical stabilization without fusion is recommended. As an alternative, a unilateral lag screw osteosynthesis has been described in oblique fracture patterns without comminution.22 In temporary occipito-cervical stabilizations the implants should be removed after bony healing of the atlas fracture to allow for regaining motion. In case of an inadequate healing and an occipito-atlantal or atlanto-axial joint incongruity under halo-traction resulting in a symptomatic nonunion, fusion of the affected motion segments is recommended to prevent the patient from persistent pain caused by posttraumatic arthritis.
Primary atlas osteosynthesis might also be indicated in cases where a unilateral lateral mass sagittal split fracture is present.13 This fracture type is characterized by a large lateral fragment of the lateral mass completely separated from the anterior and posterior arch. A recent study has indicated that this fracture type, if treated conservatively, often results in a lateral displacement of the lateral fracture fragment accompanied by a subluxation of the occipital condyle and clinically associated with nonradiating neck pain, head malposition (cock-robin-deformity), and diminished head rotation.13
Treatment
Conservative Management
The majority of patients with stable atlas fractures do well under conservative treatment. Due to the fact that there is no evidence suggesting the superiority of any form of external immobilization (halo, hard collar, soft collar) over another, the one with the lowest complication rate might be the best. Specifically in elderly patients, the use of a halo-vest should be avoided, as it has been demonstrated to have high rates of complications in geriatric patients.24
There are only small case series available about successful conservative management of unstable atlas burst fractures. However, some authors from recently reviews advocate 6 to 12 weeks of halo-fixation after reduction under traction to manage these unstable atlas fractures predominantly with Dickman type II lesion. The advantage of stabilization with a halo-vest is seen in the external stabilization without need for surgery with inherent complication risk.23 Another advantage might be the avoidance of atlantoaxial fusion. However, halo-traction as well as fixation in a halo-vest is an invasive form of conservative fracture management not without risks for the patient. Complications of halo-fixators are documented in a publication of Strohm et al,24 who evaluated halo-vest treatment in 41 patients with upper cervical spine injuries. The authors described several complications like fracture re-dislocation (20%) and screw loosening (15%).24 Furthermore, the patients were asked about the treatment comfort of halo-vest treatment with 58% rating it intolerable and only 10% tolerable.24
Due to the discomfort and potential complication of halo-vest treatment and the availability of modern operative techniques, surgical management is recommended for unstable atlas fractures, while halo-traction and halo-vest fixation is the second-choice treatment. The exemption is a displaced Gehweiler type 4 fracture especially in young patients, where the morbidity—even temporary—of occipito-atlanto-axial fixation/fusion has to be balanced individually with the risks and benefits of halo-vest treatment.
Surgical Management
Osteosynthesis of the Atlas
Until today the primary indication for a direct osteosynthesis of the atlas is an unstable burst fracture (Gehweiler type 3b) with bony avulsion of the transverse ligament (Dickman type IIa). However, up until now only mild dislocated bony avulsion fragments should be addressed by this surgical technique, otherwise a good fragment reduction associated with bony healing of the ligament avulsion might be difficult to achieve. Based on current knowledge, potential consequences of nonhealing of the bony avulsion might be a posttraumatic insufficiency of the TAL with chronically pain due to translational atlantoaxial instability.
An osteosynthesis of the atlas can be performed by anterior-transoral, isolated posterior, or by combined posterior/anterior-transoral approach (see Figure 4). For each kind of approach only case series with a few patients are available.
Figure 4.

Different treatment strategies for isolated atlas osteosynthesis: (a) transoral anterior fixation; (b) posterior fixation; (c) combined posterior and anterior fixation. For a detailed description of the surgical techniques, see the main text.
For isolated posterior atlas osteosynthesis a standard midline approach to the upper cervical spine with bilateral lateral mass screw placement has been performed.2,3,19 The trajectory of drilling is given by the anatomy of the lateral mass and especially the fracture lines that have to be carefully analyzed preoperatively.25 Fracture reduction is the key point of the osteosynthesis and might be achieved by a combination of patient positioning, monoaxial screws, dedicated reposition tools, and manually bilateral external neck compression. The permanent fixation is achieved by a screw and rod connection. It is highly recommended to achieve bicortical lateral mass screws fixation because their pull-out strength is significantly higher compared with monocortical C1 lateral mass screws.26
The anterior transoral atlas osteosynthesis was described by Ruf et al27 and is performed by a standard transoral approach. Anteriorly inserted screws should be placed in the “Safe zone.” Detailed anatomical investigations are available regarding these ideal entry points.28
The combined posterior-anterior atlas osteosynthesis described by Böhm et al29 includes a posterior screw fixation using intentionally longer bicortical C1 lateral mass screws with an additional transorally performed wiring between the screw tips to close the C1 ring anterior as well as posterior. This combined procedure enables a sufficient C1-ring reduction. However, due to the increased perioperative risk associated with 2 approaches including a transoral approach, this procedure should not be the first-choice treatment.
Posterior Atlantoaxial Fusion
Today, the indication for posterior atlantoaxial-fusion is given in some unstable atlas burst fractures with intraligamentous lesion of the transvers ligament (type Dickman I) or significant dislocated bony avulsion fragments of the TAL (major dislocated Dickman type II). It is also indicated if translatory atlantoaxial instability develops after conservative management of Dickman type II lesions or failed isolated atlas osteosynthesis.30 Atlantoaxial fusion can be performed either by transarticular C1-2 screw fixation according to Grob and Magerl20 or posterior screw and rod fixation according to Harms and Melcher.21
Conclusion
Current concepts, treatment options, and the recommendations of the experts of the Spine Section of the German Society for Orthopaedics and Trauma have been outlined. Although the evidence for the different, especially surgical, treatment strategies of atlas fractures is very low, surgical stabilization has become a standard treatment modality in specific fracture patterns.
Footnotes
Authors’ Note: The article does not contain information about medical device(s)/drug(s).
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
- 1. Kakarla UK, Chang SW, Theodore N, Sonntag VKH. Atlas fractures. Neurosurgery. 2010;66(3 suppl):60–67. [DOI] [PubMed] [Google Scholar]
- 2. Kandziora F, Chapman J, Vaccaro A, Schroeder G, Scholz M. Atlas fractures and atlas osteosynthesis: A comprehensive narrative review. J Orthop Trauma. In press. [DOI] [PubMed] [Google Scholar]
- 3. Kandziora F, Schnake K, Hoffmann R. Injuries to the upper cervical spine. Unfallchirurg. 2010;113:1023–1041. doi:10.1007/s00113-010-1896-3. [DOI] [PubMed] [Google Scholar]
- 4. Jefferson G. Fracture of the atlas vertebra: report of four cases, and a review of those previously recorded. Br J Surg Lond. 1920;7:407–422. [Google Scholar]
- 5. Dettling SD, Morscher MA, Masin JS, Adamczyk MJ. Cranial nerve IX and X impairment after a sports-related Jefferson (C1) fracture in a 16-year-old male: a case report. J Pediatr Orthop. 2013;33:e23–e27. [DOI] [PubMed] [Google Scholar]
- 6. Domenicucci M, Mancarella C, Dugoni ED, Ciappetta P, Paolo M. Post-traumatic Collet-Sicard syndrome: personal observation and review of the pertinent literature with clinical, radiologic and anatomic considerations. Eur Spine J. 2015;24:663–667. doi:10.1007/s00586-014-3527-0. [DOI] [PubMed] [Google Scholar]
- 7. Sköld G. Fractures of the neural arch and odontoid process of the axis: a study of their causation. Z Rechtsmed. 1978;82:89–103. [DOI] [PubMed] [Google Scholar]
- 8. Panjabi MM, Oda T, Crisco JJ, 3rd, Oxland TR, Katz L, Nolte LP. Experimental study of atlas injuries. I. Biomechanical analysis of their mechanisms and fracture patterns. Spine (Phila Pa 1976). 1991;16(10 suppl):S460–S465. [DOI] [PubMed] [Google Scholar]
- 9. Oda T, Panjabi MM, Crisco JJ, 3rd, Oxland TR, Katz L, Nolte LP. Experimental study of atlas injuries. II. Relevance to clinical diagnosis and treatment. Spine (Phila Pa 1976). 1991;16(10 suppl):S466–S473. [DOI] [PubMed] [Google Scholar]
- 10. Spence KF, Jr, Decker S, Sell KW. Bursting atlantal fracture associated with rupture of the transverse ligament. J Bone Joint Surg Am. 1970;52:543–549. [PubMed] [Google Scholar]
- 11. Heller JG, Viroslav S, Hudson T. Jefferson fractures: the role of magnification artifact in assessing transverse ligament integrity. J Spinal Disord. 1993;6:392–396. [PubMed] [Google Scholar]
- 12. Dickman CAC, Mamourian AA, Sonntag VKV, Drayer BPB. Magnetic resonance imaging of the transverse atlantal ligament for the evaluation of atlantoaxial instability. J Neurosurg. 1991;75:221–227. doi:10.3171/jns.1991.75.2.0221. [DOI] [PubMed] [Google Scholar]
- 13. Bransford R, Falicov A, Nguyen Q, Chapman J. Unilateral C-1 lateral mass sagittal split fracture: an unstable Jefferson fracture variant. J Neurosurg Spine. 2009;10:466–473. doi:10.3171/2009.1.SPINE08708. [DOI] [PubMed] [Google Scholar]
- 14. Hagedorn JC, 2nd, Emery SE, France JC, Daffner SD. Does CT angiography matter for patients with cervical spine injuries? J Bone Joint Surg Am. 2014;96:951–955. doi:10.2106/JBJS.M.00036. [DOI] [PubMed] [Google Scholar]
- 15. Landells CD, Van Peteghem PK. Fractures of the atlas: classification, treatment and morbidity. Spine (Phila Pa 1976). 1988;13:450–452. [DOI] [PubMed] [Google Scholar]
- 16. Gehweiler JA, Osborne RL, Becker RF. The Radiology of Vertebral Trauma. St. Louis, MO: WB Saunders; 1980. [Google Scholar]
- 17. Dickman CA, Greene KA, Sonntag VK. Injuries involving the transverse atlantal ligament: classification and treatment guidelines based upon experience with 39 injuries. Neurosurgery. 1996;38:44–50. [DOI] [PubMed] [Google Scholar]
- 18. Hein C, Richter HP, Rath SA. Atlantoaxial screw fixation for the treatment of isolated and combined unstable Jefferson fractures-experiences with 8 patients. Acta Neurochir (Wien). 2002;144:1187–1192. doi:10.1007/s00701-002-0998-2. [DOI] [PubMed] [Google Scholar]
- 19. Bednar DA, Almansoori KA. Solitary C1 posterior fixation for unstable isolated atlas fractures: case report and systematic review of the literature. Global Spine J. 2016;6:375–382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Grob D, Magerl F. Surgical stabilization of C1 and C2 fractures [in German]. Orthopäde. 1987;16:46–54. [PubMed] [Google Scholar]
- 21. Harms J, Melcher RP. Posterior C1-C2 fusion with polyaxial screw and rod fixation. Spine (Phila Pa 1976). 2001;26:2467–2471. [DOI] [PubMed] [Google Scholar]
- 22. Keskil S, Goksel M, Yuksel U. Unilateral lag-screw technique for an isolated anterior 1/4 atlas fracture. J Craniovertebr Junction Spine. 2016;7:50–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Longo UG, Denaro L, Campi S, Maffulli N, Denaro V. Upper cervical spine injuries: indications and limits of the conservative management in Halo vest. A systematic review of efficacy and safety. Injury. 2010;41:1127–1135. doi:10.1016/j.injury.2010.09.025. [DOI] [PubMed] [Google Scholar]
- 24. Strohm PC, Muller CA, Kostler W, Reising K, Sudkamp NP. Halo-fixator vest-indications and complications [in German]. Zentralbl Chir. 2007;132:54–59. doi:10.1055/s-2006-960479. [DOI] [PubMed] [Google Scholar]
- 25. Sonntag VKH. Lateral mass screw fixation of the atlas: importance of anatomy of C1 for lateral mass screw placement. World Neurosurg. 2010;74:270–271. doi:10.1016/j.wneu.2010.06.010. [DOI] [PubMed] [Google Scholar]
- 26. Eck JC, Walker MP, Currier BL, Chen Q, Yaszemski MJ, An KN. Biomechanical comparison of unicortical versus bicortical C1 lateral mass screw fixation. J Spinal Disord Tech. 2007;20:505–508. [DOI] [PubMed] [Google Scholar]
- 27. Ruf M, Melcher R, Harms J. Transoral reduction and osteosynthesis C1 as a function-preserving option in the treatment of unstable Jefferson fractures. Spine (Phila Pa 1976). 2004;29:823–827. [DOI] [PubMed] [Google Scholar]
- 28. Kandziora F, Schulze-Stahl N, Khodadadyan-Klostermann C, Schröder R, Mittlmeier T. Screw placement in transoral atlantoaxial plate systems: an anatomical study. J Neurosurg. 2001;95(1 suppl):80–87. [DOI] [PubMed] [Google Scholar]
- 29. Böhm H, Kayser R, El Saghir H, Heyde CE. Direct osteosynthesis of instable Gehweiler Type III atlas fractures. Presentation of a dorsoventral osteosynthesis of instable atlas fractures while maintaining function [in German]. Unfallchirurg. 2006;109:754–760. doi:10.1007/s00113-006-1081-x. [DOI] [PubMed] [Google Scholar]
- 30. Jacobson ME, Khan SN, An HS. C1-C2 posterior fixation: indications, technique, and results. Orthop Clin North Am. 2012;43:11–18. doi:10.1016/j.ocl.2011.09.004. [DOI] [PubMed] [Google Scholar]