

Abstract
BACKGROUND:
Many medical students, junior doctors, and other health-care professionals have been affected by the negative experience of bullying. Research is scarce on bullying experienced by medical and nonmedical students in Saudi Arabia unlike what is found in Western countries. It is unclear whether being a nonmedical student modifies the risk of being bullied.
MATERIALS AND METHODS:
A cross-sectional study included 400 university students using convenient sampling. The sample comprised 295 students who responded and were stratified into medical (n = 176) and nonmedical (n = 119) groups. Statistical Package for the Social Sciences (SPSS) version 22.0 was used to analyze our data. Normality was measured using the Kolmogorov–Smirnov test. Statistical significance was tested using chi-square test for categorical variables, and t-test for continuous variables.
RESULTS:
Almost half of the respondents were found to have experienced some bullying, victimization, or other harassment during their medical education. The most common forms of bullying were verbal abuse and undue pressure to produce work (43.8%; n = 77). Nonmedical students experienced more bullying than medical students and were more likely to be female, single, and younger in age. The number of medical students subjected to sexual harassment (1.7%; n = 3) was higher than nonmedical students (0.8%; n = 1). Physical violence was more towards nonmedical (4.2%; n = 5) than medical students (1.1%, n = 2). The rates of bullying continue to be associated with anxiety and depression.
CONCLUSIONS:
Our data suggest similar bullying rates in the developed world but higher than previously reported in a Saudi study. Bullying or harassment affects both medical and nonmedical students and is associated with high levels of anxiety and depression.
Keywords: Bullying, medical students, nonmedical, Saudi Arabia
Introduction
While the term “bullying” has a wide variety of definitions in the literature, for the purpose of our paper, we describe bullying as “a persistent behavior against another individual that is both, degrading, intimidating, malicious, or offensive and undermines the confidence and self-esteem of the recipient.”[1] Bullying in medicine has previously been described in the literature. The profession has a hierarchical structure, and medical students training to become competent physicians are seen as being at the lowest level of this hierarchy. Previous literature has determined that bullying or victimization that includes such terms as abuse, mistreatment, or harassment may affect medical students[2,3,4,5,6,7] as well as physicians in training,[8,9,10,11] physicians conducting research[11] as well as other health-care professionals.[12] In the literature, bullying or victimization of medical students has ranged from 42%[2] to 91%[4] depending on the definition given to bullying.
Literature reveals that more often than not, bullying or victimization tends to be connected to training situations, and medical students may find this upsetting but inevitable.[13] For example, a feedback on the appraisal of the performance of trainees is sometimes construed as a negative experience, depending on who gives the feedback and the way it is delivered. However, it is well documented in the literature that perceived mistreatment is the most common source of stress as seen by medical students and junior physicians.[10] One study in 2003 showed that more than one-third of medical students considered dropping out of medical school. Of those, approximately one-fourth said that they would have chosen a different profession had they been apprised of the rates of bullying and victimization that occur in a medical school.[14] Several studies have shown that the extent of bullying or victimization can be associated with long-term mental health outcomes, which may include a diagnosis of depression. It is also documented that adverse outcomes such as attempts at suicide by physicians are not uncommon.[14,15,16,17]
Research in Pakistan and other neighboring countries find that there is extensive bullying and victimization of both psychiatry trainees[11] and consultant psychiatrists.[18] There is only one study of the extent of bullying and victimization of medical students in Saudi Arabia.[19] Yet, to date, no research has been conducted in Saudi Arabia to examine the prevalence of bullying experienced by medical students. This study, therefore, was to examine the prevalence of bullying or victimization of medical students in Saudi Arabia and whether medical students experience more bullying than nonmedical students in this cohort.
Materials and Methods
The study had a cross-sectional design in which bullying of medical students was compared with nonmedical students. Students at International American University (medical and nonmedical), regardless of their year of study, age, or academic performance, were invited to participate in this study. Invitations were given directly as the questionnaires were being distributed. Of the 400 university students randomly invited to take part in this study, 295 showed interest and were included in this study. These were 176 medical students and 119 nonmedical students giving a response rate of 73.75%. Those included were medical students enrolled in the medical college and nonmedical students in the colleges of Engineering, Interior Design, and Business Management of the Imam Abdulrahman Bin Faisal University (IAFU) in the Eastern Province of Saudi Arabia.
We distributed the survey together with a form for written informed consent. Those who were interested in participating completed the consent form before their inclusion. The participation of consenting subjects (adults) was voluntary, and an anonymous survey was utilized for data collection. Confidentiality was met as no patient identifiable information was collected. Approval was obtained from the Institutional Review Board Ethical Committee of the IAFU before the commencement of the study.
A key person, either a senior postgraduate trainee or consultant, who had contacted both medical students and nonmedical students, collected the data in each college. Forms were distributed at the beginning of lectures and collected at the end of the lectures. The Medical Student's Welfare Survey, a data collection tool used by the British Medical Association, was distributed.[3] Two forms each were given out, one of which sought basic socioeconomic demographic details and asked whether the student had been subjected to bullying or victimization while in school or college. If the student answered “yes” to bullying, further details were required using a validated Arabic version of the Patient Health Questionnaire-9 (PHQ-9) and Generalized Anxiety Disorder Assessment (GAD-7) to assess the levels of depression and anxiety, respectively. These scales were used as they are multipurpose instruments for screening, diagnosing, monitoring, and measuring the severity of depression and anxiety.
The PHQ-9 is the 9-item depression module from the full PHQ, which scores each of nine DSM-IV criteria as “0” (not at all) to “3” (nearly every day). It includes statements such as “little interest or pleasure in doing things; feeling down, depressed or hopeless; trouble falling/staying asleep or sleeping too much; feeling tired or having little energy; poor appetite or overeating; feeling bad about oneself or that one is a failure or has let one's family down; trouble concentrating on things such as reading the newspaper or watching TV; moving slowing or the opposite, being so fidgety or restless that you have been moving around more than usual; and morbid thoughts of death or thoughts of self-harm.” The PHQ-9 is a reliable, valid dual-purpose measurement instrument of depression, with the same nine items making criteria-based diagnoses of depressive disorders as well as grading the severity of the depressive symptoms. Before making a final diagnosis, the clinician was expected to rule out any physical causes of depression, normal bereavement, and history of a manic episode.
The GAD-7 is a 7-item screening tool that measures the severity for anxiety disorders including GAD, panic disorder, social phobia, and posttraumatic stress disorder. The questionnaire includes a rating scale from “0” (not at all sure) to “3” (nearly every day).” It includes statements that are rated on this scale such as “feeling nervous, anxious or on edge; not being able to stop or control worrying; worrying too much about different things; trouble relaxing; being so restless that it's hard to sit still; becoming easily annoyed or irritable and; and apprehensive of impending doom.” It is 70%–90% sensitive and 80%–90% specific across disorders/cutoffs.
Statistical Package for the Social Sciences (SPSS) version 22.0 (IBM, Chicago, Illinois, USA) was used to analyze the data. Both parametric and nonparametric tests were carried out to compare groups. SPSS frequency and descriptive commands were used to measure descriptive statistics. Normality was measured using the Kolmogorov–Smirnov test. Chi-square analysis was used to determine associations between categorical variables and t-tests were used for continuous variables. All test performed at 0.05 significance level.
Results
The calculation of our sample was based on the prevalence rate reported in the study by Alzahrani 2012[20] and followed the guidance provided by Pourhoseingholi et al.[21] Based on a prevalence rate of 28%, confidence interval of 95%, and precision of 0.01, the sample size was 78. We included enough students in each group to achieve that together with a response rate of around 50%.
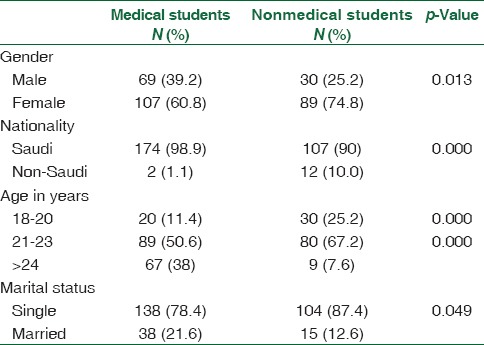
Sociodemographic characteristics showed that a total of 176 medical students and 119 nonmedical students participated in this study [Table 1]. Final analyses were conducted on the returned survey forms. The majority of the respondents (95%; n = 281) were Saudi and were aged between 18 and 23 (74%; n = 219). Thirty-four percent (34%; n = 99) were male and 82% (n = 242) were single. There were no statistically significant differences between the two subgroups of the sample studied though the medical subgroup was larger in number (176 vs. 119) and older (38% vs. 7.6%) than the nonmedical subgroup.
Table 1.
Medical and nonmedical students in sociodemographic characteristics differences
The overall prevalence rate of reported exposure to one form or another of bullying as university students (medical and nonmedical) was almost half (49.0%; n = 146) of the respondents of the sample. Of the medical students, the prevalence rate of bullying was 44% and 58% among the nonmedical students [Table 2].
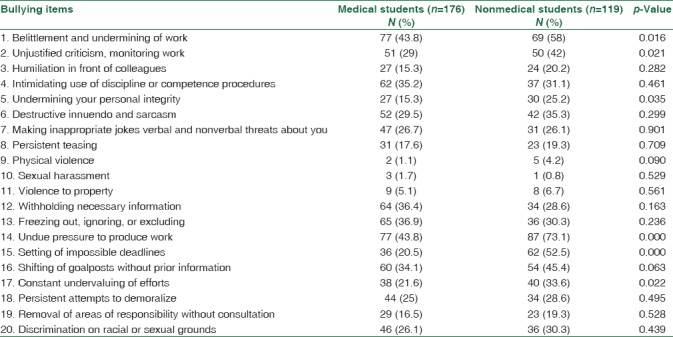
Table 2.
Comparison of the types of bullying between the two groups
The comparison of the two groups showed that nonmedical students were bullied more than medical students [Table 3], and those bullied were more likely to be female, single, and younger.
Table 3.
Means comparison for bullying, depression, and anxiety among medical and nonmedical students
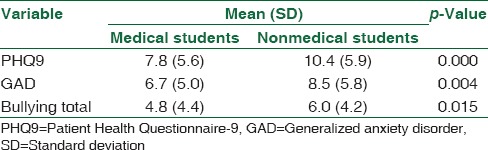
When the two groups were compared for the type of bullying experienced, there were no statistically significant differences in most of their experiences [Table 2]. The most common types of abuse suffered by the medical students were belittlement and undermining of work as reported by approximately 43.8% of the respondents. A similar number (43.8%; n = 77) were subjected to increased pressure to produce work. Only 36.9% (n = 65) of the cohort were subjected to such bullying or victimization as: “freezing out, ignoring, or excluding tactics.” Another 36.6% (n = 64) of the medical students felt bullied when important, necessary information was withheld from them. Shifting of goalposts without any warning or information to the medical students was a bullying technique that affected 34% (n = 60) of the cohort. The number of medical students subjected to sexual harassment (n = 3; 1.7%) was higher than what the nonmedical students (n = 1; 0.8%) experienced. However, physical violence was reported more by nonmedical (4.2%; n = 5) than medical students (1.1%, n = 2). Bullying was correlated with depression (r = 0.47) and anxiety (0.41) scores [Table 3].
Discussion
Bullying and victimization of medical students by those higher on the medical hierarchy can adversely impede the medical educational process and ruin one's educational experience. These experiences may also lead to long-lasting psychological scars and impairment. The literature of the last decade suggests that the prevalence and effects of bullying or victimization are well known and established.[1,2,3,4,5] However, it is difficult to compare these studies across cultures and populations owing to differing sociocultural characteristics as well as different research methodologies. Despite this, it appears that medical students across the world are not immune to the effects of bullying or victimization.
This current survey is the second published study of bullying from Saudi Arabia. However, unlike previous studies, the current document assessed and compared the phenomena of bullying of both medical and nonmedical students. It established the prevalence rate in those two groups, similarities, and possible factors contributing to any differences. In the current study, almost half of the responders had been victims of bullying. A previous study in Saudi Arabia by Alzahrani[20] found bullying to be much lower at a rate of 28%. A study conducted in the United States reported that 42% of medical students described episodes of harassment during their training and 84% described episodes of belittlement as well; this was compared with a study in Finland which reported a 50% prevalence of bullying.[3,4] These reported rates in the United States and Finland are lower than those of some other Middle Eastern countries such as Jordan which reports rates of 61%, and Pakistan which reports 52%.[1,2] Interestingly, as one reads through this literature, the rates of bullying or victimization increase as the medical students progress through three clinical levels.
Similar to previous literature, the current study concludes that the most common form of bullying includes verbal abuse, being shouted at, humiliation, and belittlement. Prevalence rates of sexual harassment in the previous literature range widely from 18%–60%. Female medical students in a Dutch study reported a rate of 20%–33% unwelcome sexual attention from patients, colleagues, or supervisors.[5] The present study found a much lower rate than this. In fact, the current rate reported in our study is even lower than the rate of 6% reported in Jordan. While three medical students and one nonmedical student reported that they had been exposed to sexual abuse, they disclosed that they had not reported the incidents to those in authority. Various reasons may have contributed for such under-reporting. One such factor is that, in the local culture, any discussion of bullying or victimization, especially a discussion of sexual abuse or harassment, is particularly frowned upon. It is, therefore, possible that students are reluctant to report sexual harassment for cultural reasons.
A study of medical students in Pakistan found that just over half the students in their final year of training reported being bullied or victimized during their training. They, too, reported that verbal abuse was the most common form of bullying and indicated that their superiors were the most frequent offenders at 46%. Interestingly, an increased risk of being bullied was associated with older age, male gender, the absence of an antibullying policy in their college, and a perception of lack of support. In the Pakistani study previously mentioned, males were more likely to have experienced bullying than their female counterparts. Yet, an analysis of subgroups shows that males were more likely to be the victims of bullying by consultant physicians, whereas females described difficulties with nurses, patients, peers, and resident physicians. It is postulated that consultants have been found to be the perpetrators of approximately half of bullying experienced by students; the results also show that males tend to report more bullying overall.
However, much of the previous literature except two studies indicate that females were more likely to talk about bullying than males,[2,5,6,7,15,19,20,21] Frank et al.[2] in their paper said that gender appeared to be only slightly significant for bullying by preclinical professors, with males reporting a 7% prevalence versus females reporting 7% frequency. However, they did not describe bullying by other groups in the medical hierarchy. Uhari's study[7] found that male students together discussed bullying by classmates, preclinical teachers, clinical preceptors, clinicians, and patients. Those studies, which have examined widespread bullying, find that sexual harassment tends to be more common with females.[2] In the current study, we found that the number of medical students subjected to sexual harassment was higher than nonmedical students, but we did not describe the data by gender and so cannot comment properly on this. We did note, however, that, in our sample, the reported sexual harassment was low, which could be because only a few students had experienced this form of harassment, possibly because of the conservative nature of our society.
In previous literature, and as discussed earlier, the perception of the lack of adequate support within an institution was an important observation. We wonder, then, if those who felt unsupported during their medical training were more likely to have experienced bullying or victimization or could it possibly reflect a pervasive culture of that particular medical college? This may be an important discussion for the future.
It is possible that there has been a reporting bias as those who had experienced bullying were more likely to have taken part in the survey and thus inflated the prevalence. However, this study had a 73.75 response rate, and seeing that 50% of respondents reported that they had never experienced bullying or harassment, we think that this may not have significantly influenced the results. This finding is almost a universal.[2,3,4,5,11] It is also noted that a limitation of this study may be the tools used for survey. Although these tools were primarily designed for medical students and their trainers, their content is valid for nonmedical students as well. A further limitation was the selection of participants who described bullying or victimization and were screened later for anxiety and depression. This may have been a valuable construct to use for other cross-sectional studies.
This study was limited to bullying or victimization perpetrated by consultants, clinical professors, and tutors as they were said to be the most frequent perpetrators in previous studies.[1,2,3] Future studies may include a more detailed questionnaire, which defines all forms of bullying in more detail, particularly sexual harassment, a topic that could be explored further. As far as we know the Medical Student's Welfare Survey has been validated for medical students, but we expect it to be applicable to nonmedical students in our study, since as university students they have a lot of social and academic issues in common with the medical students. Unfortunately, hindsight tells us that calculating the response rate separately for each group could have given us a better insight into the problem for each group.
Conclusion
Bullying rates in this study are quite similar to those reported in the literature of the developed world and higher than the previous Saudi study by Alzahrani.[20] It is possible that this prevalence report may be attributed to under-reporting and cultural factors. It appears that both medical and nonmedical students are subjected to bullying and harassment, and therefore, measures need to be taken at the institutional level to prevent this. It is important to tackle the issue of bullying because of the growth of higher medical education and the increase in the number of colleges and medical schools in Saudi Arabia over the past decade. Therefore, it is necessary to deal with the issue at this stage as a safeguard to prevent it from becoming widespread.
Medical students learn not only the complexities of the medicine but also behavior patterns of their seniors and mentors, the so-called “hidden curriculum of undergraduate medical education.”[22] The rates of bullying or victimization revealed both in this study and around the world indicate that this is clearly an issue that needs to be addressed. Previous literature has shown that certain protective factors such as having a policy in place against bullying or victimization in the medical college and making students aware of available support for any individuals thus affected are necessary. Improving the awareness of medical colleges about the prevalence of bullying or victimization and providing such support for victims could be the way forward. There should be a policy in institutions to safeguard against victimization and provide support for victims of bullying. This is essential since bullying is associated with high levels of anxiety and depression. It may also be possible to reduce the rate of bullying or victimization through staff development. It is clear that future national studies in Saudi Arabia as well as other countries with similar backgrounds are required.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Managing Conflict at Work: A Survey of the UK and Ireland. London: Chartered Institute of Personnel and Development; 2004. Chartered Institute of Personnel and Development. [Google Scholar]
- 2.Frank E, Carrera JS, Stratton T, Bickel J, Nora LM. Experiences of belittlement and harassment and their correlates among medical students in the United States: Longitudinal survey. BMJ. 2006;333:682. doi: 10.1136/bmj.38924.722037.7C. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wood DF. Bullying and harassment in medical schools. [Last accessed on 2006 Sep 28];BMJ. 2006 333:664. doi: 10.1136/bmj.38954.568148.BE. Available from: doi: https://doi.org/10.1136/bmj.38954.568148.BE . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Maida AM, Vásquez A, Herskovic V, Calderón JL, Jacard M, Pereira A, et al. A report on student abuse during medical training. Med Teach. 2003;25:497–501. doi: 10.1080/01421590310001606317. [DOI] [PubMed] [Google Scholar]
- 5.Rautio A, Sunnari V, Nuutinen M, Laitala M. Mistreatment of university students most common during medical studies. BMC Med Educ. 2005;5:36. doi: 10.1186/1472-6920-5-36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Richardson DA, Becker M, Frank RR, Sokol RJ. Assessing medical students' perceptions of mistreatment in their second and third years. Acad Med. 1997;72:728–30. doi: 10.1097/00001888-199708000-00022. [DOI] [PubMed] [Google Scholar]
- 7.Uhari M, Kokkonen J, Nuutinen M, Vainionpaa L, Rantala H, Lautala P, et al. Medical student abuse: An international phenomenon. JAMA. 1994;271:1049–51. doi: 10.1001/jama.271.13.1049. [DOI] [PubMed] [Google Scholar]
- 8.Paice E, Aitken M, Houghton A, Firth-Cozens J. Bullying among doctors in training: Cross sectional questionnaire survey. BMJ. 2004;329:658–9. doi: 10.1136/bmj.38133.502569.AE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Quine L. Workplace bullying in junior doctors: Questionnaire survey. BMJ. 2002;324:878–9. doi: 10.1136/bmj.324.7342.878. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Daugherty SR, Baldwin DC, Jr, Rowley BD. Learning, satisfaction, and mistreatment during medical internship: A national survey of working conditions. JAMA. 1998;279:1194–9. doi: 10.1001/jama.279.15.1194. [DOI] [PubMed] [Google Scholar]
- 11.Ahmer S, Yousafzai AW, Bhutto N, Alam S, Sarangzai AK, Iqbal A, et al. Bullying of medical students in Pakistan: A cross-sectional questionnaire survey. PLoS One. 2008;3:e3889. doi: 10.1371/journal.pone.0003889. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Stebbing J, Mandalia S, Portsmouth S, Leonard P, Crane J, Bower M, et al. A questionnaire survey of stress and bullying in doctors undertaking research. Postgrad Med J. 2004;80:93–6. doi: 10.1136/pmj.2003.009001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Quine L. Workplace bullying in NHS community trust: Staff questionnaire survey. BMJ. 1999;318:228–32. doi: 10.1136/bmj.318.7178.228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Paice E, Firth-Cozens J. Who's a bully then? BMJ. 2003;326:S127. doi: 10.1136/bmj.326.7393.S127. [DOI] [PubMed] [Google Scholar]
- 15.Sheehan KH, Sheehan DV, White K, Leibowitz A, Baldwin DC., Jr A pilot study of medical student ‘abuse'. Student perceptions of mistreatment and misconduct in medical school. JAMA. 1990;263:533–7. [PubMed] [Google Scholar]
- 16.Larsson C, Hensing G, Allebeck P. Sexual and gender-related harassment in medical education and research training: Results from a Swedish survey. Med Educ. 2003;37:39–50. doi: 10.1046/j.1365-2923.2003.01404.x. [DOI] [PubMed] [Google Scholar]
- 17.Richman JA, Flaherty JA, Rospenda KM, Christensen ML. Mental health consequences and correlates of reported medical student abuse. JAMA. 1992;267:692–4. [PubMed] [Google Scholar]
- 18.Frank E, Dingle AD. Self-reported depression and suicide attempts among U.S. Women physicians. Am J Psychiatry. 1999;156:1887–94. doi: 10.1176/ajp.156.12.1887. [DOI] [PubMed] [Google Scholar]
- 19.Gadit AA, Mugford G. A pilot study of bullying and harassment among medical professionals in Pakistan, focussing on psychiatry: Need for a medical ombudsman. J Med Ethics. 2008;34:463–6. doi: 10.1136/jme.2007.021832. [DOI] [PubMed] [Google Scholar]
- 20.Alzahrani HA. Bullying among medical students in a Saudi medical school. BMC Res Notes. 2012;5:335. doi: 10.1186/1756-0500-5-335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Pourhoseingholi MA, Vahedi M, Rahimzadeh M. Sample size calculation in medical studies. Gastroenterol Hepatol Bed Bench. 2013;6:14–7. [PMC free article] [PubMed] [Google Scholar]
- 22.Nora LM, McLaughlin MA, Fosson SE, Stratton TD, Murphy-Spencer A, Fincher RM, et al. Gender discrimination and sexual harassment in medical education: Perspectives gained by a 14-school study. Acad Med. 2002;77:1226–34. doi: 10.1097/00001888-200212000-00018. [DOI] [PubMed] [Google Scholar]