

Abstract
BACKGROUND:
Workplace violence in healthcare settings is a common, but an underreported problem that has been largely ignored. Violence against healthcare workers can have an adverse effect on their performance outcomes and thus influence patients' health and satisfaction. The aim of this study was to determine the frequency and types of violence against healthcare workers in a Saudi Arabian city. It was also to identify the risk factors of violence against healthcare workers and to investigate the possible consequences of such behavior.
MATERIALS AND METHODS:
In Abha city, there are two government hospitals and ten primary healthcare centers. All healthcare workers in these healthcare institutions including physicians, nurses, dentists, pharmacists, laboratory technicians or specialists, radiologists, social workers, and psychologists were eligible to participate in this cross-sectional study. Data were collected using a structured self-administered questionnaire.
RESULTS:
A total of 738 healthcare workers responded (92% response rate). The mean age was 31 ± 7.7 years (range 21–60) and the majority (64.9%) were females and 69.4% were Saudis. More than half (57.5%) had experienced some workplace violence at least once. Verbal assaults and slaps were the most common form of workplace-related violence (58%).
CONCLUSIONS:
Violence against healthcare workers in Abha city is more common, especially against nurses. The reasons need to be explored in order to set and develop policies, regulations and interventions to prevent violence against workers.
Keywords: Healthcare workers, Saudi Arabia, violence
Introduction
Healthcare workers are at high risk of violence all over the world. Between 8% and 38% of healthcare workers suffer some physical violence at some point in their careers.[1] Many more are threatened or exposed to verbal aggression.[1] Most violence is perpetrated by patients and visitors. Also, in disaster and conflict situations, health workers sometimes become the targets of collective or political violence.[1] The categories of health workers most at risk are nurses and other staff directly involved in patient care, emergency room staff, and paramedics.[1] Violence against healthcare workers can have a negative impact on their performance outcomes and consequently influence patients' health and satisfaction.[2] The National Institute for Occupational Safety and Health (NIOSH) defines workplace violence as “violent acts, including physical assaults and threats of assaults, directed toward persons at work or on duty”.[3] Hospitals have a special status and role in public health and health care, as they are the terminal points of health service systems.[4] In the USA, the NIOSH notes that the public place where most violence toward employees is observed is hospitals.[5] In other words, healthcare workers are the professionals who are the most vulnerable to workplace violence.[6]
The sources of violence against healthcare workers were varied: some from the patients or from patients' relatives or even other health workers. When violence occurs in the workplace, there are direct and indirect consequences for both staff and patients, as well as compromised patient care.[7]
In a study conducted in 2009, in Al-Hassa, Saudi Arabia, it was found that about 28% of the 1091 workers studied had been exposed to at least one violent event in the previous year; 92.1% of this was emotional and 7.9% physical.[8]
Another study done in 2012 on Palestinians showed that around 80.4% of physicians and nurses reported that they had been victims of violence in the previous 12 months. Some of the many reasons were the lack of incident reporting policy/procedure and management support, previous experience of lack of action against the perpetrators, and fear of adverse consequences.[9] Another study done in the emergency departments of Palestinian hospitals in 2013 showed that around 35.6% of staff had been exposed to physical assaults and 71.2% exposed to nonphysical assaults.[10]
The studies conducted in health institutions in Aseer Region are not enough to give us a clear picture of the violence against healthcare workers. More research is, therefore, required to explore this issue further. This study aimed to determine the frequency and types of violence against healthcare workers in a Saudi Arabian city. It was also to identify the risk factors of violence against healthcare workers and investigate the possible consequences of this behavior.
Materials and Methods
The current study included a representative sample of all healthcare workers in the government health sector in Abha. In the city of Abha, there were two government hospitals and ten primary healthcare centers (PHCCs). All healthcare workers in these institutions including physicians, nurses, dentists, pharmacists, laboratory technicians or specialists, radiologists, social workers, and psychologists were eligible to participate. A cross-sectional study was conducted using a random sampling technique. A total of 800 healthcare workers were invited to participate. Of them, 738 healthcare workers responded with complete data giving a response rate of 92.2%. Of 738 workers, 151 were selected from ten PHCCs and 587 from two government hospitals (Aseer Central Hospital and Abha General Hospital). All health workers in the selected PHCCs as well as those working in different departments of the hospitals were randomly selected by a proportional allocation technique.
Data were collected using a structured self-administered questionnaire designed by the study researchers and reviewed by two independent experts. Comments and modifications suggested by the experts were used to improve the reliability and validity of the questionnaire which covered demographic data and work-related data including job title and job timing. There was a definition of violence at the beginning of the questionnaire, as well as a complete section which dealt with exposure to violence, types of violence, effects of violence, and on performance and the perceived causes of violence. The questionnaire was distributed to the eligible staff who had given their consent to participate and were collected the next day or later, until all complete records had been received. Ethical approval from the institutional review board/ethics committee had been obtained, and informed written consent was obtained from all participants in the study. Statistical Package for the Social Sciences (SPSS) version 23 (IBM Corporation, Armonk. New York, USA) was used for data entry and analysis after filtering error from the data. Descriptive statistics were used as the number of frequencies and percentage for categorical data. Chi-square or Fisher's exact tests were used to test the association between participants' exposure to violence and their demographic and work-related characteristics. P ≤ 0.05 was considered statistically significant. All presented graphs were constructed using Microsoft Office Excel Software 2016.
Results
A total of 738 healthcare workers responded. The mean age was 31 ± 7.7 years (range 21–60), and the majority of healthcare workers were female (64.9%). The study included 512 (69.4%) Saudis and 226 (30.6%) non-Saudis. More than half (57.5%) of healthcare workers had experienced some kind of workplace violence at least once [Figure 1]. Regarding the types of violence, 55.9% of healthcare workers who had been exposed to violence had been verbally abused, 32.9% had been exposed to both physical and verbal violence, and only 11.1% had been exposed to physical violence only [Figure 2]. Slaps with verbal abuse were the most commonly recorded violent actions (58%) followed by other unpleasant experiences (17%), being pushed (17%), being spat at (13%), restraining and punching were the least frequent (5% for both) [Figure 3].
Figure 1.
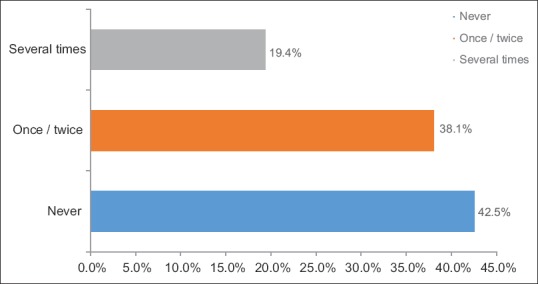
Prevalence of exposure to violence among healthcare workers
Figure 2.
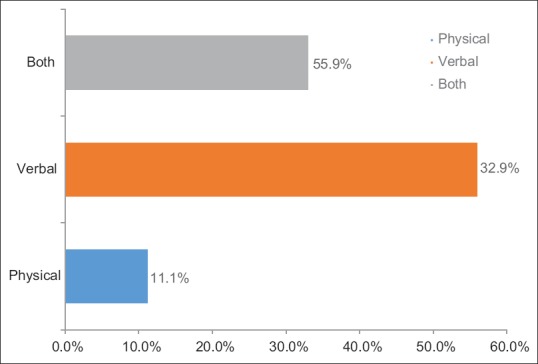
Types of violence experienced by healthcare workers
Figure 3.
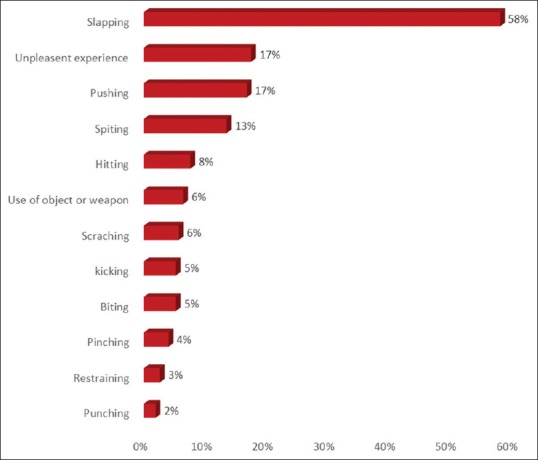
Types of experienced violence
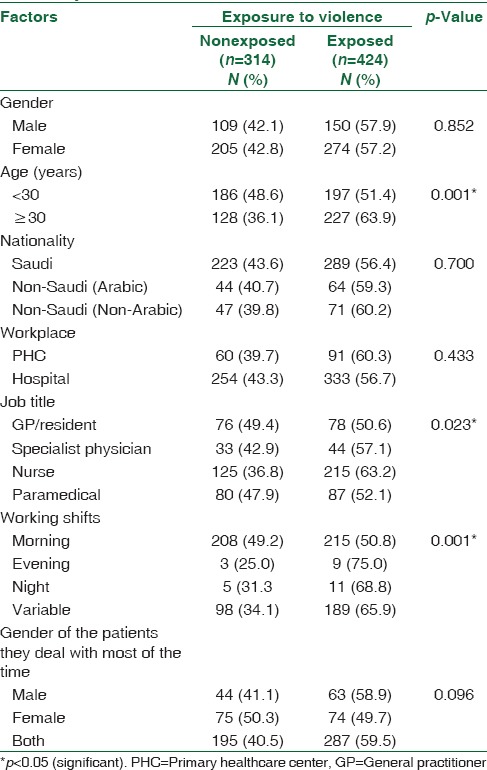
Table 1 shows that 57.9% of the male workers had been exposed to violence compared to 57.2% females with no statistical significance (P > 0.05). With regard to age, 63.9% of the healthcare workers above the age of 30 years were exposed to violence compared to 51.4% of those below 30 years (P < 0.05). On nationality, 56.4% of the Saudi staff had experienced some violence in comparison to 60.2% foreign non-Arabic staff (P > 0.05). In addition, about two-thirds of the staff in PHCCs had experienced some violence compared to 56.7% of the hospitals staff. According to job, the most frequent exposed to violence were nurses (63.2%) while those the least affected were general practitioner (GP)/resident staff (50%) (P <0.05). Violent behavior occurred most frequently during the night shift (68.8%) and least frequently during the morning shift (50.8%), with recorded statistical significance (P < 0.05). Regarding to patients ‘gender that staff dealt with, about 59% of the staff who dealt with male patients had been abused compared to 49% of those who dealt with female patients. Statistical significance was borderline.
Table 1.
Relation between history of exposure to violence and characteristics of healthcare workers in Abha city
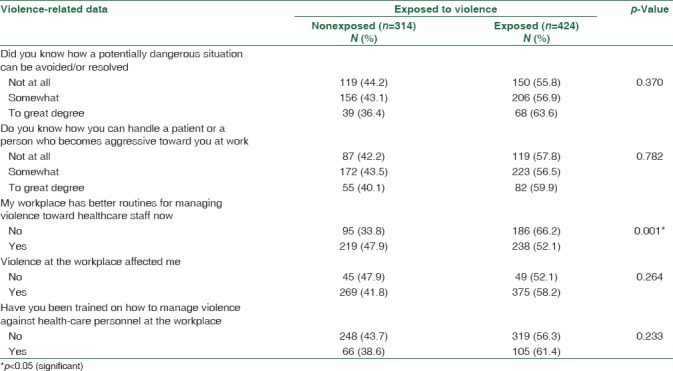
On relating exposure to violence and violence-related experience among the interviewed staff [Table 2], it was clear that 63.6% of the staff who knew how to avoid dangerous situations were exposed to violence compared to 55.8% of those who did not. Further, staff who were able to handle aggressive patients and those who could not had been exposed to a similar number of violent actions (around 58% for both). More than half (52.1%) of the staff working at settings with planned routine for managing violent behavior were exposed to violence compared to 66.2% of those who had no plans against violence in place in their workplace (P < 0.05). About 58% of those who had been exposed to violence reported that there was an effect on their performance. Two-thirds of those who had been taught how to deal with violent behavior had been exposed to violence at least once compared to 56.3% of others who had not had any training.
Table 2.
Relation between history of exposure to violence and violence-related experiences of healthcare workers
A multiple logistic regression modeling was done to identify the predictors of violence against healthcare workers [Table 3]. The model included all studied characteristics of the sample as predictors for violence, among which age, job title, and working shifts, keeping all other factors constant, were found to be statistically significant predictors.
Table 3.
Predictors of violence among healthcare workers
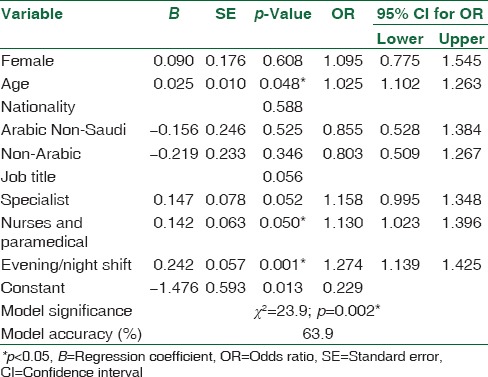
With regard to age as a predictor, it was found that older healthcare workers were associated with increased risk of violence by about 3% more than younger healthcare workers (odds ratio [OR] =1.03; P = 0.048). Specialists were 15% more at risk of being assaulted at their work place than GPs (OR = 1.15; P = 0.052) while nurses and paramedical jobs were shown to be 13% more at risk (OR = 1.13; P = 0.050). With regard to shifts, those who worked evening and night shifts were 27% more at risk of violence from inpatients or their relatives than those who worked mainly in the mornings (OR = 1.27; P = 0.001). All studied predictor effects were adjusted for other included predictors. As for model significance, P value for the model was < 0.01 with overall classification accuracy of about 64% (moderate model quality).
Figure 4 outlines the causes of workplace violence as perceived by the sampled healthcare workers. Patients' or relatives' lack of education and long waiting time were the most perceived causes (56% for each), followed by culture and personality (55%), staff shortage (52%), overcrowding (48%), workload (42%), and lack of security (41%). Drug abuse by patients' relatives and the lack of witnesses were the least perceived causes (22% and 19%, respectively).
Figure 4.
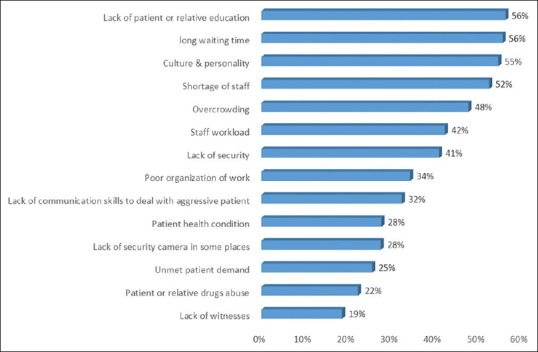
Perceived causes of violence reported by healthcare workers
Discussion
Workplace violence includes harassment, verbal threats, and physical assaults. One-third of all nonfatal injuries and lost days as a result of violence in the workplace occur in healthcare settings.[11] Healthcare workers are at a high risk of violence. This study revealed that more than half (57.5%) of the participating healthcare workers had experienced at least one type of violence at the workplace. These findings had agreed with those reported by Hegney et al.,[12] who concluded that 60% of their participants had experienced some form of workplace violence. Farrell et al.[13] in Tasmania reported that as high as 63.5% of their participants had experienced verbal or physical abuse in the past 4 working weeks. Local studies such as those done by El-Gilany et al.[8] in Al-Hassa, Saudi Arabia, reported that verbal and physical violence accounted for 92.1% and 7.9% of violent workplace events against healthcare providers, respectively.
In the current study, verbal abuse was recorded in 55.9% of those who were exposed to violence followed by 32.9% who had been exposed to both physical and verbal abuse while only 11.1% were exposed to physical violence only. Opie et al.[14] reported that the most common forms of violent incidents at the workplace in Australia against nurses were verbal aggression, followed by physical violence.
Most surveys on violence against healthcare personnel have revealed that verbal abuse is usually more common than physical violence.[15] Variable prevalence rates of physical violence experienced by healthcare personnel within the last 12 months were reported in Sophia, Bulgaria (7.5%); Rio de Janeiro, Brazil (6.4%); Beirut, Lebanon (5.8%); Thailand (10.5%); and Johannesburg, South Africa (9%–17%). While, the experiences of verbal abuse against healthcare personnel within the last 12 months were reported as follows: 67% in Australia, 39.5% in Brazil, 32.2% in Bulgaria, 40.9% in Lebanon, 27.4%–51% in Portugal, 52%–60.1% in South Africa, 47.7% in Thailand, and 72.5% in Karachi.
The results of the present study showed that the perpetrators of violence were mainly patients or their relatives. Violent behavior occurred more in the night shifts (68.8%) and was least frequent during the morning shifts (50.8%) with recorded statistical significance of P < 0.05. In Mansoura, Egypt, Abou-ElWafa et al.[16] found that doing shift work, younger age, and having few colleagues were significant independent predictors of different types of violence.
The causes of violence as perceived by the sampled healthcare workers were the lack of education and long waiting time (56% for each), followed by culture and personality (55%), staff shortage (52%), overcrowding (48%), workload (42%), lack of security (41%), while drug abuse by patients' relatives was recorded by 22% and the lack of witnesses by 19%. These figures are as same as those suggested by Roakes.[17] He suggested that the reasons for the high prevalence of workplace violence in emergency departments were understaffing, inadequate security, long waiting times, lack of privacy, and anger from patients and families. Gillespie et al.[18] mentioned certain characteristics that have been found to be more associated with increased risk of being targets of violence at workplace in the healthcare setting. They included the gender of the worker, age, years of experience, marital status, and previous training in workplace violence.
El-Gilany et al.,[8] in Al-Hassa, Saudi Arabia, concluded that the leading contributing factors for workplace violence include unmet needs of patients, overcrowding, and reaction to injury or illness.
Night shifts are associated with higher prevalence of violent incidents. This may be due to the fact that patients who come to a health center at night are usually urgent cases with a low threshold for waiting and perhaps are unwilling to listen any advice or excuse from healthcare providers.
All the findings indicate that violence against healthcare workers is common and that healthcare providers should be advised, trained, and encouraged to report incidents of violence either against them. Hospital/primary healthcare administrators should follow up reported incidents, take action against the perpetrators, and provide feedback to the victims. In addition, administrators and supervisors should provide support to those who report the violent incidents and protect them against adverse repercussions. However, patients and their relatives should be educated on patients' rights and policy, and how to lodge a complaint soon after an event in order to get satisfactory outcomes for all parties involved. There is an urgent need for the control and prevention of violence in healthcare facilities.
It is noteworthy that none of participants in the present study reported any incidents of sexual harassment. Kisa et al.[19] explained that the issue of sexual harassment in healthcare institutions has not been adequately investigated in the Middle East region because healthcare workers, especially females, would be reluctant to respond to questions due to the cultural sensitivity of the issue and the fear of being stigmatized. Therefore, studies on this matter with an assurance of extreme confidentiality are needed. However, even though recall bias is one of the limitations of this study, the main issue is training the health workers in how to deal with violent behavior. In addition, managers and administrators have to establish rules and regulations on violence in the workplace.
Conclusions
Like all other employees, healthcare workers have a right to being safe at work. Unfortunately, violence against healthcare workers in Abha city is more common, especially verbal insults with physical assaults. Nurses were the largest category of workers exposed to violence, especially at PHCCs. The reasons need to be further explored in order to help develop policies, regulations, and interventions to prevent violence. Healthcare workers need to learn how to deal with such situations when they arise. There are also gaps in the research on the effect of workplace violence on healthcare staff and healthcare outcomes. Preventive measures are urgently needed to reduce the incidence of workplace violence and make healthcare institutions safer places of work.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.WHO. Violence against Health Workers. [Last accessed on 2017 Oct 25]. Available from: http://www.who.int/violence_injury_prevention/violence/workplace/en .
- 2.Schyve PM. The Joint Commission. Preventing Violence in the Health Care Setting. [Last accessed on 2016 Oct 19]. Available from: https://www.jointcommission.org/jc_physician_blog/violence_in_the_health_care_setting/
- 3.U.S. Department of Labor. Occupational Safety and Health Administration: Guidelines for Preventing Workplace Violence for Health Care and Social Service Workers (OSHA3148-01R, 2004) 2007b. [Last retrieved on 2017 Mar 20]. Available from: http://www.osha.gov/index.html .
- 4.Morken T, Johansen IH, Alsaker K. Dealing with workplace violence in emergency primary health care: A focus group study. BMC Fam Pract. 2015;16:51. doi: 10.1186/s12875-015-0276-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Violence: Occupational Hazards in Hospital. Cincinnati, OH, USA: National Institute for Occupational Safety and Health; 2002. Centers for Disease Control and Prevention. [Google Scholar]
- 6.Kamchuchat C, Chongsuvivatwong V, Oncheunjit S, Yip TW, Sangthong R. Workplace violence directed at nursing staff at a general hospital in Southern Thailand. J Occup Health. 2008;50:201–7. doi: 10.1539/joh.o7001. [DOI] [PubMed] [Google Scholar]
- 7.Lipscomb JA, El Ghaziri M. Workplace violence prevention: Improving front-line health-care worker and patient safety. New Solut. 2013;23:297–313. doi: 10.2190/NS.23.2.f. [DOI] [PubMed] [Google Scholar]
- 8.El-Gilany AH, El-Wehady A, Amr M. Violence against primary health care workers in Al-Hassa, Saudi Arabia. J Interpers Violence. 2010;25:716–34. doi: 10.1177/0886260509334395. [DOI] [PubMed] [Google Scholar]
- 9.Kitaneh M, Hamdan M. Workplace violence against physicians and nurses in Palestinian public hospitals: A cross-sectional study. BMC Health Serv Res. 2012;12:469. doi: 10.1186/1472-6963-12-469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hamdan M, Abu Hamra A. Workplace violence towards workers in the emergency departments of Palestinian hospitals: A cross-sectional study. Hum Resour Health. 2015;13:28. doi: 10.1186/s12960-015-0018-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Brown BG, Burns C. Hospital violence and the role of the occupational health nurse. Workplace Health Saf. 2013;61:475–8. doi: 10.1177/216507991306101103. [DOI] [PubMed] [Google Scholar]
- 12.Hegney D, Eley R, Plank A, Buikstra E, Parker V. Workplace violence in Queensland, Australia: The results of a comparative study. Int J Nurs Pract. 2006;12:220–31. doi: 10.1111/j.1440-172X.2006.00571.x. [DOI] [PubMed] [Google Scholar]
- 13.Farrell GA, Bobrowski C, Bobrowski P. Scoping workplace aggression in nursing: Findings from an Australian study. J Adv Nurs. 2006;55:778–87. doi: 10.1111/j.1365-2648.2006.03956.x. [DOI] [PubMed] [Google Scholar]
- 14.Opie T, Lenthall S, Dollard M, Wakerman J, MacLoad M, Knight S, et al. Trends in workplace violence in the remote area nursing workforce. Aust J Adv Nurs. 2005;27:18–23. [Google Scholar]
- 15.Zafar W, Siddiqui E, Ejaz K, Shehzad MU, Khan UR, Jamali S, et al. Health care personnel and workplace violence in the emergency departments of a volatile metropolis: Results from Karachi, Pakistan. J Emerg Med. 2013;45:761–72. doi: 10.1016/j.jemermed.2013.04.049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Abou-ElWafa HS, El-Gilany AH, Abd-El-Raouf SE, Abd-Elmouty SM, El-Sayed Rel-S. Workplace violence against emergency versus non-emergency nurses in Mansoura university hospitals, Egypt. J Interpers Violence. 2015;30:857–72. doi: 10.1177/0886260514536278. [DOI] [PubMed] [Google Scholar]
- 17.Roakes DK. Workplace Violence: Emergency Department versus Medical Surgical Nurses. Gardner-Webb University. Nursing Theses and Capstone Projects. 2012 [Google Scholar]
- 18.Gillespie GL, Gates DM, Miller M, Howard PK. Workplace violence in healthcare settings: Risk factors and protective strategies. Rehabil Nurs. 2010;35:177–84. doi: 10.1002/j.2048-7940.2010.tb00045.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kisa A, Dziegielewski SF, Ates M. Sexual harassment and its consequences: A study within Turkish hospitals. J Health Soc Policy. 2002;15:77–94. doi: 10.1300/J045v15n01_05. [DOI] [PubMed] [Google Scholar]