

Abstract
BACKGROUND:
With the increase in life expectancy, the number of older persons is constantly rising. Disability rates for elderly people are also on the rise with an increase in the burden of chronic diseases depriving them of independence and the performance of activities of daily living. The study aimed to estimate the prevalence of physical disability and determine its correlates among elderly population of rural Haryana.
MATERIALS AND METHODS:
A community-based cross-sectional study was conducted among 322 elderly participants aged 60 years and above in the rural area of Haryana, India. Data pertaining to sociodemographic profile, self-reported chronic diseases/ailments, and disability assessment by means of Barthel and Katz index of activities of daily living was collected and analyzed.
RESULTS:
Overall, 21.4% and 18% elderly people had some form of disability according to the Barthel index and Katz index, respectively. With aging, disability increased and 52.5% of the elderly aged 75 years and above were found to have disability according to the Barthel's index. Females (P = 0.014), those who were currently not married (P = 0.001), currently unemployed (P = 0.001), and those with chronic diseases/ailments (P = 0.002), had significantly higher disability rates. Binary logistic regression analysis revealed age 75 years and above, current unemployment, and the presence of three or more chronic diseases/ailments as significant factors related to physical disability.
CONCLUSION:
Disability is associated with increasing age and an increase in the burden of chronic health ailments in the elderly. Consequently, there is the need to prioritize preventive, promotive, curative, and rehabilitative services for the geriatric population.
Keywords: Activities of daily living, Barthel index, disability, elderly, Katz index
Introduction
The global demographic trend indicates an increase in life expectancy over decades as a result of social, economic, and public health development and advances in medical technologies creating a large aging population. The proportion of older persons is increasing rapidly in populations across the globe and the number of older persons, aged 60 years and above, is estimated to increase from 12.3% in 2015 to around 20% by 2050 worldwide.[1] In India, 8.9% of the population was aged 60 years and above in 2015, and this is estimated to reach 19.4% by 2050.[1]
An increase in the elderly population is associated with high prevalence of noncommunicable diseases and chronic conditions. Elderly people are at high risk for multiple comorbidities which results in higher disability rates in them.[2] Disability in simple terms implies restriction in the performance of normal activities of day-to-day life.[3] Disability makes a person dependent on others for support and care and also increases the burden on the health system. The most common causes of disability include chronic diseases such as diabetes, cancer, cardiovascular disease and stroke; injuries; mental impairment; birth defects; HIV/AIDS; and other communicable diseases.[4]
Disability can be assessed by measuring the individual's ability to perform activities of daily living (ADL) using instruments like Barthel or Katz index. Barthel index is a 10-item index and Katz index is a 6-item index of ADL for the assessment of disability.[5,6] Based on 10-item ADL index, the prevalence of physical disability in the elderly in various rural areas of India have been reported to be as low as 16.16% in West Bengal[7] and as high as 32.4% in Bengaluru.[8] The prevalence of disability using the same scale was estimated to be around 15% to 28.3% in studies conducted in other developed and developing countries.[9,10,11,12] The present study was carried out to estimate the prevalence of physical disability and its association with sociodemographic variables and health-related factors in elderly persons in a rural area of Haryana state of India.
Materials and Methods
A community-based cross-sectional study of 322 elderly persons aged 60 years and above was conducted for 6 months from July 2015 to December 2015. The study area comprised the rural field practice area (Barara) of Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana in the district Ambala of Haryana. Considering the 23.4% disability prevalence (using 10 item ADL Index) reported in a recent study from a rural area of Uttar Pradesh state of India,[13] we obtained a sample size of 315 participants at a relative precision of 20% (N = Z2p (1 − p)/(pd)2 where Z = 1.96, p is prevalence and d is relative precision or allowable error). Finally, 322 elderly participants aged 60 years and above were included in the study.
A list of all elderly aged 60 years and above was drawn from the field survey register of rural health and training center of the Institute, and 322 elderly participants were selected by the simple random sampling technique. We designed a semi-structured questionnaire and interviewed the study participants in house-to-house visits. Information was also obtained from close family members of those elderly who were unable to give the required details. The data were collected from the subjects after assurance of confidentiality of the data and obtaining informed written consent from them.
The information obtained from the study participants included questions pertaining to the sociodemographic factors and self-reported chronic diseases/ailments such as hypertension, diabetes mellitus, cataract, heart diseases, arthritis, chronic obstructive pulmonary symptoms, and hearing impairment. To assess physical disability, Barthel and Katz index which provide an objective measurement of the person's ability to perform ADL were used independently. Barthel index is a 10-item index that includes performance in feeding, bathing, dressing, grooming, toileting, bladder control, bowel control, transfer from bed to chair, walking, and stair climbing for disability assessment.[5] Katz index is a 6-item index that gives an assessment of the performance in the six functions of bathing, dressing, toileting, transferring, continence, and feeding.[6] For this study, physical disability was defined as needing help in one or more of these ADL activities. Socioeconomic status was determined with the help of updated BG Prasad socioeconomic classification scale,[14] which is based on per capita monthly income of the family and is commonly used in India to measure the socioeconomic status in both rural and urban areas. Ethical approval was obtained from the Institutional Ethics Committee of Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana, Ambala (Haryana).
The data obtained were analyzed by IBM SPSS Statistics for Windows, Version 20.0. (Armonk, New York: IBM Corp) and Chi-square test was applied to find the association between physical disability and the study variables. Crude odds ratios (ORs) with 95% confidence intervals were calculated. The study variables with P < 0.05 obtained from Chi-square analysis were entered into binary logistic regression analysis. Using “forward conditional method” of binary logistic regression, predictors of physical disability in elderly population with adjusted ORs were obtained.
Results
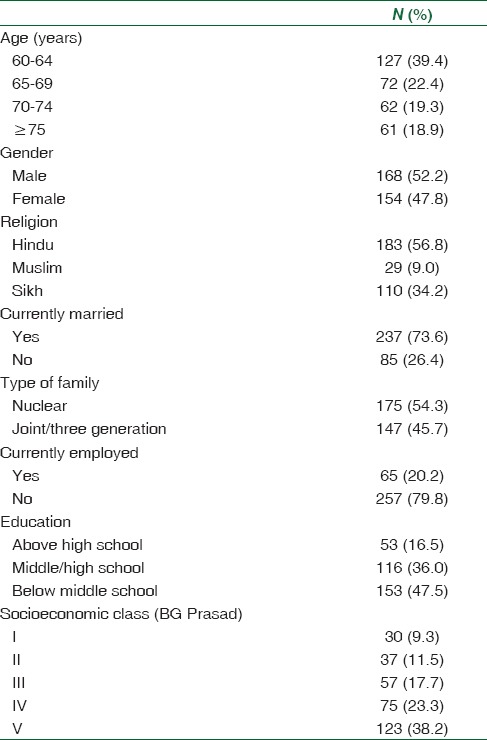
Of the 322 study participants, 39.4% (127) were aged 60–64 years and the distribution of participants in the remaining age groups was similar. With respect to gender (males 52.2% and females 47.8%) and type of family (nuclear 54.3% and joint/three generation 45.7%), participants were almost equally distributed. 73.6% and 20.2% of the participants were currently married and currently employed, respectively. The majority of the participants belonged to socioeconomic Class IV (23.3%) and Class V (38.2%) of BG Prasad socioeconomic classification [Table 1].
Table 1.
Sociodemographic characteristics of the study participants (n=322)
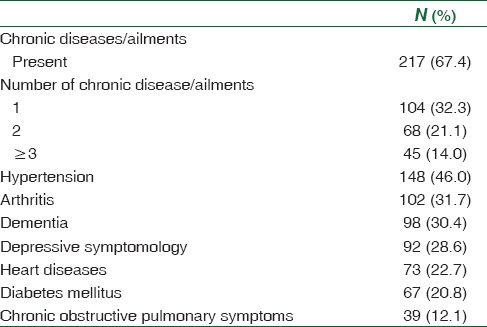
Around two thirds (67.4%) of the participants suffered from one or more chronic diseases/ailments. About 32.3% of the participants had one chronic disease/ailment, while 21.1% and 14% participants had two and three or more chronic diseases/ailments, respectively. The three most frequently reported chronic diseases were hypertension (46.0%), arthritis (31.7%), and cataract (30.4%) [Table 2].
Table 2.
Pattern of self-reported chronic diseases/ailments among study participants (n=322)
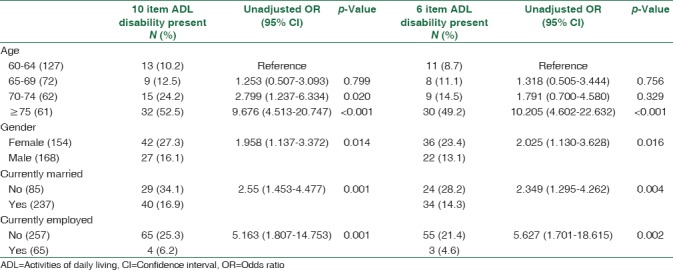
The prevalence of physical disability in the elderly population was 21.4% according to the 10-item ADL index (Barthel's index) and the same was estimated to be around 18% as per the 6-item ADL index (Katz index) [Table 3]. Disability increased significantly with an increase in the age of the participants. Around half of the participants aged 75 years and above had difficulty in performing 6- (52.5%) and 10-(49.2%) item ADL. Prevalence of disability was around two odds higher in females than males (OR of 1.958 and 2.025 by 10 and 6 item ADL index, respectively). Current marital and employment status were also significantly associated with ADL disability (P < 0.05) with both the scales [Table 4]. However, no significant association was observed between physical disability and other sociodemographic variables such as religion, literacy level, type of family, and socioeconomic status.
Table 3.
Prevalence of disability among study population according to 10-item and 6-item index of activities of daily living (n=322)
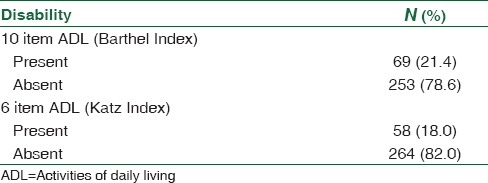
Table 4.
Statistically significant sociodemographic correlates of physical disability
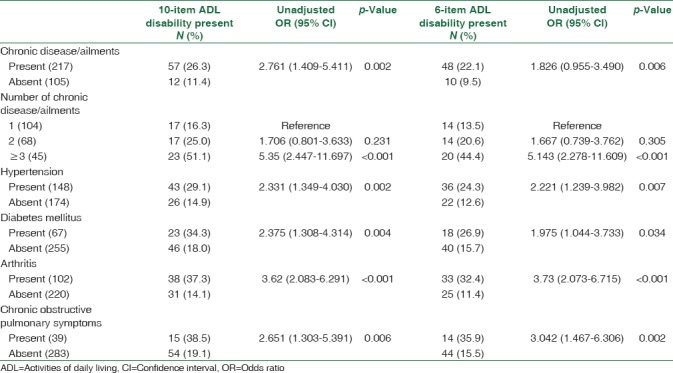
Participants with one or more self-reported chronic diseases/ailments had significantly higher disability rates compared to those who had none of the chronic diseases/ailments (10 item OR = 2.761, P = 0.002; 6 item OR = 1.826, P = 0.006). Around half of the participants (51.1% by 10-item ADL and 44.4% by 6-item ADL) with three or more chronic diseases reported some ADL disability. Moreover, chronic diseases/ailments such as hypertension, diabetes mellitus, arthritis, and chronic obstructive pulmonary symptoms were significantly (P < 0.05) associated with disability in the study participants [Table 5]. However, disability was not significantly associated with cataract, hearing impairment, and heart diseases.
Table 5.
Association between self-reported chronic diseases/ailments and physical disability among study participants
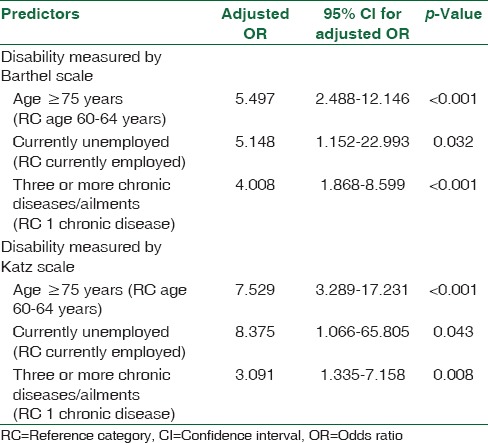
Binary logistic regression analysis for disability using both the ADL scales revealed that age 75 years or more (OR = 5.497, P < 0.001 by Barthel index and OR = 7.529, P < 0.001 by Katz index), current unemployment (OR = 5.148, P = 0.032 by Barthel index and OR = 8.375, P = 0.043 by Katz index), and the presence of three or more chronic diseases/ailments (OR = 4.008, P < 0.001 by Barthel index and OR = 3.091, P = 0.008 by Katz index) were the statistically significant predictors of physical disability in the study participants [Table 6].
Table 6.
Logistic regression analysis: Factors related to physical disability among elderly
Discussion
In the present cross-sectional study conducted in a rural area of Haryana, the prevalence of physical disability in elderly people aged 60 years and above, assessed with the 10-item index of ADL (Barthel index) was 21.4%. Using the same index, a disability prevalence of 22% and 23.4% was reported in studies of some rural areas of two other states of India, Tamil Nadu[15] and Uttar Pradesh,[13] respectively. Other rural community-based studies using the 10-item ADL index found a disability prevalence of 16.16% in the state of West Bengal,[7]17.6% in Haryana,[16] and a much higher prevalence of 32.4% in a study from Bengaluru city in the Karnataka state of India.[8] The prevalence of 10 item ADL disability in the Indian studies is comparable to findings from studies conducted in other countries such as 15% in USA,[9]20% in Japan,[10]24.7% in Malaysia,[11] and 28.3% in Nigeria.[12]
Using the 6-item index of ADL (Katz index), 18% of elderly subjects were found to have difficulty in performing one or more of the 6 ADLs. Two studies conducted in rural areas of Malaysia and Nigeria reported 6-item ADL disabilities in 14.4% and 15.7% elderly participants, respectively.[11,12] However, based on the same Katz index of ADL, a study in Dubai, UAE, revealed a higher prevalence of ADL disability of 27.5%,[17] which may be due to the inclusion of participants above 65 years of age.
Physical disability increased significantly with the increasing age of participants; the same has been reported consistently in the previous studies.[7,8,9,10,11,12,13,15,16,17,18] More than half (52.5%) of the elderly aged 75 years and above were physically disabled as per 10 item ADL index. Studies conducted in Malaysia and Nigeria also reported 10 item ADL disability in 49.6% and 50.5% of the elderly aged 75 years and above, respectively.[11,12] Effect of gender on physical disability revealed that females were significantly more disabled than men, which is in accordance with findings from various studies conducted in India and elsewhere.[10,11,12,13,15,16,18] This gender difference in disability of the elderly may be attributed to the fact that women tend to have higher survival rates for various diseases and have less severe underlying comorbidity than men.[19,20] Further, there may be a greater influence of musculoskeletal problems on functional limitations in females than males as women who have musculoskeletal diseases have been found to have relatively greater physical disability than men.[21]
ADL disability rates were significantly lower in ‘currently married’ elderly than those whose marital status was ‘not married’, which is consistent with findings of many studies.[9,10,11,12,16] In the present study, we found significantly higher disability rates in participants who were currently unemployed compared to those who had employment. This is also supported by findings from previous studies.[10,16]
The presence of chronic diseases/ailments in the participants was associated with disability, which became more severe with an increase in the number of chronic diseases/ailments the participants had. More than half (51.1%) of the elderly suffering from three or more chronic diseases/ailments were disabled. Previous studies also revealed that there were more disabilities in the elderly who had more than one chronic disease and the rates of disability increased with an increase in the number of chronic diseases.[11,12] In the present study, disability was significantly associated with chronic health ailments such as hypertension, diabetes, arthritis, and chronic obstructive pulmonary symptoms. Previous studies have also reported significant association of disability with hypertension,[22] diabetes,[10,11,12] arthritis,[7,9,10,11,12] and chronic obstructive pulmonary disease.[7,9,16]
A binary logistic regression analysis was carried out to determine independent predictors of disability in the present study. The analysis revealed that age 75 years and above, current unemployment, and presence of three or more chronic diseases/ailments were significantly associated with physical disability in ADL of the elderly participants. Increasing age is one of the strongest independent risk factors for disability as shown in binary logistic regression analysis in previous studies.[7,9,10,11,12] Although age is a nonmodifiable risk factor for physical disability, prevention and control of chronic diseases may reduce the burden of physical disability in the elderly population. Thus, there is a need to prioritize the implementation of various national programs and policies for the prevention of chronic diseases and focus on preventive, promotive, curative, and rehabilitative services for the geriatric population.
Conclusion
One in every five elderly persons aged 60 years and above and one out of two elderly aged 75 years and above are disabled. Increasing age and multiple comorbidities are independently associated with higher disability rates. Owing to the rapid increase in our aging population, there is a need to emphasize the primary preventive measures and early diagnosis and treatment of chronic diseases, particularly associated with physical disability. Functional assessment of the elderly provides objective data to evaluate their health status, and give an indication of its future improvement or decline that may necessitate intervention.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.United Nations, Department of Economic and Social Affairs, Population Division. World Population Ageing 2015 (ST/ESA/SER.A/390) 2015. [Last accessed on 2017 Sep 19]. Available from: http://www.un.org/en/development/desa/population/./pdf/ageing/WPA2015_Report.pdf .
- 2.Gijsen R, Hoeymans N, Schellevis FG, Ruwaard D, Satariano WA, van den Bos GA, et al. Causes and consequences of comorbidity: A review. J Clin Epidemiol. 2001;54:661–74. doi: 10.1016/s0895-4356(00)00363-2. [DOI] [PubMed] [Google Scholar]
- 3.Verbrugge LM, Jette AM. The disablement process. Soc Sci Med. 1994;38:1–4. doi: 10.1016/0277-9536(94)90294-1. [DOI] [PubMed] [Google Scholar]
- 4.Disability and Rehabilitation. WHO Action Plan 2006-2011. [Last accessed on 2017 Oct 17]. Available from: http://www.who.int/entity/disabilities/publications/dar_action_plan_2006to2011.pdf?ua=1 .
- 5.Wade DT, Collin C. The Barthel ADL Index: A standard measure of physical disability? Disabil Rehabil. 1988;10:64–7. doi: 10.3109/09638288809164105. [DOI] [PubMed] [Google Scholar]
- 6.Katz S, Downs TD, Cash HR, Grotz RC. Progress in development of the index of ADL. Gerontologist. 1970;10:20–30. doi: 10.1093/geront/10.1_part_1.20. [DOI] [PubMed] [Google Scholar]
- 7.Chakrabarty D, Mandal PK, Manna N, Mallik S, Ghosh P, Chatterjee C, et al. Functional disability and associated chronic conditions among geriatric populations in a rural community of India. Ghana Med J. 2010;44:150–4. doi: 10.4314/gmj.v44i4.68913. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Deepthi R, Kasthuri A. Visual and hearing impairment among rural elderly of South India: A community-based study. Geriatr Gerontol Int. 2012;12:116–22. doi: 10.1111/j.1447-0594.2011.00720.x. [DOI] [PubMed] [Google Scholar]
- 9.Chaudhry SI, McAvay G, Ning Y, Allore HG, Newman AB, Gill TM, et al. Geriatric impairments and disability: The cardiovascular health study. J Am Geriatr Soc. 2010;58:1686–92. doi: 10.1111/j.1532-5415.2010.03022.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Yoshida D, Ninomiya T, Doi Y, Hata J, Fukuhara M, Ikeda F, et al. Prevalence and causes of functional disability in an elderly general population of Japanese: The Hisayama study. J Epidemiol. 2012;22:222–9. doi: 10.2188/jea.JE20110083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hairi NN, Bulgiba A, Cumming RG, Naganathan V, Mudla I. Prevalence and correlates of physical disability and functional limitation among community-dwelling older people in rural Malaysia, a middle-income country. BMC Public Health. 2010;10:492. doi: 10.1186/1471-2458-10-492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Abdulraheem IS, Oladipo AR, Amodu MO. Prevalence and correlates of physical disability and functional limitation among elderly rural population in Nigeria. J Aging Res. 2011;2011:369894. doi: 10.4061/2011/369894. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Gupta S, Yadav R, Malhotra AK. Assessment of physical disability using Barthel index among elderly of rural areas of district Jhansi (U.P), India. J Family Med Prim Care. 2016;5:853–7. doi: 10.4103/2249-4863.201178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Mangal A, Kumar V, Panesar S, Talwar R, Raut D, Singh S, et al. Updated BG prasad socioeconomic classification, 2014: A commentary. Indian J Public Health. 2015;59:42–4. doi: 10.4103/0019-557X.152859. [DOI] [PubMed] [Google Scholar]
- 15.Venkatorao T, Ezhil R, Jabbar S, Ramakrishnan R. Prevalence of disability and handicaps in geriatric population in rural South India. Indian J Public Health. 2005;49:11–7. [PubMed] [Google Scholar]
- 16.Gupta P, Mani K, Rai SK, Nongkynrih B, Gupta SK. Functional disability among elderly persons in a rural area of Haryana. Indian J Public Health. 2014;58:11–6. doi: 10.4103/0019-557X.128155. [DOI] [PubMed] [Google Scholar]
- 17.Al Yousef NJ, Hussein H, Al Faisal W, Makhlouf MM, Wasfy A. Prevalence of functional disabilities and sources of care provided for elderly patients population in Dubai, UAE. Adv Appl Psychol. 2015;1:6–9. [Google Scholar]
- 18.Wandera SO, Ntozi J, Kwagala B. Prevalence and correlates of disability among older Ugandans: Evidence from the Uganda National Household Survey. Glob Health Action. 2014;7:25686. doi: 10.3402/gha.v7.25686. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Guralnik JM, Kaplan GA. Predictors of healthy aging: Prospective evidence from the Alameda county study. Am J Public Health. 1989;79:703–8. doi: 10.2105/ajph.79.6.703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Oman D, Reed D, Ferrara A. Do elderly women have more physical disability than men do? Am J Epidemiol. 1999;150:834–42. doi: 10.1093/oxfordjournals.aje.a010088. [DOI] [PubMed] [Google Scholar]
- 21.Wray LA, Blaum CS. Explaining the role of sex on disability: A population-based study. Gerontologist. 2001;41:499–510. doi: 10.1093/geront/41.4.499. [DOI] [PubMed] [Google Scholar]
- 22.Hajjar I, Lackland DT, Cupples LA, Lipsitz LA. Association between concurrent and remote blood pressure and disability in older adults. Hypertension. 2007;50:1026–32. doi: 10.1161/HYPERTENSIONAHA.107.097667. [DOI] [PMC free article] [PubMed] [Google Scholar]