

Abstract
Early life adversity, ranging from material deprivation and parental dysfunction to abusive and life-threatening events, has been associated with hoarding symptom severity. Moreover, both victims of early life adversity and individuals with hoarding disorder have been found to have a higher tendency toward detail-oriented visual processing. This study aimed to investigate the role of detail-oriented visual processing in the relationship between early life adversity and hoarding-related dysfunction. Childhood exposure to life adversity, hoarding symptom severity, and emotional attachment to possessions, a hoarding-related dysfunction thought to be most closely related to adversity exposure, were assessed. Detail-oriented visual processing was evaluated using the Central Coherence Index, which was calculated based on the drawing process during the Rey-Osterrieth Complex Figure Test. It was found that detail-oriented visual processing was not significantly associated with hoarding symptom severity, emotional attachment to possessions, or the relationship between early life adversity and hoarding symptom severity. It did, however, act as a significant moderator in the relationship between early life adversity and emotional attachment to possessions. These findings add to the literature by identifying the role of a specific neurocognitive processing style in the mechanism through which early life adversity affects the development of a key hoarding-related dysfunction, elevated emotional attachment to possessions.
Keywords: hoarding, early life adversity, visual processing style
1. Introduction
The core features of hoarding disorder (HD) include persistent difficulty discarding possessions, due to perceived need to save them and distress associated with discarding them, leading to the accumulation of excessive amounts of clutter (American Psychiatric Association, 2013). The cognitive-behavior model of compulsive hoarding (Frost and Hartl, 1996), which depicts HD as a multifaceted problem, identifies four areas of hoarding-related dysfunction that underlie the clinical presentation of HD. They are: 1) abnormal emotional attachment to possessions, 2) dysfunction in information processing, 3) abnormal beliefs about possessions, and 4) avoidance.
In examining potential environmental contributors to hoarding, experiences of life adversity, ranging from major life stressors such as parental dysfunction and disruption of interpersonal relationships to traumas such as physical and sexual assaults, have been found to be associated with hoarding symptom severity (Ayers et al., 2010; Dozier et al., 2016; Hartl et al., 2005; Landau et al., 2011; Przeworski et al., 2014; Timpano et al., 2011; Tolin et al., 2010). Moreover, life adversity has been associated with one of the four proposed areas of hoarding related dysfunctions, emotional attachment to possessions. Specifically, it has been suggested that, for individuals whose safety has been compromised, emotional attachment to possessions may develop as a way to gain a sense of protection and safety (Hartl et al., 2005). This hypothesized relationship between life adversity and emotional attachment to possessions awaits empirical investigation. In addition, potential factors affecting the proposed relationships between life adversity and both emotional attachment to possessions and hoarding symptom severity have not yet been explored.
To identify potential moderators of the effects of life adversity on hoarding related symptoms and cognitions, we reviewed the literature for another psychiatric illness that is the direct result of an extreme form of life adversity (i.e., trauma), posttraumatic stress disorder (PTSD). In PTSD, the tendency to vividly retain the visual details rather than an integrated global impression or personal meaning of a trauma has been suggested as a risk factor for the development of PTSD symptoms (Bisby et al., 2009; Brewin et al., 2010; Hagenaars et al., 2016). A similar bias towards retaining detailed and local over contextual and global information has also been found among individuals with HD: in performing a sorting task, individuals with HD more often consider detailed features of objects compared to healthy controls (Frost and Hartl, 1996; Grisham et al., 2010; Wincze et al., 2007). While this detail-oriented visual processing style is associated with more severe psychological consequences of trauma among individuals with PTSD, its effect on the relationship between trauma and hoarding has not yet been examined. It is possible that the tendency to focus on details rather than on global impressions predisposes individuals to see each object as unique, thereby intensifying the emotional attachment toward the item, and thus, the behavioral symptoms of hoarding (i.e., difficulty discarding and obsessive acquisition).
One of the most widely used assessment tools for visual processing is the Rey-Osterrieth Complex Figure Test (RCFT; Osterrieth, 1944). In studies examining visual processing using the RCFT, poorer performance has been associated with both life adversity and hoarding. For example, trauma victims consistently copied the complex figure less accurately than those who had not reported significant traumatic experiences (Stein et al., 2002). Similarly, individuals with HD are less successful in constructing the complex figure, missing key component parts or creating more fragmented copies in comparison to healthy individuals during the copying stage (Hartl et al., 2004; Tolin et al., 2011). In sum, the bias towards local and detailed information over global and integrated information, at least in some contexts, has been observed in both trauma victims and hoarding populations, as has poorer accuracy in visual information processing as manifested by performance on the RCFT. However, the potential effect of detail-oriented visual processing on the relationship between life adversity and hoarding has not yet been examined.
In this study, we examined the relationships between life adversity, hoarding symptoms, and visual processing style in individuals with HD and in healthy controls. We hypothesized that detail-orientated visual processing styles would significantly moderate the relationship between frequent exposure to life adversity and more severe hoarding symptoms (e.g., Cromer et al., 2007; Hartl et al., 2005; Landau et al., 2011; Przeworski et al., 2014; Tolin et al., 2010). We also hypothesized, based on the previous literature (Hartl et al., 2005), that we would find a significant relationship between life adversity and emotional attachment to possessions, and that detail-orientation visual processing style would significantly enhance the strength of this relationship. As an initial exploration of this topic, we focused on relationship-related life adversities in childhood (i.e., before age 18), since early exposure to relationship-related adversities, as opposed to other types of adverse experiences such as natural disasters and material deprivation, have been associated more negative outcomes, in both the contexts of PTSD and HD, and in the context of neurological development (Landau et al., 2011; Maughan and McCarthy, 1997; Penza et al., 2003; Tomalski and Johnson, 2010).
2. Methods
2.1. Participants
The participants for this study included 24 individuals with HD (16.7% male, age range 20 to 74) and 40 healthy individuals (40.0% male, age range 19 to 78), who were recruited for a larger study aimed at examining neurocognitive function in HD. Participants were recruited through media advertisements and health clinics throughout the San Francisco Bay Area. HD participants were included if they met DSM-5 criteria for HD (American Psychiatric Association, 2013), plus two out of three of the following: 1) a score of ≥ 40 on the Saving Inventory, Revised (SI-R) (Frost et al., 2004), 2) a score of ≥ 20 on the UCLA Hoarding Symptom Scale (UHSS) (Saxena et al., 2015), and 3) a score of ≥ 12 on the Clutter Image Rating Scale-Revised (CI-R) (Frost et al., 2008). HD participants were not excluded on the basis of co-occurring psychiatric disorders, with the exceptions noted below. Healthy participants were included if they did not meet DSM-5 criteria for a current Axis I disorder including HD, and met at least two of the following: 1) a score of ≤ 20 on the SI-R, 2) a score of ≤ 10 on the UHSS, and 3) a score of ≤ 8 on the CI-R. Regardless of diagnosis status, individuals with active psychotic symptoms, intellectual disability, dementia, or any acute medical condition that is known or suspected to affect cognitive function (including, but not limited to, head trauma) were excluded. Participants with a history of substance use were required to be sober from all substances (except tobacco) for three months prior to participation in the study.
2.2. Diagnostic interviews
The Structured Interview for Hoarding Disorder (SIHD) (Nordsletten, 2013) was utilized to assign HD diagnosis. Other psychiatric symptoms were assessed using the Structured Clinical Interview for Diagnosis of DSM disorders (SCID) (First et al., 1997).
2.3. Clinical assessments
The Saving Inventory, Revised (SI-R) (Frost et al., 2004) was used to assess overall hoarding severity. The Possession Comfort Scale (PCS) (Hartl et al., 2005) was used to assess emotional attachment to possessions. The PCS is a 31-item scale assessing various aspects pertaining to emotionality in relation to possessions. These aspects include physical and emotional comfort, vulnerability and loneliness. Responses are made on a 1 (strongly disagree) to 7 (strongly agree) scale with higher scores indicating stronger emotional attachment to possessions. Finally, the Beck Depression Inventory-Second Edition (BDI-II) (Beck et al., 1996) and Beck Anxiety Inventory (BAI) (Steer et al., 1993) were used to assess depression and anxiety symptoms respectively. Satisfactory internal consistency within the current sample was found for these measures (Cronbach’s Alpha = 0.98 for SI-R, 0.97 for PCS, 0.93 for BDI-II, and 0.96 for BAI).
2.4. Early life adversity
The Adverse Childhood Experience Questionnaire (ACE) (Felitti et al., 1998; McGavock and Spratt, 2014) was used to assess cumulative exposure to 10 types of early life adversity, including childhood abuse (i.e., verbal, physical, or sexual abuse), neglect (i.e., deprivation of food, attention, or other types of resources), and household dysfunction (i.e., parental divorce, mental illnesses, substance abuse, or imprisonment). The total scores range from 0 to 10. Scores of 4 or higher have been found to be significantly associated with a variety of negative mental health outcomes, psychophysiological and psychosocial vulnerabilities (e.g., Anda et al., 2010; Chapman et al., 2007; Chapman et al., 2011; Dube et al., 2009).
2.5. Visual-spatial Processing
The Rey-Osterrieth Complex Figure Test (RCFT) (Osterrieth, 1944) was used to assess the accuracy and style of visual-spatial processing. The accuracy score (range 0-36) was rated based on the quality of drawings of 18 elements in the complex figure. In order to assess visual-spatial processing style, Booth’s method (Booth, 2006) was adopted to evaluate whether the drawing process was detail- or globally-oriented. In this method, first, the order of construct index (OCI; ranges between 0 and 3.3.) is calculated by awarding a score of 0, 1, 3, or 4 to the first 6 elements drawn based on the hierarchical categories to which they belong, and averaging the sum. A higher score in the OCI indicates a greater involvement of global, as opposed to detailed, features at the initial stage of visual processing. Second, the style index (SI; ranges between 0 and 2) is derived by awarding a 0 to 2 score to the first 6 elements drawn based on the degree of continuity and averaging the sum. A higher score on the SI indicates greater continuity in the drawing style. Finally, the central coherence index (CCI; ranges between 0 and 2) was obtained by adding the proportion of the total possible scores in OCI (score/3.3) and SI (score/2). The CCI was used to indicate the style of visual-spatial processing, with a lower score meaning a more detail-oriented style, and a higher score meaning a more global-oriented style.
2.6. Other measures
To account for the potential contribution of general cognitive function on the effect of visual processing style in predicting the dependent measures, the National Adult Reading Test (NART) (Nelson, 1982; Nelson and Willison, 1991) was utilized to estimate the full scale intelligence quotient (IQ).
2.7. Procedures
The study took place at University of California, San Francisco (UCSF), and was approved by the UCSF Institutional Review Board. Self-report questionnaires, the SI-R (Frost et al., 2004), UHSS (Saxena et al., 2015), and CI-R (Frost et al., 2008), and clinical interviews with a licensed psychologist or psychiatrist were conducted to determine eligibility. Next, participants completed clinical assessment and assessment of early life adversity, followed by a battery of neuropsychological tests with trained research staff who were blinded to participants’ clinical diagnosis. All participants provided verbal and written informed consent to participate in the study and were financially compensated for their participation ($20 per hour).
2.8. Statistical Analyses
All statistical analyses were performed with SPSS version 21 (SPSS Inc, Chicago, IL, USA). For each continuous variable, the approximation of normal distribution was examined and established using methods applied in previous studies (Chou et al., 2014). Specifically, when the skewness score of a continuous variable was 3 times larger than the standard error of the skewness score, the variable would be determined to be significantly skewed, and a square-root transformation would be applied. A square-root transformation was applied to the following variables: frequency of early life adversity, depression and anxiety symptom scores, detail-oriented visual processing style (i.e., CCI score), and visual processing accuracy (i.e., RCFT accuracy score).
Pearson’s correlations were conducted to examine the relationships between the key variables (i.e., early life adversity, detail-oriented visual processing style, visual processing accuracy, overall hoarding severity, and emotional attachment to possessions. Two linear regression models were then examined in the entire sample. The first model examined the moderating effect of detail-oriented visual processing style on the relationship between early life adversity and overall hoarding symptom severity, with the latter being the dependent variable. The second model examined the moderating effect of detail-oriented visual processing style on the relationship between early life adversity and emotional attachment to possessions, with the latter being the dependent variable. In both models, the main predictors included early life adversity, detail-oriented visual processing style, and the interaction term of the two. Basic demographic variables (i.e., gender and age) were included as covariates in the regression models. Moreover, to account for potential confounding effect of general cognitive capacity on visual processing style, full IQ as estimated by the NART was included as a covariate. Similarly, since symptoms of anxiety and depression have been associated with early life adversity (Young et al., 1997), BAI (Steer et al., 1993) and BDI (Beck et al., 1996) scores were also included as covariates. As exploratory analyses, Pearson’s correlations were used to examine the correlations between these covariates and the dependent variables, hoarding symptom severity and emotional attachment to possessions, in this study sample. Moreover, when a significant moderating effect of detail-oriented visual processing style was found in the regression models, post hoc Pearson’s correlations between early life adversity and the hoarding measures (e.g., hoarding symptom severity or emotional attachment to possessions) were computed separately among those with higher versus those with lower detail-oriented visual processing tendency (defined by mid-split) in order to clarify the moderating effect. The two correlation coefficients were then transformed into z scores using the Fisher Z-transformation to examine whether the difference between them was statistically significant.
3. Results
Descriptive data of the entire sample, as well as that of the HD and health sub-samples are summarized in Table 1. As shown in Table 1, individuals in the HD sub-sample were significantly older, showed higher IQ scores, greater severity in the clinical measures, and more experiences of early life adversities. Gender distribution between the healthy (40% male) and HD participants (17% male) showed a trend towards significance (χ2(1) = 3.80, p = 0.051). There were no significant differences in detail-oriented visual processing tendency or accuracy in visual processing between the healthy and HD participants. Current co-occurring psychiatric disorders among those with HD included social phobia (n = 5), major depressive disorder (n = 4), generalized anxiety disorder (n = 3), specific phobia (n = 3), PTSD (n = 2), and bulimia nervosa (n = 1).
Table 1.
Descriptive data for the entire sample and comparison by group
| Overall (N=64) | Hoarding (n=24) | Healthy (n=40) | |||||
|---|---|---|---|---|---|---|---|
|
| |||||||
| M | SD | M | SD | M | SD | ||
|
|
|||||||
| Age | 49.33 | 15.43 | 54.21 | 11.91 | 46.40 | 16.66 | t(60) = 2.18, p = 0.033 |
| IQ | 116.28i | 6.52i | 118.49 | 4.80 | 114.85i | 7.13i | t(59) = 2.19, p = 0.032 |
| Overall hoarding severitya | 26.41j | 24.05j | 53.38 | 14.36 | 9.82j | 8.78j | t(61) = 14.97, p < 0.001 |
| Emotional attachment to possessionsb | 69.00 | 35.28 | 96.13 | 36.17 | 52.70 | 22.66 | t(62) = 5.92, p < 0.001 |
| Anxiety levelc | 5.20 | 6.75 | 10.21 | 8.36 | 2.20 | 2.80 | t(62) = 5.01, p < 0.001 |
| Depression leveld | 6.36 | 10.65 | 13.92 | 14.01 | 1.83 | 3.34 | t(62) = 5.24, p < 0.001 |
| Early life adversitye | 1.84 | 2.20 | 3.45h | 2.48h | 0.95 | 1.40 | t(60) = 4.97, p < 0.001 |
| Accuracy in visual processingf | 33.95 | 4.07 | 33.56 | 5.14 | 34.19 | 3.32 | t(62) = −0.43, p = 0.666 |
| Detail-oriented visual processing styleg | 1.45 | 0.31 | 1.42 | 0.40 | 1.48 | 0.24 | t(62) = −0.54, p = 0.592 |
Saving Inventory, Revised scores;
Possession Comfort Scale scores;
Beck Anxiety Inventory scores;
Beck Depression Inventory scores;
Adverse Childhood Experience scores;
RCFT accuracy scores;
RCFT Central Coherence Index score, smaller number represent a more detail-oriented visual processing style;
data from 2 participants were missing;
data from 3 participants were missing;
data from 1 participant were missing
Note. All data in this table are non-transformed data.
In the combined sample, more frequent exposure to early life adversity was significantly correlated with both more severe hoarding symptoms (r = 0.50, p < 0.001), and stronger emotional attachment to possessions (r = 0.38, p = 0.003). Frequent exposure to early life adversity was also significantly correlated with more detail-oriented visual processing style (i.e., lower CCI score; r = −0.36, p = 0.004). However, detail-oriented visual processing style was not significantly correlated with hoarding symptom severity (r = −0.08, p = 0.520) or emotional attachment to possessions (r = 0.17, p = 0.183). Additionally, the two measures of visual processing (i.e., detail-oriented style and accuracy) were significantly and positively correlated (r = 0.32, p = 0.011).
The results from the regression analyses are shown in Tables 2 and 3. The first model predicting hoarding symptom severity accounted for 58% of the variance (F(8, 49) = 8.50, p < 0.001). Depression symptom severity (p = 0.001) were the only significant predictors of hoarding symptom severity (Table 2). The second model predicting emotional attachment to possessions accounted for 48% of the variance (F(8, 50) = 5.84, p < 0.001). Depression symptom severity (p = 0.034), and the interaction between early life adversity and detail-oriented visual processing style (p = 0.031) were significant predictors of emotional attachment to possessions, suggesting a significant moderating effect of detail-oriented visual processing style (Table 3). Exploratory analyses showed that most of the covariates were significantly correlated with the dependent variable in each of the two regression models (Table 4). Moreover, to clarify the moderating effect found in the second regression model, post hoc Pearson’s correlations were applied. As shown in Figure 1, there was a significant and positive correlation between early life adversity and emotional attachment to possessions among those with greater detail-oriented visual processing tendency (r = 0.44, p = 0.011), but not among those with lower detail-oriented visual processing tendency (r = 0.34, p = 0.073). However, the difference between the two correlation coefficients were not statistically significant (p = 0.33).
Table 2.
Regression model predicting overall hoarding symptom severity
| Standardized coefficients | |||
|---|---|---|---|
|
| |||
| β | t | p | |
| Age | 0.07 | 0.61 | 0.546 |
| Gender | 0.21 | 2.01 | 0.050 |
| IQ | 0.17 | 1.54 | 0.129 |
| Anxiety level | 0.12 | 0.87 | 0.386 |
| Depression level | 0.45** | 3.45 | 0.001 |
| Early life adversity | 0.77 | 1.71 | 0.093 |
| Detail-oriented visual processing style | 0.15 | 1.08 | 0.286 |
| Early life adversity × Detail-oriented visual processing style | −0.58 | −1.39 | 0.170 |
p < 0.01
Table 3.
Regression model predicting emotional attachment to possessions
| Standardized coefficients | |||
|---|---|---|---|
|
| |||
| β | t | p | |
| Age | −0.08 | −0.66 | 0.513 |
| Gender | 0.15 | 1.33 | 0.189 |
| IQ | 0.21 | 1.77 | 0.082 |
| Anxiety level | 0.21 | 1.44 | 0.155 |
| Depression level | 0.31 | 2.18 | 0.034 |
| Early life adversity | −0.82 | −1.67 | 0.101 |
| Detail-oriented visual processing style | 0.03 | 0.19 | 0.853 |
| Early life adversity × Detail-oriented visual processing style | 1.02* | 2.23 | 0.031 |
p < 0.05
Table 4.
Correlation coefficients between dependent variables and covariates in regression models
| Covariates | Dependent variable: first model Hoarding symptom severity | Dependent variable: second model Emotional attachment to possessions | ||||
|---|---|---|---|---|---|---|
|
| ||||||
| n | r | p | n | r | p | |
| Age | 63 | 0.25 | 0.053 | 64 | 0.15 | 0.242 |
| Gender | 63 | 0.33** | 0.008 | 64 | 0.23 | 0.068 |
| IQ | 60 | 0.29* | 0.028 | 61 | 0.21 | 0.097 |
| Anxiety level | 63 | 0.58*** | <0.001 | 64 | 0.47*** | <0.001 |
| Depression level | 63 | 0.59*** | <0.001 | 217 | 0.06*** | <0.001 |
p <0.05,
p <0.01,
p <0.001
Figure 1.
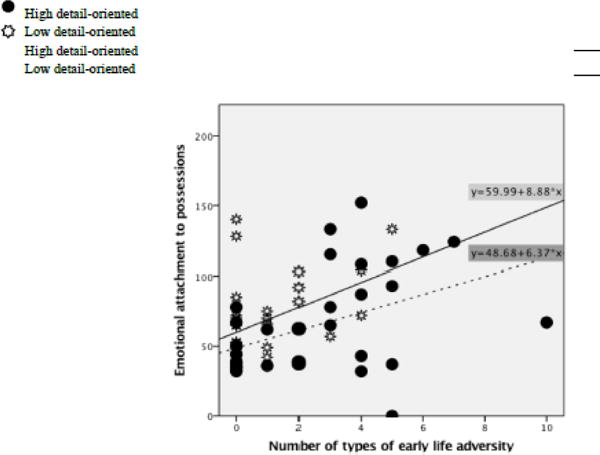
Associations between early life adversity and emotional attachment to possessions by level of detail-oriented visual processing style
Note. The dots. ● and ☼, represent data points of individuals with high vs low detail-oriented visual processing style, respectively: whereas the solid and dashed lines represent the line of best fit for the data points of those with high vs. low detail-oriented visual processing style, respectively
4. Discussion
Exposure to life adversity or trauma has been associated with more severe hoarding symptoms (Ayers et al., 2010; Dozier et al., 2016; Hartl et al., 2005; Landau et al., 2011; Przeworski et al., 2014; Timpano et al., 2011; Tolin et al., 2010), and hypothesized to be associated with the development of excessive emotional attachment to possessions, one of the core dysfunctions related to hoarding (Hartl et al., 2005). The current study examined the relationships between adversity occurred in childhood, overall hoarding symptom severity, and emotional attachment to possessions. More specifically, we were interested in whether detail-oriented visual processing style, a neurocognitive vulnerability for the development of posttraumatic symptoms following trauma (Bisby et al., 2009; Brewin et al., 2010), would moderate the effect of early life adversity on these hoarding-related measures.
First, we found that individuals with HD reported significantly more types of adversity in childhood than the healthy participants. Moreover, in the entire sample, more frequent exposure to early life adversity was significantly associated with worse current hoarding severity and stronger emotional attachment to possessions. These findings are consistent with the literature suggesting life adversity as a risk factor for HD (Ayers et al., 2010; Dozier et al., 2016; Hartl et al., 2005; Landau et al., 2011; Przeworski et al., 2014; Timpano et al., 2011; Tolin et al., 2010). They also support the hypothesized association between life adversity and emotional attachment to possessions (Hartl et al., 2005).
Second, consistent with findings in the previous study (Hartl et al., 2004), there was no significant difference in the accuracy scores for copying the complex figure in the RCFT (Osterrieth, 1944) between the healthy and HD participants. That is, individuals with HD have similar capacity to attend to and construct a copy of complex visual stimuli compared to healthy individuals. However, inconsistent results have been found when examination is focused more closely on the key or global components of the figure. Specifically, previous work had shown that individuals with HD tended to miss or create more fragmented copies of the key components in RCFT (Hartl et al., 2004; Tolin et al., 2011). In contrast, the current study found that there was no significant difference between healthy individuals and those with HD in detail-oriented visual processing style. The diverse findings may be due to differences in the measure examined in these studies vs. that examined in the current study. Specifically, the measure used in the previous work evaluated overall performance on copying key components of the figure, regardless of the order of construction (Savage et al., 1999). However, detail-oriented visual processing style (Booth, 2006) assessed “what the first six components are that draw one’s attention as well as one’s capacity is to accurately and smoothly copy them”. It is possible that individuals with HD do not have significant difficulties in identifying the global and key features of a complex visual stimulus in the early stage of visual processing, hence do not show a greater tendency of detail-oriented visual processing. However, their overall capacity to construct and complete the copying of the key components may be compromised as suggeste by previous findings (Hartl et al., 2004; Tolin et al., 2011). It would be of interest to examine factors that may contribute to this phenomena, and whether the compromised performance is more reflected among the global or key features than the more local and detailed features of the RCFT image.
On the other hand, regardless of hoarding tendencies, frequent exposure to early life adversity was found to be associated with detail-oriented visual processing style. That is, instead of capturing elements that compose the fundamental structure of an image, individuals who had experienced more adversities in early life tended to be drawn to the details in the initial stage of visual processing. The contrast between this finding and the nonsignificant relationship between visual processing style and the hoarding measures suggests a stronger association between detail-oriented visual processing style and early life adversity than hoarding symptoms or emotional attachment to possessions. In other words, detail-oriented visual processing style, by itself, may not be significantly influential to the symptom severity of HD or to emotional attachment to possessions which has been associated with HD. Its impact on hoarding, if any, would be indirect and likely to stem from its association with early life adversity.
Consistently, and supporting our original hypothesis, detail-oriented visual processing style did significantly moderate the relationship between early life adversity and emotional attachment to possessions. It is possible that the tendency to attend to detailed components of objects strengthens the perception and/or belief that each and every object is unique and irreplaceable, which is a common cognitive distortion of HD (Frost and Hartl, 1996), and thereby intensifies the existing strong association between early life adversity and emotional attachment to possessions. Based on findings in the regression model, the significance of this moderating effect on emotional attachment to possessions was stronger than early life adversity or detail-oriented visual processing style. In other words, when the experience of early life adversity is coupled with the tendency to attend to details rather than global features of visual stimuli, the ‘risk’ of heighted emotional attachment to possessions increases more significantly than it would in the presence of either factor on its own. These results echo previous studies suggesting the contribution of detail-oriented information processing to the development of psychopathologies that are directly associated with trauma, such as PTSD (Bisby et al., 2009; Brewin et al., 2010; Hagenaars et al., 2016), or that present high prevalence of exposure to trauma or life adversities, such as anorexia nervosa (Lopez et al., 2008). It would also be of interest to examine the effect of detail-oriented visual processing on psychopathologies that are not as closely associated with trauma, since this visual processing style may not be exclusive to trauma- or hoarding-related psychological vulnerabilities.
Although a significant moderating effect of detailed-oriented visual processing style on the relationship between early life adversity and hoarding symptom severity was not found, the data suggested that detailed-oriented visual processing may, at least, exacerbate the effect of life adversity on one of the main underlying dysfunctions of HD: emotional attachment to possessions. It is of interest to examine how detail-oriented visual processing style may affect the relationships between early life adversity (or trauma) and other hoarding related dysfunctions (Frost and Hartl, 1996), and in turn affect HD symptom severity in future research.
The current study contains several limitations. First, the current sample was recruited from a previous study, which intentionally excluded individuals with mild-to-moderate hoarding symptom severity (i.e., SI-R scores between 20-40, or UHSS scores between 10-20). Thus, the use of this convenience sample may limit the generalizability of the current findings. In other words, it would not be reliable to apply the current conclusions, especially those related to hoarding symptom severity, to individuals with moderate hoarding tendencies. Although appropriate statistical methods were applied to minimize the potential impact of this issue, future studies in population samples should be conducted. Second, the current sample consisted of individuals from a large urban city and its surrounds who were motivated to participate and complete a study that involved long hours of neurocognitive testing and other clinical assessments. Therefore, some of the current findings (e.g., IQ scores among individuals with HD) may not be consistent with previous studies that used different recruitment methods or study designs. These limitations should be considered when generalizing the findings to other populations. Third, individuals with HD were older than the healthy participants in the current sample, and had a variety of comorbid diagnoses. Age and the comorbid diagnoses may have contributed to the current findings to some degree. While the effect of age was statistically accounted for in the regression analyses, future studies should either adopt a more homogenous sample in terms of psychiatric diagnosis or a larger sample to allow examination of comorbid conditions statistically. Fourth, we assessed the number of specific types of early life adversity using the ACE (Felitti et al., 1998; McGavock and Spratt, 2014). Although this measure estimates individuals’ experiences of a variety of common early life stressors, more detailed inquiries about these experiences (e.g., age when the events happened, the frequency of each type of life adversity, severity and psychological impacts of the events then and at the assessment) are needed to clarify how these other aspects of life adversity affect hoarding behaviors. Finally, we adopted a diagnostic tool based on the DSM-IV (SCID-I) to assess Axis I disorders other than HD. A diagnostic method based on the most current DSM system should be adopted in future studies.
Overall, the current study applied a method specifically designed to measure detail-vs.-global-oriented visual processing style (Booth, 2006), to our knowledge, for the first time in the literature of life adversity and hoarding. While a significant association was found between the commonly used RCFT accuracy index, and the style index (CCI), only the latter showed a significant relationship with exposure to early life adversity. This finding suggests a stronger impact of early life adversity on how, rather than how accurately, visual stimuli are processed. The findings also add to the literature by providing empirical evidence for the relationship between early life adversity and hoarding-related dysfunctions, and furthers the understanding of this relationship by identifying a neurocognitive feature, detail-oriented visual processing style, as a moderating factor. These results help clarify the mechanism through which early life adversity affects HD. Examination of detail-oriented visual processing style in more naturalistic settings using personal belongings of individuals who hoard (rather than standardized neuropsychological tests) in future research could help illuminate potential differences and similarities in the impacts of processing “symptom provoking” stimuli. Moreover, the current study only focused on one of the hoarding-related dysfunctions, emotional attachment to possessions. Future studies are needed to explore whether and how life adversity affects other identified dysfunctions (i.e., beliefs about possessions, other domains of information processing, and behavioral avoidance; Frost and Hartl, 1996) using measures such as the Saving Cognition Inventory (Steketee et al., 2003). Finally, longitudinal studies would be helpful to shed lights on causal relationships between these factors.
Highlights.
Life adversity predicts hoarding severity.
Life adversity predicts emotional attachment to possessions.
Detail-oriented visual processing strengthens the second relationship.
Acknowledgments
This study was funded jointly by PCORI grant CE-1304-6000 and NIH grant R21 MH087748.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th. American Psychiatric Publishing; Arlington, VA: 2013. [Google Scholar]
- Anda RF, Butchart A, Felitti VJ, Brown DW. Building a framework for global surveillance of the public health implications of adverse childhood experiences. Am J Prev Med. 2010;39(1):93–98. doi: 10.1016/j.amepre.2010.03.015. [DOI] [PubMed] [Google Scholar]
- Beck A, Steer R, Brown G. Manual for the BDI-II. Psychological Corporation; San Antonio, TX: 1996. [Google Scholar]
- Bisby JA, Brewin CR, Leitz JR, Curran HV. Acute effects of alcohol on the development of intrusive memories. Psychopharmacology. 2009;204(4):655–666. doi: 10.1007/s00213-009-1496-5. [DOI] [PubMed] [Google Scholar]
- Booth RDL. Local-global processing and cognitive style in autism spectrum disorders and typical development. University of London; 2006. [Google Scholar]
- Brewin CR, Gregory JD, Lipton M, Burgess N. Intrusive images in psychological disorders: characteristics, neural mechanisms, and treatment implications. Psychol Rev. 2010;117(1):210. doi: 10.1037/a0018113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chapman DP, Dube SR, Anda RF. Adverse childhood events as risk factors for negative mental health outcomes. Psychiatric Annuals. 2007;37(5):359–364. [Google Scholar]
- Chapman DP, Wheaton AG, Anda RF, Croft JB, Edwards VJ, Liu Y, et al. Sleep Med. 2011;12:773–779. doi: 10.1016/j.sleep.2011.03.013. [DOI] [PubMed] [Google Scholar]
- Chou CY, La Marca R, Steptoe A, Brewin CR. Heart rate, startle response, and intrusive trauma memories. Psychophysiology. 2014;51(3):236–246. doi: 10.1111/psyp.12176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cromer KR, Schmidt NB, Murphy DL. Do traumatic events influence the clinical expression of compulsive hoarding? Behav Res Ther. 2007;45(11):2581–2592. doi: 10.1016/j.brat.2007.06.005. [DOI] [PubMed] [Google Scholar]
- Dube SR, Fairweather D, Pearson WS, Felitti VJ, Anda RF, Croft JB. Cumulative childhood stress and autoimmune disease. Psychom Med. 2009;71:243–250. doi: 10.1097/PSY.0b013e3181907888. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. Am J Prev Med. 1998;14(4):245–258. doi: 10.1016/s0749-3797(98)00017-8. [DOI] [PubMed] [Google Scholar]
- First M, Spitzer RL, Gibbon M, William J. Structured Clinical Interview for the DSM-IV Axis I Disorders (SCID-I), Clinician Version. Arlington, VA: American Psychiatric Publishing; 1997. [Google Scholar]
- Frost RO, Hartl TL. A cognitive-behavioral model of compulsive hoarding. Behav Res Ther. 1996;34(4):341–350. doi: 10.1016/0005-7967(95)00071-2. [DOI] [PubMed] [Google Scholar]
- Frost RO, Steketee G, Grisham J. Measurement of compulsive hoarding: saving inventory-revised. Behav Res Ther. 2004;42(10):1163–1182. doi: 10.1016/j.brat.2003.07.006. [DOI] [PubMed] [Google Scholar]
- Frost RO, Steketee G, Tolin DF, Renaud S. Development and validation of the clutter image rating. J Psychopathol Behav Assess. 2008;30(3):193–203. [Google Scholar]
- Grisham JR, Norberg MM, Williams AD, Certoma SP, Kadib R. Categorization and cognitive deficits in compulsive hoarding. Behav Res Ther. 2010;48(9):866–872. doi: 10.1016/j.brat.2010.05.011. [DOI] [PubMed] [Google Scholar]
- Hagenaars M, Engelhard I, Putman P. Eye for detail: local versus global visual processing style predicts the development of re-experiences after analogue trauma. J Exp Psychopathol. 2016;7(3):391–403. [Google Scholar]
- Hartl TL, Duffany SR, Allen GJ, Steketee G, Frost RO. Relationships among compulsive hoarding, trauma, and attention-deficit/hyperactivity disorder. Behav Res Ther. 2005;43(2):269–276. doi: 10.1016/j.brat.2004.02.002. [DOI] [PubMed] [Google Scholar]
- Hartl TL, Frost RO, Allen GJ, Deckersbach T, Steketee G, Duffany SR, et al. Actual and perceived memory deficits in individuals with compulsive hoarding. Depress Anxiety. 2004;20(2):59–69. doi: 10.1002/da.20010. [DOI] [PubMed] [Google Scholar]
- Landau D, Iervolino AC, Pertusa A, Santo S, Singh S, Mataix-Cols D. Stressful life events and material deprivation in hoarding disorder. J Anxiety Disord. 2011;25(2):192–202. doi: 10.1016/j.janxdis.2010.09.002. [DOI] [PubMed] [Google Scholar]
- Lopez C, Tchanturia K, Stahl D, Booth R, Holliday J, Treasure J. An examination of the concept of central coherence in women with anorexia nervosa. Int J Eat Disord. 2008;41(2):143–152. doi: 10.1002/eat.20478. [DOI] [PubMed] [Google Scholar]
- Mackin RS, Vigil O, Insel P, Kivowitz A, Kupferman E, Hough CM, et al. Patterns of Clinically Significant Cognitive Impairment in Hoarding Disorder. Depress Anxiety. 2016;33(3):211–218. doi: 10.1002/da.22439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maughan B, McCarthy G. Childhood adversities and psychosocial disorders. Br Med Bull. 1997;53(1):156–169. doi: 10.1093/oxfordjournals.bmb.a011597. [DOI] [PubMed] [Google Scholar]
- McGavock L, Spratt T. Prevalence of adverse childhood experiences in a university population: Associations with use of social services. Br J Soc Work. 2014;44(3):657–674. [Google Scholar]
- Nelson HE. The National Adult Reading Test (NART): Test Manual 1982 [Google Scholar]
- Nelson HE, Willison J. National Adult Reading Test (NART) Nfer-Nelson; 1991. [Google Scholar]
- Nordsletten AE, Fernandez de la Cruz L, Pertusa A, Reichenberg A, Hatch SL, Mataix-Cols D. The Structured Interview for Hoarding Disorder (SIHD): Development, usage and futher validation. J Obsessive Compuls Relat Disord. 2013;2(3):346–350. doi: 10.1016/j.jocrd.2013.06.003. [DOI] [Google Scholar]
- Osterrieth P. Rey’s complexe figuur test. Swets & Zeitlinger Publishers; Amsterdam: 1944. [Google Scholar]
- Penza KM, Heim C, Nemeroff CB. Neurobiological effects of childhood abuse: implications for the pathophysiology of depression and anxiety. Arch Womens Ment Health. 2003;6(1):15–22. doi: 10.1007/s00737-002-0159-x. [DOI] [PubMed] [Google Scholar]
- Przeworski A, Cain N, Dunbeck K. Traumatic life events in individuals with hoarding symptoms, obsessive-compulsive symptoms, and comorbid obsessive-compulsive and hoarding symptoms. J Obsessive Compuls Relat Disord. 2014;3(1):52–59. [Google Scholar]
- Saxena S, Ayers CR, Dozier ME, Maidment KM. The UCLA hoarding severity scale: development and validation. J Affect Disord. 2015;175:488–493. doi: 10.1016/j.jad.2015.01.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steer RA, Ranieri WF, Beck AT, Clark DA. Further evidence for the validity of the Beck Anxiety Inventory with psychiatric outpatients. J Anxiety Disord. 1993;7(3):195–205. [Google Scholar]
- Stein MB, Kennedy CM, Twamley EW. Neuropsychological function in female victims of intimate partner violence with and without posttraumatic stress disorder. Biol Psychiatry. 2002;52(11):1079–1088. doi: 10.1016/s0006-3223(02)01414-2. [DOI] [PubMed] [Google Scholar]
- Steketee G, Frost RO, Kyrios M. Cognitive aspects of compulsive hoarding. Cognit Ther Res. 2003;27(4):463–479. [Google Scholar]
- Tolin DF, Meunier SA, Frost RO, Steketee G. Course of compulsive hoarding and its relationship to life events. Depress Anxiety. 2010;27(9):829–838. doi: 10.1002/da.20684. [DOI] [PubMed] [Google Scholar]
- Tolin DF, Villavicencio A, Umbach A, Kurtz MM. Neuropsychological functioning in hoarding disorder. Psychiatry Res. 2011;189(3):413–418. doi: 10.1016/j.psychres.2011.06.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tomalski P, Johnson MH. The effects of early adversity on the adult and developing brain. Curr Opin Psychiatry. 2010;23(3):233–238. doi: 10.1097/YCO.0b013e3283387a8c. [DOI] [PubMed] [Google Scholar]
- Wincze JP, Steketee G, Frost RO. Categorization in compulsive hoarding. Behav Res Ther. 2007;45(1):63–72. doi: 10.1016/j.brat.2006.01.012. [DOI] [PubMed] [Google Scholar]
- Woody SR, Kellman-McFarlane K, Welsted A. Review of cognitive performance in hoarding disorder. Clin Psychol Rev. 2014;34(4):324–336. doi: 10.1016/j.cpr.2014.04.002. [DOI] [PubMed] [Google Scholar]
- Young EA, Abelson JL, Curtis GC, Nesse RM. Childhood adversity and vulnerability to mood and anxiety disorders. Depress Anxiety. 1997;5(2):66–72. [PubMed] [Google Scholar]