

Abstract
Men employed in male-dominated occupations are at elevated risk of work-related fatalities, injuries, and suicide. Prior research has focused on associations between psychosocial and physical exposures at work and health outcomes. However, masculine norms may also contribute to mental health. We used data from the baseline survey of the Australian Longitudinal Study on Male Health to examine whether: (a) men in male-dominated jobs report greater adherence to masculine norms; (b) being in a male-dominated occupation is associated with poorer mental health; and (c) being in a male-dominated occupation modifies the association between masculine norms and mental health. Masculine norms were measured using the Conformity to Masculine Norms Inventory (CMNI-22). Mental health was assessed using the SF-12. Results of regression analysis (adjusted for covariates) suggest a linear relationship between the extent to which an occupation is male-dominated and endorsement of values on the CMNI-22. Many CMNI-22 subscales were related to poorer mental health. However, the need for self-reliance was identified as the strongest predictor of poorer mental health. The mental health scale did not appear to be patterned by occupational gender composition and we did not find an interaction between the gender ratio of an occupation and the CNMI-22 scale. These findings highlight the need to address harmful aspects of masculinity as a potential cause of mental health problems. More longitudinal research is needed on the social domains in which gender and health are experienced, such as in the workplace.
Keywords: work disorders, occupational health, mental health
Similar to other countries around the world, a substantial proportion of men in Australia are employed in male-dominated jobs, such as construction, mining, manufacturing, and emergency services (Australian Bureau of Statistics, 2006). Men in male-dominated industries are at elevated risk of work-related fatalities (Safe Work Australia, 2017b) and injury (Safe Work Australia, 2017a). International evidence also suggests that workers in male-dominated industries have elevated rates of suicide (Milner, Page, & LaMontagne, 2013; Roberts, Jaremin, & Lloyd, 2012) and there is some evidence that these men also have elevated risk of common mental health problems (Roche et al., 2016). Harmful physical and psychological working conditions (e.g., unsupportive workplace relationships, job overload, and job demands) are thought to explain part of the elevated disease burden in male-dominated occupations (Battams et al., 2014).
Masculine norms [defined as those culturally accepted rules and standards that guide and constrain masculine behaviors (Mahalik et al., 2003)], may also contribute to poorer health outcomes in male-dominated occupations. There are two common approaches to the study of masculine norms. The first is the social norms perspective, which views norms as socially learned and transmitted from an individual’s environment (Addis, Reigeluth, & Schwab, 2016). In contrast, the social constructivist perspective argues that there are a myriad of individual, microsocial, and macrosocial factors involved in the representation of gender (Addis et al., 2016). The social norms approach is much more commonly used in quantitative studies, as described below. These studies often emphasize the extent to which an individual adheres (or not) to masculine norms and, because of this, is of relevance to the current article.
In Western countries, norms and standards about masculine norms have been described and measured across a number of key domains, including attitudes toward employment, the desire for dominance (e.g., drive to win and be successful, being comfortable with asserting oneself or controlling a situation), importance of emotional control and self-reliance, and willingness to engage in risk-taking behaviors (Mahalik et al., 2003). Endorsement of these norms has been associated with a range of poor health behaviors [e.g., smoking, excessive drinking, or refusing to wear a seatbelt (Mahalik, Burns, & Syzdek, 2007)], stronger personal stigma related to mental health problems (Latalova, Kamaradova, & Prasko, 2014), and avoidance of health services (Latalova et al., 2014). Masculine norms may also influence how an individual perceives and experiences conditions such as depression, which may be manifested through somatic symptoms and externalizing behaviors (McDermott, Schwartz, & Rislin, 2016). Recent research has also linked some aspects of masculine norms to greater risk of thoughts about suicide (Pirkis, Spittal, Keogh, Mousaferiadis, & Currier, 2017).
An individual’s adoption of gender norms appears to be particularly related to socialization (Mahalik et al., 2007). For example, a major influence on the development of gender normative behaviors in childhood and adolescence are family, peers in school system, and media (among others) (Adler, Kless, & Adler, 1992; Leaper & Farkas, 2014). At the same time, research has also shown the influence of an occupation on reinforcing gender norms (Arkin & Dobrofsky, 1978; Barrett, 1996). However, the relationships between work and gender norms are likely to be bidirectional. Fouad, Whiston, and Feldwisch (2016) argue that males seek a sense of congruence between gender roles and employment throughout their working life, beginning when they first consider going into the labor market.
In this study, we seek to examine whether poorer mental health among males in male-dominated occupations is related to harmful gender norms. As a first step in investigating this topic, we assess whether men in male-dominated jobs report greater adherence to masculine norms, as measured using the Conformity to Masculine Norms Inventory-22. We then assess the mental health effects of being a male in a male-dominated occupation. Finally, we examine whether being in a male-dominated occupation modifies the association between masculine norms and male mental health. This study will use the Australian Longitudinal Study on Male Health, which is the largest cohort of its kind. Based on the research above, we hypothesized that (a) males in male-dominated occupations are more likely to endorse masculine norms; (b) masculine norms are associated with poor mental health; and (c) the impact of male-dominated occupations on mental health is greater among men who endorse traditionally masculine gender norms.
Methods
Sample
We used data from baseline survey of the Australian Longitudinal Study on Male Health (Ten to Men). Ten to Men is a national longitudinal study of boys and men aged 10 to 55 years at baseline. The study aims to collect data on a range of life domains, including demographic and socioeconomic characteristics, physical and mental health and well-being, health behaviors, and use and knowledge of health services. Sampling, recruitment, and data collection methods are described elsewhere (Pirkis et al., 2016). For this analysis, males 18 years and older were included (n = 13,884) as few males under the age of 17 years were participating in the workforce. This study received approval from the University of Melbourne Human Research Ethics Committee and conformed to the principles embodied in the Declaration of Helsinki.
Description of Gender Ratio of Occupations
Population data by occupation (sourced from the 2011 Australian census) (ABS, 2016) were used to create a continuous measure representing a ratio of males to females. We were able to extract population data for 44 occupations, corresponding to the two-digit occupation codes of the Australian and New Zealand Standard Classification of Occupations (ABS, 2009).
The continuous measure was skewed as many of the men in the cohort were employed in highly male-dominated occupations. Because of this, we created a categorical variable based on the ratio of males to females in an occupation: “not male-dominated occupation” (between 0.22 and 1 males to females), “slightly male dominated” (1 to 1.11 males to females), “moderately male dominated” (up to 2.48 males to females), “heavily male dominated” (2.49 to 5.79), and “very heavily male dominated” (5.80 or greater males to females). These categories corresponded to the quintiles of the original continuous variable. The occupations allocated to each of these categories can be seen in Appendix 1.
Masculine Norms
We used the Conformity to Masculine Norms Inventory (CMNI-22) to assess masculinity. This represents an abbreviated version of the original 94-item CMNI that was designed to measure cognitive, behavioral, and affective conformity to dominant masculine ideologies (Mahalik et al., 2003). The CMNI-22 uses the two highest loading items for each of the 11 factors from the original CNMI study and has a correlation of 0.92 with the full version of the questionnaire (Rochlen, McKelley, Suizzo, & Scaringi, 2008), which had scale reliability scores ranging from 0.44 (pursuit of status) to 0.81 (playboy). The inventory asks respondents to think about their own actions, feelings, and beliefs and indicate how much they personally agree or disagree with each of 22 statements which are scored from 0 (strongly disagree) to 3 (strongly agree). Some examples of pairs of statements correspond to 11 factors:
work (the sum of two scales: “My work is the most important part of my life” and “I don’t like giving all my attention to work” [reverse coded]);
emotional control (the sum of two scales: “I like to talk about my feelings” (reverse scored) and “I tend to share my feelings” (reverse scored)
We used the CMNI-22 as a continuous variable, with low scores indicating nonconformity and higher scores increasing conformity. Given that concerns have been raised about the internal consistency of the total scale (e.g., Rochlen et al. [2008] observed an internal estimate of 0.65), we also inspected each of the subscales of the CMNI-22. The internal consistency of these scales ranged from 0.81 for the playboy subscale to 0.44 for the work subscale.
Mental Health
Our outcome was the mental health subscale (psychological distress and psychological well-being) from the SF-12, the abbreviated form of the Short Form-36 (SF-36). Evidence suggests that this measure can be used to assess common mental health conditions (depression and anxiety) (Andrews, 2002; Salyers, Bosworth, Swanson, Lamb-Pagone, & Osher, 2000; Sanderson & Andrews, 2002a, 2002b; Sanderson, Andrews, & Jelsma, 2001) and has acceptable reliability within clinical samples (Salyers et al., 2000). A clinically meaningful decline in the SF-12 would be a reduction of 4.2, which corresponded to 12-month cutoff for depressive illnesses in a large multinational study (Vilagut et al., 2013). In the Australia context, scores below 45 were assessed as being a clinical cutoff for depression, while scores below 50 were indicative of any common mental disorder (Gill, Butterworth, Rodgers, & Mackinnon, 2007).
Covariates
Our covariates included: age (18–24 years, 25–34 years, 35–44 years, 45–54 years, 55 years and over), education (less than 12 years, more than 12 years), relationship status (never married, widowed, divorced, separated but not divorced, married/de facto), and combined household income (scored from 1 representing $3840 or more per week ($200,000 or more per year) to 12 representing $1–$189 per week ($1–$9,999 per year)). These were analyzed as categorical variables.
Analysis
For hypothesis one, we examined mean levels of the CMNI-22 by the categorical occupation gender ratio variable, with 95% confidence intervals. We graphed the overall mean of the CMNI-22 (and its subscales) by each level of the occupational gender ratio. Following this, we conducted an ordinary least squares (OLS) linear regression (StataCorp, 2017) model with the CMNI-22 (and all subscales) as the outcome and categorical occupation gender ratio variable as the main predictor adjusting for all covariates.
For hypothesis two and three, we conducted an OLS regression model with the mental health subscale of the SF-12 as the overall outcome. We assessed the main effects of the CMNI-22 scale (and all subscales) and the occupational gender ratio on mental health. These variables were included in the model both jointly as well as being considered separately. An interaction term between the occupational gender ratio and the CMNI-22 (and all subscales) was included to assess the possibility of effect modification. The covariates mentioned above were controlled for in the model. A Wald test was used to determine model fit with the covariates—a test statistic of zero strongly suggests that removing them from the model will not substantially reduce the fit of that model. A likelihood ratio test was used to assess the significance of a model with an interaction term compared to one without.
Analytic Sample
The process of selecting participants can be seen in Figure 1. Participants were excluded if it was missing on any of the variables. An overall description of the sample can be seen in Table 1.
Figure 1.
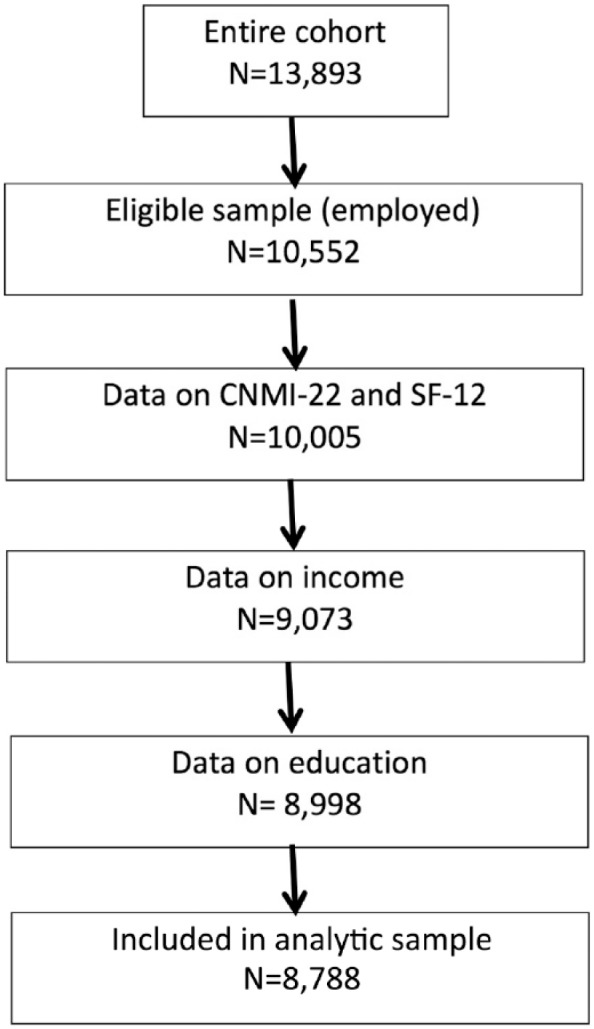
Description of the analytic sample.
Table 1.
Description of the Sample.
| Mean | 95% CI | |
|---|---|---|
| Mental health (SF-12) (mean, 95% CI) | 50.64 | [50.46, 50.81] |
| n | % | |
| Occupational gender ratio | ||
| Not male dominated | 1,756 | 19.98 |
| 1 to 1.11 males to females | 413 | 4.7 |
| 1.12 to 2.48 males to females | 2,200 | 25.03 |
| 2.49 to 5.79 males to females | 2,299 | 26.16 |
| Over 5.80 males to females | 2,120 | 24.12 |
| Age group | ||
| 18–24 years | 774 | 8.81 |
| 25–34 years | 2,078 | 23.65 |
| 35–44 years | 2,872 | 32.68 |
| 45–54 years | 2,890 | 32.89 |
| 55 years | 174 | 1.98 |
| Relationship status | ||
| Never married | 1,612 | 18.34 |
| Widowed | 26 | 0.3 |
| Divorced | 312 | 3.55 |
| Separated | 202 | 2.3 |
| Married/de facto | 6,636 | 75.51 |
| Employment arrangement | ||
| Permanent | 6,314 | 71.85 |
| Casual/fixed term | 1,116 | 12.7 |
| Self-employed | 1,358 | 15.45 |
| Occupational skill level | ||
| High | 3,510 | 39.94 |
| Medium–high | 2,717 | 30.92 |
| Medium–low | 922 | 10.49 |
| Low | 1,639 | 18.65 |
| Education | ||
| Under 12 years | 3,291 | 37.45 |
| Over 12 years | 5,497 | 62.55 |
| Income | ||
| $3,840 or more per week ($200,000 or more) | 933 | 10.62 |
| $2,880–$3,839 per week ($150,000–$1,999) | 1,161 | 13.21 |
| $2,400–$2,879 per week ($125,000–$1,499) | 1,063 | 12.1 |
| $1,920–$2,399 per week ($100,000–$1,249) | 1,427 | 16.24 |
| $1,530–$1,919 per week ($80,000–$99,999) | 1,328 | 15.11 |
| $1,150–$1,529 per week ($60,000–$79,999) | 1,214 | 13.81 |
| $960–$1,149 per week ($50,000–$59,999) | 610 | 6.94 |
| $1–$959 per week ($1–$49,999) | 1,052 | 11.97 |
Note. CI = confidence interval.
Results
The mean score of the CMNI-22 in the analytic sample was 27.37 (95% CI [27.25, 27.48]) (Table 1). As can be seen in Figure 2, there were differences in the CMNI-22 depending on the gender ratio of an occupation. There appears to be a relatively linear relationship between the extent to which an occupation is more heavily male dominated and endorsement of values on the CMNI. There was, however, a slight flattening out of the CNMI in the moderately male-dominated occupations, followed by an increase in the most male-dominated occupations.
Figure 2.

Overall mean (with 95% confidence intervals) of the CMNI by occupation gender ratio, ten to men.
Note. NMD = not male dominated; m/f = ratio of males to females in an occupation.
Regression models for the relationship between subscales of the CMNI-22 by the gender ratio of an occupation can be seen in Table 2 (after controlling for covariates). As can be seen, there was considerable diversity in the gender ratio of an occupation. There was a clear stepwise gradient (where higher scores of the subscale were associated with a higher male to female gender ratio) for power over women, emotional control, and heterosexual presentation. Those in more male-dominated occupations also tended to endorse the violence subscale. However, there was lower endorsement of the pursuit of status subscale in more male-dominated occupations. Those in only slightly male-dominated occupations had higher scores on the playboy subscale, followed by heavily male-dominated occupations.
Table 2.
The Relationship Between the Subscales of the CNMI-22 and Occupational Gender Ratio, Regression Model, Adjusted for Covariates.
| Occupational gender ratio | Estimate (95% CI) | p value | Occupational gender ratio | Estimate (95% CI) | p value | ||
|---|---|---|---|---|---|---|---|
| Pursuit of status (CNMI-22 subscale) | Winning (CNMI-22 subscale) | ||||||
| NMD | Ref | NMD | Ref | ||||
| 1 to 1.11 m/f | 0.10 | [−0.01, 0.21] | .063 | 1 to 1.11 m/f | 0.12 | [0.01, 0.23] | .025 |
| 1.12 to 2.48 m/f | 0.02 | [−0.04, 0.08] | .581 | 1.12 to 2.48 m/f | 0.10 | [0.03, 0.16] | .005 |
| 2.49 to 5.79 m/f | −0.07 | [−0.13, −0.01] | .020 | 2.49 to 5.79 m/f | 0.01 | [−0.06, 0.07] | .947 |
| Over 5.80 m/f | −0.10 | [−0.16, −0.04] | .001 | Over 5.80 m/f | 0.02 | [−0.05, 0.09] | .561 |
| Playboy (CNMI-22 subscale) | Self-reliance (CNMI-22 subscale) | ||||||
| NMD | Ref | NMD | Ref | ||||
| 1 to 1.11 m/f | 0.21 | [0.06, 0.34] | .005 | 1 to 1.11 m/f | 0.03 | [−0.08, 0.15] | .606 |
| 1.12 to 2.48 m/f | 0.09 | [0.01, 0.17] | .023 | 1.12 to 2.48 m/f | 0.09 | [0.03, 0.16] | .006 |
| 2.49 to 5.79 m/f | 0.07 | [−0.01, 0.15] | .093 | 2.49 to 5.79 m/f | 0.05 | [−0.01, 0.12] | .115 |
| Over 5.80 m/f | 0.12 | [0.03, 0.20] | .006 | Over 5.80 m/f | 0.09 | [0.02, 0.16] | .013 |
| Heterosexual presentation (CNMI-22 subscale) | Violence (CNMI-22 subscale) | ||||||
| NMD | Ref | NMD | Ref | ||||
| 1 to 1.11 m/f | 0.06 | [−0.11, 0.22] | .496 | 1 to 1.11 m/f | −0.06 | [−0.21, 0.10] | .459 |
| 1.12 to 2.48 m/f | 0.10 | [0.01, 0.20] | .043 | 1.12 to 2.48 m/f | −0.01 | [−0.10, 0.08] | .846 |
| 2.49 to 5.79 m/f | 0.19 | [0.10, 0.28] | < .001 | 2.49 to 5.79 m/f | 0.12 | [0.03, 0.21] | .009 |
| Over 5.80 m/f | 0.36 | [0.26, 0.46] | < .001 | Over 5.80 m/f | 0.14 | [0.06, 0.24] | .002 |
| Dominance (CNMI-22 subscale) | Work (CNMI-22 subscale) | ||||||
| NMD | Ref | NMD | Ref | ||||
| 1 to 1.11 m/f | 0.02 | [−0.09, 0.14] | .674 | 1 to 1.11 m/f | 0.02 | [−0.10, 0.14] | .769 |
| 1.12 to 2.48 m/f | 0.15 | [0.08, 0.21] | < .001 | 1.12 to 2.48 m/f | 0.05 | [−0.03, 0.12] | .214 |
| 2.49 to 5.79 m/f | 0.05 | [−0.01, 0.12] | .103 | 2.49 to 5.79 m/f | 0.04 | [−0.04, 0.11] | .331 |
| Over 5.80 m/f | 0.04 | [−0.03, 0.11] | .242 | Over 5.80 m/f | −0.01 | [−0.08, 0.07] | .826 |
| Power over women (CNMI-22 subscale) | Emotional control (CNMI-22 subscale) | ||||||
| NMD | Ref | NMD | Ref | ||||
| 1 to 1.11 m/f | 0.10 | [−0.02, 0.20] | .059 | 1 to 1.11 m/f | 0.07 | [−0.08, 0.22] | .354 |
| 1.12 to 2.48 m/f | 0.13 | [0.06, 0.19] | < .001 | 1.12 to 2.48 m/f | 0.14 | [0.06, 0.22] | .001 |
| 2.49 to 5.79 m/f | 0.14 | [0.08, 0.20] | < .001 | 2.49 to 5.79 m/f | 0.19 | [0.11, 0.27] | < .001 |
| Over 5.80 m/f | 0.21 | [0.15, 0.28] | < .001 | Over 5.80 m/f | 0.19 | [0.11, 0.28] | < .001 |
| Risk taking (CNMI-22 subscale) | Total CNMI-22 | ||||||
| NMD | Ref | NMD | Ref | ||||
| 1 to 1.11 m/f | 0.10 | [−0.02, 0.22] | .109 | 1 to 1.11 m/f | 0.81 | [0.23, 1.39] | .006 |
| 1.12 to 2.48 m/f | 0.06 | [−0.01, 0.13] | .078 | 1.12 to 2.48 m/f | 0.95 | [0.60, 1.30] | < .001 |
| 2.49 to 5.79 m/f | −0.03 | [−0.10, 0.04] | .438 | 2.49 to 5.79 m/f | 0.78 | [0.44, 1.12] | < .001 |
| Over 5.80 m/f | 0.04 | [−0.04, 0.10] | .323 | Over 5.80 m/f | 1.15 | [0.79, 1.50] | < .001 |
Note. Models adjusted for educational level, household income, employment arrangements, age, and relationship status. NMD = not male dominated; m/f = ratio of males to females in an occupation.
Table 3 shows the main effects of each of the CMNI subscales on mental health, after controlling for the occupational gender ratio (which was not independently associated with mental health) and covariates. As can be seen, a greater score on self-reliance was associated with a 1.50 decline in mental health. There were small declines in mental health associated with violence, emotional control, power over women, and the playboy subscale. The only subscales that were not associated with mental health were risk taking, heterosexual presentation, and pursuit of status subscales. The effect of the total CMNI-22 scale was −0.17 (95% CI [−0.20, −0.13], p < .001). In regression models with the CMNI subscale*occupation gender ratio interaction, there was no evidence that the gender ratio of an occupation moderated the effect of total CMNI-22 scale or any subscale on mental health (mental health subscale of the SF-12) (results available on request). The effects of the CMNI on mental health were retained after the occupation gender ratio was removed from the model.
Table 3.
Individual Models Describing the Effect of Each Subscale of the CNMI-22 on Mental Health, After Adjusting for Covariates.
| Variable | Estimate (95% CI) | p value | |
|---|---|---|---|
| Total CNMI-22 scale | −0.17 | [−0.20, −0.13] | < .001 |
| Emotional control | −0.42 | [−0.57, −0.29] | < .001 |
| Pursuit of status | 0.04 | [−0.23, 0.14] | .657 |
| Playboy | −0.75 | [−0.90, −0.61] | < .001 |
| Heterosexual presentation | 0.04 | [0.07, 0.16] | .450 |
| Dominance | −0.20 | [−0.38, 0.03] | .020 |
| Power over women | −0.41 | [−0.60, −0.24] | < .001 |
| Risk taking | −0.02 | [−0.18, 0.14] | .830 |
| Winning | −0.36 | [−0.52, −0.18] | .010 |
| Reliance | −1.50 | [−1.66, −1.33] | < .001 |
| Violence | −0.48 | [−0.60, −0.36] | < .001 |
| Work | 0.37 | [0.22, 0.53] | < .001 |
Note. Each subscale assessed in separate models, adjusting for occupational gender ratio, educational level, household income, employment arrangements, age, and relationship status.
Discussion
This study has shown that endorsement of masculinity appears to be patterned by occupation in Australia. Men in the most highly male-dominated occupations tended to more strongly adhere to certain masculine gender norms, including those regarding the pursuit of women (the “playboy” subscale), emotional control, the endorsement of violence, heterosexual presentation, and having power over women. Our study suggests that many of these subscales were related to worse mental health. However, the need for self-reliance was identified as the strongest predictor of poorer mental health. The mental health scale did not appear to be patterned by the gender composition of a job and we did not find an interaction between the gender ratio of an occupation and the CMNI-22 scale. As we discuss below, there are a number of possible explanations of this relationship.
Masculine Norms in Male-Dominated Jobs
These results confirm previous research suggesting that men in highly male-dominated environments are more likely to endorse specific gender norms (Arkin & Dobrofsky, 1978; Barrett, 1996). There has been limited previous research examining the subscales of the CMNI-22 by occupational group; hence, it is difficult to find other studies to compare our research too. However, there have been a number of qualitative and sociological studies that have examined gender within a variety of organizational contexts. This research suggests that in highly male-dominated jobs, males actively participate in reinforcing models around “men’s work” and masculinity as the normative standard (e.g., Acker, 1990; Denissen, 2010; Simpson & Lewis, 2005). For example, in construction, male workers hold each other accountable for doing tasks in “masculine” ways emphasizing the need for characteristics such as strength and roughness, and devaluing perceived “feminine” behaviors (Simpson & Lewis, 2005). As noted by Acker (1990), these performative aspects of gender begin during the hiring and training processes and continue throughout an entire job. Thus, men who are employed in male-dominated jobs may be regularly exposed to gender norms reinforcing the “playboy” stereotype, the need for emotional control, endorsement of violence, heterosexual presentation, and having power over women. It is also important to acknowledge the likelihood of self-selection into gender-dominated or neutral occupations, in that workers who identify more strongly with cultural norms around masculinity/femininity may be drawn to more male/female dominated occupations, respectively (Acker, 1990). This point has also been recognized in vocational research. For example, Holland’s theory (Holland, 1997; Nauta, 2013 cited in Fouad et al., 2016) recognizes that people are likely to seek out work environments that fit with their vocational personalities.
Masculine Norms and Mental Health
As mentioned in this article’s introduction, there is evidence from numerous fields that masculine gender norms are associated with poorer health, including mental health conditions and suicide (Latalova et al., 2014; Pirkis et al., 2017). Our study adds support to this literature. The specific subscales associated with poorer mental health included endorsement of violence, the perception that men should have power over women, and the playboy subscale. However, by and large, we saw the largest reductions in mental health associated with the self-reliance subscale. This finding reinforces a recent study on masculinity and suicidality (Pirkis et al., 2017). The CMNI-22 assesses self-reliance in terms of behavioral and affective response to help seeking: “I never ask for help” (Item 18) and “It bothers me when I have to ask for help” (Item 22) (Pirkis et al., 2017). Males who endorse these items may therefore be less likely to reach out to support services (including family and friends) when they are experiencing mental health problems. We would note however that the decline we observed was relatively small and unlikely to be clinically meaningful at an individual level.
The occupational gender ratio did have an effect on mental health. This finding differs from a recent study by Caroli and Weber-Baghdiguian (2016), which assessed the relationship between the gender ratio of a job and self-rated health using data from the United States. This found that men working in female- and male-dominated environments reported worse health than men employed in mixed gender environments. However, the extent to which this study can be compared with ours is limited considering the differences in contexts and outcomes under study. It is also possible that the relationship between mental health and occupational gender ratio for men is altogether more complex. For example, there may be other confounders we have not considered or within-person effects. There is substantial research suggesting that suicide rates are higher in male-dominated jobs, but findings regarding mental health are less clear (Roche et al., 2016).
Limitations and Strengths
The weaknesses of this study are that we have limited ability to state a causal relationship about the variables we examined because of the cross-sectional design. Related to this, we are unable to rule out reverse causality (e.g., that poor mental health causes problematic gender norms). We are also unable to establish the extent to which an occupation changes gender norms versus the possibility that specific males holding certain gender norms select into occupations. To some extent, these issues will be able to be resolved when additional waves of data are analyzed and we are able to repeat this study prospectively. Additional waves of data will also mean that we are able to better control for individual sources of variation (e.g., personality) through the use of fixed-effects models, which apply within-person clustering to analysis. Another problem affecting this study is dependent misclassification, as both the exposure and the outcome were self-reported. We also acknowledge the fact that the measurement of masculinity is highly complex. The scale we used was developed in the United States (Mahalik et al., 2003) and may not have identified aspects of masculinity pertinent to the Australian context. It is also necessary to note that previous studies have shown that the total scale only has a moderate internal consistency, particularly when compared with the full version of the scale consistency (Rochlen et al., 2008). This suggests the importance of assessing the subscales as separate constructs. This may also explain why we found fewer studies using the CNMI-22.
Future Work and Implications for Policy
Within public health, there is growing understanding of the role of gender as an important social determinant of health (Krieger, 2003; Phillips, 2005). However, there are still a variety of perspectives on which aspects of gender are the most critical for health (Fikree & Pasha, 2004; Sen & Östlin, 2008). Individually held gendered norms may influence an individual’s likelihood to seek treatment, and to receive meaningful and adequate treatment (Latalova et al., 2014; Pirkis et al., 2017). The ways in which gender is constructed within a social group may also be a powerful influence on health outcomes (Caroli & Weber-Baghdiguian, 2016). These myriad of perspectives highlight the need for a greater amount of public-health orientated research on the ways in which gender influences a wide range of health outcomes. This article constitutes one of the first quantitative assessments of the relationship between masculine norms, occupation, and mental health. We would suggest the need for more research in this area, in particular focusing on the social domains in which gender and health are experienced, such as in the workplace.
Acknowledgments
The research on which this article is based on was conducted as part of the Australian Longitudinal Study on Male Health by the University of Melbourne.
Appendix
Appendix 1.
Australian and New Zealand Standard Classification of Occupations (ABS, 2009) by the Gender Ratio of the Occupation.
| Occupation: Two-digit ANZSCO | Observation | % |
|---|---|---|
| Not male dominated | ||
| Carers and aides | 111 | 5.18 |
| Cleaners and laundry workers | 127 | 5.93 |
| Education professionals | 364 | 16.99 |
| Food preparation assistants | 80 | 3.73 |
| General clerical workers | 75 | 3.5 |
| Health professionals | 252 | 11.76 |
| Health and welfare support workers | 84 | 3.92 |
| Hospitality workers | 112 | 5.23 |
| Inquiry clerks and receptionists | 1 | 0.05 |
| Legal, social, and welfare professionals | 125 | 5.84 |
| Numerical clerks | 77 | 3.59 |
| Office managers and program administrators | 121 | 5.65 |
| Other clerical and administrative workers | 210 | 9.8 |
| Personal assistants and secretaries | 1 | 0.05 |
| Sales assistants and salespersons | 307 | 14.33 |
| Sales support workers | 1 | 0.05 |
| Sports and personal service workers | 94 | 4.39 |
| 1 to 1.11 males to females | ||
| Business, human resource, and marketing professionals | 461 | 100 |
| 1.12 to 2.48 males to females | ||
| Arts and media professionals | 87 | 3.33 |
| Clerical and office support workers | 68 | 2.6 |
| Factory process workers | 250 | 9.57 |
| Food trades workers | 180 | 6.89 |
| Hospitality, retail, and service managers | 384 | 14.7 |
| Inadequately described | 90 | 3.45 |
| Other technicians and trades workers | 157 | 6.01 |
| Sales representatives and agents | 182 | 6.97 |
| Skilled animal and horticultural workers | 188 | 7.2 |
| Specialist managers | 1,026 | 39.28 |
| 2.49 to 5.79 males to females | ||
| Chief executives, general managers, and legislators | 128 | 4.68 |
| Design, engineering, science, and transport professionals | 515 | 18.82 |
| Engineering, Information and communications technology, and science technicians | 378 | 13.82 |
| Farm, forestry, and garden workers | 164 | 5.99 |
| Farmers and farm managers | 331 | 12.1 |
| ICT professionals | 312 | 11.4 |
| Machine and stationary plant operators | 244 | 8.92 |
| Other laborers | 213 | 7.79 |
| Protective service workers | 303 | 11.07 |
| Storepersons | 148 | 5.41 |
| Over 5.80 males to females | ||
| Automotive and engineering trades workers | 650 | 25.02 |
| Construction trades workers | 625 | 24.06 |
| Construction and mining laborers | 227 | 8.74 |
| Electrotechnology and telecommunications trades workers | 420 | 16.17 |
| Mobile plant operators | 227 | 8.74 |
| Road and rail drivers | 449 | 17.28 |
Footnotes
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. The authors are grateful to the Australian Government Department of Health for funding and to the boys and men who provided survey data. AM was supported by the Victorian Health and Medical Research Fellowship.
ORCID iD: Allison Milner  https://orcid.org/0000-0003-4657-0503
https://orcid.org/0000-0003-4657-0503
References
- ABS. (2009). ANZSCO— Australian and New Zealand Standard Classification of Occupations (1st ed, Revision 1, Cat. No. 1220.0). Canberra: Australian Bureau of Statistics. [Google Scholar]
- ABS. (2016). Tablebuilder pro. census—2011. Canberra: Australian Bureau of Statistics. [Google Scholar]
- Acker J. (1990). Hierarchies, jobs, bodies: A theory of gendered organizations. Gender and Society, 4(2), 139–158. [Google Scholar]
- Addis M. E., Reigeluth C. S., Schwab J. R. (2016). Social norms, social construction, and the psychology of men and masculinity. In Wong J., Wester S. R. (Eds.), APA handbook of men and masculinities (pp. 81–104). Washington, DC: American Pyschological Association. [Google Scholar]
- Adler P. A., Kless S. J., Adler P. (1992). Socialization to gender roles: Popularity among elementary school boys and girls. Sociology of Education, 65(3), 169–187. doi: 10.2307/2112807 [DOI] [Google Scholar]
- Andrews G. (2002). A brief integer scorer for the SF-12 validity of the brief scorer in Australian community and clinic settings. Australian & New Zealand Journal of Public Health, 26, 508–510. [DOI] [PubMed] [Google Scholar]
- Arkin W., Dobrofsky L. R. (1978). Military socialization and masculinity. Journal of Social Issues, 34(1), 151–168. doi: 10.1111/j.1540-4560.1978.tb02546.x [DOI] [Google Scholar]
- Australian Bureau of Statistics. (2006). 2006 census: Labour force: Occupation 06 (ANZSCO) (OCC06P)—2 digit by Sex Male/Female (SEXP) counting: Persons, place of usual residence. viewed 1 april 2017. Canberra: Australian Bureau of Statistics. [Google Scholar]
- Barrett F. J. (1996). The organizational construction of hegemonic masculinity: The case of the US navy. Gender, Work & Organization, 3(3), 129–142. doi: 10.1111/j.1468-0432.1996.tb00054.x [DOI] [Google Scholar]
- Battams S., Roche A. M., Fischer J. A., Lee N. K., Cameron J., Kostadinov V. (2014). Workplace risk factors for anxiety and depression in male-dominated industries: A systematic review. Health Psychology and Behavioral Medicine, 2(1), 983–1008. doi: 10.1080/21642850.2014.954579 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caroli E., Weber-Baghdiguian L. (2016). Self-reported health and gender: The role of social norms. Social Science & Medicine, 153, 220–229. doi: 10.1016/j.socscimed.2016.02.023 [DOI] [PubMed] [Google Scholar]
- Denissen A. M. (2010). The right tools for the job: Constructing gender meanings and identities in the male-dominated building trades. Human Relations, 63(7), 1051–1069. [Google Scholar]
- Fikree F. F., Pasha O. (2004). Role of gender in health disparity: The South Asian context. BMJ: British Medical Journal, 328(7443), 823–826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fouad N. A., Whiston S. C., Feldwisch R. (2016). Men and men’s careers. In Wong Y. J., Wester S. R. (Eds.), APA handbook of men and masculinities (pp. 503–524). Washington, DC: American Psychological Association. [Google Scholar]
- Gill S. C., Butterworth P., Rodgers B., Mackinnon A. (2007). Validity of the mental health component scale of the 12-item short-form health survey (MCS-12) as measure of common mental disorders in the general population. Psychiatry Research, 152, 63–71. doi: 10.1016/j.psychres.2006.11.005 [DOI] [PubMed] [Google Scholar]
- Krieger N. (2003). Genders, sexes, and health: What are the connections–and why does it matter? International Journal of Epidemiology, 32(4), 652–657. [DOI] [PubMed] [Google Scholar]
- Latalova K., Kamaradova D., Prasko J. (2014). Perspectives on perceived stigma and self-stigma in adult male patients with depression. Neuropsychiatric Disease and Treatment, 10, 1399–1405. doi: 10.2147/NDT.S54081 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leaper C., Farkas T. (2014). The socialization of gender during childhood and adolescence. In Grusec J. E., Hastings P. D. (Eds.), Handbook of socialization: Theory and research (2nd ed., pp. 541–565). New York, NY: Guilford Publications. [Google Scholar]
- Mahalik J. R., Burns S. M., Syzdek M. (2007). Masculinity and perceived normative health behaviors as predictors of men’s health behaviors. Social Science Medicine, 64(11), 2201–2209. doi: 10.1016/j.socscimed.2007.02.035 [DOI] [PubMed] [Google Scholar]
- Mahalik J. R., Locke B. D., Ludlow L. H., Diemer M., Scott R. P. J., Gottfried M., Freitas G. (2003). Development of the conformity to masculine norms inventory. Psychology of Men & Masculinity, 4, 3–25. [Google Scholar]
- McDermott R. C., Schwartz J. P., Rislin J. L. (2016). Men’s mental health: A biopsychosocial critique. In Wong Y. J., Wester S. R. (Eds.), APA handbook of men and masculinities (pp. 731–751). Washington, DC: American Psychological Association. [Google Scholar]
- Milner A., Spittal M. J., Pirkis J., LaMontagne A. D. (2013). Suicide by occupation: systematic review and meta-analysis. British Journal of Psychiatry, 203(6), 409-416. doi: 10.1192/bjp.bp.113.128405 [DOI] [PubMed] [Google Scholar]
- Phillips S. P. (2005). Defining and measuring gender: A social determinant of health whose time has come. International Journal for Equity in Health, 4, 11–11. doi: 10.1186/1475-9276-4-11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pirkis J., Currier D., Carlin J., Degenhardt L., Dharmage S., Giles-Corti B., … English D. (2016). Cohort profile: Ten to men (The Australian Longitudinal Study on Male Health). International Journal of Epidemiology, 46(3), 793–794. doi: 10.1093/ije/dyw055 [DOI] [PubMed] [Google Scholar]
- Pirkis J., Spittal M. J., Keogh L., Mousaferiadis T., Currier D. (2017). Masculinity and suicidal thinking. Social Psychiatry Psychiatr Epidemiolgy, 52(3), 319–327. doi: 10.1007/s00127-016-1324-2 [DOI] [PubMed] [Google Scholar]
- Roberts S. E., Jaremin B., Lloyd K. (2012). High-risk occupations for suicide. Psychological Medicine, 43(6), 1231–1240. doi: 10.1017/s0033291712002024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roche A. M., Pidd K., Fischer J. A., Lee N., Scarfe A., Kostadinov V. (2016). Men, work, and mental health: A systematic review of depression in male-dominated industries and occupations. Safety and Health at Work, 7(4), 268–283. doi: 10.1016/j.shaw.2016.04.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rochlen A. B., McKelley R. A., Suizzo M.-A., Scaringi V. (2008). Predictors of relationship satisfaction, psychological well-being, and life satisfaction among stay-at-home fathers. Psychology of Men & Masculinity, 9(1), 17–28. doi: 10.1037/1524-9220.9.1.17 [DOI] [Google Scholar]
- Safe Work Australia. (2017. a). Disease and injury statistics by industry. Retrieved from https://www.safeworkaustralia.gov.au/statistics-and-research/statistics/disease-and-injuries/disease-and-injury-statistics-industry
- Safe Work Australia. (2017. b). Fatality statistics by industry. Retrieved from https://www.safeworkaustralia.gov.au/statistics-and-research/statistics/fatalities/fatality-statistics-industry
- Salyers M. P., Bosworth H. B., Swanson J. W., Lamb-Pagone J., Osher F. C. (2000). Reliability and validity of the SF-12 health survey among people with severe mental illness. Medical Care, 38, 1141–1150. [DOI] [PubMed] [Google Scholar]
- Sanderson K., Andrews G. (2002. a). Prevalence and severity of mental health related disability and relationship to diagnosis. Psychiatric Services, 53, 80–86. [DOI] [PubMed] [Google Scholar]
- Sanderson K., Andrews G. (2002. b). The SF-12 in the Australian population: Cross-validation of item selection. Australian & New Zealand Journal of Public Health, 26, 343–345. [DOI] [PubMed] [Google Scholar]
- Sanderson K., Andrews G., Jelsma W. (2001). Disability measurement in the anxiety disorders: Comparison of three brief measures. Journal of Anxiety Disorders, 15, 333–344. [DOI] [PubMed] [Google Scholar]
- Sen G., Östlin P. (2008). Gender inequity in health: Why it exists and how we can change it. Global Public Health, 3(suppl 1), 1–12. doi: 10.1080/17441690801900795 [DOI] [PubMed] [Google Scholar]
- Simpson R., Lewis P. (2005). An investigation of silence and scrutiny of transparency: Re-examining gender in organization literature through the concepts of voice and visibility. Human Relations, 58(10), 1253–1275. [Google Scholar]
- StataCorp. (2017). Stata 15 base reference manual (pp. 1–25). College Station, TX: Stata Press. [Google Scholar]
- Vilagut G., Forero C. G., Pinto-Meza A., Haro J. M., de Graaf R., Bruffaerts R., … Alonso J. (2013). The mental component of the short-form 12 health survey (SF-12) as a measure of depressive disorders in the general population: Results with three alternative scoring methods. Value in Health, 16(4), 564–573. Retrieved from 10.1016/j.jval.2013.01.006 [DOI] [PubMed] [Google Scholar]