

Abstract
The Joint Commission provides accreditation standards for staging hospital waste, but there are no federal lifting safety standards for linen bags. We evaluated hospital laundry bag lifting using the Revised National Institute for Occupational Safety and Health (NIOSH) Lifting Equation. We hypothesized that the permitted 32-gallon linen container capacity might allow filling to weights above our calculated Recommended Weight Limit (RWL) for some lifting positions and contents. We found that 30- and 40-gallon bags filled with loose dry linen had predicted weights within estimated RWLs only for lifts close to the body. 30- and 40-gallon bags filled more than halfway with dry compact linen had predicted weights above estimated RWLs for all lifting positions. 30- and 40-gallon bags filled with wet compact linen exceeded estimated RWLs for all positions when less than one-quarter full. Bag volume and filling controls may be considered to ensure linen bags are not excessively heavy.
Keywords: healthcare, linen, manual handling, safety
Introduction:
In the United States, the healthcare and social assistance sector employed over 18 million workers in 2014, with the number of jobs in this sector projected to increase to nearly 21.9 million by 2024 (6). High quality, safe healthcare depends not only on the work of direct patient care providers, but also on the work performed by non-patient care healthcare workers who clean, maintain, and supply healthcare facilities and grounds. Among such non-patient care healthcare workers, those performing hospital laundry collection tasks face unique safety challenges and may be exposed to infectious and toxic materials (3), improperly disposed of sharps (7), and significant musculoskeletal injury risks (8) from work that is repetitive, strenuous, and requires awkward postures and frequent bending (9).
The United States National Occupational Research Agenda (NORA) includes a declaration of the critical need for improved safety for all healthcare sector workers (10). In particular, the NORA Healthcare and Social Assistance Agenda has identified non-patient care workers, including laundry workers, as an occupational group requiring prioritized attention. In the case of soiled linen bag handling, although lifting close to the body is generally recommended to reduce stress on the lower back during manual materials handling tasks (1, 11), linen collection workers must balance ideal lifting technique with the need to minimize body contact with soiled linen bags in order to avoid potential contact with contaminated waste or concealed sharps (9).
High volume soiled linen collection is a universal challenge for healthcare facilities. The Joint Commission provides guidelines for staging and handling hospital waste, including capacity limits for waste and soiled linen storage containers in healthcare or ambulatory service areas outside of protected waste collection areas (12). These accreditation standards for waste management reflect fire safety and infection control considerations (12). For containers outside of designated waste collection areas, the Joint Commission limits container capacity to not more than 32 gallons for a single container or 0.5 gallons per square foot where there are multiple containers (12). However, there is no federal ergonomics standard covering materials handling work performed during soiled linen collection, and therefore, there are no regulatory standards for linen bag volumes or weights from a lifting safety perspective. While some linen bag manufacturers’ instructions may recommend filling bags no more than 50% to prevent bag rupture or excessively heavy bags, most bags are not labelled individually or marked with a maximum filling line, limiting the communication of manufacturer recommendations to all end-users of these bags in hospital work environments.
The purpose of this investigation was to evaluate materials handling work performed during healthcare linen collection from an ergonomic perspective, while also taking into consideration the infection control implications of hospital linen handling and the demands unique to hospital work environments. In this study, we applied the Revised National Institute for Occupational Safety and Health (NIOSH) Lifting Equation (1, 11) to estimate Recommended Weight Limits (RWLs) for manual handling of linen bags during bag transfers into a pneumatic chute system from trolleys in waste collection rooms, where linen bags from patient care areas are collected. Our hypothesis was that in the absence of specific controls, the 32-gallon capacity currently permitted for linen collection receptacles might permit filling of liner bags to weights greater than our estimated RWL for some lifting positions and types of bag contents.
Methods:
Institutional Review Board (IRB) approval was obtained prior to data collection for this study from the Harvard T.H. Chan School of Public Health IRB (#15–0709) and the Partners Human Research Committee (#2015P000188).
Work Area Measurements
Members of the research team visited eight linen and waste collection rooms connected by a pneumatic chute system at one academic medical center in order to obtain work area measurements and observe work processes. The bag handling task studied in this analysis consisted of the transfer of bags from a bulk collection trolley into the access door of a pneumatic chute system in a waste and linen collection room (Figure 1). During this task, linen bags were transferred one by one out of the collection trolley and into the chute system by a worker specifically trained in the use of the chute system. Bags in the bulk collection trolley had been previously filled and brought there by other hospital staff responsible for cleaning patient rooms and other care areas.
Figure 1.
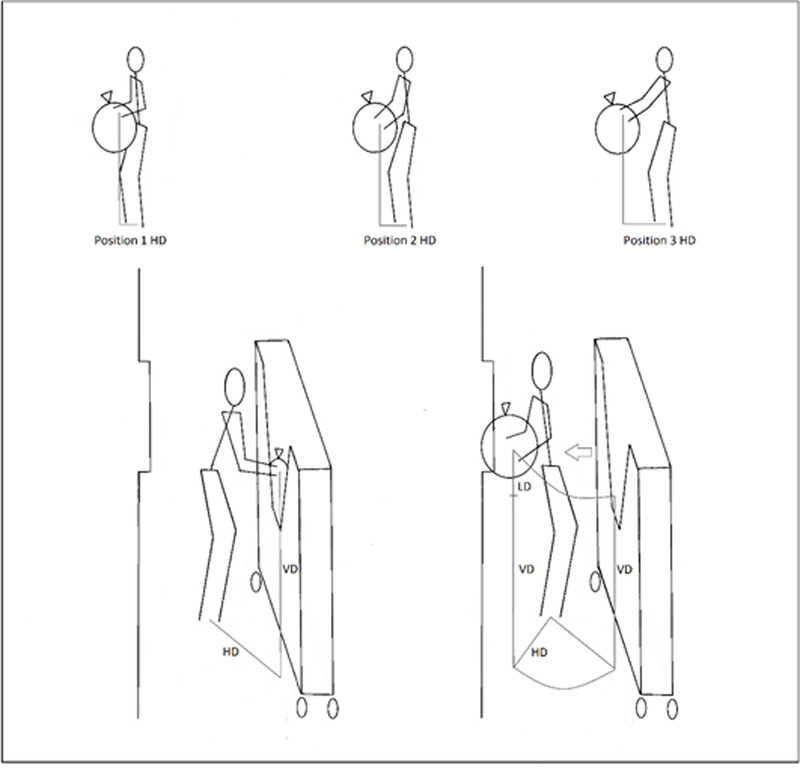
Work process schematic depicting bags transfers from the collection trolley to the pneumatic chute door. Measurements shown are for horizontal distance (HD); vertical distance (VD); and lift distance (LD). Elbow extension (Position 3) results in an increase in HD compared to varying degrees of elbow flexion (Positions 1 and 2), which bring the lifted object closer to the body.
In each waste collection room, collection cart and linen chute opening heights were measured using a digital Bosch DLR130 Laser Distance Measurer (Bosch, Farmington Hills, MI). Chute opening heights were measured from the bottom of the chute door opening to the floor. Collection cart opening heights were measured from the open edge of the wedge-shaped opening on the front of each cart. The mean height of the chute door opening measured in the eight collection rooms was 38.4 ± 2.4 inches (mean ± standard deviation). The mean height of the wedge-shaped bulk collection trolley opening was 36 ± 2.4 inches.
Linen Measurements
In order to estimate the possible range of linen bag weights that might be encountered during bag transfer work, we measured the weight per volume of the following types of linen items: sheets, gowns, and towels. We used an Extech Digital Force Gauge (Model 475055, Extech Instruments, West Nashua, NH), which can measure up to 220 pounds (lbs), with a margin of error of 0.1 lbs. Representative linen items of each type were weighed while dry, partially wet, and fully wet. Fluid saturation conditions were defined as immersion of either 50% of the item (partially wet) or the entire item in water (wet), followed by wringing out twice so that fluid was not actively dripping from the material before weighing.
Linen weights per volume were measured for unfolded single items using a 6-gallon clear plastic bin (Model 17191004, Sterilite Corporation, Townsend, MA) with volumetric markings on all four sides at one-liter intervals. Volumes were measured first by loosely placing individual items in the marked container (loose) and then by tightly compacting the items by pressing each down into the container using a rigid 9.5 × 12 inch folder to uniformly compress each item (compacted).
All weight and volume measurements were repeated five times for individual linen items of the three types: sheets, gowns, and towels. Clean linen items were obtained for measurement from a hospital linen vendor (Angelica Corporation, Somerville, MA). Weight per volume measurements were then used to calculate bag weight estimates according to filling proportions for linen collection bags of sizes 10-, 30-, and 40-gallons.
Recommended Weight Lift Limit Calculations
Recommended Weight Limits (RWL) were calculated using the Revised NIOSH Lifting Equation: RWL = LC * HM * VM * DM * AM * FM * CM, where LC is the load constant, 51 lbs, which is the recommended weight lift limit under ideal conditions; HM is the horizontal multiplier; VM is the vertical multiplier; DM is the distance multiplier; AM is the asymmetry multiplier; FM is the frequency multiplier; and CM is the coupling multiplier (1, 11).
Work area measurements obtained to determine these multipliers are depicted in Figure 1. The value of each multiplier used in the Revised NIOSH Lifting Equation ranges between 0 and 1, based on the work area measurements for a given lifting task, which are then matched with multiplier values in the reference tables provided in the Applications Manual for the Revised NIOSH Lifting Equation (1, 11). Optimal lifting conditions have multiplier values closer to one, while lifting conditions that are not biomechanically favorable will have values less than one and reduce the overall RWL.
Based on work observations and discussions with workers who regularly perform bag transfer tasks, the Frequency Multiplier (FM) was assigned as 0.84 for four bag lifts per minute and continuous lifting task duration less than one hour (1, 11). The Asymmetry Multiplier (AM) for the studied task was assigned as 0.86 based on 45° body rotations during lifting. Linen bags in all work areas were made of heavy duty plastic, and bags were gripped at the top or sides, without specialized grips. Therefore, the Coupling Modifier (CM), which reflects the quality of the grips on the lifted object, was assigned as 0.90.
During bag transfers, workers may hold the bags at different horizontal distances (HD), depending on arm position (Figure 1). Positions in which lifted objects are held close to the body are considered to be optimal and are associated with higher multiplier values. Three different arm positions during lifting were considered in our task analysis: lifting with the bag held close to the body in an ideal biomechanical position to maximize the RWL (Position 1); lifting with the elbows in a mid-flexion position, somewhat reducing body contact but not keeping the bag as far as possible away from the body (Position 2); and lifting with the bag held at a maximal distance away with the arms in full extension, as the bag might be held to avoid body contact with the bag (Position 3) (Figure 1). We then compared our estimated RWLs with predicted bag weights for different bag volumes and filling conditions.
In order to estimate the range of possible horizontal lift distances for a diverse workforce, we estimated the HD range using anthropometry data reported in the Centers for Disease Control (CDC) Vital and Health Statistics Series 11 from 2007–2010 (13). We used the reported mean male and female upper arm lengths for all United States racial and ethnic groups for the 25th, 50th, and 75th percentiles to calculate predicted forearm and full arm lengths, based on the size ratio for the bones of the upper arm (humerus) and forearm (ulna). For these calculations, we used a humerus: ulna length ratio of 1.22 which was reported by Pietak et al. based on examination and measurement of 46 sets of human upper limb bones (14). Maximum horizontal reach distance by percentile was calculated as the sum of the upper and forearm lengths using the following equation: total arm length = upper arm length + (upper arm length/1.22). Based on the upper arm length percentiles reported by the CDC for all racial and ethnic groups, the calculated arm lengths for the 25th to 75th percentiles: 12 – 13 inches (forearm) and 27 – 29 inches (full arm) for males and 11 – 12 inches (forearm) and 25 – 27 inches (full arm) for females.
These calculated arm lengths were then used to define the horizontal distances (HD) used to calculate RWL ranges for lifts in the three different positions: Position 1, bag held as close to the body as possible, HD = 10 inches; Position 2, bag held in mid-position, elbows slightly bent, HD = 17 inches; and Position 3, bag held maximally away, elbows extended, HD = 25 inches.
Given that bags may be collected from varying starting heights, depending on the fullness of the collection trolley in the waste staging area, RWL calculations were performed for a range of possible starting lift heights, corresponding to bag transfers from the bottom of the collection trolley (vertical lift starting height = 20 inches), at the level of the trolley opening (vertical lift starting height = 35 inches), and from a position with the bags piled above the trolley opening (vertical starting lift height = 50 inches). All lifts were assumed to have the same end-lift height of 40 inches, just above the mean height measured for the chute opening (mean chute opening height = 38.4 ± 2.4 inches).
Analysis
Chute height and cart measurements for the eight collection rooms were recorded during work area visits. Linen weight and volume measurements were obtained using multiple (n = 5) clean linen items of each type and repeated for each item after a standardized water saturation protocol. Data were recorded and all calculations were performed using Microsoft Excel.
Results
Linen Measurements
Mean linen weights per volume ranged from 0.44 – 0.51 lbs/gallon for loose, dry items of different types, while weights for compacted, dry items ranged from 1.14 – 1.46 lbs/gallon. When fully saturated with water, linen item weights increased between 2.7 – 4.3 times, resulting in wet weights per volume of 1.64 – 3.43 lbs/gallon and 3.56 – 4.59 lbs/gallon, for loose and compact wet items, respectively. The mean weights per volume averaged across the three item types were the following: 0.48 lbs/gallon for dry loose linen; 1.26 lbs/gallon for dry compact linen; 2.08 lbs/gallon for partially wet compact linen; and 4.03 lbs/gallon for wet compact linen. Table 1 presents the mean individual weights and weights per volume for linen items of each type.
Table 1.
Dry and Wet Single Item Weights and Weights per Volume
| Item | Dry Weight (lbs) |
100% Wet Weight (lbs) |
Loose Weight per Volume (lbs/gallon) |
Compact Weight per Volume (lbs/gallon) |
||||
|---|---|---|---|---|---|---|---|---|
| Dry | 50% Wet | 100% Wet | Dry | 50% Wet | 100% Wet | |||
| Sheet | 1.1 ± .03 | 3.3 ± .14 | 0.5 ± .03 | 1.3 ± .16 | 3.1 ± .61 | 1.1 ± .14 | 2.2 ± .42 | 3.6 ± .69 |
| Gown | 0.9 ± .02 | 2.4 ± .07 | 0.5 ± .05 | 0.9 ± .05 | 1.6 ± .17 | 1.5 ± .33 | 2.1 ± .58 | 3.9 ± .82 |
| Towel | 0.6 ± .03 | 2.6 ± .32 | 0.4 ± .04 | 1.4 ± .15 | 3.4 ± .79 | 1.2 ± .05 | 1.9 ± .23 | 4.6 ± .74 |
| Mean | - | - | 0.48 | 1.21 | 2.71 | 1.26 | 2.08 | 4.03 |
Recommended Weight Lift Limit and Bag Weight Calculations
Figure 1 depicts the bag transfer task and the distances used to calculate RWL values. Table 2 presents the distance measurements, multiplier values, and RWL for each arm position and starting lift height. Depending on the starting lift height, the RWL range for Position 1 lifts (bag held as close to the body as possible) was 28 – 32 lbs; the RWL range for Position 2 lifts (elbows partially but not fully extended) was 17 – 19 lbs; and the RWL range for Position 3 lifts (bag held as far from the body as possible) was 11 – 13 lbs. For subsequent comparisons with bag weight predictions, the lower bounds of these RWL intervals for each arm position were used as the RWL for the task, since transferring bags from the collection carts might require starting lift heights at, below, or above the collection cart opening.
Table 2.
Recommended Weight Lift Limits (RWL) in pounds, by arm position and starting lift height according to the Revised National Institute of Occupational Safety and Health Lifting Equation (1). For all calculations, Asymmetry Multiplier (AM) = 0.86; Frequency Multiplier (FM) = 0.84; Coupling Multiplier (CM) = 0.90.
| Lift starting below cart opening height |
Lift starting at cart opening height |
Lift starting above cart opening height |
|||||
|---|---|---|---|---|---|---|---|
| Vertical distance (VD) and Lift distance (LD) (inches) |
VD | LD | VD | LD | VD | LD | |
| 20 | 20 | 35 | 5 | 50 | 10 | ||
| Vertical Multiplier (VM) and Distance Multiplier (DM) |
VM | DM | VM | DM | VM | DM | |
| 0.93 | 0.91 | 0.96 | 1.00 | 0.85 | 1.00 | ||
| Arm position during lift | Horizontal Multiplier (HM) |
Recommended Weight Lift Limit (pounds) |
|||||
|
Position 1 Bag held as close to the body as possible (HD = 10 inches) |
1.00 | 28 | 32 | 28 | |||
|
Position 2 Bag held in mid-position, elbows slightly bent (HD = 17 inches) |
0.59 | 17 | 19 | 17 | |||
|
Position 3 Bag held maximally away, elbows extended (HD = 25 inches) |
0.40 | 11 | 13 | 11 | |||
Lower bound RWL values were compared to the predicted bag weights for 10-, 30-, and 40-gallon soiled linen collection bags filled to varying proportions with dry loose linen (0.48 lbs/gallon); dry compact linen (1.26 lbs/gallon); partially wet compact linen (2.08 lbs/gallon); and wet compact linen (4.03 lbs/gallon) (Figure 2). Bags filled with loose dry linen remained within the lower bound RWL for all filling proportions only for lifts with the bag held as close to the body as possible (Position 1). Notably, the predicted weight for a 30-gallon bag filled with dry compact linen exceeded the RWL for all arm positions for bags filled to greater than half capacity, and 30-gallon bags filled with partially wet items were within the RWL for lifts as close to the body as possible only when no more than one-quarter filled. Bags filled with completely wet items exceeded the calculated RWL for all arm positions for 30-gallon bags even when less than one-quarter filled.
Figure 2.
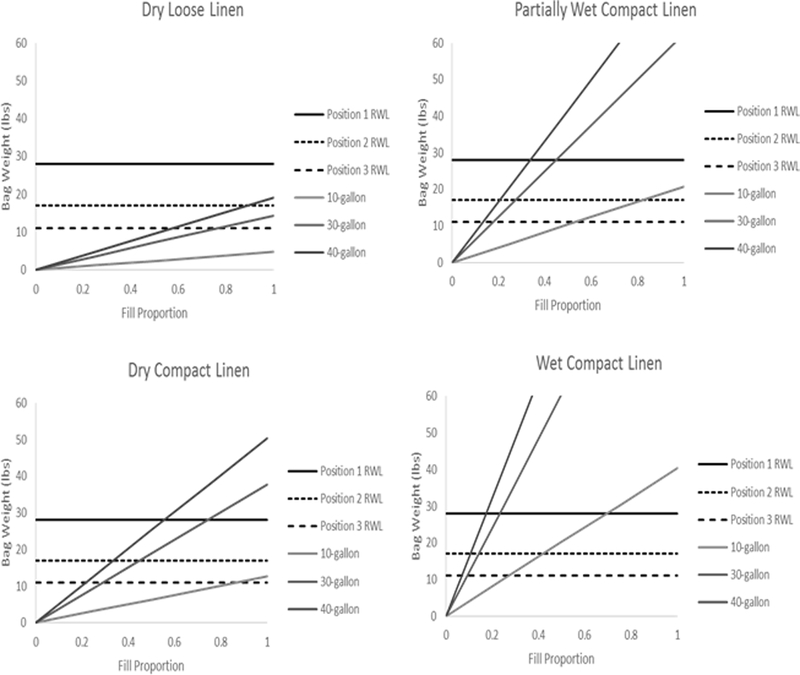
Predicted Bag Weights by Contents and Fill Proportion versus Recommended Weight Limits (RWL) by Arm Position
Discussion
For the bag transfer task studied in this analysis, we found that 30- and 40-gallon bags filled with loose dry linen remained within the lower bound RWL for all filling proportions only for lifts with the bag held as close to the body as possible. We also found that the predicted weights for 30- and 40-gallon bags filled more than halfway with dry compact linen exceeded our calculated RWL for all lifting positions. For perspective, 17 lbs was the estimated RWL for lifting a bag with the arms held slightly away from the body but not with the elbows fully extended. This would be the weight of a 30-gallon bag filled slightly less than halfway with compact dry linen or a 30-gallon bag filled approximately one-quarter with partially wet compact linen. Notably, bags filled with compact wet linen exceed the 17 lb RWL even when less than one-quarter full. These results suggest that where linen bags require manual handling for collection, specific limits on linen hamper volume, filling proportion, compacting of hamper contents, and handling of wet linens may be considered to ensure that linen bags are not excessively heavy.
The NIOSH Lifting Equation was originally formulated as an approach to help identify ergonomic interventions to decrease physical stresses during manual lifting tasks and thereby reduce rates of occupational low back injuries. In 1981, NIOSH published the Work Practices Guide for Manual Lifting which described a method for calculating recommended weight limits for symmetric, two-handed lifts (15). In 1993, the Revised NIOSH Lifting Equation was published as an update to this method and included added factors in the equation to account for lift asymmetry and grip quality (1, 11, 16, 17). To calculate a relative estimate of the physical stress associated with a given lifting task using the Revised NIOSH Lifting Equation, the Lifting Index (LI) is calculate as the load weight for a task divided by the RWL (1, 11). A previous cross-sectional study of 677 workers at nine industrial sites found that the odds of low back pain were significantly increased among workers performing manual lifting tasks where the calculated LI was greater than 1 and less than or equal to 3 (18).
As noted in the Applications Manual for the Revised NIOSH Lifting Equation, the equation was designed to be used as part of a comprehensive approach to preventing work-related low back injury, and as such, the recommended weight lift limits derived from the equation are not considered to be individually validated. The consideration of materials handling tasks using the Revised NIOSH Lifting Equation, however, is intended to highlight opportunities to improve lifting safety, rather than to set specific quantitative weight limits. The RWL values determined in this study therefore represent only estimates, rather than specific weight limits for the task studied (1).
Notable limitations of the current study include the focus of our analysis on only a single materials handling task in the sequence of linen collection and the need for further research to investigate bag weights and individual work processes in varying clinical environments. The work practices of patient care staff responsible for filling linen bags prior to their transfer to central collection areas also remain to be investigated. The RWLs estimated in this study also do not account for the additional manual tasks performed by workers whose jobs include, but are not limited to soiled linen bag handling work. Future studies investigating bag weight ranges in varied clinical settings, individual differences in body positions during task performance, and linen collection work organization are needed to identify effective approaches for reducing bag weights and enhancing lifting safety during healthcare linen collection. Outside of waste accumulation areas, nurses, aides, environmental services staff, and other healthcare providers use linen collection hampers, but many of these healthcare staff will never lift these bags and may not be aware of how heavy bags can become when filled with compressed or wet items.
In the hospital linen bag handling task studied in this analysis, holding the bag close to the body during lifting presents the most straightforward approach for increasing the RWL. However, one further consideration that must also be noted is that this position brings the bag into close proximity to the body and may place workers at risk for sharps injuries (7) and/or contact with infectious or other hazardous materials if the bag tears or if its exterior has been contaminated (2, 3). Infection and biohazard control issues are therefore a specific and necessary component of the lifting task under study, in addition to body mechanics. Whether used healthcare linen is visibly soiled or not, it requires special handling using appropriate personal protective equipment. The contents of soiled linen bags may be contaminated with bacteria, viruses, or parasites such as lice (4, 5). These organisms can remain infectious for extended periods, with gram-negative species such as E. coli and P. aeruginosa reported to survive up to four hours on fabric surfaces and gram-positive species such as S. aureus and and C. difficile found to survive on fabrics for days to months (5).
Avoiding contact with contaminated linen items during bag handling is essential for preventing transfer of pathogens onto workers’ skin and clothing which can then be inadvertently transferred onto surfaces outside waste storage areas (5). Highlighting the need for further study of contact transfer of pathogens in healthcare settings, a 2012 study of surface contamination in the general environment in three hospitals in Ontario, Canada identified the presence of five unique methicillin resistant S. aureus (MRSA) strains and eight C.difficile ribotypes in cultures from blood pressure machines, isolation carts, glove box holders, chair backs, and hand rails, among other locations (19). While a 1986 study of soiled linen and waste bags from patient isolation rooms reported comparable rates of positive surface cultures for the exterior surfaces of both single- and double-bagged waste and soiled linen, a significant limitation of that study was that cultures in this study were obtained after bags were set outside patients’ rooms, not after the bags had been manipulated repeatedly or stacked in collection trolleys with other bags that might be torn or spilled (20).
Limiting the weight of linen collection bags so that these can be lifted at a distance from the body presents one opportunity within soiled linen hygiene protocols for reducing surface contact transfers during manual bag handling, in addition to the need to control bag weights to reduce the risk of musculoskeletal injuries. The results of this analysis suggest that specific controls on linen hamper filling may be helpful to ensure that linen bags are not excessively heavy. Further studies are needed to fully characterize variations in soiled linen collection practices across different healthcare facilities and to identify effective interventions that promote efficiency and safety in healthcare linen collection work.
ACKNOWLEDGEMENTS:
This research was supported by Grant No. 2 T42-OH008416–09 from the National Institute for Occupational Safety and Health (NIOSH) and NIH/NIAMS: T32AR055885, K24AR057827, and P60AR47782 and financial contributions from Harvard University and its affiliated academic healthcare centers. The content is solely the responsibility of the authors and does not necessarily represent the official views of Harvard University and its affiliated academic health care centers, the National Center for Research Resources, the National Institutes of Health, or NIOSH.
Footnotes
Conflict of interest statement: the authors have no conflicts of interest to disclose related to the content of this manuscript.
References
- 1.Waters TR, Putz-Anderson V, Garg A. Applications Manual for the Revised NIOSH Lifting Equation. Cincinnati, OH: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute of Occupational Safety and Health, Division of Biomedical and Behavioral Science; 1994. Available from: http://www.cdc.gov/niosh/docs/94-110/pdfs/94-110.pdf. [Google Scholar]
- 2.Handorean A, Robertson CE, Harris JK, Frank D, Hull N, Kotter C, et al. Microbial aerosol liberation from soiled textiles isolated during routine residuals handling in a modern health care setting. Microbiome 2015;3:72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Fijan S, Turk S. Hospital textiles, are they a possible vehicle for healthcare-associated infections? Int J Environ Res Public Health 2012;9(9):3330–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ziady LE, Small N. Prevent and control infection Cape Town: Juta Academic; 2004. viiiii i.e. viii , 264 p. p. [Google Scholar]
- 5.Bloomfield S, Exner M, Flemming HC, Goroncy-Bermes P, Hartemann P, Heeg P, et al. Lesser-known or hidden reservoirs of infection and implications for adequate prevention strategies: Where to look and what to look for. GMS Hyg Infect Control 2015;10:Doc04. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Henderson R Industry Employment and Output Projections to 2024 Bureau of Labor Statistics; 2015.
- 7.Lakbala P, Azar FE, Kamali H. Needlestick and sharps injuries among housekeeping workers in hospitals of Shiraz, Iran. BMC Res Notes 2012;5:276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Salwe K, Kumar S, Hood J. Nonfatal occupational injury rates and musculoskeletal symptoms among housekeeping employees of a hospital in Texas. J Environ Public Health 2011;2011:382510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Caring for Our Caregivers: Facts About Hospital Worker Safety 2013.
- 10.National Healthcare and Social Assistance Agenda for Occupational Safety and Health Research and Practice in the United States Healthcare and Social Assistance Sector National Institute of Occupational Safety and Health; 2013. [Google Scholar]
- 11.Waters TR, Putz-Anderson V, Garg A, Fine LJ. Revised NIOSH equation for the design and evaluation of manual lifting tasks. Ergonomics 1993;36(7):749–76. [DOI] [PubMed] [Google Scholar]
- 12.Standards FAQ Details: Containers - Hazardous Areas The Joint Commission; 2016.
- 13.Fryar CD, Gu Q, Ogden CL. Anthropometric reference data for children and adults: United States, 2007–2010. Vital Health Stat 11 2012(252):1–48. [PubMed] [Google Scholar]
- 14.Pietak A, Ma S, Beck CW, Stringer MD. Fundamental ratios and logarithmic periodicity in human limb bones. J Anat 2013;222(5):526–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Work Practices Guide for Manual Lifting Cincinnati, OH; 1981. Report No.: DHHS (NIOSH) Publication No 81–122. [Google Scholar]
- 16.Waters T, Putz-Anderson V, Garg A. Applications Manual for the Revised NIOSH Lifting Equation Cincinnati, OH: United States Department of Health and Human Services, Centers for Disease Control and Prevention; 1994. [Google Scholar]
- 17.Waters T, Putz-Anderson V, Garg A, Fine L. Revised NIOSH equation for the design and evaluation of manual lifting tasks. Ergonomics 1993;36(7):749–76. [DOI] [PubMed] [Google Scholar]
- 18.Waters TR, Lu ML, Piacitelli LA, Werren D, Deddens JA. Efficacy of the revised NIOSH lifting equation to predict risk of low back pain due to manual lifting: expanded cross-sectional analysis. J Occup Environ Med 2011;53(9):1061–7. [DOI] [PubMed] [Google Scholar]
- 19.Faires MC, Pearl DL, Ciccotelli WA, Straus K, Zinken G, Berke O, et al. A prospective study to examine the epidemiology of methicillin-resistant Staphylococcus aureus and Clostridium difficile contamination in the general environment of three community hospitals in southern Ontario, Canada. BMC Infect Dis 2012;12:290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Maki DG, Alvarado C, Hassemer C. Double-bagging of items from isolation rooms is unnecessary as an infection control measure: a comparative study of surface contamination with single- and double-bagging. Infect Control 1986;7(11):535–7. [DOI] [PubMed] [Google Scholar]