

Abstract
Tenofovir is a nucleotide reverse transcriptase inhibitor, a commonly prescribed antiretroviral as part of initial therapy. It is widely used and has been recognized as a cause of acquired Fanconi syndrome, a disorder characterized by renal tubular dysfunction, which leads to hypophosphatemia, hypokalemia, and metabolic acidosis, as well as symptoms of polyuria and dehydration, which can ultimately lead to defects in bone mineralization and increase risk of fracture.
We describe a 14-year-old girl with a perinatal HIV infection who developed Fanconi syndrome as a result of tenofovir treatment and subsequently sustained bilateral hip and wrist fractures.
The goal of this case report is to raise awareness of the adverse drug complications that can occur in pediatric patients treated for HIV infection.
With tenofovir cessation and management of Fanconi syndrome, the bone recovers its ability to repair and remodel. A careful patient evaluation, including and suspicion of adverse drug complications, is essential for proper management and prevention of fractures in patients with HIV infection treated with antiretroviral medications.
History
A 14-year-old Chilean girl presented with a perinatal HIV infection diagnosed at age 6 years. She came from a rural environment. She had deceased parents and a poor support network.
At the age of 12, genotyping was performed, which showed resistance to three drugs. The patient began therapy with abacavir, Kaletra, and tenofovir, with good adherence and tolerance.
After 1 year on treatment, she presented with generalized weakness, lower extremity pain, functional impotence, swallowing disorder, and loss of muscle mass. Neurologic assessment by neuromuscular pathology was negative.
She was evaluated by a nephrologist. Laboratory results showed hypercalciuria, hypophosphatemia, creatinine elevation, and metabolic acidosis and bone densitometry demonstrated osteoporosis (z-score 3−4.2). Fanconi syndrome and secondary osteoporosis were diagnosed; treatment was initiated with bicarbonate, vitamin D, and phosphorus.
On admission, laboratory results showed renal dysfunction, hypophosphatemia, and an elevated alkaline phosphatase level. Radiographs showed bilateral hip (Figure 1) and wrist (Figure 2) fractures.
Figure 1.

Pelvic radiograph demonstrates bilateral femoral neck fracture.
Figure 2.

Radiographs of the wrist demonstrating bilateral wrist fracture.
Proximal renal tubular dysfunction, consistent with Fanconi syndrome, most likely secondary to tenofovir and bilateral hip and wrist fractures, was diagnosed.
Multidisciplinary management was started, her tenofovir therapy was interrupted, and her antiretroviral medication was changed. She was rehydrated with intravenous fluids and was started on calcitriol and calcium phosphate. The vitamin D level was corrected.
The hip fractures were treated with closed reduction and internal fixation with 3- and 5-mm locking compression proximal femur plates (Figure 3). The wrist fractures were managed with closed reduction and a cast.
Figure 3.
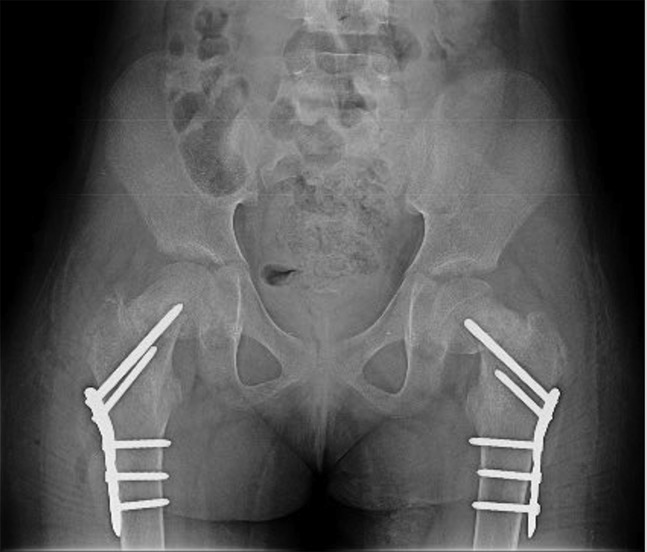
Pelvic radiograph demonstrates reduction and fixation with locking compression proximal femur plate.
The patient's symptoms rapidly improved, with resolution of generalized bone pain and fatigue.
After a month, the laboratory results were normal. The patient also increased weight and improved her nutritional status.
She was left without weight bearing for 8 weeks; after 4 weeks of follow-up, she had no hip pain.
At 8 weeks, we observed the wrist and hip fractures healing (Figure 4). At 10 weeks, we observed remodeling of the hip fractures (Figure 5). The patient returned to previous functional status.
Figure 4.

Wrist radiograph 8 weeks after fracture, demonstrating healing and remodeling.
Figure 5.

Pelvic radiograph 10 months after fracture. Bone remodeling is evident.
Discussion
Metabolic bone disorders are common in patients with HIV infection, and many patients have premature osteoporosis and an increased risk of fracture.1
Tenofovir, an antiretroviral medication, is classified as a nucleotide reverse transcriptase inhibitor that prevents the action of the enzyme reverse transcriptase required for HIV viral production.2 Tenofovir has been associated with an adverse reaction known as Fanconi syndrome, which can lead to osteomalacia.3,4,5,6,7
Rebolledo et al8 described bilateral pathologic hip fracture secondary to tenofovir treatment in a 54-year-old patient with HIV infection. To our knowledge, there has been no reported case of pathologic fractures secondary to tenofovir treatment and Fanconi syndrome in the pediatric population.
Hussain et al9 describe a case of Fanconi syndrome in a 12-year-old child with perinatal HIV infection while on tenofovir, lopinavir-ritonavir, and didanosine.
We describe here the first report of bilateral pathologic hip and wrist fracture and Fanconi syndrome secondary to tenofovir treatment in the pediatric population.
Fanconi syndrome and pathologic fracture are uncommon complications, even more so in the pediatric than in older populations. The renal complication from tenofovir should be anticipated and must be suspected in the presence of weight loss, polyuria, polydipsia, dehydration, and generalized bone pain.
Routine biochemical monitoring, including serum calcium, phosphate, bicarbonate, creatinine, glucose, vitamin D levels, and plasma and urine electrolytes, should be part of in the evaluation of all patients with HIV infection taking antiretroviral medications.
If any sign of tubulopathy develops, tenofovir should be stopped,10 and multidisciplinary management focused on bone metabolism, kidney function, and antiretroviral treatment correction should be started. With tenofovir cessation and management of Fanconi syndrome, the bone recovers its ability to repair and remodel.
In conclusion, careful evaluation of patients and suspicion of adverse drug complications are essential for proper management and prevention of fractures in HIV-infected patients being treated with antiretroviral medications.
Footnotes
The authors have no conflicts of interest to disclose.
References
- 1.Prior J, Burdge D, Maan E, Milner R, Hankins C, Klein M, Walmsley S: Fragility fractures and bone mineral density in HIV positive women, 2007 fractures and bone mineral density in HIV positive women: A case-control population based study. Osteoporos Int 2007;18:1345–1353. [DOI] [PubMed] [Google Scholar]
- 2.Fung HB, Stone EA, Piacenti FJ: Tenofovir disoproxil fumarate: A nucleotide reverse transcriptase inhibitor for the treatment of HIV infection. Clin Ther 2002;24:1515–1548. [DOI] [PubMed] [Google Scholar]
- 3.Verhelst D, Monge M, Meynard J, et al. : Fanconi's syndrome and renal failure induced by tenofovir: A first case report. Am J Kidney Dis 2002;40:1331–1333. [DOI] [PubMed] [Google Scholar]
- 4.Earle KE, Seneviratne T, Shaker J, Sboback D: Fanconi's syndrome in HIV1 adults: Report of three cases and literature review. J Bone Miner Res 2004;19:714. [DOI] [PubMed] [Google Scholar]
- 5.Clarke BL, Wynne AG, Wilson DM, Fitzpatrick LA: Osteomalacia associated with adult Fanconi's syndrome: Clinical and diagnostic features. Clin Endocrinol (Oxf) 1995;43:479–490. [DOI] [PubMed] [Google Scholar]
- 6.Wanner DP, Tyndall A, Walker UA: Tenofovir-induced osteomalacia. Clin Exp Rheumatol 2009;27:1001–1003. [PubMed] [Google Scholar]
- 7.Perrot S, Aslangul E, Szwebel T, Caillat-Vigneron N, Le Jeunne C: Bone pain due to fractures revealing osteomalacia related to tenofovir-induced proximal renal tubular dysfunction in a human immunodeficiency virus-infected patient. J Clin Rheumatol 2009;15:72–74. [DOI] [PubMed] [Google Scholar]
- 8.Rebolledo BJ, Unnanuntana A, Lane JM: Bilateral pathologic hip fractures associated with antiretroviral therapy: A case report. J Bone Joint Surg Am 2011;93:e78. [DOI] [PubMed] [Google Scholar]
- 9.Hussain S, Khayat A, Tolaymat A, Rathore MH: Nephrotoxicity in a child with perinatal HIV on tenofovir, didanosine and lopinavir/ritonavir. Pediatr Nephrol 2006;21:1034–1036. [DOI] [PubMed] [Google Scholar]
- 10.Barrios A, Benayas-Garcia T, Gonzalez-Lahoz J, Soriano V: Tenofovir- related nephrotoxicity in HIV-infected patients. AIDS 2004;18:960–963. [DOI] [PubMed] [Google Scholar]