

Supplemental Digital Content is available in the text.
Abstract
Objective:
To improve oral rehydration therapy (ORT) after discharge for children presenting to the emergency department (ED) with acute gastroenteritis (AGE).
Methods:
We designed and implemented a quality improvement initiative to improve caregiver adherence to ORT in children 6 months to 21 years old with AGE. The intervention consisted of ORT “kits” with rehydration supplies and caregiver instructions. In the preintervention period we monitored patient/caregiver adherence to ORT recommendations and additionally monitored ORT kit and educational material distribution during the intervention phase via a caregiver survey after discharge. We utilized statistical process control methodology to assess responses to the intervention. As a balancing measure, we monitored the ED length of stay for patients with AGE.
Results:
Over the study period from November 2013 to April 2015, we included 174 encounters during the preintervention period and 256 encounters during the intervention period. More than 9 of 10 children received ORT kits in the intervention period. Self-reported adherence to ORT between the 2 time periods remained constant. The ED length of stay did not change between the preintervention and intervention period.
Conclusions:
Despite successful distribution of novel ORT materials and education for caregivers of children with AGE in a pediatric ED, caregiver self-reported adherence to ORT postdischarge visit was unchanged. An unexpected high baseline adherence to ORT practices may have limited improvement.
INTRODUCTION
Studies in a variety of health care settings, including the emergency department (ED), indicate that instructions for home care after medical treatment are often not effectively communicated to patients and their caregivers,1,2 and this can result in adverse medical events and unnecessary return visits.3,4 Acute gastroenteritis (AGE) is among the most prevalent conditions treated in pediatric EDs.5 Oral rehydration therapy (ORT) is widely regarded as the most effective means of rehydrating most pediatric patients with AGE and can be done effectively at home.6,7
In our ED, we follow a local evidenced-based guideline with recommendations based on the Center for Disease Control endorsed by the American Academy for Pediatrics.8 Clinicians follow these guidelines supporting ORT over intravenous hydration. However, we do not routinely provide formalized caregiver education for ORT during the visit, as providers are often unable to devote adequate time to the comprehensive step-by-step instruction of ORT. As a result, we observed that caregivers often did not follow ORT practice while in the ED examination room, which raised concerns that suboptimal ORT could also lead to poor adherence to basic ORT principles after the ED visit. We thus hypothesized that provision of a patient-directed rather than clinician-taught intervention including detailed paper-based educational materials on how to administer ORT plus an ORT “kit” would improve adherence to ORT by patients/caregivers post-ED visit.
METHODS
Setting
We conducted this improvement initiative in an ED of an urban tertiary academic pediatric medical center with an annual volume of approximately 60,000 visits per year. The department is divided into 5 care teams of physicians, nurses, and clinical assistants. Each team consists of 1–2 attending and trainee physicians, 2–3 nurses, and 1 clinical assistant.
Study Design
A quality improvement (QI) initiative was developed using the Model for Improvement approach9 to increase caregiver adherence to best ORT practices both during and after the ED visit. This work met criteria for QI activities exempt from IRB review at Boston Children’s Hospital.
Patient Cohort
Patients between 6 months and 21 years old presenting to the ED with chief complaint of either vomiting or diarrhea consistent with AGE who were subsequently discharged from the ED were eligible. We excluded patients if they had a complex medical history (such as diabetes mellitus, ventriculoperitoneal shunt presence)10 or if they were non–English speaking.
Data Collection
We identified all children with an ED diagnosis of vomiting, diarrhea, or gastroenteritis (International Classification of Diseases, 9th Revision Clinical Modification [ICD-9-CM] 558.9, 787.03, 787.91, 787.01, 009.0) from the hospital’s data warehouse. An electronic list was generated daily of all patients seen the prior day and then was manually reviewed by study investigators (MS/SP) to identify patients who met inclusion criteria. Families of patients with AGE were called by trained research coordinators within 72 hours of ED visit to survey caregivers/patients with 2 goals in mind, the first to assess the clinical condition of the patient and the second to assess adherence to ORT at home. A clinician was made available within 1 hour of a call to address any medical concerns from the patient/caregiver. Families were surveyed for 16 weeks leading up to the initiative and for 32 weeks of the intervention phase.
INTERVENTIONS
Planning the Intervention
Although there were instructions for use at home recommending administration of ORT to a child with AGE before the improvement effort, there were no paper-based detailed ORT instructions given to families during their ED visit. Also, there were rudimentary ORT supplies consisting of a plastic bag with a cup and straw that accompanied the rehydration fluids. To begin the improvement effort, we assembled a team consisting of 2 ED physicians, 2 ED nurses, a quality consultant, and interested parents. Key stakeholders were convened to discuss the barriers to distribution. A further discussion was focused on development of a step-by-step oral rehydration flow diagram and improved educational materials for use in the ED and for caregivers to take home after the visit. Stakeholders agreed that because the clinical staff felt they were not able to allocate sufficient time for comprehensive caregiver training in ORT steps, caregiver activation and self-direction would be the focus of this improvement initiative.
Key Drivers
We identified several key drivers outlined in a driver diagram (Fig. 1). The key drivers were improved understanding of the process of care of AGE in the ED, increasing parental comfort with the care of AGE while in the ED and improving satisfaction with care of AGE in the ED. Change strategies to support the key drivers were the following: (1) Development of new ORT supplies with fluid administration implements, paper-based step-by-step pictorial flow diagram on how to orally hydrate, and AGE-specific educational handouts including information on anti-emetic medication. (2) Engagement of ED staff including buy-in by ED nurses using Plan, Do, Study, Act (PDSA) cycles to distribute the materials to the caregivers to engage and activate. Using these changes strategies we developed 2 main interventions focused on the improvement of staff engagement: the new ORT supplies with educational materials, and education and adherence of patient/caregivers to ORT.
Fig. 1.
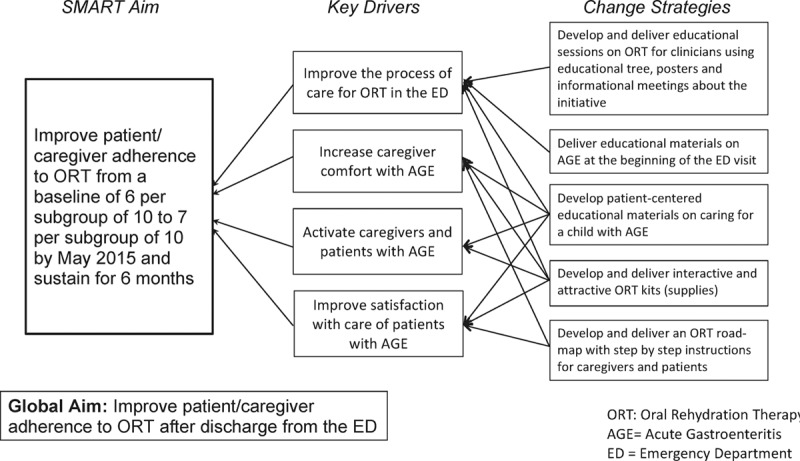
Key driver diagram: improving patient and caregiver adherence to oral rehydration therapy after discharge.
Development of ORT Materials
We developed refined ORT kits that included age-appropriate ORT materials. One developed for patients ≤2 years old included a syringe, medicine cup, and sippy cup (not available prior in our ED), whereas the second for patients >2 years old included straw and paper cup placed in visually appealing packaging. We also included age appropriate rehydration fluid. Also, we developed 2 paper-based handouts with AGE-specific education for patients and caregivers adapted from the preexisting instructions, and they were edited by hospital-based education staff to be at a fifth-grade reading level. (See figure, Supplemental Digital Content 1, http://links.lww.com/PQ9/A3). To develop the instructions, we engaged stakeholders through an iterative process with input from ED doctors, nurses, and caregivers on readability and usability. Using the same iterative approach, we added a flow diagram with pictures that outlined the model visit for a patient with AGE, emphasizing correct ORT technique while in the ED. Each kit costs approximately $0.75, with the highest cost attributed to the “sippy cups.” For the process measure, we determined the number of eligible patients receiving ORT materials over time.
Engagement of ED Personnel
We engaged ED providers in improvement through a structured process (the Pathman model of implementation [awareness, agreement, adoption, and adherence]).11 This included an introductory email and recurring educational sessions to reach a majority of clinical staff including nurses, clinical assistants, and doctors. Also, we used a local education “tree” that has been used successfully in the past in our ED for individualized in-person education and buy-in to include nurses who may have missed formal educational sessions.12 ED providers received periodic email reminders throughout the intervention phase. The nursing staff was integral to the process as they were the frontline staff handing out the new ORT kits and activating caregivers to use them. After the decision to perform ORT had been made, nurses were asked to deliver the ORT supplies. Before this intervention, there was no formal process of delivery of ORT materials. For the intervention phase, nurses were asked to deliver the kits to all eligible patients; caregiver instruction was at the discretion of the bedside nurse.
Using PDSA methodology, we increased nurse accessibility to ORT materials, added signs in patient rooms to further activate patients and caregivers, placed engaging posters throughout the department encouraging provider delivery, and gave verbal and visual reminders to use the supplies. We also added modifications to the ORT educational handouts acknowledging that patients or caregivers may receive a follow-up phone call to increase the response rate to follow-up calls.
Measurement of Patient/Caregiver Response to the Intervention
We designed a survey with branching logic for patients/caregivers asking about their child’s condition, the ED experience, and adherence to ORT within 72 hours after their ED visit. Research coordinators attempted to contact 5 patients per day who met inclusion criteria. The survey was also designed to ask about receipt of and satisfaction with ORT handouts. The survey tool was created in consultation with a survey methodologist, key stakeholders, and families, and focused on anticipated care at home. The survey also addressed caregiver comfort with managing gastroenteritis and overall satisfaction with the ED visit. The survey was piloted with 10 patients and families and modified through an iterative process for understandability and ease of use (See figure, Survey Tool, Supplemental Digital Content 2, http://links.lww.com/PQ9/A4). To measure adherence to ORT recommendations, we created a composite score of 4 questions. Each was equally weighted; one point was given for each response in alignment with the ORT handouts distributed. We then dichotomized the results to adherent or nonadherent. Patient/caregiver answers were defined as adherent if any question was answered in alignment with the information distributed, whereas they were categorized as nonadherent if no questions were answered in alignment with the instructions. More specifically, caregivers were first asked whether the patient recently seen in the ED had emesis after the visit. If they had emesis, there was an opportunity to try ORT at home. Subsequently, they were asked questions regarding volume, the timing of ORT, and diet at home. They were deemed adherent if they answered one of the questions correctly. We were not specific about the amount of emesis. This was designed to be sensitive to any success of the caregiver/patient-directed care.
Caregivers were additionally asked to rate the value of the educational handouts, satisfaction with care while in the ED, and their comfort with caring for the patient with AGE at home also on a 6-point Likert scale. We opted for a 6-point Likert scale as it has been shown to have increased discrimination without change in reliability for results. We knew a priori we would dichotomize results and a 6-point scale decreases the likelihood of a neutral response.13
The survey was validated using face validity ensuring the questions were associated with handouts given while in the ED. Also, we examined construct validity reviewing the information with content experts and caregivers through an iterative process of the questions relating to the ORT materials.
Outcome and Process Measures
Our primary outcome was the number of patients with AGE reporting adherence to ORT at home. Adherence was measured using the telephone survey administered within 72 hours of the visit to caregivers of children with AGE. Secondary outcomes included percent of caregivers’ rating of satisfaction as reported during the telephone survey. Lastly, we measured the rate of return visits that led to admission for all patients with AGE compared with the rate for patients in the intervention period.
Our primary process measure was the number of patients or caregivers in each subgroup reporting receipt of the ORT kit with paper-based instructional materials. Our balancing measure was the mean ED length of stay for patients discharged with AGE to insure that the change in care did not adversely affect ED throughput.
Data Analysis
We compared demographic characteristics of patients/caregivers (age, sex, and educational level [higher than high school, less than high school and declined]) in the preintervention and intervention periods for both the population we were able to survey by phone. We obtained similar data for control patients we were unable to reach to assess for possible bias in the surveyed group. The medians were compared for the demographical data as it was not normally distributed and evaluated using chi-square analysis. Regarding adherence, the analysis was limited to patients who vomited at home because the improvement objective was primarily to address patients with ongoing vomiting. The demographical data and adherence composite score were generated and analyzed using STATA13 (StataCorp LP, College Station, Tex.). We used statistical process control charts for analysis of the outcomes and process measures. We used NP-charts to display results. NP-charts are a type of control chart used when there are nonconforming units in a sample. They can be used instead of P-charts, which use proportions.14 Each subgroup consisted of 10 sequential successfully completed phone surveys. We found that use of NP-charts supported interpretation of the data when there was variability in recruitment over time. These charts were used to display caregivers/patients reporting (1) adherence to ORT recommendations; (2) satisfaction with educational materials; (3) comfort of caring for the child at home; and (4) eligible patients who received the intervention.
It is notable that during our study period, there was an interruption in research coordinator availability leading to a gap in data collection from July to November 2014.
RESULTS
During the preintervention and intervention periods from November 2013 to April 2015, 2432 pediatric patients had one or more of the selected ICD-9 diagnoses. Of these, 697 patients were excluded based on non-English primary language or complex medical history. Of the remaining eligible patients, 1305 could not be reached at follow-up by phone either due to missing or inaccurate contact information or due to 2 unsuccessful attempts. Of the remaining cases, 174 patients or caregivers were contacted in the preintervention phase and 256 patients or caregivers during the intervention. There was no difference in the age, gender, or educational level of the population surveyed compared with those we were unable to contact. There was no statistical difference in age of the population surveyed between the preintervention and intervention periods. The level of education for caregivers was “greater than high school” in both the pre- and postperiods at 54.5% and 59.8%, respectively (Table 1).
Table 1.
Patient Demographics: Preintervention and Intervention Phases

For the primary outcome, there was no change in adherence to ORT over the course of the intervention (Fig. 2), with an average of 7 of 10 caregivers adhering to ORT recommendations over the entire period. For secondary outcomes, satisfaction with the educational handouts reached 81% after dichotomizing responses. We found the rate of return to the ED leading to hospitalization for the population surveyed was 0.46%, compared with that of all patients with AGE, which was 1.7%.
Fig. 2.
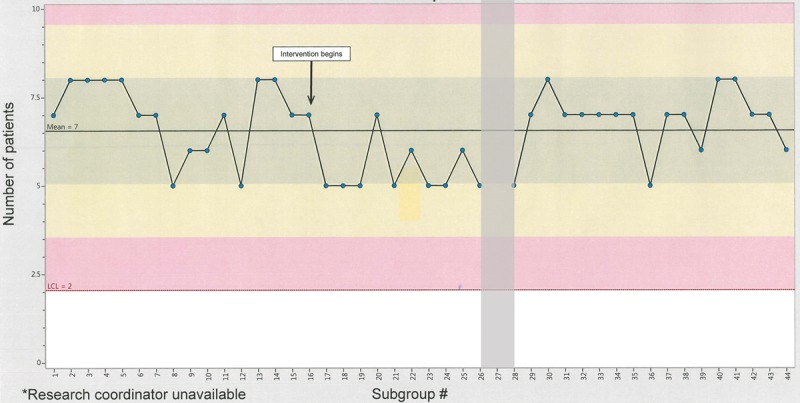
NP chart of the number of patients/caregivers adhering to ORT recommendations after discharge. *Research coordinator unavailable during the shaded interval.
Delivery of ORT supplies to patients and caregivers increased from 6 to 9 of 10 caregivers in each subgroup (Fig. 3).
Fig. 3.
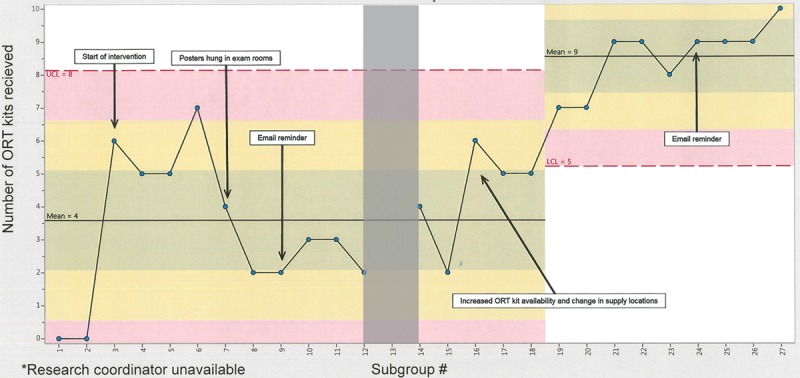
NP chart of the number of patients/caregivers reporting receipt of ORT kits per 10 consecutive patients reached after discharge. *Research coordinator unavailable during shaded interval.
As a balancing measure, there was no change in the median length of stay of patients with AGE discharged from the ED during the preintervention and intervention time periods at 159 and 166 minutes (P = 0.64), respectively.
DISCUSSION
We implemented a QI initiative to (1) improve the rates at which ORT supplies are provided for children with uncomplicated AGE in the ED, and (2) test the hypothesis that providing diagnosis-specific detailed “how-to” and educational materials during the ED visit would improve adherence to ORT at home.
We demonstrate that we were able to successfully dispense ORT kits to patients with AGE in a busy tertiary care pediatric ED. A key feature of our implementation strategy is the successful utilization of the Model of Improvement framework with iterative input from all key stakeholders, including caregivers.9 In addition to contributing to the redesign of the ORT kits and educational materials, this team identified lack of awareness and inefficient obscure placement of materials as barriers to distribution. Thus, we relocated ORT supplies to high traffic areas close to patient rooms. Meetings were held with physicians, nursing staff, and clinical assistant staff to review enhancements in the materials and location for ease in disbursement and utilization. Although this helped in initial weeks of implementation, the rate of distribution initially remained less than 60% of eligible AGE patients. To better understand this lagging response, the team resurveyed the nursing staff and learned that access was a persistent barrier. Therefore, the locations were further optimized. The improvement team was simultaneously increasing informal conversations with nurses and nurse educators during clinical shifts regarding the potential added value. These 2 main PDSA cycles improved “buy-in” and efficiency, which was fundamental to process improvement. This second round of changes led to more eligible patients receiving supplies. An additional strategy for enhancing delivery of kits was parent activation by alerting caregivers of patients with AGE that ORT kits were available by signs posted in the examination rooms, although we were unable to quantify this.
Despite achieving the goal of delivery of the intervention, we were not able to increase the rate of self-reported adherence to ORT at home, our main outcome. The baseline self-reported adherence to ORT was high, which may be tied to the high education level of the population served in our ED.15 Almost 60% of the caregivers had at least a high school education. It also may represent reluctance of caregivers to report a lack of adherence. Social desirability bias, the tendency of survey respondents to answer questions in a manner that will be viewed favorably, may have played a role. The surveys were completed by phone and therefore were confidential but not anonymous.16 We chose this approach to allow caregivers to ask questions and check on the clinical condition of the patient. Finally, implementation of other QI initiatives has included scripted discussions as part of the improvement, and our efforts may have benefited from this approach. A global health study focused on the distribution of oral rehydration solution and direct education to parents on ORT, which successfully increased its use.17 Given time constraints elicited by providers at the brainstorming sessions, we specifically chose a patient-directed intervention. This choice allowed us to test a possible approach in our ED and to determine its value as an improvement strategy. Although the scripting may have changed our rates of adherence, a review of ORT efforts in a community setting did find differences in adherence when mothers were exposed to mass media campaigns.18 In this case, we learned that adherence was likely high at baseline, but this approach might benefit from being tested in a less educated population. Another approach would be development of video instructions that could be shown during the ED ORT period.
The self-reported satisfaction with ORT educational materials was approximately 81%, which can be considered satisfactory in an ED setting. Ratings of overall satisfaction for emergency care are commonly lower than those for other healthcare environments, likely due to the unanticipated need for emergency care, the anxiety of caregivers and lack of a preexisting relationship with providers,19 among others. Engel et al.20 observed that patients have difficulty remembering their medical care in the ED soon after leaving, including trouble recalling specifics about their diagnosis and care. We surveyed the care provider within 3 days after being seen in the ED. We hoped that the ORT kits and written educational materials, taken home, would serve as a robust physical reminder postvisit.
One limitation was the difficulty contacting caregivers within 72 hours leading to a possible sampling bias. However, there was no difference in the ability to reach caretakers between the preintervention and intervention periods. There are 2 main reasons why we missed some caregivers. First, as this was a QI project, the caregivers/patients were contacted as follow-up to their clinical visit. Although our registration team makes substantial efforts to obtain accurate contact information, some phone numbers may have been inaccurate or went unanswered. We considered patient emails, but email addresses were not obtained reliably at intake during the study period. Future considerations include texting, emailing, or a website for families.
Hospital-based QI efforts are often met with the challenging task of improving complex processes with multiple stakeholders. Iterative input from a diverse stakeholder team including members of the nursing and clinical care staff was critical for identifying and overcoming these barriers. Our experience, similar to other attempts to improve care in other large academic medicine centers, points to a need to robustly engage nursing and clinical care staff in both the planning and implementation of QI initiatives and to carefully consider the educational level and novel contact strategies for caregivers.
CONCLUSIONS
We developed and implemented a QI initiative that included delivery of novel ORT kits to patients and caregivers with AGE to increase adherence to ORT after the ED visit. Despite successfully implementing the intervention, a high level of self-reported preintervention adherence to ORT after discharge may have precluded the ability to demonstrate improvement in our outcome.
DISCLOSURE
The authors have no financial interest to declare in relation to the content of this article.
Footnotes
Supplemental digital content is available for this article. Clickable URL citations appear in the text.
REFERENCES
- 1.Kripalani S, Jackson AT, Schnipper JL, et al. Promoting effective transitions of care at hospital discharge: a review of key issues for hospitalists. J Hosp Med. 2007;2(5):314–323.. doi:10.1002/jhm.228. [DOI] [PubMed] [Google Scholar]
- 2.Vashi A, Rhodes K V. “Sign right here and you’re good to go”: a content analysis of audiotaped emergency department discharge instructions. Ann Emerg Med. 2011;57(4):315–322.e1.. doi:10.1016/j.annemergmed.2010.08.024. [DOI] [PubMed] [Google Scholar]
- 3.Hastings S, Barrett A, Weinberger M, et al. Older patients’ understanding of emergency department discharge information and its relationship with adverse outcomes. J Patient Saf. 2011;7(1):19–25.. doi:10.1097/PTS.0b013e31820c7678. [DOI] [PubMed] [Google Scholar]
- 4.Grover G, Berkowitz C, Lewis R. Parental recall after a visit to the emergency department. Clin Pediatr (Phila). 1994;33(4):194–201.. [DOI] [PubMed] [Google Scholar]
- 5.Elliott E. Acute gastroenteritis in children. BMJ. 2007;334:35 doi:10.1136/bmj.39036.406169.80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.King C, Glass R, Bresee J. Center for Disease Control and Prevention. Managing acute gastroenteritis among children: oral rehydration, maintenance, and nutritional therapy. MMWR Recomm Rep. 2003;21(52):1–16.. [PubMed] [Google Scholar]
- 7.Bellemare S, Hartling L, Wiebe N, et al. Oral rehydration versus intravenous therapy for treating dehydration due to gastroenteritis in children: a meta-analysis of randomised controlled trials. BMC Med. 2004;2(1):1–8.. doi:10.1186/1741-7015-2-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.King CK, Glass R, Bresee JS, Duggan C. Managing acute gastroenteritis among children: oral rehydration, maintenance, and nutritional therapy. MMWR Recomm Rep. 2003;52(RR-16):1–16.. [PubMed] [Google Scholar]
- 9.Langley G, Moen R, Nolan K, et al. The Improvement Guide: A Practical Approach to Enhancing Organizational Performance. 20092nd ed San Francisco: Jossey-Bass. [Google Scholar]
- 10.Feudtner C, Christakis DA, Connell FA. Pediatric deaths attributable to complex chronic conditions: a population-based study of Washington State, 1980–1997. Pediatrics. 2000;106(1 Pt 2):205–209.. doi:10.1542/peds.106.1.S1.205. [PubMed] [Google Scholar]
- 11.Pathman D, Konrad T, Freed G, et al. The awareness-to-adherence model of the steps to clinical guideline compliance: the case of pediatric vaccine recommendations. Med Care. 1996;34(9):873–889.. [DOI] [PubMed] [Google Scholar]
- 12.Akenroye AT, Stack AM. The development and evaluation of an evidence-based guideline programme to improve care in a paediatric emergency department. Emerg Med J. 2016;33:109–117.. doi:10.1136/emermed-2014–204363. [DOI] [PubMed] [Google Scholar]
- 13.Chomeya R. Quality of psychology test between likert scale 5 and 6 points. J Soc Sci. 2010;6(3):399–403.. doi:10.3844/jssp.2010.399.403. [Google Scholar]
- 14.Cheung Y, Jung B, Sohn JH, et al. Quality initiatives: statistical control charts: simplifying the analysis of data for quality improvement. RadioGraphics. 2012;32(7):2113–2126.. 10.1148/rg.327125713. [DOI] [PubMed] [Google Scholar]
- 15.Lowe DA, Monuteaux MC, Ziniel S, et al. Predictors of parent satisfaction in pediatric laceration repair. Acad Emerg Med. 2012;19(10):1166–1172.. doi:10.1111/j.1553-2712.2012.01454.x. [DOI] [PubMed] [Google Scholar]
- 16.Ong AD, Weiss DJ. The impact of anonymity on responses to sensitive questions. J Appl Soc Psychol. 2000;30(8):1691–1708.. doi:10.1111/j.1559–1816.2000.tb02462.x. [Google Scholar]
- 17.Sengupta P, Mondal SK, Ghosh S, et al. Review on development and community implementation of oral rehydration therapy. Indian J Public Heal. 1994;38(2):50–57.. [PubMed] [Google Scholar]
- 18.Lenters LM, Das JK, Bhutta ZA. Systematic review of strategies to increase use of oral rehydration solution at the household level. BMC Public Health. 2013;13(Suppl 3):S28 doi:10.1186/1471-2458-13-S3-S28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Trout A, Magnusson AR, Hedges JR. Patient satisfaction investigations and the emergency department: what does the literature say? Acad Emerg Med. 2000;7(6):695–709.. doi:10.1111/j.1553–2712.2000.tb02050.x. [DOI] [PubMed] [Google Scholar]
- 20.Engel KG, Buckley BA, Forth VE, et al. Patient understanding of emergency department discharge instructions: where are knowledge deficits greatest? Acad Emerg Med. 2012;19(9):E1035–E1044.. doi:10.1111/j.1553-2712.2012.01425.x. [DOI] [PubMed] [Google Scholar]