

Abstract
Introduction:
Given the aging population, it is necessary to develop strategies for the prevention and promotion of mental health in the elderly. Hope as the ability to trace and maintain paths can be used as a key construct for these strategies, promoting cognitive health if stimulated.
Objective:
Evaluate the behavior and cognitive development of elderly people through hope training as a clinical strategy for health promotion.
Methods:
A clinical experiment with a comparative and cross-sectional design. There were 2 data collection phases over a 6-month period. The sample comprised 51 participants, divided into groups having received either more or less than 6 months of stimulation. The instruments used were the Mini-Mental State Examination (MMSE), Geriatric Depression Scale (GDS), and Expectations/Hope Scale About the Future and Life's Guidance. The Wilcoxon signed-ranks test (t test) was used to analyze the data.
Results:
Hope in addition to cognitive stimulation shows more significant results in elderly people at initial stimulation (0.18), mainly at the permanence and troubleshooting on the paths concerned; this corresponds with the results obtained for hope (0.18). Depressive symptomatology showed significant differences among the 2 groups (0.39 and 0.02). In the between-groups comparisons, only GDS showed significance (0.46).
Hope training has an impact on the remission of depressive symptoms and, despite increased hope levels, training was effective for the reduction of depression symptoms for up to 6 months, thereafter only playing a maintenance role. Broadly, hope has been shown to promote elderly people's mental health.
Keywords: cognitive stimulation, elderly people, hope, mental health
1. Introduction
Nowadays, there is a vast range of research seeking to deconstruct not only theoretically, but most of all socially, an understanding of aging as a stage of life marked by loss. Classical academic works such as Cheik and collaborators,[1] Neri,[2] and Baltes,[3] have not evaluated the argument that aging must be understood as a biopsychosocial phenomenon that defines an individual and the totality of his/her existence in society. Rather, aging is an irreversible process marked by individuals’ lived experiences and idiosyncrasies, subject to cultural particularities.
The experience of aging may arguably be determined by personality, family history, personal trajectory, and socioeconomic conditions.[2,3] Therefore, it entails dealing with positive events, but especially, negative events experienced throughout life, such as a spouse's death, loss of loved ones, declining health and physical functionality, loss of status social and prestige, retirement, experiencing violence, and accumulation of functions; these occur alongside the increasing proximity of death, among others. The results of these stressful situations may reflect on one's life, affecting physical, emotional, and social dimensions, and requiring the individual to develop cognitive abilities to approach events in a positive way.[4]
Unexpected health-related events, which occur most often in old age, require a great adaptive effort from one and challenge the individual's personality, orienting him/her to face challenges arising from an unwanted event and to psychologically and emotionally adjust, as this intensely affects people's emotional and cognitive resources. Successful adaptation entails meeting the demands of an event, which is an important indicator of an individual's resilience and hopefulness.[5]
Nowadays, constructs such as hope have been configured as 1 of the salient psychological variables in discussions about positive psychology. Positive psychology researchers affirm the existence of qualities that buffer one against mental illness, such as hope, optimism, resilience, ethics, and courage.[6]
The movement initiated by Seligman has surpassed the theoretical domain and is becoming increasingly intertwined with different application fields.[9] Psychological practice draws from the development of health-promoting abilities, personal growth, and motivation as ideal personal characteristics.[8,9] This perspective can enhance patient/client functioning.[7,10] This positive outlook seeks to impart constructs such as hope, the focus of this study. This study aims to evaluate cognitive and behavioral performance among the elderly through hope training, as a clinical strategy for the prevention of mental illness. This paper is a product of the postgraduate program in health sciences at ABC Paulista Medical School and forms part of the corresponding author's postdoctoral work, with co-operation of the Study Group on the Mental Health of the Elderly at the University of Pernambuco, linked to the National Council for Scientific and Technological Development (CNpq).
1.1. Hope
It has been years since the importance of hope in the understanding of human behavior was identified, but the development of instruments measuring hope only commenced in the last few years.[11] Hope can be defined as goal-directed thinking. It is characterized by the ability to find routes that lead to desired goals and thoughts, with the motivation needed to reach those routes.[12]
Hope can be learned, given the brain's ability to continually create new brain connections, referred to as neuroplasticity. However, learning thereof requires training, which, for example, involves turning to friends, believing that the world can be a good place, envisioning a future and having faith—whether in God, something greater, the government, or whatever it may be.[12] At another point, hope is not determined through heredity, as it is a fully learned configuration in relation to goal-directed thinking.[13]
Based on the definition of hope, it is clear that a hopeful outlook by individuals contributes significantly towards overcoming the difficulties and obstacles in daily life, whether in the family, work, school, or community environment. Nonetheless, any environment presents challenging situations. In these situations, hope can contribute towards steering action in the best possible way, helping individuals to maximize benefits for themselves.[13,14] This is because a sense of hope influences human behavior, determining how we approach events. Existing literature highlights the centrality of this phenomenon in determining the salience of other constructs, such as resilience, in challenging situations.[7,9,10]
Moreover, in relation to depressive disorder, individuals may have the unipolar or bipolar disorder. The first is characterized by mainly a depressed mood and anhedonia, in addition to psychosocial consequences. Bipolar depression may alternate with episodes of mania, where hyperthymia can lead to aggressive behavior and psychomotor agitation.[15,16]
Brain imaging studies indicate changes in the 2 types of depression mentioned above. The review by Serafini et al points to a reduction in the volume of the basal ganglia and hippocampus in unipolar depression in children, whereas in bipolar depression, the reduction is mainly in the corpus callosum, in addition to the increase in white matter hyperintensities.[15]
In the elderly, the review by Rozenthal et al shows changes in the basal ganglia, other than subcortical white matter, especially in the periventricular area, and thalamus anatomical changes in the frontal areas, mainly in the bilateral orbital cortex among elderly persons with unipolar and bipolar disorders. Microstructural changes in the white matter lateral to the anterior cingulate area are related to a decrease in the rate of emotional remission in the elderly with unipolar depression. This can be identified in elderly people with and without unipolar and bipolar depression and has a neurodegenerative effect that directly affects mood.[16]
Based on the above, our hypothesis is that hope as a cognitive and behavioral process, when stimulated, can go against these neurodegenerative changes, with neuroplasticity reinforcing new learning.
It is important to note that hope entails a cognitive process. The most accepted view in this regard is espoused by Snyder, Lehman, Kluck, and Mossone[17] and Snyder, Lopez, Shorey, Rand, and Feldman.[18] Thus, according to a widely used definition, hope is a cognitive process derived from a sense of agency with goal-oriented determination and successful paths, meaning that it entails planning in order for one to achieve proposed goals.[19]
Hope as a construct is based on realistic assessment of desires and means of accomplishing them. The construct entails 3 components, namely, an objective, routes, and agency.[20] First, the objective is related to the envisaged goal and must be sufficiently important for the individual to set. Second, routes refer to the ability to generate adequate paths to achieve the desired goal. Developing several routes is particularly important when barriers are interposed between the subject and the target. Third, agency is the motivational component that drives the search for the goal, using the routes, and must be present throughout the process, so that the subject feels constantly motivated to use the routes that he or she traced. The hypothesis emanating from this is that the production of routes and the agency relating to that is important for the prevention of depression in the elderly.
This is a cross-sectional and quantitative study. It is characterized as epidemiological and various measures were taken to represent facets of a phenomenon that participants experience subjectively and to examine its effects on them.[21] The phenomenon described here is the construct, hope. Given these characteristics, the study is a randomized, controlled, parallel, open, and 2-arm clinical trial.
The research also had a comparative aspect. A comparative study does not have a control group. So, in this study,[22] data were collected twice within a 6-month period, between April and October of 2017; the results obtained were compared. The 2 participant groups, which will be presented in the “Participants” section, were assessed through the same instruments and exposed to the training program.
Figure 1 presents the study design, which is discussed in detail in the sub-sections below.
Figure 1.
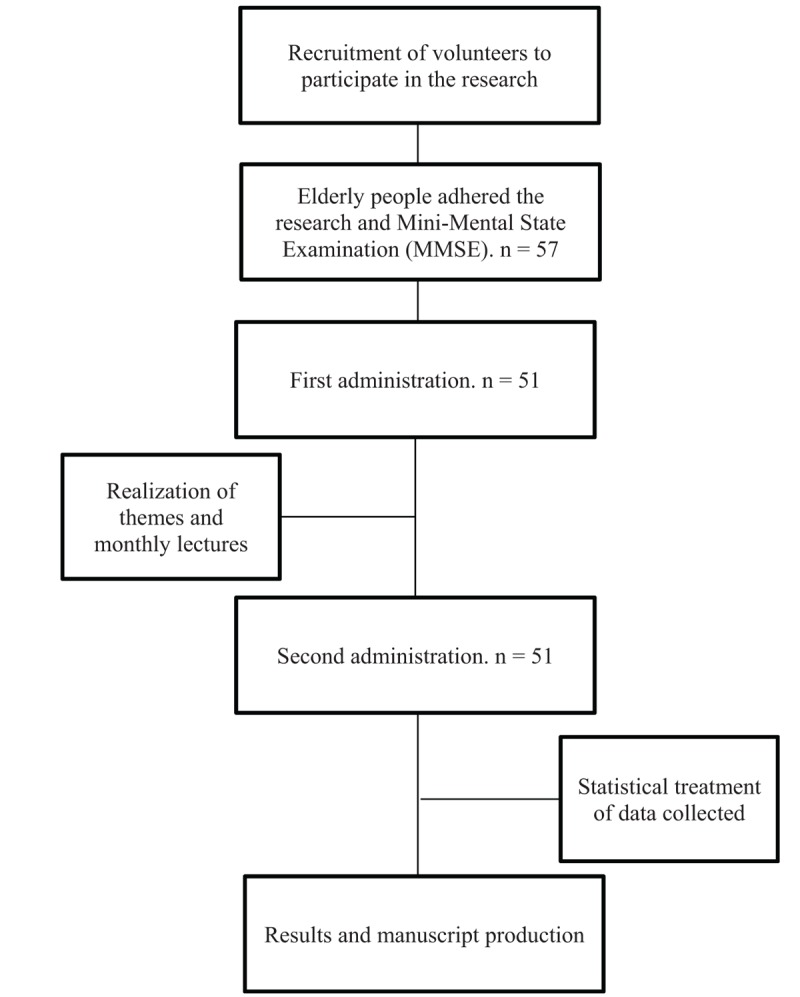
Study design flowchart.
1.2. Study setting
The research took place in a cerebral gymnasium (Metodo Supera Institution), where activities pertaining to neuropsychological rehabilitation and cognitive stimulation are carried out. The school is located in Boa Viagem, in the city of Recife, Pernambuco.
The study site was chosen due to the methodology used at the institution, ideal for presenting lectures on topics such as hope. With the mission of developing brain potential and stimulating thinking and action, the methodology used on Metodo Supera is governed by the following three principles: novelty, variety, and increasing challenge, all based on three pillars, namely, theories of learning, education, and neuroscience.
In addition to the usual classes, a topic was discussed each month, and each week, a new reflection relating to the monthly theme; this was an important feature for the study setting.
1.3. Participants
The inclusion criterion was being aged 60 years or more. Participation was voluntary. Of the 57 initial participants, 6 dropped out during the course of the study. Five prospective participants withdrew from the study and 1 fell ill. Forty-three of the participants were female, and 8 were male. The participants’ average age was 75 years and all had completed at least elementary education. Participants were divided into 2 subgroups, 1 comprising those who participated in the school activities for less than 6 months (n = 16), which we will call “Group 1,” and the other comprising those who had participated for more than 6 months (n = 35), which we will call “Group 2.” All participants attended the activities at the gymnasium assiduously during the study period.
1.4. Instruments
Participants underwent the Mini-Mental State Examination (MMSE) as an inclusion criterion for the study, to assess the level of cognitive impairment.[23] The instruments used to achieve the objectives of the present study were: Snyder's Expectations/Hope Scale About the Future and Life's Guidance, adapted by Ribeiro et al[24]; and the short version of the Geriatric Depression Scale (GDS), validated by Yesavage et al, in Brazil by Almeida and Almeida, and tested in studies by Paradela et al.[25–27]
The MMSE's items tap into spatial and temporal orientation, recall, calculation, attention, comprehension, and execution of instructions.[23] The short version of the GDS consists of 15 questions, to be answered with “Yes” or “No.” A score of ≥5 among the elderly indicates depression.[26]
Expectations/Hope Scale About the Future and Life's Guidance provides 3 scores: 1 on global hope, resulting from the sum of all 8 items; and scores for each of the 2 dimensions of hope, resulting from the total scores for all 4 items pertaining to a particular dimension of hope.[24]
The first factor of the Expectations/Hope Scale About the Future and Life's Guidance, initiative, is self-explanatory and deals with the capacity to take initiative in different situations that life imposes on us or that we set out to experience. The second, paths, is related to the capacity to remain steadfast through experiences while seeking resolutions and setting out to overcome adverse situations in our paths.[24]
In addition to assessments using the above-mentioned instruments, participants completed activities through our partnership with the research site. Our aim was to directly or indirectly incorporate the hope construct into the cognitive stimulation program, known as “cerebral gymnastics” at the study site, which was performed daily. In the intervals between the 2 data collection phases and along with the daily activities, monthly lectures were held.
Presumably, adding the hope construct to cognitive stimulation, which we call “hope training,” would enable neuroplasticity to facilitate the development of initiative and paths as aspects of hope among the elderly participants. In addition to the cognitive factors, also considering changes in the social scope of the elderly, having initiative and the ability to generate paths could also stimulate maintenance of their networks and life goals.
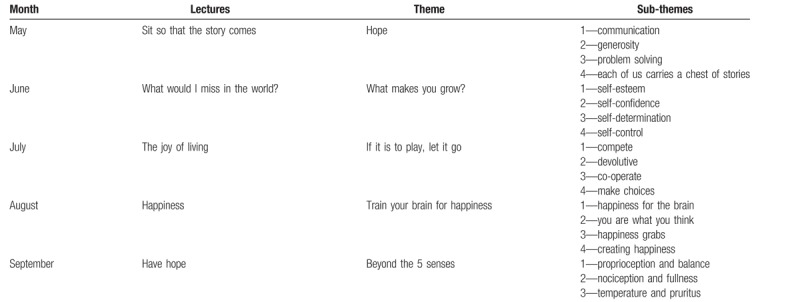
Monthly themes, divided into weekly sub-themes, were presented. All were directly or indirectly linked to hope and, broadly, positive psychology. The table below (Table 1) details the themes and sub-themes presented. The themes and sub-themes presented in the monthly lectures where incorporated in the daily activities at the institution
Table 1.
Lectures, themes, and sub-themes presented.
1.5. Data collection procedures
Data collection took place on the days of the elderly participants’ lectures, and the instruments were applied in the following order: MMSE, GDS, and Expectations/Hope Scale About the Future and Life's Guidance. The second data collection phase followed the same order, except for assessment using the MMSE.
1.6. Data analysis
The data collected were analyzed. Between-groups and within-groups differences were determined.
The Wilcoxon signed-ranks test (non-parametric analysis, NCSS), or t test,[28] were run, with 2 distinct samples paired and compared. Significance was set at 0.5.
The between-groups comparisons were conducted using data crossing. The data of the 2 groups were cross-checked to analyze the relationships between the study variables. This means that analyses were run on total scores on the GDS and the Expectations/Hope Scale About the Future and Life's Guidance, and on each of the latter's 2 factors, namely, initiative and paths.[29]
Those agreeing to participate in the study signed an informed consent form according to Resolution 466/2012.[30]
2. Results
Participants who had completed 5 to 8 years of schooling obtained an average score of 24.66 in the MMSE; this population had a cut-off point of 26.5. Fifteen participants who completed 9 to 11 years of schooling obtained a mean score of 25.28. The cut-off point for this population was 28. Thirty-three participants with >11 years of study obtained a mean score of 27.06 and a cut-off point of 29.
Although Group 1 and Group 2 obtained mean scores below the minimum expected on the MMSE, indicating signs of dementia, participants displayed clinical characteristics based on the extent of their exposure to the stimulation activities that they took part in at the research site. The group with less than 6 months in the cognitive stimulation program (Group 1) obtained a mean score of 26.77 on the MMSE, and the group with more than 6 months (Group 2), 24.56.
The results confirm those of previous studies, which state that cognitive stimulation after a certain period may improve the cognitive functions of elderly people.[31,32] The stimulation program at the research site spans a minimum period of 18 months, after which elderly participants presumably present with more enhanced cognition, due to maximum exposure to the program.
2.1. Group 1 results
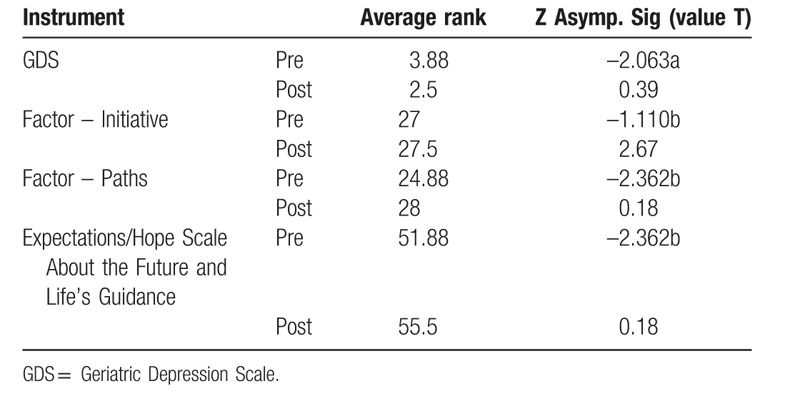
Group 1 obtained a mean score of 3.88 at first administration of the GDS and 2.5 at second administration. This yielded a significance level of 0.39 in the t test, pointing to the effectiveness of incorporation of the hope construct in the activities of the cognitive stimulation program. The highest and lowest scores on the 2 tests were, respectively, 9 and 8, and 1 and 0.
Hope, when stimulated, can benefit the cognitive, affective, and behavioral domains, which are other constructs of positive psychology; this observation supports the downward oscillation of the GDS scores.[9,24] Because depression blunts affect those affected by it,[25] high levels of hope can render it a strong ally in the treatment of depression.[26] This relationship is discussed further below.
Results regarding the Expectations/Hope Scale About the Future and Life's Guidance are presented based on scores on each of its 2 factors and the overall score.
Group 1's mean score on the first factor, initiative, was 27 at first administration; the maximum score was 32. A mean score of 27.5 was obtained at second administration. The t test yielded a value of 2.67, which does not indicate a substantial increase in the score on initiative.
Group 1 obtained a mean score of 24.88 and 28 on paths, the second factor of the Expectations/Hope Scale About the Future and Life's Guidance, at first and second administration, respectively. At a significance of 0.18, the result shows a greater probability that hope influences participants’ paths in various aspects of their lives, more than it does the initiative to take these paths. This result suggests that considering elderly people who received less than 6 months of cognitive stimulation, hope can facilitate individuals’ confrontation of most situations (the paths factor) than it can their initiative to take these paths.
Overall scores on the Expectations/Hope Scale About the Future and Life's Guidance were as follows: 51.88 and 55.5 out of a possible total of 64 at first and second administration, respectively. With a level of significance of 0.18, there was an apparent significant increase in the levels of hope, which supports studies indicating that hope is a learned construct that can be stimulated throughout life.[12,18] Moreover, because it is a construct that acts at the cognitive level, the theoretical link between hope and cognitive stimulation may have resulted in the increased levels of hope.
Table 2 presents the results discussed above.
Table 2.
Group 1's statistical results.
The results of the GDS and the Expectations/Hope Scale About the Future and Life's Guidance show an inversely proportional relationship, with a decrease in the scores on the former coinciding with an increase in the latter scores. Hopeful beliefs about the self and the future are often stimulated in psychotherapy for individuals with depression, along with strategies for maintaining social support networks; these tend to be effective.[33] In their review, Marback and Persoli found that hopelessness is 1 of the most recurrent symptoms in depressed patients, including those with suicidal ideation.[33] Thus, we could argue that there is a relationship between the variables.
2.2. Group 2 results
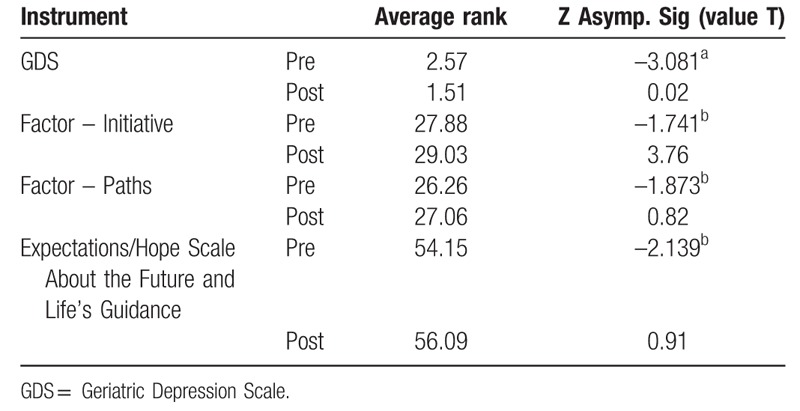
For Group 2, the GDS yielded scores of 2.57 and 1.51 at first and second administration, respectively. The t test yielded a value of 0.02, demonstrating a significant difference in the scores on this scale. As in Group 1, we argue that cognitive stimulation, along with hope training, facilitated a decrease in participants’ depressive symptomatology.
Scores of 27.88 and 29.03 at first and second administration, respectively, were obtained on the initiative factor of the Expectations/Hope Scale About the Future and Life's Guidance. The t test yielded a significance value of 0.82, indicating no significant difference; a similar result was obtained for Group 1. This result opens up the possibility of discussion about other constructs within positive psychology that influence initiative.
Mean scores of 26.26 and 27.6 were obtained for the paths factor, with a T level of 3.76. Notably, for Group 2, the results obtained for the factors did not show substantial increases, thereby demonstrating that elderly people who attend the cerebral gymnasium for a longer period display initiative and are more likely to follow their chosen paths, therefore justifying the non-expressive increase in scores. Hopeful people tend to make decisions and implement them faster and more meticulously, showing less vulnerability to frustrations.[17,18] The GDS results reinforce the above.
The mean score on the overall GDS for this group was 54.15 at first administration and 56.09 at second administration. The t test yielded a value of 0.91, showing no significance and confirming the lack of significant differences in the 2 factors’ scores when evaluated separately. Table 3 shows the results discussed above.
Table 3.
Group 2's statistical results.
The low mean GDS score and high punctuations shown by the Expectations/Hope Scale About the Future and Life's Guidance suggest that hopeful elderly people tend to have lower depressive symptomatology, regardless of the period of stimulation. However, older individuals with longer cognitive stimulation tend to have lower depressive symptoms and a higher expectation index, and therefore have a greater capacity to face adversities, initiate new challenges, and find solutions to problems.[33] Despite the lower scores, Group 1 also demonstrated lower depressive symptomatology and a high hope index. This issue will be expanded on in the next section.
2.3. Between-group comparisons
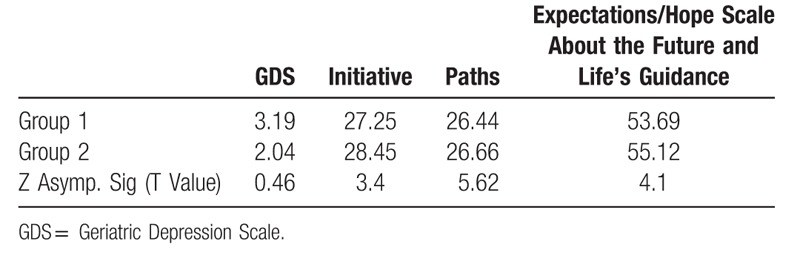
In the between-groups comparison for the GDS, the t test yielded a value of 0.46, indicating slight significance. Group 1's mean score was 3.19 and that of Group 2, 2.04. Therefore, we can conclude that, although no significant correlation between depression and hope has been shown, cognitive stimulation incorporating hope training serves more as a protective factor against depression among elderly participants receiving a minimum of 6 months of training, compared to those receiving less than 6 months of training.
A combination of these in treatment would enhance mental health, particularly in relation to depressive symptomatology within the first 6 months, thereafter mainly serving to maintain it. This was shown by the results obtained by the 2 groups, with Group 1 showing a decrease of 1.38 in the mean score on the GDS, and Group 2, a decrease of 1.06.
There was no correlation between the 2 factors of the Expectations/Hope Scale About the Future and Life's Guidance. Groups 1 and 2 obtained mean scores of 27.25 and 28.45, respectively, on the initiative factor. The t test yielded a value of 3.4. The lack of association shows that the capacity for initiative is not associated with hope training and the duration of cognitive stimulation.
We could, therefore, argue that initiative, which showed an increase in both groups, plays an active role only in the first few months of the intervention. This was shown by the significant differences between the scores obtained by Group 1 across the 2 tests, and the considerable increase in the initiative score for this group at second administration of the test. This observation is expected because the initiative factor predominates over the paths factor and is therefore essential.[24]
Group 1 obtained a mean score of 26.44 and Group 2, 26.66 for the paths factor. The t test yielded a value of 5.62. There was a slight difference of only 0.22 between the groups. The substantial increase in the scores of Group 1 across the 2 tests shows that the paths factor is strengthened among elderly people receiving cognitive stimulation for a shorter period. Along with the considerable increase in initiative, it is apparent that the greatest potential for plasticity with regard to hope is within the first few months of cognitive stimulation since, as previously mentioned, it is learned and new apprenticeship provides new neural connections. Recent literature points to the benefits of cognitive stimulation programs to enhance tolerance for frustration and problem-solving.[31,34] For this reason, an elderly person's change of position during problem-solving prompts flexibility and exertion of more effort. When you reach such a level in the Paths factor, the increasing level in this 1, we presume here a minimum time of 6 months, becomes less noticeable.
Total scores on the Expectations/Hope Scale About the Future and Life's Guidance were 53.69 for Group 1 and 55.12 for Group 2. The t test result yielded a value of 4.1, indicating no significant differences between the 2 groups, similar to the results obtained for each of the 2 factors. Table 4 summarizes the between-group comparisons.
Table 4.
Between-group comparisons of the scores.
We argue that the social aspect of the research site also contributed to the high levels of hope in both groups. Social support networks, ranging from family to institutions such as the 1 researched, provide support for the maintenance of an active social life, which promotes mental health in all its spheres. Hence, affect and cognition are constantly stimulated due to the motivational factor of socialization,[35] thereby promoting quality of life and buffering subjects against depressive symptomatology, as well as enhancing cognitive and behavioral factors such as hope, resilience, perseverance, and empathy.[2,5,36]
2.4. Limitations
The study included elderly people who had already undergone some cognitive stimulation programs, albeit for a short period. In addition, the small sample size does not allow for the results to be generalized. Therefore, the results can be used to inform future research in the field. The study did not have a control group and, therefore, the extent to which hope training can benefit elderly people who have never participated in such programs is unclear.
3. Conclusions
Some considerations could be formulated in view of the results and the initial objective of the research, which was to evaluate the cognitive and behavioral functioning of elderly people, based on hope training as a clinical strategy for mental illness prevention.
Some of the results corroborate those in studies on psychology and aging. First, participants undergoing a cerebral gymnastics program mostly obtained a low score on the GDS, which assessed depressive symptomatology before exposure to a program entailing hope training; exposure further reduced the symptomatology. Second, we suggest that an environment conducive to the formation of support networks promotes mental health.
We found that hope training facilitated better neuroplasticity among the elderly in the early stages of cognitive stimulation. The more experienced and trained a subject becomes in the construct, the fewer the cognitive and behavioral changes that occur. As shown by the significance of the t test results regarding the paths factor and the overall score on the Expectations/Hope Scale About the Future and Life's Guidance, Group 1 showed significant improvement, with a mean increase of 3.12 in both the factors mentioned in the overall scale. In existing literature, we found that cognitively strong elderly people have already reached acceptable levels of neuronal plasticity, and therefore learn faster, unlike those not receiving brain stimulation.[37] This corroborates the slightly higher scores obtained by Group 2, which received cognitive stimulation for more than 6 months.
Based on the above, we can conclude that hope as a facilitator of the paths to be carved by the elderly tends to be more effective if training therein is provided to individuals who do not habitually experience brain stimulation or have recently started doing so. This would preserve and promote mental health both in terms of cognition and behavior, and enhance persistence among individuals. The cognitive aspect is important because it acts as an agent of neuronal plasticity, facilitating new learning and coping ability, whereas behavioral strategies are important for producing healthy, proactive behaviors that promote good practices.
The plasticity resulting from learning hope opens the door for application in other domains. This stimulation can be extended beyond professional programs, to any activity that has the power to facilitate plasticity, and not least, psychotherapy.[38]
For elderly people who are in the habit of boosting their cognitive functions, hope is seemingly an ally in the maintenance of mental health. This was shown by Group 2's results, demonstrating sustained hopefulness, as shown by the slight improvement.
Due to this field being largely unexplored and the marginal quantitative results obtained, we cannot generalize the results and reflections from this study. For generalizability, there is a need for more studies with larger sample sizes. Another limitation of this study was the low control of the variables; moreover, we could not identify other factors that may have influenced the obtained scores, despite the hypotheses that emerged in the discussion of the results. For example, other constructs of positive psychology that correlates with hope, such as empathy and faith, may have somehow played a role. In addition, the 6-month time frame did not present significant changes in the scores on the Expectations/Hope Scale About the Future and Life's Guidance, raising questions as to whether a longer training period could yield more significant changes.
The results from this study and discussion thereof serve to prompt new research and training strategies aimed at enhancing not only hope but also other constructs in positive psychology. This research focuses on hope and its implications for behavior and cognitive processes, as a clinical strategy for the prevention of mental illness, as well as enhancement of mental health, along with hopefulness.
In conclusion, hopeful elders may tend to, at first, take initiative, pursuing their goals, and then remaining steadfast in their chosen paths or having the flexibility to change them in order not to deviate from them. It is important to consider that the elderly need to develop strategies for maintaining their mental health in an environment that often devalues this stage of their lives. Notwithstanding the physiological deterioration associated with old age, hope facilitates cognitive and behavioral reinforcement for elderly people, enabling them to face daily life. A training program enabling valid inferences from the quantitative results, and also generating qualitative improvement is of great importance.
Acknowledgments
We would like to express our immense gratitude to the Postgraduate Program at ABC Medical School. Dr. Hartmann-Júnior, JAS is a regular postdoctoral fellow in the area of collective health (2017–2018).
Author contributions
HJJAS was the researcher responsible for the research, active in all its stages. This is his postdoctoral research. FALAF, PKSCB, ALLL, QMFS, CMRC, and ARCT were involved in the 2 data collection phases, administering the instruments and analyzing the results. MAGAP was involved in the 2 data collection phases, administering the instruments and analyzing the results, and contributed towards the development of the manuscript. VCAC proofread the manuscript provided support throughout all the stages of the research. RNML was the supervisor of the main author's research, providing support in all the research stages and contributed towards the development and revision of the manuscript.
Conceptualization: José Antônio Spencer Hartmann Junior, Modesto Leite Rolim Neto.
Data curation: José Antônio Spencer Hartmann Junior, Modesto Leite Rolim Neto.
Formal analysis: José Antônio Spencer Hartmann Junior.
Investigation: José Antônio Spencer Hartmann Junior, Alina Laís Almeida de Farias Fernandes, Antônio Gabriel Araújo Pimentel de Medeiros, Keny Silva Castelo Branco Pinheiro, Lucyelli Luna Lopes de Amorim, Mariana Ferreira Silveira de Queiroga, Marianne Rodrigues Correia da Cruz, Rebeca Cristine Torres de Araújo.
Methodology: José Antônio Spencer Hartmann Junior, Antônio Gabriel Araújo Pimentel de Medeiros.
Project administration: José Antônio Spencer Hartmann Junior.
Resources: José Antônio Spencer Hartmann Junior.
Supervision: José Antônio Spencer Hartmann Junior, Carlos Augusto Carvalho de Vasconcelos, Modesto Leite Rolim Neto.
Validation: Modesto Leite Rolim Neto.
Visualization: Modesto Leite Rolim Neto.
Writing – original draft: Antônio Gabriel Araújo Pimentel de Medeiros.
Writing – review & editing: José Antônio Spencer Hartmann Junior, Carlos Augusto Carvalho de Vasconcelos, Modesto Leite Rolim Neto.
José Antônio Spencer Hartmann Júnior orcid: 0000-0002-6799-2599
Footnotes
Abbreviations: GDS = Geriatric Depression Scale, MMSE = Mini-Mental State Examination, t test = Wilcoxon signed ranks test.
The research was approved by the Research Ethics Committee, CAAE: 64997917.4.0000.5207. Because it is a clinical trial, the study was registered in the “Registro Brasileiro de Ensaios Clínicos” (ReBEC), with identification number RBR-4gh83t, with the link: http://www.ensaiosclinicos.gov.br/rg/RBR-4gh83t/
All data generated or analyzed during this study are included in this manuscript.
The authors declare that they have no competing interests.
This study received no financial contribution.
The authors have no conflicts of interest to disclose.
References
- [1].Cheik NC, Reis IT, Heredia RAG, et al. Efeitos do exercício físico e da atividade física na depressão e ansiedade em indivíduos idosos. Revista Brasileira de Ciência e Movimento 2003;11:45–52. [Google Scholar]
- [2].Neri AL, Freire SA. E por Falar Em Boa Velhice. 1st ed. Campinas: Papirus; 2000. [Google Scholar]
- [3].Baltes PB, Prefácio, Neri AL. Psicologia do envelhecimento: temas relacionados na perspectiva do curso de vida. Campinas: Papirus 1995. [Google Scholar]
- [4].Pinheiro DPN. A resiliência em discussão. Psicol Estud 2004;9:67–75. doi: 10.1590/S1413-73722004000100009. [Google Scholar]
- [5].Fontes AP, Neri AL. Resilience in aging: literature review. Ciên Saúde Colet 2015;10: 1590/1413-81232015205.00502014. [DOI] [PubMed] [Google Scholar]
- [6].Junqueira MFPS, Deslandes SF. Resiliência e maus-tratos à criança. Cadernos de Saúde Pública 2013;doi: 10.1590/S0102-311X2003000100025. [DOI] [PubMed] [Google Scholar]
- [7].Paludo SS, Koller SH. Psicologia positiva: uma nova abordagem para antigas questões. Paidéia 2007;16:9–20. [Google Scholar]
- [8].Seligman MP. Positive psychology, positive prevention, and positive therapy. In: Seligman, M.P., editor. Handbook of Positive Psychology. New York: Oxford University Press; 2002:3–9. [Google Scholar]
- [9].Seligman MP, Steen TA, Park N, et al. Positive psychology progress: empirical validation of interventions. Am Psychol 2005;60:410–21. [DOI] [PubMed] [Google Scholar]
- [10].Pacico JC, Bastianello, MR. As origens da psicologia positiva e os primeiros estudos brasileiros. In: Hutz, C.S., editor. Avaliação em Psicologia Positiva. 1th ed. Porto Alegre: Artmed; 2014:13–51. [Google Scholar]
- [11].Marques S, Ribeiro JLP. Contribuição para o estudo psicometrico e estrutural da Escala de Esperança para crianças: estudo preliminar. In: Actas da XI Conferência Internacional de Avaliação Psicológica: Formas e Contextos; 2006 out 5–7; Braga, Portugal: Faculdade de Psicologia e de Ciências da Educação. 301–07. [Google Scholar]
- [12].Snyder CR, Lopez SJ. Psicologia positiva: Uma abordagem científica e prática das qualidades humanas. Porto Alegre: Artmed 2009. [Google Scholar]
- [13].Snyder CR. The psychology of hope: you can get there from here. New York: Free Press 1994. [Google Scholar]
- [14].Snyder CR, Lehman KA, Kluck B, et al. Hope for rehabilitation and vice versa. Rehabilit Psychol 2006;doi: 10.1037/0090-5550.51.2.89. [Google Scholar]
- [15].Serafini G, Pompili M, Borgwardt S, et al. Brain changes in early-onset bipolar and unipolar depressive disorders: a systematic review in children and adolescents. Europe Child Adolesc Psychiatry 2014;doi: 10.1007/s00787-014-0614-z. [DOI] [PubMed] [Google Scholar]
- [16].Rozenthal M, Laks J, Engelhardt E. Aspectos neuropsicológicos da depressão. Revista de Psiquiatria 2004;26:204–12. [Google Scholar]
- [17].Snyder CR, Lopez SJ, Shorey HS, et al. Hope theory, measurements and applications to school psychology. Sch Psychol 2003;doi: 10.1521/scpq.18.2.122.21854. [Google Scholar]
- [18].Snyder CR, Harris C, Anderson JR, et al. The will and the ways: development and validation of an individual-differences measure of hope. J PersonalSoc Psychol 1991;60:570–85. [DOI] [PubMed] [Google Scholar]
- [19].Snyder CR, Lopez SJ. The Handbook of Positive Psychology. New York: Oxford University Press; 2005. [Google Scholar]
- [20].Jekel JF, Katz DV, Elmore JG. Epidemiologia, bioestatística e medicina preventiva. Porto Alegre: Artmed 2005. [Google Scholar]
- [21].Hochman B, Nahas FX, Oliveira Filho RS, et al. Desenhos de Pesquisa. Acta Cirúrgica 2005;doi: 10.1590/S0102-86502005000800002. [DOI] [PubMed] [Google Scholar]
- [22].Brucki SMD, Nitrini R, Caramelli P<, et al. Sugestões para o uso do miniexame do estado mental no Brasil. Arquivos de Neuropsiquiatria 2003;doi: 10.1590/S0004-282X2003000500014. [DOI] [PubMed] [Google Scholar]
- [23].Ribeiro JL, Pedro L, Marques S. Contribuição para o estudo psicométrico e estrutural da escala de esperança (de futuro). In. Actas 6( Congresso Nacional de Psicologia da Saúde; Faro, Portugal: Faculdade de Arquitetura do Porto; 2006:75–81. [Google Scholar]
- [24].Beck JT. Terapia Cognitivo-comportamental: teoria e prática. Porto Alegre: Artmed 2013. [Google Scholar]
- [25].Yesavage JA, Brink TL, Rose TL, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res 1983;17:37–49. [DOI] [PubMed] [Google Scholar]
- [26].Almeida OP, Almeida SA. Confiabilidade da versão brasileira da escala de depressão geriátrica (GDS) versão reduzida. Arquivos de Neuro-Psiquiatria 1999;doi: 10.1590/S0004-282X1999000300013. [DOI] [PubMed] [Google Scholar]
- [27].Paradela EMP, Lourenço RA, Veras RP. Validação da escala de depressão geriátrica em um ambulatório geral. Revista de Saúde Pública 2005;doi: 10.1590/S0034-89102005000600008. [DOI] [PubMed] [Google Scholar]
- [28].Wilxocon F, Katti SK, Wilcox RA. Critical clues and probability levels for the Wilcoxon Rank Sum Test and the Wilcoxon Rank Test. New York: Lederle Laboratories Division; 1963. [Google Scholar]
- [29].Bussab WO, Morettin P. Estatística básica. Recife: Saraiva 2017. [Google Scholar]
- [30].Ministry of Health (Brazil). Resolution n(. 466, December 12, 2012. Resolução para determinações éticas em pesquisa com seres humanos. Diário Oficial da União 12 dez 2012; Seção 1. [Google Scholar]
- [31].Malloy-Diniz LF, Fuentes D, Consenza RM. Neuropsicologia do Envelhecimento. Porto Alegre: Artmed 2013. [Google Scholar]
- [32].Simon SS, Ribeiro MPO. O comprometimento cognitivo leve e reabilitação neuropsicológica: uma revisão bibliográfica. Psicologia em Revista 2011;20:93–122. [Google Scholar]
- [33].Marback RF, Pelisoli C. Terapia cognitivo-comportamental no manejo da desesperança e pensamentos suicidas. Revista Brasileira de Terapias Cognitivas 2014;doi: 10.5935/1808-5687.20140018. [Google Scholar]
- [34].Taveira RBB, Taveira DLR, Caixeta L. Abordagens não farmacológicas na Doença de Alzheimer. In: Caixeta, L., editor. Doença de Alzheimer. Porto Alegre: Artmed; 2014:353–68. [Google Scholar]
- [35].Neri AL, Yassuda MS. Velhice bem-sucedida: aspectos afetivos e cognitivos. Campinas: Papirus 2004. [Google Scholar]
- [36].Charles LT, Carstensen LL. Social and Emotional Aging. Annl Rev Psychol 2010;doi: 10.1146/annurev.psych.093008.100448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [37].Abrisqueta-Gomez J. Reabilitação neuropsicológica: abordagem interdisciplinar e modelos conceituais na prática clínica. Porto Alegre: Artmed 2011. [Google Scholar]
- [38].Hartmann Júnior JAS, Medeiros AGAPM, Vasconcelos CAC, Rolim Neto ML, Gomes GC. A Psicologia no processo de resiliência em idosos. In: Albuquerque, C.G.S.C., Moreira, L.P.C., Sousa, R.G., Nóbrega, R.J.T., editors. Reflexões à Luz do Envelhecimento. Recife: Libertas; 2017:160–81. [Google Scholar]