

Short abstract
Background
The consumption of addictive substances is common in adolescence and raises concerns about future addiction. We investigated addictive substance consumption among young people to inform the design of drug intervention programmes.
Methods
Participants were a population-based sample of 14- to 24-year-olds from Paredes, northern Portugal. A self-report questionnaire measured social and health variables, including tobacco, alcohol and illicit drug consumption.
Results
Data were analysed for 731 valid responses. Participants who had drunk alcohol did so first at 14.7 years (mean); 15.3% (95% confidence intervals [CI]: 12.9–18.1) drank alcohol regularly (more than 1/week, adjusted for age and sex) (95% CI: 12.9–18.1). Participants who had smoked tobacco did so first at 14.8 years (mean); 16.6% (95% CI: 14.0–19.5) were regular smokers. Illicit drug consumption was reported by 16.7% of participants (95% CI: 14.2–19.6) and 10.4% consumed drugs regularly.
Conclusion
We found a high prevalence of addictive substance consumption, particularly alcohol. As cultural attitudes likely influence alcohol consumption, a multigenerational approach is needed to address adolescent consumption. Participants’ main sources of drug information were family members. Strategies are needed to promote drug literacy in parents and other relatives to change adolescents’ culturally acquired habits of addictive substance consumption.
Keywords: Adolescent, tobacco use, alcohol drinking, substance-related disorders, health education, social planning
Introduction
Adolescence is the stage of life between childhood and adulthood and involves substantial physical, psychological and social growth and development. This period is characterised by the development of self-identity, autonomy and independence. During adolescence, the capacity for abstract thought increases and individuals become more interested in intimate relationships and sexuality. This period is also characterised by the consolidation of moral values and the desire to make plans about future adult life.1
Adolescence is a period of experimentation. Adolescents often engage in novelty seeking and risk-taking behaviours, which can lead to special social and health care needs.2 The desire for experimentation can result in the adoption of new and unhealthy habits, lifestyles and behaviours that have short- or long-term social and health consequences.
During the complex stage of adolescence, an individual begins to consolidate his or her personality in the context of wider society. Teenagers learn that their choices have positive or negative impacts in the community. Thus, a full understanding of adolescence requires a multifaceted approach that includes both teenagers’ own personal trajectories and the general social context.3 Portuguese4–7 and international studies8,9 have examined the biological, psychological, sociological and educational context of adolescence and have delineated specific research goals and strategies. However, most of these studies focus on school-based populations and have excluded adolescents who have left school, either because they had finished their academic courses or because they had dropped out of school. A global perspective is needed on the experiences, needs and expectations of young people outside school.
The aim of this study was to investigate patterns of addictive substance consumption (alcohol, tobacco and other drugs) among young people aged between 14 and 24 years using a population-based approach.
Methods
Type of study
We conducted a cross-sectional, population-based, self-report survey of individuals aged between 14 and 24 years from Paredes, a county in northern Portugal. Paredes is a semi-urban region located 35 km from the region’s capital, Porto, and has good rail and road access. The county has almost 87,000 inhabitants distributed across 157 km2 (18.6% of whom are under 15 years old) and is one of the 10 newest Portuguese counties. Paredes was historically an industrial area and most of the population worked in the secondary economic sector, mainly in civil construction and the furniture industry. However, in the last 20 years the tertiary sector has grown and now 51.3% of the active workforce is employed in this sector. Rural workers comprise less than 2% of the population.
Sampling
According to the 2011 Portuguese National Census, Paredes has 12,312 inhabitants between 14 and 24 years old, living in 24 different civil parishes. We used stratified sampling, maintaining the proportion of civil parish inhabitants, assuming a design effect of 2.00. A sample size of 746 participants was estimated based on a 95% confidence interval (CI) and a maximum error of 5%. Table 1 shows the sample distribution across the 24 civil parishes.
Table 1.
Sample distribution by civil parish.
| Civil parish | Population* | Sample |
|---|---|---|
| Aguiar de Sousa | 205 | 12 |
| Astromil | 127 | 8 |
| Baltar | 616 | 37 |
| Beire | 309 | 19 |
| Besteiros | 233 | 14 |
| Bitarães | 438 | 27 |
| Castelões de Cepeda | 1040 | 63 |
| Cete | 395 | 24 |
| Cristelo | 297 | 18 |
| Duas Igrejas | 670 | 41 |
| Gandra | 991 | 60 |
| Gondalães | 199 | 12 |
| Lordelo | 1417 | 86 |
| Louredo | 211 | 13 |
| Madalena | 284 | 17 |
| Mouriz | 412 | 25 |
| Parada de Todeia | 264 | 16 |
| Rebordosa | 1279 | 77 |
| Recarei | 628 | 38 |
| Sobreira | 630 | 38 |
| Sobrosa | 366 | 22 |
| Vandoma | 312 | 19 |
| Vila Cova de Carros | 108 | 7 |
| Vilela | 881 | 53 |
| TOTAL | 12,312 | 746 |
*Data from the 2011 National Census
In each stratum, we used the random route method10 of participant selection. The order of the streets, house numbers and the dwellings in each building to be visited was determined in a random way prior to the survey, excluding institutional and non-residential buildings.
In each household, we interviewed members who met the inclusion criteria. If there was more than one eligible individual, we selected the individual whose birth date was the closest and fell before the date of the interview. If the selected individuals declined to participate, we proceeded to the following street until the required number of participants had been obtained according to the calculated sample size.
Participants
All young people aged 14 to 24 years from Paredes were eligible for participation. The participants, or their parent or guardian if they were younger than 16 years old, gave their written, informed consent for participation. We excluded individuals who had been away from home for more than 6 months, temporary visitors, travellers and guests, individuals who did not speak Portuguese and those without the physical or mental ability to answer the questionnaire.
Data collection methods
Data collection occurred from January 2014 to September 2014. The questionnaire measured the following social and health variables: social characteristics; education, jobs and expectations; nutrition, physical activity and body image; social identity, daily routines and youth behaviours; health issues; and demographic characteristics. For the present analysis, we included data for social and demographic characteristics, social identity, daily routines and youth behaviours (consumption of alcohol, tobacco or other drugs) and health (using a question on self-perception of global health status, rated on a 5-point Likert scale, and the frequency of self-reported symptoms of headache, back pain, stomach ache, dizziness, tiredness, sadness, sleeping problems, anxiety, anger, and fear). To measure consumption of addictive substances, participants were asked if they had already tried the substance, how old they were when they tried it for the first time, how often they used it (daily, weekly, monthly, at least once in the last 3 months, sometimes), and if they had experienced being drunk.
The questionnaire was pilot-tested with a group of teenagers who were not part of the study population to check the face validity and comprehensibility.
The interviewers were local volunteers (from the Paredes Town Hall Voluntary Program) who were trained to deliver the questionnaire using the following protocol: selection of participants in accordance with the procedure described above, manual delivery of the form and the informed consent form, provision of additional information and reassurance to participants, and collection and sealing of the questionnaires and forms in an envelope (to guarantee participant anonymity). All interviewers were supervised and supported by the study coordinators.
Questionnaires on which more than half of the items had been answered were included in data analysis. All items with incomplete responses were treated as missing data.
After excluding non-valid questionnaires, an additional 17 questionnaires were distributed (using the same participant selection method, in the same civil parishes) to reach the required sample size.
Ethical issues
This study was approved by the ethics committee of São João Central Hospital, Porto and the Faculty of Medicine, University of Porto. The study procedures were in accordance with the Declaration of Helsinki and the Oviedo Convention on the rights of individuals taking part in biomedical investigations.
All participants (or their parents or guardians) signed an informed consent form. The questionnaires were completely anonymous and sealed in an envelope after being collected.
Statistical analysis
We used descriptive and inferential statistics to calculate prevalence. CIs were calculated using the Wald method. Prevalence for the main outcome was estimated after standardisation for age and sex based on data from the 2011 Portuguese National Census. For hypothesis testing, we used logistic regression (analyses were adjusted for age and sex), Student’s t-tests or nonparametric tests, and Pearson correlations, depending on the variables. The Kolmogorov–Smirnov test was used to check for normal distributions. The significance level was set at 0.05. Data were encoded and registered in a Microsoft Office Excel 2010® database and analysed using IBM SPSS Statistics®, version 21.0 (IBM Corp., Armonk, NY, USA).
Results
The total sample included 746 participants. Questionnaires for which the sex of the respondent was not specified (n = 15) were excluded, leaving 731 valid responses. Of the respondents who reported their sex, 399 (54.6%) were female and 332 (45.4%) were male. The mean age of respondents was 18.3 ± 2.9 years (18.3 ± 2.8 for female respondents and 18.5 ± 3.0 for male respondents). Table 2 shows the sociodemographic characteristics of the sample by sex. Most participants were still attending school (70.6%). Of respondents aged ≤16 years, 99.6% were still attending school; of those aged ≤18 years, 94.4% were still attending school. There was no significant sex difference in school attendance. Of the total sample, 30.2% were current college students (aged ≥18 years) and slightly more college attendees were female (34.9%) than male (24.7%). Respondents aged ≥18 years old who had already left school were older than those still attending school: 21.3 years (95% confidence intervals [CI]: 21.0–21.7) versus 19.6 years (95% CI: 19.3–19.8) for both sexes.
Table 2.
Demographic characteristics of respondents (N = 731).
|
Sex |
||
|---|---|---|
| Male(n = 332/731) | Female(n = 399/731) | |
| Age, years, mean ± SD | 18.5 ± 3.0 | 18.3 ± 2.8 |
| Age, years, median (IQD) | 18 (5) | 18 (4) |
| Civil status | ||
| Single | 312 (94.0%) | 377 (94.4%) |
| Married | 9 (2.7%) | 11 (2.8%) |
| Other (including no response) | 11 (3.3%) | 11 (2.8%) |
| Main household income source | ||
| Work | 295 (88.9%) | 358 (89.7%) |
| Subsidies | 16 (4.8%) | 14 (3.5%) |
| Pensions | 2 (0.6%) | 14 (3.5%) |
| Other (including no response) | 19 (5.7%) | 13 (3.3%) |
| Occupationa | ||
| Active worker | 77 (23.2%) | 62 (15.5%) |
| Unemployed | 40 (12.0%) | 53 (13.3%) |
| Retired | 1 (0.3%) | - |
| Current student | 225 (67.8%) | 291 (72.9%) |
| Economic sector of active workers | ||
| Primary sector | - | - |
| Secondary sector | 32 (41.6%) | 20 (32.3%) |
| Tertiary sector | 40 (51.9%) | 33 (53.2%) |
| Other (including no response) | 5 (6.5%) | 9 (14.5%) |
Data are presented as number of responses (percentage) unless otherwise indicated. aThe totals in this section are >100%, as some students were also active workers. SD: standard deviation; IQD: interquartile distance.
Young people at least 18 years old who had already left school were older: 21.3 years (95% CI: 21.0–21.7) versus 19.6 years (95% CI: 19.3–19.8) for both sexes.
Habits and substance consumption
After adjustment for age and sex, 84.4% of participants (95% CI: 81.6–86.9) had drunk alcoholic beverages at least once, and 15.3% (95% CI: 12.9–18.1) drank more than once a week. We found that 57.6% (95% CI: 53.9–61.3) had tried smoking and 16.6% (95% CI: 14.0–19.5) smoked regularly (at least once a week).
The estimated population prevalence of alcohol consumption was 16.2% for regular alcoholic beverages (95% CI: 15.6–16.7) and 17.4% for tobacco smoking (95% CI: 16.7–18.0). Table 3 shows the outcomes by sex.
Table 3.
Substance consumption patterns by sex, adjusted for age.
|
Male(n = 332) |
Female(n = 399) |
||||
|---|---|---|---|---|---|
| Absolute proportionn (%) | Adjusted proportion% (95% CI) | Absolute proportionn (%) | Adjusted proportion% (95% CI) | ||
| Has drunk any alcoholic beverages | 284 (85.5%) | 87.9% (84.0–91.1) | 310 (77.7%) | 81.3% (77.1–84.9) | P = 0.009c |
| Age when drunk any alcoholic beverages for the first time [years], mean (95% CI) | 14.2 (13.9–14.6) | 15.2 (14.9–15.5) | P < 0.001a | ||
| Drinks alcoholic beverages ≥1 times/weekd | 73 (22.0%) | 24.6 (20.3–29.6) | 24 (6.01%) | 7.5 (5.3–10.6) | P < 0.001c |
| Has been drunk | 111 (33.4%) | 38.3 (33.0–43.6) | 84 (21.0%) | 24.0 (20.1–28.6) | P = 0.001c |
| Has never drunk any alcoholic beverages, % (95% CI) | 43 (13.0%) | 80 (20.1%) | |||
|
No response, % (95% CI) |
5 (1.5%) |
|
9 (2.2%) |
|
|
| Has smoked tobacco | 195 (58.7%) | 64.7 (59.3–69.8) | 192 (48.1%) | 51.7 (46.6–56.6) | P = 0.002c |
| Age of first smoking experience [years], mean (95% CI) | 14.4 (14.0–14.8) | 15.2 (14.8–15.5) | P = 0.012a | ||
| Smokes ≥1 times/weekd | 72 (21.7%) | 24.8 (20.3–29.8) | 36 (9.0%) | 9.7 (7.0–12.9) | P < 0.001c |
| Has never smoked, % (95% CI) | 122 (36.7%) | 190 (47.6%) | |||
|
No response, % (95% CI) |
15 (4.5%) |
|
17 (4.3%) |
|
|
| Has tried addictive drugs | 74 (22.3%) | 25.0 (20.5–29.8) | 39 (9.8%) | 9.8 (7.1–13.0) | P < 0.001c |
| Age at first addictive drug use [years], mean (95% CI) | 16.4 (15.9–16.9) | 17.0 (16.6–17.5) | P = 0.089b | ||
| Has never tried addictive drugs, % (95% CI) | 251 (75.6%) | 353 (88.5%) | |||
| No response, % (95% CI) | 7 (2.1%) | 7 (1.8%) | |||
aMann–Whitney U test; bStudent’s t-test; clogistic regression; dThe cutoff of ≥1 per week was based on the World Health Organizations’s Alcohol Use Disorders Identification Test (AUDIT) categories or on clinical experience. CI, confidence interval.
The results suggest that the consumption of both alcohol and tobacco is more common in males, who begin experimenting at a younger age.
Of the participants, 16.7% (95% CI: 14.2–19.6) had consumed illegal drugs. Cannabinoids were the drugs most frequently consumed (15.2%; 95% CI: 12.6–17.9), followed by drugs acquired at “smart shops” (which sell psychoactive substances and are now illegal in Portugal) (4.9%; 95% CI: 3.5–6.6).
Figure 1 shows the prevalence of drug use in both sexes, adjusted for age.
Figure 1.
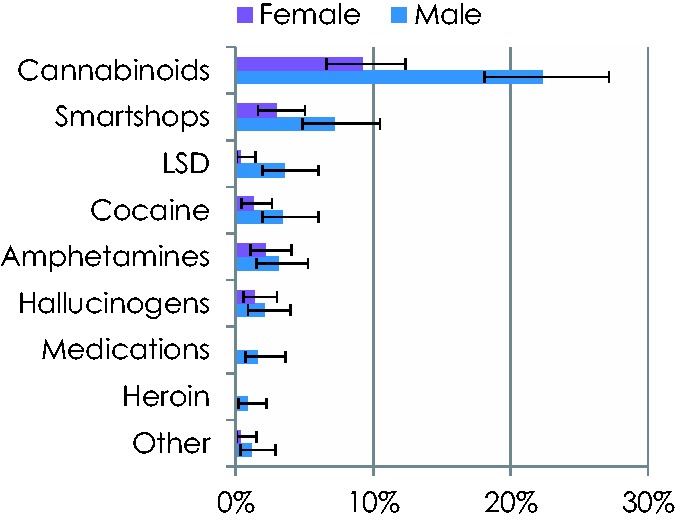
Prevalence of drug consumption by sex, adjusted for age
The mean age at which drug use started was 16.6 years (95% CI: 16.2–17.0), higher than the mean age for alcohol consumption (14.7 years; 95% CI: 14.5–15.0, P < 0.001) and tobacco consumption (14.8 years; 95% CI: 14.5–15.0, P < 0.001).
Drug consumption was most common in participants who already drank alcohol (P < 0.001), or smoked tobacco (P < 0.001), supporting the common assumption that consumption of legal substances leads to consumption of other substances. When asked about frequency, 10.4% of participants reported consuming drugs at least once a week and 72.6% reported that they rarely consumed drugs (there were no sex differences).
There was a positive and significant correlation between age and prevalence of alcohol consumption (Pearson correlation = 0.792, P = 0.004), of tobacco smoking (Pearson correlation = 0.811, P = 0.002) and of drug use (Pearson correlation = 0.838, P = 0.001) (Figure 2).
Figure 2.
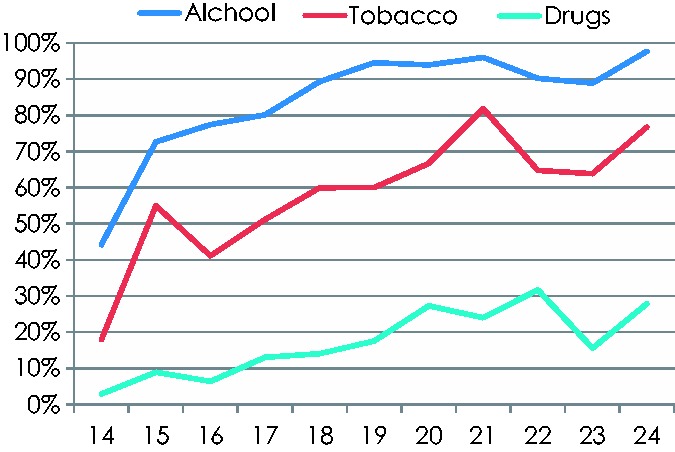
Proportion of consumption (at least once) of different substances by age
Outcomes are adjusted for age and sex.
After adjustment for age and sex, there were no differences in casual or regular consumption of alcohol or tobacco between participants still attending school and those who had left school. However, school attendance was associated with lower use of other substances (odds ratio [OR] = 0.546; 95% CI: 0.299–0.997; P = 0.049). In addition, unemployment in participants who had been active workers was associated with a greater use of illicit drugs (OR = 2.263; 95% CI: 1.101–4.652; P = 0.026), but not with alcohol or tobacco consumption.
Having tried tobacco smoking was associated with greater consumption of other drugs (OR = 2.930; 95% CI: 1.469–5.841; P = 0.002) as was regular smoking (OR = 6.004; 95% CI: 3.065–11.760; P < 0.001). However, sporadic or regular drinking was not associated with greater consumption of other drugs. A history of experimentation with any drug was associated with consumption of other drugs (OR = 7.135; 95% CI: 3.694–13.782, P < 0.001).
General perception of health status was rated on a scale from 1 (very bad) to 5 (very good). The total mean score was 3.16 (±0.651) and health status was better in males (3.27 ± 0.606) than in females (3.07 ± 0.675), P < 0.001; health status for females declined with increasing age (Pearson correlation = −0.171, P = 0.001). Substance consumption did not affect health status perception.
More than half of the participants experienced psychological symptoms, such as sadness, sleeping problems, anxiety, anger and fear at least once a week: 54.7% (95% CI: 51.0–58.3); these were more frequent in females (60.6%; 95% CI: 55.7–65.4) than in males (47.5%; 95% CI: 42.0–53.0; P = 0.001) and in tobacco and drug users, irrespective of age.
We also assessed the source of adolescents’ information about substance consumption. Figure 3 shows the main information sources. Both males and females obtained most information from family and friends. Health care providers were minor sources of information for this sample.
Figure 3.
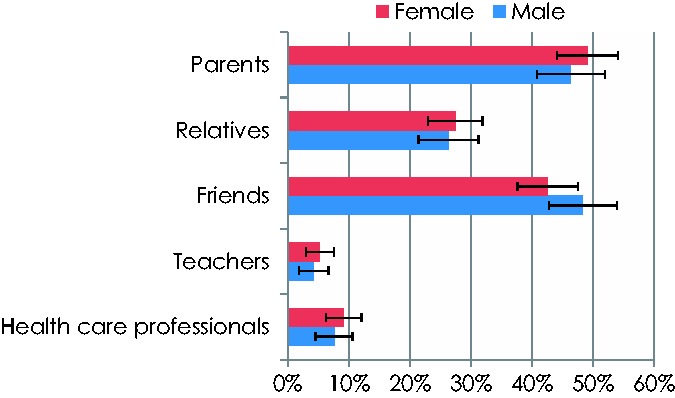
Main source of information about substance consumption
Bars show adolescents’ main sources of information (after adjustment for age) and 95% confidence interval. The “relatives” category excludes parents.
Discussion
The estimated prevalence of regular alcohol drinking for this sample of 14- to 24-year-olds was 16.2% (the national estimate = 16.4%). We found that 17.4% of participants smoked regularly (the national estimate = 17.5%). In this sample, 17.4% had tried drugs and 1.8% took drugs regularly (the national estimate = 17.6% and 1.8%, respectively). These findings suggest that this was a representative population-based sample.
One possible study limitation relates to the adequacy of randomisation. The random route method is a popular method of sample selection and permits representative sampling of the population of interest.10 However, the method is expensive and time-consuming. Our interviewers were volunteers from the Paredes Town Hall Voluntary Program and the participant selection process took much longer than we anticipated. However, our sample data by age and sex are similar to population distribution data from the 2011 Portuguese National Census, suggesting that the sample was representative and wider conclusions can be drawn from the data.
Another limitation was the size of the questionnaire. This study was part of the Morpheus project, which aims to profile the physical, psychological and social characteristics of young people in Paredes. The questionnaire had to include a large number of variables (379 in total), resulting in a large response burden. However, the quality audits performed on the questionnaire did not reveal any substantial problems.
Several sample characteristics should be mentioned. Most participants were single, still in the academic system and economically dependent on their family. Those who were active workers were mainly employed in the tertiary sector. These characteristics are representative of Portuguese 14- to 24-year-olds. The present demographic findings differ from those of some other Portuguese studies, but this may because those studies used school-based samples.4,6 The population-based approach used here is a strength of the study design, allowing the inclusion of teenagers without the potential bias of a classroom-based survey. In addition, the interviewers distributed and collected the questionnaire, so participants were not required to use public transport or have Internet access to take part.
The mean age of respondents in our sample was higher than that of the HBSC study,6 a school-based study involving 6026 teenagers with a mean age of 14 years, but lower than that of the ULisboa-2012 study,4 a college student survey of 3327 non-randomly selected participants with a median age of 20 to 22 years. The target populations of the HBSC and ULisboa-2012 studies were school-based, which could explain several differences between the findings of these studies and the present findings. In the HBSC study, 41% of participants had tried alcohol; participants had first tried alcohol at a mean age of 13 years and 17% of participants had experienced being drunk. In the same study, 22% of participants had started smoking tobacco at 13 years (or 33% if we consider only 1st year high school students). Our results show a higher prevalence of tobacco smoking, even if we consider the age distribution. In the ULisboa-2012 study, 33.9% of college students reported smoking tobacco, 15.7% on a regular basis, and 97.5% had drunk alcohol (72.6% in the previous month).
The 3rd National Survey of the Consumption of Psychoactive Substances in the General Population in Portugal (2012) found that 72.1% of respondents were lifelong drinkers and 47.5% had smoked.11
Regarding illicit drug use, 8% of participants (mostly males) of the HBSC study had tried cannabinoids (the most used substance) and had started when they were 14 years old. In the ULisboa-2012 study, this proportion was higher, at 40%.
In France, the prevalence of substance use is higher, both in the community12 and in schools.13 In a study in Colorado, USA, Young et al. found a prevalence of tobacco and illicit drug use in college students similar to our own, but lower occasional and regular alcohol consumption.14 However, other studies have reported higher prevalence of consumption of alcohol, tobacco and other substances5 and one Spanish study reported a consumption pattern similar to our own.16
The present findings were in accord with those of previous studies regarding the association of age and sex (male) with a greater likelihood of occasional or regular substance consumption, mostly beginning in adolescence. Our results support the notion of a progression in drug use and addiction. Drug consumption is more common in individuals who have already tried alcohol or tobacco. Taking one drug is positively associated with consumption of other drugs during the individual’s lifetime. As the psychological mechanisms of self-control are incipient in adolescents,17 the development of strategies aimed at avoidance of first drug consumption is particularly important.
We found that social context and leisure activities influenced substance use. Compared with participants who were still at school, those who were unemployed had greater consumption of substances other than alcohol and tobacco. In Portugal, school education is mandatory until 18 years of age (or 12 academic years). The school environment plays a role in health choices and risky behaviours in young people. Therefore, it is crucial that the school community promotes healthy goals to young people.
The Portuguese Youth and Child National Health Program recommends the health screening of adolescents across three different visits according to the key ages of individual development: 10 to 13 years, 15 years and 18 years. The aim is to establish trust and communication channels between health and education. However, our results show that young people do not regard health care providers as partners who can provide substance consumption counselling, perhaps because young people do not perceive their health status as associated with consumption history. It is possible that young people do not regard substance consumption as a health problem or as risky behaviour and therefore do not mention it in medical visits. In addition, doctors often adopt a punitive, or at least a prohibitive, attitude toward young people who use drugs. However, our findings indicate that parents and other relatives play an important role when young people are seeking advice. Therefore, it may be more effective to focus on educating individuals such as family members to provide clear and reliable information on drug use to young people. It is crucial that parents acquire knowledge and skills to enable them to influence the attitudes of the next generation. Although the media is an important tool in this endeavour, other interventions directed at core groups are also valid.18,19 The promotion of health literacy is the key to effective change in daily habits and lifestyles.20 Health providers need to review their attempts to communicate with young people to achieve better outcomes21 and to realise that prevention programs aimed at health promotion are cost-effective9 in the short and long term.8,22
Psychological symptoms were more common in participants who had used tobacco and other drugs (but not alcohol). Future research needs to confirm whether psychological symptoms are a cause or consequence of drug use. The lack of association between psychological symptoms and alcohol consumption may be a result of positive cultural perceptions of alcohol consumption in Portugal. Aside from the question of the cause and effect relationship between psychological symptoms and drug use, this association raises concerns about the social consequences of drug use and the ability of young people to integrate successfully into society. There is a need to implement inclusion strategies to promote social skills; the association between substance consumption and unemployment found here suggests that pro-employment policies may be useful.
Conclusion
Portuguese adolescents showed a high prevalence of substance consumption, particularly alcohol. As this may stem from cultural attitudes to alcohol, a multigenerational approach is needed in future studies on substance consumption in adolescents. The main sources of information for participants were family members, indicating the need to educate parents (and other relatives) to change culturally acquired habits.
Acknowledgements
We thank Paredes Town Hall for administrative support.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This article was supported by the ERDF (European Regional Development Fund) through the operation POCI-01-0145-FEDER-007746, funded by the Programa Operacional Competitividade e Internacionalização – COMPETE2020, and by national funds from the FCT (Foundation for Science and Technology) through the CINTESIS Research and Development Unit (reference UID/IC/4255/2013).
References
- 1.Neinstein LS. Adolescent health care: a practical guide Lippincott Williams & Wilkins, 2008.
- 2.Programa Nacional de Saúde Infantil e Juvenil.
- 3.Pais JM. Jovens e cidadania. Sociologia, problemas e práticas 2005: 49: 53–70. [Google Scholar]
- 4.Alcântara da Silva P, Borrego R, Ferreira VS, et al. Consumos e Estilos de Vida no Ensino Superior: o caso dos estudantes da U Lisboa-2012 www.sicad.pt 2015, p.179.
- 5.Feijão F, Lavado E, Calado V. Estudo sobre o consumo de álcool, tabaco e drogas ECATD/2011 2011. www.sicad.pt: Instituto da Droga e Toxicodependência, IP.
- 6.Matos MG, Simões C, Camacho I, et al. Relatório do estudo HBSC 2014. http://aventurasocial.com/arquivo/1437158618_RELATORIO%20HBSC%202014e.pdf: FMH/Universidade de Lisboa, 2015, p.212.
- 7.Viana V, Santos PLd, Guimarães MJ. Comportamento e hábitos alimentares em crianças e jovens: uma revisão da literatura. Psicologia, Saúde & Doenças 2008; 9: 209–231. [Google Scholar]
- 8.Hatzis CM, Papandreou C, Kafatos AG. School health education programs in Crete: evaluation of behavioural and health indices a decade after initiation. Prev Med 2010; 51: 262–267. DOI: 10.1016/j.ypmed.2010.05.015. [DOI] [PubMed] [Google Scholar]
- 9.Hoeflmayr D, Hanewinkel R. Do school-based tobacco prevention programmes pay off? The cost-effectiveness of the ‘Smoke-free Class Competition'. Public Health 2008; 122: 34–41. DOI: 10.1016/j.puhe.2007.05.007. [DOI] [PubMed] [Google Scholar]
- 10.Hoffmeyer-Zlotnik JH. New sampling designs and the quality of data. In: Ferligoj A and Mrvar A (eds) Developments in applied statistics Ljubljana: FDV Methodoloski zvezki 2003: 205–217.
- 11.Balsa C, Vital C, Urbano C. III Inquérito Nacional ao Consumo de Substâncias Psicoativas na População Geral - Portugal 2012 www.sicad.pt: Serviço de Intervenção nos Comportamentos Aditivos e nas Dependências, 2014, p.296.
- 12.Redonnet B, Chollet A, Fombonne E, et al. Tobacco, alcohol, cannabis and other illegal drug use among young adults: the socioeconomic context. Drug Alcohol Depend 2012; 121: 231–239. DOI: 10.1016/j.drugalcdep.2011.09.002. [DOI] [PubMed] [Google Scholar]
- 13.Tavolacci MP, Ladner J, Grigioni S, et al. Prevalence and association of perceived stress, substance use and behavioral addictions: a cross-sectional study among university students in France, 2009–2011. BMC Public Health 2013; 13: 724. DOI: 10.1186/1471-2458-13-724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Young SE, Corley RP, Stallings MC, et al. Substance use, abuse and dependence in adolescence: prevalence, symptom profiles and correlates. Drug Alcohol Depend 2002; 68: 309–322. [DOI] [PubMed] [Google Scholar]
- 15.O'Malley PM, Johnston LD. Epidemiology of alcohol and other drug use among American college students. Journal of Studies on Alcohol Supplement 2002; 23–39. [DOI] [PubMed]
- 16.Font-Mayolas S, Gras ME, Cebrian N, et al. Types of polydrug use among Spanish adolescents. Addict Behav 2013; 38: 1605–1609. DOI: 10.1016/j.addbeh.2012.09.007. [DOI] [PubMed] [Google Scholar]
- 17.Leeman RF, Patock-Peckham JA, Potenza MN. Impaired control over alcohol use: an under-addressed risk factor for problem drinking in young adults? Exp Clin Psychopharmacol 2012; 20: 92–106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Santos P, Martins C, Sá L, et al. Health education: five years' experience of teaching preventive medicine at the Faculty of Medicine of Oporto University. Education for primary care: an official publication of the Association of Course Organisers, National Association of GP Tutors, World Organisation of Family Doctors 2014; 25: 103–107. 2014/03/07. [DOI] [PubMed] [Google Scholar]
- 19.Harris KC, Kuramoto LK, Schulzer M, et al. Effect of school-based physical activity interventions on body mass index in children: a meta-analysis. CMAJ 2009; 180: 719–726. DOI: 10.1503/cmaj.080966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Santos P, Sá L, Couto L, et al. Health literacy as a key for effective preventive medicine. Cogent Social Sciences 2017; 3: 1407522. [Google Scholar]
- 21.Vorilhon P, Picard V, Marty L, et al. Attitudes of family physicians towards adolescent cannabis users: a qualitative study in France. Fam Pract 2014; 31: 585–591. DOI: 10.1093/fampra/cmu030. [DOI] [PubMed] [Google Scholar]
- 22.Kellam SG, Wang W, Mackenzie AC, et al. The impact of the Good Behavior Game, a universal classroom-based preventive intervention in first and second grades, on high-risk sexual behaviors and drug abuse and dependence disorders into young adulthood. Prev Sci 2014; 15 Suppl 1: S6–18. DOI: 10.1007/s11121-012-0296-z. [DOI] [PMC free article] [PubMed] [Google Scholar]