

Abstract
Background:
Yoga is proven beneficial in improving quality of life among breast cancer survivors receiving chemotherapy, but its effectiveness in lymphoma patients needs to be explored. As chemotherapy-induced neutropenia is very common among lymphoma patients, they are much prone to infections from the environment. Furthermore, trained yoga instructors are not available in every setting, so there is a need to develop home-based yoga program modules for lymphoma patients receiving chemotherapy.
Aim:
The aim of the study was to explore the feasibility and safety of yogic exercises among lymphoma patients during chemotherapy.
Subjects and Methods:
An interventional, single-arm prepost design study was conducted at a tertiary health-care center. Patients suffering from malignant lymphoma (18–65 years) with Eastern Cooperative Oncology Group performance status from 0 to 2, planned to receive chemotherapy were administered a home-based yoga program over a period of 2 months from the start of chemotherapy. The primary outcome variables were retention rate, acceptance rate, safety, and adherence. Health-related quality of life (HRQOL), fatigue level, overall sleep quality, depression, anxiety level, and pain were also assessed.
Statistical Analysis:
Descriptive statistics was used to see the feasibility and adherence. The paired t-test was used to compare various pre and postintervention outcome measures.
Results:
Fourteen patients (median age: 36 years, range13–65 years) of malignant lymphoma were enrolled in the study. Male-to-female ratio was 9:5. Non-Hodgkin's lymphoma patients constituted 64%. The recruitment rate was 93%. Favorable retention (100%), acceptability (97%), adherence (78.6%), and no serious adverse events following yoga practice were reported. Improvement was also found in HRQOL, fatigue, sleep, depression, and anxiety. However, it needs further validation in a randomized study.
Conclusion:
Home-based yoga program is safe and feasible among the patients suffering from malignant lymphoma receiving chemotherapy.
Keywords: Acceptability, adherence, chemotherapy, malignant lymphoma, recruitment rate, retention rate
Introduction
Lymphoma is a hematological malignancy treated with multiagent chemo-immunotherapy, radiation therapy, and other biological agents. Lymphoma patients receiving these therapies often report fatigue as one of the most distressing symptoms, even worse than other symptoms such as pain, nausea, and vomiting, which are usually treatable with medications. They suffer 2.5–3 times more fatigue than the general population.[1] Fatigue leads to decline in physical activity during the period of chemotherapy treatment. The chemotherapeutic medications are likely to negatively affect the health-related quality of life (HRQOL).[2]
Over the past few years, yoga has emerged as an effective intervention in improving overall well-being. It has been reported to improve sleep and reduce anxiety and depression, thus improving overall quality of life among breast cancer patients.[3]
One limitation for integration of yoga in mainstream oncology practice is lack of availability of a trained yoga instructor to every patient. Often, cancer patients are advised isolation in post-chemo phase. Therefore, they cannot attend community yoga program during chemotherapy treatment. In the current era, access to audio-visual (AV) devices is very easy even in rural parts of our country. Hence, this study was designed to assess feasibility and safety of home-based yoga intervention administered through AV devices and printed guidebooks after a direct supervised yoga session.
Subjects and Methods
Study design and settings
This was a single-arm pre- and postdesign interventional study conducted at Postgraduate Institute of Medical Education and Research in Chandigarh, India.
As a feasibility pilot study, a total of 14 patients diagnosed with malignant lymphoma, planned to receive chemotherapy were recruited and study intervention was carried out during first 2 months of chemotherapy (September to November 2016). The inclusion criteria were: (a) aggressive lymphoma patients (Stage II–IV) planned to receive any of the three chemotherapy schedules, i.e., cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP); CHOP + rituximab; adriamycin, bleomycin, vinblastine, and Dacarbazine(ABVD); (b) age group of 18–65 years; (c) Eastern Cooperative Oncology Group (ECOG) performance status score 0–2 (If the ECOG score was >2 at the time of starting chemotherapy, then these patients were reassessed at the time of beginning of 2nd chemotherapy cycle). In case, the score improved to ECOG <2, then these patients were also offered to participate in the study; (d) participants having access to AV display device (CD player, multimedia/smartphone, and laptop); (e) able to complete questionnaire (by self or by interview) in Hindi, Punjabi, or English. Exclusion criteria were Stage I lymphoma patients, ECOG performance score of 3–4 even at 2nd chemotherapy cycle.
Feasibility of yoga-based intervention in lymphoma patients
The feasibility criteria were taken from a yoga feasibility study done in Japan among breast cancer patients.[4] It included recruitment, retention, and acceptability rates which were defined as:
Recruitment rate: The rate of consenting patients divided by the number of eligible patients approached to participate in the study
Retention rate: Number of recruited participants who completed pre and postintervention questionnaires
Adherence was assessed using the self-reported number of completed yoga sessions over a period of 2 months, if participants practiced a complete session in a day; it was counted as one yoga session. 20 sessions/month were taken as good adherence
Acceptability of the intervention was assessed after completion of the program using a 3-point Likert scale
Safety: Participants were asked to report untoward problem that occurred due to yoga practice in their yoga log books.
Study tools
Well-validated and reliable tools were used in the study:
Sociodemographic profile was assessed on the day of registration in the clinic
Physical performance status was assessed using ECOG performance scale[5]
HRQOL and fatigue were assessed using lymphoma-specific instruments, i.e., functional assessment of cancer therapy-lymphoma scale[6]
Functional assessment of chronic illness therapy-Fatigue scale[7]
Quality of sleep was measured with Pittsburgh sleep quality index[8]
Depression was assessed using Patient Health Questionnaire-9[9]
Generalized anxiety disorder-7 tool (GAD-7) for measuring anxiety[10]
Numerical pain rating scale to determine intensity of pain.[11]
The participants were asked to report the adverse events occurring due to yoga practice on their yoga log books.
Intervention
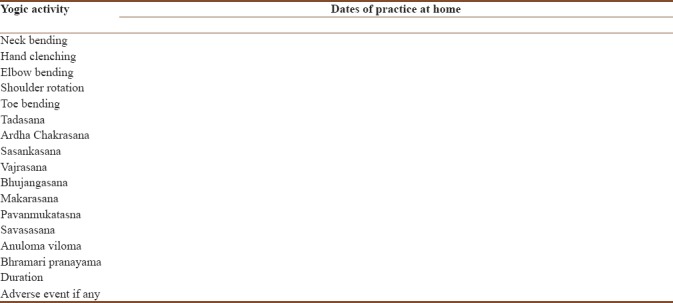
Yoga protocol was taken from the common yoga protocol followed by Government of India on the occasion of “International Yoga Day” 2016.[12] It included warm-up exercises, Asanas, and Pranayam as detailed in Table 1. At the time of recruitment, participants were taught and then supervised yogic exercises on one-to-one basis by the certified yoga instructor (first author). Once this author was convinced with their practice, they were asked to do same yogic exercises daily at home for 30 min. Yoga video and booklets in different languages guided them in the same. Adherence was measured through yoga logbooks [Table 2] maintained by the participants at their home. Biweekly telephonic reinforcement was done to countercheck and enhance adherence.
Table 1.
Various yogic exercises included in the Yoga protocol
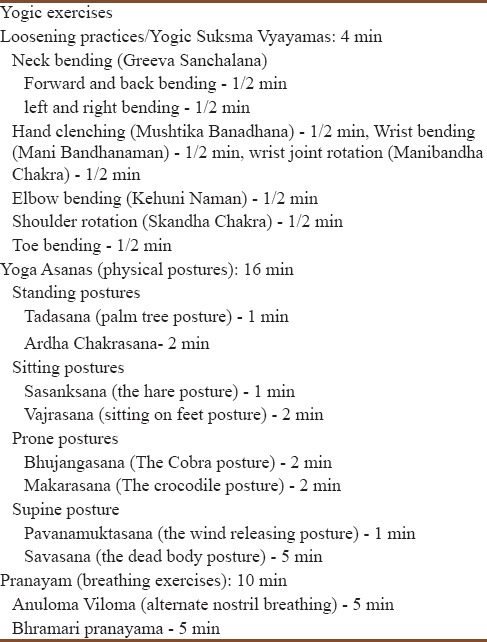
Table 2.
Performa on adherence (please put √ for particular activity done and × for not done)
Study procedure
Ethical approval was obtained from the Institute's Ethical Committee. Informed consent was obtained from all participants. In orientation phase, every participant was informed about the yogic exercises to be done at home during the chemotherapy period. Subsequently, they were taught yogic exercises and maintenance of daily yoga logbook. A yoga booklet and video were also provided to them. Biweekly telephonic reinforcement emphasized about protocol adherence. Follow-up was done at 2nd month of commencement of the program.
Statistical analysis
Statistical Package for the Social Sciences (IBM Corp.SPSS version 22. Armonk, New York) was used for data analysis. Descriptive statistics was done for socioeconomic characteristics of the participants. Paired t-test was applied to check the difference between baseline and postintervention mean scores.
Results
Recruitment and participant's characteristics
After assessing 25 patients for eligibility, 10 patients were found ineligible to participate in the study (ECOG performance score was 3–4 even at 2nd chemotherapy cycle). One patient refused to participate due to personal reasons; finally, 14 patients were included in the study.
Tables 3 and 4 show the summary of a sociodemographic and clinical profile of the participants, respectively.
Table 3.
Baseline characteristics of the participants (n=14)
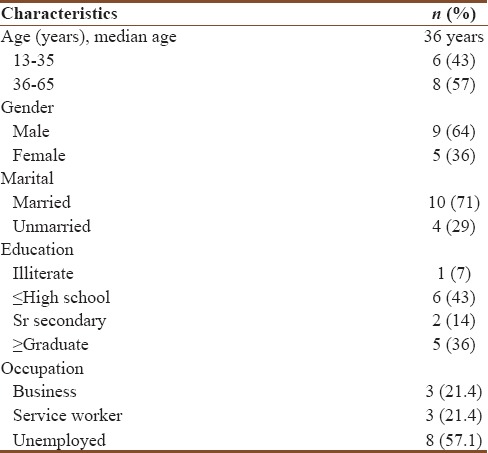
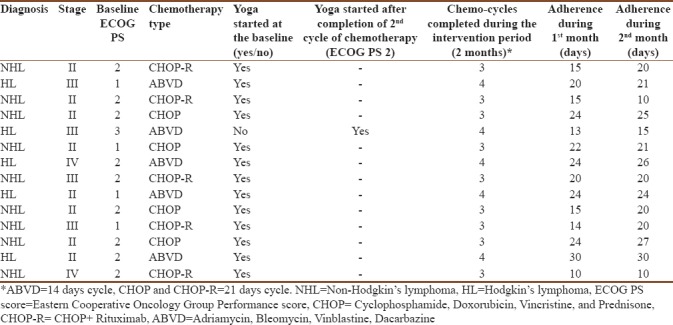
Table 4.
Participant’s clinical details and adherence in terms of number of days of performance of yogic exercises during 1st and 2nd month of chemotherapy
Reported access of audio-visual gadgets and booklet by the patients
Except one, all participants reportedly used yoga video as a guide to yoga practice at home (11 watched it on smartphone, 1 on CD player, and 2 on laptop). Thirteen literate participants reportedly read the yoga booklet at home.
Feasibility of the yoga program
Recruitment rate was 93% and retention rate was reported to be 100%. All the participants maintained the Yoga Log book daily at home. Table 4 shows reported adherence to yoga by the participants during 1st and 2nd month of chemotherapy. Table 5 shows reported adherence to the various components of the yogic exercises.
Table 5.
Good adherence* in terms of number of participants practicing various components and complete yoga session (n=14)
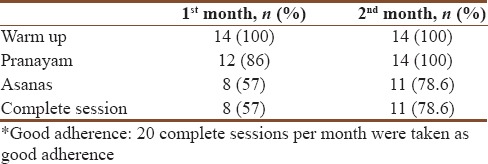
Side effects of chemotherapy such as fatigue, pain in upper extremity where chemotherapy was administered, nausea and vomiting, fever, and diarrhea along with the absence of companion, and low mood were cited as the most frequent reason for skipping the yoga practice at home. The improvement was observed in all secondary outcome variables except pain [Table 6]. At the end of 2nd month of intervention, all participants completed intervention acceptability questionnaire and acceptability rate was found to be 97% [Table 7].
Table 6.
Effects of Yoga on patient.rated outcome at baseline (before start) and 2nd month of chemotherapy
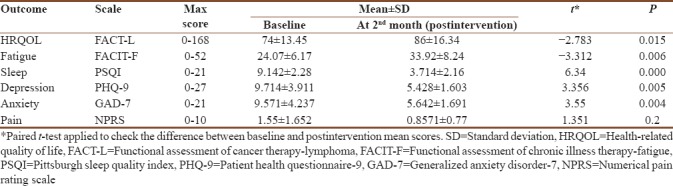
Table 7.
Acceptability of the yoga program (n=14)

Adverse events
No yoga-related serious adverse event was reported by the patients during the study period.
Discussion
Considering the good 100% retention rate, 93% recruitment rate, 97% acceptability rate, 78.6% adherence rate, and no “yoga” related serious adverse events during chemotherapy, it can be suggested that home-based yoga intervention among lymphoma patients undergoing chemotherapy is feasible and safe.
Adherence to the warm-up exercises was good, i.e., 100% in both 1st and 2nd month, and it improved for Asanas from 57% to 78.6% and for Pranayam from 86% to 100% in the 2nd month as compared to the 1st month of chemotherapy. It is understandable that Yogic Asanas are more complex than warm-up exercises. They need slightly more physical fitness than the warm-up activity. In our study, we believe that, after one/two chemotherapy, cycle reduction in tumor burden might have led to improvement in physical condition of the patients which would have enabled them to perform Yogic Asanas in an easier manner than at the time of recruitment. Another possible explanation for better performance is the knowledge that chemotherapy-related adverse events are more likely in the first few weeks of starting of chemotherapy and they may hinder any kind of physical activity.[13] We feel that good adherence in our study was may be due to cultural aspects of our study population, as acceptance for Yoga is higher in Indian culture.
Our intervention program was home based, so it was more convenient for the participants to comply with it. Further, patients undergoing chemotherapy are neutropenic so are extremely susceptible to get infection which may be of serious life-threatening infections in nature.[13] Hence, practicing yoga at home is preferable for this highly immunosuppressed cohort.
One of the hindrances in use of yoga with the modern medicine is lack of availability of trained yoga instructor at every place, especially semi-urban/rural areas do not have access to trained yoga experts. On the contrary, these days, electronic sources such as smartphone/laptops are readily available even in the rural settings. The results of this study show that the use of these gadgets can help patients to practice yoga at home.
The secondary outcomes, for example, quality of life, fatigue, anxiety, depression and sleep also improved in our study and these results are consistent with the result of other similar studies done in cancer survivors.[14,15] Hence, yoga-based programs should be considered in the management of lymphoma patients.
As this was a feasibility study for home-based yoga intervention, however, it needs further validation about improvement in HRQOL, fatigue, sleep, anxiety, and depression by taking up future randomized study on a larger study sample.
Conclusion
The results of the present study support the safety and feasibility of yogic interventions in patients diagnosed with lymphoma undergoing multiagent chemotherapy.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Daniëls LA, Oerlemans S, Krol AD, van de Poll-Franse LV, Creutzberg CL. Persisting fatigue in Hodgkin lymphoma survivors: A systematic review. Ann Hematol. 2013;92:1023–32. doi: 10.1007/s00277-013-1793-2. [DOI] [PubMed] [Google Scholar]
- 2.Dodd MJ, Miaskowski C, Paul SM. Symptom clusters and their effect on the functional status of patients with cancer. Oncol Nurs Forum. 2001;28:465–70. [PubMed] [Google Scholar]
- 3.Taso CJ, Lin HS, Lin WL, Chen SM, Huang WT, Chen SW, et al. The effect of yoga exercise on improving depression, anxiety, and fatigue in women with breast cancer: A randomized controlled trial. J Nurs Res. 2014;22:155–64. doi: 10.1097/jnr.0000000000000044. [DOI] [PubMed] [Google Scholar]
- 4.Komatsu H, Yagasaki K, Yamauchi H, Yamauchi T, Takebayashi T. A self-directed home yoga programme for women with breast cancer during chemotherapy: A feasibility study. Int J Nurs Pract. 2016;22:258–66. doi: 10.1111/ijn.12419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982;5:649–55. [PubMed] [Google Scholar]
- 6.Hlubocky FJ, Webster K, Cashy J, Beaumont J, Cella D. The development and validation of a measure of health-related quality of life for non-Hodgkin's lymphoma: The functional assessment of cancer therapy – Lymphoma (FACT-Lym) Lymphoma. 2013. [Last accessed on 2018 Feb 21]. Available from: https://www.hindawi.com/journals/lymph/2013/147176/
- 7.Yellen SB, Cella DF, Webster K, Blendowski C, Kaplan E. Measuring fatigue and other anemia-related symptoms with the functional assessment of cancer therapy (FACT) measurement system. J Pain Symptom Manage. 1997;13:63–74. doi: 10.1016/s0885-3924(96)00274-6. [DOI] [PubMed] [Google Scholar]
- 8.Buysse DJ, Reynolds CF, 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989;28:193–213. doi: 10.1016/0165-1781(89)90047-4. [DOI] [PubMed] [Google Scholar]
- 9.Kochhar PH, Rajadhyaksha SS, Suvarna VR. Translation and validation of brief patient health questionnaire against DSM IV as a tool to diagnose major depressive disorder in Indian patients. J Postgrad Med. 2007;53:102–7. doi: 10.4103/0022-3859.32209. [DOI] [PubMed] [Google Scholar]
- 10.Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch Intern Med. 2006;166:1092–7. doi: 10.1001/archinte.166.10.1092. [DOI] [PubMed] [Google Scholar]
- 11.Firdous S, Mehta Z, Fernandez C, Behm B, Davis M. A comparison of numeric pain rating scale (NPRS) and the visual analog scale (VAS) in patients with chronic cancer-associated pain. J Clin Oncol. 2017;35(31 Suppl):217. [Google Scholar]
- 12.International Day of Yoga. Common yoga protocol. New Delhi: Ministry of AYUSH. Government of India; 2016. Jun 21st, Ministry of Ayurveda,Yoga and Naturopathy, Unani, Sidha and Homoeopathy (AYUSH) pp. 3–36. 2016. [Google Scholar]
- 13.Fortner BV, Tauer KW, Okon T, Houts AC, Schwartzberg LS. Experiencing neutropenia: Quality of life interviews with adult cancer patients. BMC Nurs. 2005;4:4. doi: 10.1186/1472-6955-4-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lin KY, Hu YT, Chang KJ, Lin HF, Tsauo JY. Effects of yoga on psychological health, quality of life, and physical health of patients with cancer: A meta-analysis. Evid Based Complement Alternat Med. 2011;2011:659876. doi: 10.1155/2011/659876. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Cohen L, Warneke C, Fouladi RT, Rodriguez MA, Chaoul-Reich A. Psychological adjustment and sleep quality in a randomized trial of the effects of a Tibetan yoga intervention in patients with lymphoma. Cancer. 2004;100:2253–60. doi: 10.1002/cncr.20236. [DOI] [PubMed] [Google Scholar]