

Abstract
Objective
We aimed to investigate the effects of migraine and tension-type headaches (TTH) on female sexual function.
Material and methods
In this prospective study, sexually active females; 45 who were suffering from migraines, 47 who were TTH patients as diagnosed by a neurology clinic, and 50 who were healthy women that served as the control group were included. Sexual functions of the cases were evaluated through the Female Sexual Function Index (FSFI) with Turkish validation and the results were compared among the groups.
Results
There was no significant difference between the ages and body mass index (BMI) of the migraine, TTH, and control groups. Although there was no significant difference between the FSFI scores of women with migraines and TTH, the FSFI scores of these two groups were found to be statistically significantly lower than that of the control group (16.77±4.27, 17.56±3.47, 26.81±3.19) (p<0.001). When all subgroup scales of FSFI scores were examined, both migraine and TTH groups were found to be significantly lower than the control group (p<0.001).
Conclusion
This study shows that migraines and TTH disrupt the quality of life for patients and cause female sexual dysfunction. Therefore, it is important that patients with neurologic disorders are also evaluated for sexual dysfunction.
Keywords: Female sexual dysfunction, migraine, tension-type headache
Introduction
The migraine is a common disease with a prevalence of 3–35 percent of the population and is more common in women than it is in men. It is more prevalent for those between the ages of 30–50.[1,2] It is a disease accompanied by a severe headache, nausea, vomiting, and light and/or sound sensitivity. A migraine diagnosis is made clinically.
Tension-type headaches (TTH) are the most common type of headache in society.[1] A typical TTH has a bilateral, mild to moderate, non-throbbing pain pattern. The pain is felt as blunt, pressure, or compression. Blood test results, brain radiographic images, and spinal fluid analysis come back normal.
Sexuality is an important part of human life. It is a multidimensional, complex phenomenon with biological, social, interpersonal, and cultural aspects.[3] Sexual function is closely related to a large number of different organ systems, including the neurological, mental, vascular, and endocrine systems.[4] Sexual dysfunction is defined as a level of impairment that can be caused by interpersonal difficulties and stress in psychophysiological changes that constitute the cycle of sexual desire or sexual response.[5]
Although there are established definitions, epidemiological data, diagnostic methods, and treatments for male sexual dysfunction, studies on female sexual dysfunction (FSD) are still in the developmental phase. The aforementioned advances have served to increase the rates of admission to physicians for patients in developed countries due to sexual problems. In a study conducted by Berman et al.[5], 42 percent of women with sexual complaints consulted a physician and 54 percent of those who did not seek a consultation indicated that, in truth, they desired one.
Migraines and TTH significantly affect the productivity of individuals and their daily activities.[1] Studies on sexual dysfunctions of migraine and TTH patients have shown different results.[6–8] It has also been demonstrated that chronic pain can cause sexual dysfunction.[9–11] Ambler et al.[11], in their review of such literature, stated that chronic pain has an adverse effect on sexual desire, stimulation, and activity. It has also been reported that the dopamine-prolactin axis plays an important role in some primary headaches-especially migraines.[6]
In this study, we aimed to investigate the effect of migraines and tension-type headaches-which are closely associated to quality of life-on female sexual functions.
Material and methods
This study was performed as prospective, single center, and cross-sectional, while also using a control group. The ethics committee permission was obtained from the Samsun Training and Research Hospital (reference number: 33646832). Forty-five migraine and forty-seven TTH suffering female patients, who were sexually active and newly diagnosed according to the diagnostic criteria required by the neurologist, were enrolled in the study. The control group consisted of fifty healthy women from the same age group.
The age at onset and duration of the disease were questioned, the neurological examinations of the patients were performed, and the medications used were recorded. Informed consent forms were obtained from the patients diagnosed with migraines and TTH by the neurology clinic after informing them about the study. Then, a detailed history of all patients was introduced to the study; the history included demographics, known diseases, past surgical procedures, smoking habits, alcohol habits, sexual life status, and urology physicians asked about any history of urogenital disease. Patients were then asked to complete the Female Sexual Function Index (FSFI) with a Turkish validation sexual function index.[12] FSFI is a six-aspect measure of sexual desire, arousal, lubrication, orgasm, satisfaction, and pain across 19 questions that were developed by Rosen et al.[13] in 2000 to evaluate female sexual function. Higher scores indicate better sexual function. A total FSFI score under 26.55 indicates low sexual function, with domain scores below 3.6 signifying abnormal function in the respective areas. Patients with known hormonal dysfunction and/or are receiving treatment for this reason, those diagnosed with psychiatric reasons and being treated for this purpose, and patients with malignities were excluded from the study.
Statistical analysis
IBM Statistical Package for the Social Sciences (IBM SPSS Corp.; Armonk, NY, USA) version 23 software was used for statistical evaluations. The Shapiro Wilk test was used for compliance with normal distribution. The one way ANOVA was used for statistical analysis, and the Kruskal Wallis test was used for comparison of quantitative data without normal distribution. The results are presented in mean (± SD) and frequency (percent). The significance level was taken as p<0.05.
Results
Forty-five migraine-suffering patients and forty-seven TTH-suffering patients, all of whom sexually active females, and fifty healthy women from the same age group were enrolled in this study. There was no significant difference between the average age or body mass index (BMI) of these three groups (Table 1). The rates of smoking were 24% in the control group, 23% in the TTH group and, 22% in the migraine group respectively.
Table 1.
Comparison of age, BMI, FSFI and FSD percentile of migraine, TTH and control groups
| Control | Migraine | TTH | p | |
|---|---|---|---|---|
| Age (years) | 37.0±1.43 | 36.6±1.06 | 37.18±1.53 | 0.310 |
| BMI (kg/m2) | 25.70±0.78 | 25.46±0.86 | 27.08±0.61 | 0.106 |
| FSFI | 26.81±3.19 | 16.77±4.27 | 17.56±3.47 | <0.001* |
| FSD (%) | 40% (n=20) | 65% (n=29) | 60% (n=28) | 0.025 |
BMI: body mass index; FSFI: female sexual function index; FSD: female sexual dysfunction; TTH: tension-type headaches
Although there was no significant difference between the FSFI scores of women with migraines and TTH, the FSFI scores of these two groups were found to be statistically significantly lower than the control group
The mean FSFI of the migraine, TTH, and control groups was 16.77±4.27, 17.56±3.47, and 26.81±3.19, respectively; the FSFI scores of migraine and TTH groups were statistically significantly lower than the control group (p<0.001). There was no statistically significant difference between the migraine and TTH group. When subgroup scales of the FSFI scores were examined, all subgroup scales of the migraine and TTH groups were found to be significantly lower than that of the control group (p<0.001) (Figure 1). Characteristic comparisons of the cases are summarized in Table 2.
Figure 1.
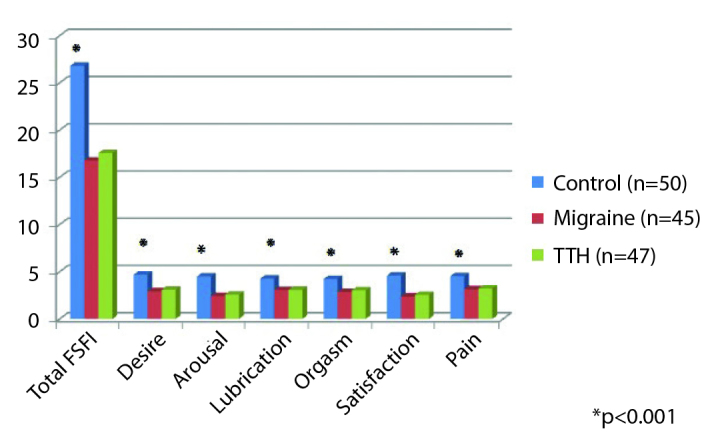
Comparison of FSFI subgroup scores of the groups
*Although there was no significant difference between the FSFI scores of women with migraines and TTH, the FSFI scores of these two groups were found to be statistically significantly lower than the control group
Table 2.
Comparison of the groups by FSFI and subgroup scales
| Control (n=50) | Migraine (n=45) | TTH (n=47) | p* | |
|---|---|---|---|---|
| Total FSFI | 26.81±3.19 | 16.77±4.27 | 17.56±3.47 | <0.001 |
| Desire | 4.69±0.88 | 2.92±1.48 | 3.10±1.10 | <0.001 |
| Arousal | 4.50±1.02 | 2.42±1.33 | 2.58±1.02 | <0.001 |
| Lubrication | 4.27±1.15 | 3.06±1.66 | 3.08±0.90 | <0.001 |
| Orgasm | 4.23±1.09 | 2.85±1.14 | 3.03±1.04 | <0.001 |
| Satisfaction | 4.60±1.26 | 2.38±1.60 | 2.55±1.26 | <0.001 |
| Pain | 4.53±1.04 | 3.15±1.14 | 3.22±1.06 | <0.001 |
FSFI: female sexual function index; TTH: tension-type headaches
Although there was no significant difference between the FSFI scores of women with migraines and TTH, the FSFI scores of these two groups were found to be statistically significantly lower than the control group
In addition, the percentage of patients with sexual dysfunction according to the FSFI 26.55 cut-off was 65 percent in the migraine group and 60 percent in the TTH group. These values were significantly higher than that of the control group, which was 40 percent (p=0.025) (Table 1).
Discussion
Sexual dysfunction is an important health problem with myriad medical and social effects. It often cannot be expressed due to societal and cultural pressures and seriously disturbs the individual’s quality of life.[14] There are several prevalence studies for European countries in literature. In a study that Braun et al.[15] conducted on 3,145 sexually active women, the prevalence of FSD was 31.1 percent. In Turkey, the prevalence study conducted by Cayan et al.[16] indicated that the prevalence of FSD by age was as follows: 21.7 percent between the ages of 18–27, 25.5 percent between the ages of 28–37, 53.5 percent between the ages of 38–47, 65.9 percent between the ages of 48–57, and 92.9 percent between the ages of 58–67. In our study, FSD was prevalent in 40 percent of the control group, 65 percent in the migraine group, and 60 percent in the TTH group.
Several risk factors were examined in all studies, and smoking, length of marriage, past pelvic surgery, and contraceptive methods were found to not be risk factors for FSD; conversely, age, education level, unemployment, chronic disease, pregnancy, multiparity, and menopause were considered significant risk factors.[15–18]
The complexity of sexual response is universally known and there are many possible explanations for the link between primary headache and sexual dysfunction. In general, chronic pain has adverse effects on sexual desire, stimulation, and activity.[11] Indeed, women with a history of primary headaches are affected by a chronic condition that can affect pain thresholds and nociceptive pathways at different levels and impair genital arousal and orgasm function.[19] In addition, medical conditions, especially mood disorders, are very common in primary headache sufferers and can significantly affect the neuroendocrine balance involved in the mechanisms controlling sexual arousal, mental stimulation, and overall satisfaction.[20,21] On the other hand, symptomatic medications such as psychoactive substances, beta-blockers, and painkillers may affect the modulation of neurotransmitters on both the central and peripheral systems.[22] Finally, various instinctual and interpersonal factors associated with the headache condition may be responsible for a negative attitude toward sexual behavior between couples.[23]
A limited number of studies evaluating the effects of primary headaches on sexual function, which are common in almost all populations, are available. Del et al.[24] observed a higher rate of self-reported masturbation in the control group, although they did not observe a difference in sexual desire between the headache and control groups. In another study, Ifergane et al.[7] reported that in researching migraine and sexual dysfunction in female students, there was more pain and less satisfaction during sexual activity in the migraine group despite there being no difference in sexual activity, desire, or orgasm frequency between the migraine and control groups. These researchers concluded that migraines adversely affect sexual life. In our study, FSD is more prevalent in migraine and TTH patients than the control group, but there was no significant difference between the migraine group and the TTH group.
In the evaluation performed by Bestepe et al.[25] using the Arizona Sexual Experiences Scale (ASEX), all parameters, except satisfaction, in the subgroup scores for sex drive, sexual stimulation, penile erection or vaginal lubrication, orgasm, and orgasmic satisfaction in the migraine group and 5 sub-parameters of ASEX in the TTH group were found to be lower than the control group. In our study, all parameters of FSFI, such as sexual desire, arousal, lubrication, orgasm, satisfaction, and pain were found to be significantly lower in both the migraine and TTH groups than the control group. In the evaluation between the migraine group and the TTH group, Bestepe et al.[25] concluded that tension-type headaches are associated with higher levels of sexual dysfunction as compared to migraines.
Another study based on the hypothesis that migraines and sexual drive could be modified with similar serotonergic systems suggests that migraine patients report a higher sexual drive than tension-type headache patients.[8] Our study, similar to the study conducted by Nappi et al.[26], did not show a significant difference in terms of FSD between migraine and TTH patients. These differences between studies may be due to symptomatic treatments used by patients. For example, the chronic use of triptans may have adverse effects on female desire and stimulation via the serotonergic system.[27] It is also known that sexual dysfunction increases with age in women.[28,29] For this reason, differences in sexual function between studies may also be due to age differences in the studied populations. Similarly, some characteristics of migraines, such as the frequency of attacks, may have produced this difference through the study population.[30]
There were some limitations of our study: we could not evaluate some conditions that may affect sexual function, such as anxiety and depression, in our patients. In addition, cultural and religious differences specific to our country may have had an influence on our results. For this reason, there is a need for more extensive studies to be conducted by taking these parameters into account.
A primary headaches are a condition more frequently observed in women and severely impairs their quality of life. In our study, we examined the effects of migraines and TTH on female sexual functions frequently observed in society and found negative effects on female sexual function in both diseases. For this reason, it should be taken into account that women with these types of primer headaches that are frequently observed in society may suffer from serious sexual dysfunction and these patients should be evaluated for sexual dysfunction.
Footnotes
Ethics Committee Approval: Ethics committee approval was received for this study from the ethics committee of Samsun Training and Research Hospital (Reference number: 33646832).
Informed Consent: Written informed consent was obtained from patients who participated in this study.
Peer-review: Externally peer-reviewed.
Author Contributions: Concept - M.A.; Design - M.A.; Supervision - M.A., M.K.A.; Resources - M.A., A.B.; Materials - M.A.; Data Collection and/or Processing - M.A., A.Y., C.M.; Analysis and/or Interpretation - M.A., L.İ., A.B.; Literature Search - M.A., L.İ., A.Y.; Writing Manuscript - M.A., A.B.; Critical Review - M.A., A.B., L.İ., A.Y., C.M., M.K.A.; Other - M.A., C.M., M.K.A.
Conflict of Interest: The authors have no conflicts of interest to declare.
Financial Disclosure: The authors declared that this study has received no financial support.
References
- 1.Rasmussen BK. Epidemiology of headache. Cephalalgia. 2001;21:774–7. doi: 10.1046/j.1468-2982.2001.00248.x. [DOI] [PubMed] [Google Scholar]
- 2.Breslau N, Rasmussen BK. The impact of migraine: epidemiology, risk factors, and co-morbidities. Neurology. 2001;56:4–12. doi: 10.1212/WNL.56.suppl_1.S4. [DOI] [PubMed] [Google Scholar]
- 3.Gökyıldız S, Beji NK. The effect of pregnancy on sexual life. J Sex Marital Ther. 2005;31:201–15. doi: 10.1080/00926230590513410. [DOI] [PubMed] [Google Scholar]
- 4.Fitzpatrick LA. Libido and The Perimenopausal Women. Menapouse. 2004;11:136–7. doi: 10.1097/01.GME.0000115558.48673.46. [DOI] [PubMed] [Google Scholar]
- 5.Berman J, Berman L, Goldstein I. Female Sexual Dysfunction: Insidence, Pathophsysiology, Evoluation and Treatment Options. Urology. 1999;54:385–91. doi: 10.1016/S0090-4295(99)00230-7. [DOI] [PubMed] [Google Scholar]
- 6.Bosco D, Belfiore A, Fava A, De Rose M, Plastino M, Ceccotti C, et al. Relationship between high prolactin levels and migraine attacs in patients with microproactinoma. J Headache Pain. 2008;9:103–7. doi: 10.1007/s10194-008-0016-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ifergane G, Ben-Zion IZ, Plakht Y, Regev K, Wirguin I. Not only headache: higher degree of sexual pain symptoms among migraine sufferers. J Headache Pain. 2008;9:113–7. doi: 10.1007/s10194-008-0028-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Houle TT, Dhingra LK, Remble TA, Rokicki, Penzien DB. Not tonight I have a headache? Headache. 2006;46:983–90. doi: 10.1111/j.1526-4610.2006.00470.x. [DOI] [PubMed] [Google Scholar]
- 9.Kwan KS, Roberts LJ, Swalm DM. Sexual dysfunction and chronic pain: the role of psychological variables and impact on quality of life. Eur J Pain. 2005;9:643–52. doi: 10.1016/j.ejpain.2004.12.008. [DOI] [PubMed] [Google Scholar]
- 10.Kalichman L. Association between fibromyalgia and sexual dysfunction in women. Clin Rheumatol. 2009;28:365–9. doi: 10.1007/s10067-009-1093-3. [DOI] [PubMed] [Google Scholar]
- 11.Ambler N, Williams AC, Hill P, Gunary R, Cratchley G. Sexual difficulties of chronic pain patients. Clin J Pain. 2001;17:138–45. doi: 10.1097/00002508-200106000-00006. [DOI] [PubMed] [Google Scholar]
- 12.Oksuz E, Malhan S. Reliability and validity of the Female Sexual Function Index in Turkish population. Sendrom. 2005;17:54–60. [Google Scholar]
- 13.Rosen R, Brown C, Heiman J, Leiblum S, Meston C, Shabsigh R, et al. The female sexual function index (FSFI): a multidimensional self-report instrument for the assessment of female sexual function. J Sex Marital Ther. 2000;26:191–208. doi: 10.1080/009262300278597. [DOI] [PubMed] [Google Scholar]
- 14.Ege E, Akın B, Yaralı Arslan S, Bilgili N. Prevalence and Risk Factors of Female Sexual Dysfunction Among Healthy Women. TUBAV Bilim. 2010;3:137–44. [Google Scholar]
- 15.Braun M, Korda B, Sommer F, Engelmann UH. Prevelence and therapy necessity of sexual dysfunction (FSD), a different look at the epidemiology of female sexual disorders: results of the “Cologne 20000 men survey”. J Urol. 2004;171(Suppl):A888. [Google Scholar]
- 16.Çayan S, Akbay E, Boslu M, Canbolat B, Acar D. The prevalence of female sexual dysfunction and potential risk factors that may impair sexual function in Turkish Women. Urol Int. 2004;72:52–7. doi: 10.1159/000075273. [DOI] [PubMed] [Google Scholar]
- 17.Aydin M, Cayonu N, Kadihasanoglu M, Irkilata L, Atilla MK, Kendirci M. Comparison of Sexual Functions in Pregnant and Non-Pregnant Women. Urol J. 2015;12:2339–44. [PubMed] [Google Scholar]
- 18.Oksuz E, Malhan S. Prevalence and risk factors for female sexual dysfunction in Turkish Women. J Urol. 2006;175:654–8. doi: 10.1016/S0022-5347(05)00149-7. [DOI] [PubMed] [Google Scholar]
- 19.Bezov D, Ashina S, Jensen R, Bendtsen L. Painperception studies in tension-type headache. Headache. 2011;51:262–71. doi: 10.1111/j.1526-4610.2010.01768.x. [DOI] [PubMed] [Google Scholar]
- 20.Jenser R, Stovner LJ. Epidemiology and comorbidity of head-ache. Lancet Neurol. 2008;7:354–61. doi: 10.1016/S1474-4422(08)70062-0. [DOI] [PubMed] [Google Scholar]
- 21.Antonaci F, Nappi G, Galli F, Manzoni GC, Calabresi P, Costa A. Migraine and psychiatric comorbidity: A review of clinical findings. J Headache Pain. 2011;12:115–25. doi: 10.1007/s10194-010-0282-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Basson R, Schultz WW. Sexual sequelae of general medical disorders. Lancet. 2007;369:409–24. doi: 10.1016/S0140-6736(07)60197-4. [DOI] [PubMed] [Google Scholar]
- 23.Lipton RB, Bigal ME, Kolodner K, Stewart WF, Liberman JN, Steiner TJ. The family impact of migraine: Population-based studies in the USA and UK. Cephalalgia. 2003;23:429–40. doi: 10.1046/j.1468-2982.2003.00543.x. [DOI] [PubMed] [Google Scholar]
- 24.Del BE, Conti C, Poggioni M, Sicuteri F. Sexuality and headache. Adv Neurol. 1982;33:209–14. [PubMed] [Google Scholar]
- 25.Bestepe E, Cabalar M, Kucukgoncu S, Calıkusu C, Ornek F, Yayla V, et al. Sexual dysfunction in women with migraine versus tension-type headaches: A comparative study. Int J Impot Res. 2011;23:122–7. doi: 10.1038/ijir.2011.16. [DOI] [PubMed] [Google Scholar]
- 26.Nappi RE, Terreno E, Tassorelli C, Sances G, Allena M, Guaschino E, et al. Sexual function and distress in women treated for primary headaches in a tertiary university center. J Sex Med. 2012;9:761–9. doi: 10.1111/j.1743-6109.2011.02601.x. [DOI] [PubMed] [Google Scholar]
- 27.Loder E. Triptan therapy in migraine. N Engl J Med. 2010;363:63–70. doi: 10.1056/NEJMct0910887. [DOI] [PubMed] [Google Scholar]
- 28.Laumann EO, Paik A, Rosen RC. Sexual dysfunction in the United States: prevalence and predictors. JAMA. 1999;281:537–44. doi: 10.1001/jama.281.6.537. [DOI] [PubMed] [Google Scholar]
- 29.Nobre PJ, Pinto-Gouveia J, Gomes FA. Prevalence and comorbidity of sexual dysfunctions in a Portuguese clinical sample. J Sex Marital Ther. 2006;32:173–82. doi: 10.1080/00926230500442334. [DOI] [PubMed] [Google Scholar]
- 30.Launer LJ, Terwindt GM, Ferrari MD. The prevalence and characteristics of migraine in a population-based cohort: the GEM study. Neurology. 1999;53:537–42. doi: 10.1212/WNL.53.3.537. [DOI] [PubMed] [Google Scholar]