

Abstract
Because of the long and variable learning curve of laparoscopic surgery, before its actual application, a well-designed practical simulating instruments like laparoscopic training boxes are needed. But because of unfavourable cost-effectiveness and huge sizes of these boxes, surgeons hardly procure, and carry them. We aimed to design a new, cheap, light and handy laparoscopic training box. Our training box is made of aluminium and used with smartphone or tablet. There is no need for a power unit. Our foldable box has dimensions of 52×38×4 cm, and weighs 2.8 kg and foldable. There are 5 working ports in it. Compared to its alternatives “Fu-Lap T-Box” is much cheaper, lighter and more comfortable. In our opinion it is possible to design and use a new cheaper and portable simulator to gain more hands-on experience before the real surgery.
Keywords: Laparoscopy, surgical training, training box
Introduction
Laparoscopic surgery continues to become the golden standard treatment in many branches today. Long and changing learning curve of laparoscopic surgery has created the requirement to develop laparoscopic surgery skills before performing surgery on human beings. A high range of application models changing from laparoscopic training boxes (LTBs) for both laparoscopic and robotic surgery to living animal and human cadaver models are available. The interest increases towards virtual operators where standard techniques or a complete procedure can be studied. The general presumption is the certain requirement for using non-living models before passing to living models.[1] This is due to the fact that laparoscopic surgeries contain the concurrent coordination among surgeon’s hands, brain and eyes.
Non-living training models provide opportunity for useful manoeuvres such as touching areas of different height and depth in the area passing objects between the instruments, towards the obstacles, cutting and tissue manipulation. Real operation scenarios can be imitated by using different kinds of materials such as paper, sponge, gloves and tubes made of rubber and may thus play the main roles in acquiring general skills.
Non-living animal tissue models can also be used. Its advantage is to create a more realistic environment by creating a real touch of tissue. Generally cheap tissues which can be acquired from butchers and markets are used. For example after separating chicken gizzard and esophagus, it is laparoscopically stitched in a way imitating vesicourethral anastomosis or pyeloplasty.[2]
Despite many models available in the market, our aim in this study was to present Fu-Lap T-Box (Functional Laparoscopic Training Box) which is ergonomic and cheap, easy to setup and end, doesn’t require a separate energy source. Besides it can provide training without connecting to computer and monitor. It does not occupy much space, and provides usage comfort.
Material and methods
It has an imaging system, and a suitable box for locating standard LTB ports, source of light and camera/lens. The angle formed between the right and left hand instruments for optimal position should be between 25 and 45 degrees and the angle between the instruments and horizontal plane should be less than 55 degrees.[3] Training boxes containing in-house camera carriers which make LTB much more practical without requiring the help of a “camera user”. Because you may use the smartphone/tablet focus properties. But these are expensive and high-volume commercial simulators whose procurement, and transport may be problematic for the clinics and interested surgeons.
We aimed to design affordable, light, robust, durable, easy to carry and practical LTB to be used in laparoscopic surgical training. Our model is formed by three main plates. Due to its foldability, it can easily turn into a triangular prism during use and thin rectangular prism in storage mode (Figure 1).
Figure 1.

Our model can easily turn into triangular prism during use
There are five ports with a width of 6–10 mm on the plate where the trocar entrances and imaging mechanism (smartphone or tablet) are located. We planned the distance between the ports in line with five finger-rule in the horizontal plan and four finger rule in the vertical plan. We designed the port entrances with an angular distance of 10 to 45 degrees between the horizontal plane and instruments. The box has a posterior plate and it is formed by three rectangular spaces providing a decrease in volume when folding. It constitutes the base of the model. A threaded holder mechanism keeps the materials to be studied steady.
Due to its advantages such as removing the requirement for camera user, preventing the high cost caused by an additional imaging system, removing the need for a separate energy source and usability anywhere, we designed the imaging system of training box in line with personal smartphone or tablet use (Table 1).
Table 1.
Fu-Lap T-Box
| You need | You don’t need |
|---|---|
| Training box (Fu Lap T-Box) | Energy |
| A smartphone/Tablet | VGA cable |
| Lap. Instruments | Webcam |
| Laptop or PC | |
| Screen |
The monitoring device (smartphone or tablet) was placed on the plate indicated with red arrow. This plate is to carry the device. The back camera of the monitoring device was adjusted to the space pointed with blue arrow and the inner side of the training box was observed (Figure 2). Thus the finished product has a foldable aluminium box with dimensions of 52×38×4 cm and a weight of 2.8 kg which costed nearly $55.
Figure 2.

Foldable aluminium box with dimensions of 52×38×4 cm and a weight of 2.8 kg costed nearly $55
Discussion
Surgical competence is defined by technical and non-technical skills.[4] Traditionally, these skills required to operate and care for a real patient are transferred from the master to the apprentice during the training period. Non-technical skills such as surgical adjudication, anticipating and refraining from the problems and economical acting can be acquired only under the surveillance of an experienced mentor and through experience. They can be acquired during real operational procedures or simulation trainings with technical skills.
In a study made in University of California in 2010, a laparoscopic renal surgical study was made in a training model of nearly five days and it was reported that 73% of the students applied laparoscopic renal surgery after three years.[5] A similar situation was observed also in robotic surgery training and 90% of 47 urologists taking a 5 days long simulation training for robotic radical prostatectomy applied this procedure in their own practices in three-year follow-up.[6]
One of the most important issues which should be considered in simulation design is acting close to the anatomic reality. In fact, rectangle is the combination of triangular prisms rather than rectangular prisms contrary to the general belief (Figure 3). For example laparoscopic renal, adrenal, liver or gall bladder surgeries are classically applied within this triangular area. Most of standard boxes are designed in the shape of a prism and drift away from this anatomic reality. We think that rectangular prism shaped models are not ergonomic when we consider especially the port entrances and the arm-elbow angle and postures. When the disadvantages mentioned above are considered, we think that a training model designed in the shape of a triangular prism would be more appropriate.
Figure 3.
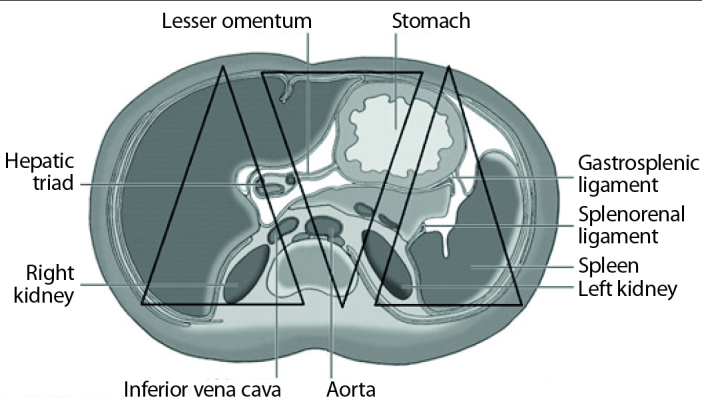
The combination of triangular prisms
Although the benefit of these training models in the development of technical surgical skills is proven, it is known that they cannot be used satisfactorily. In addition to the difficulty of its procurement due to its higher cost, and many difficulties related to the comfort of use for the training boxes can be the reason. Many users cannot effectively use their LTBs due to the requirement of an additional monitor, connection cable and additional energy requirement for source of light. The requirement for additional monitor, connection cable and additional energy source is removed as the vision is directly provided through personal smartphone/tablet in the Fu-Lap T-Box we designed.
Similarly many users can not carry their LTBs with them as the box is heavy and bulky. This disadvantage limits the usability of the training models. Today, a box which can be directly used with the personal smartphones/tablets all users carry and can be folded on itself, has a relatively lower volume and weight which provides a benefiting opportunity for the users anytime and anywhere.
According to LTB users, the most important difficulty is encountered when terminating the setup and use of LTB. Lee et al.[7] stated that the setup of LTB designed could be terminated within less than 20 minutes in a study they made. Ending operations for both setup and use of Fu-Lap T-Box model take a few minutes (1–3 minutes). We believe that this characteristic will increase the usage motivation of LTB.
Speculative data on the average cost of LTBs available in the literature. For example, while Lee et al.[7] reported LTB cost to be nearly $60, Newmark et al.[8] reported the standard LTB cost to be nearly $1463. The cost of LTBs vary widely as we can understand. The cost of Fu-Lap T-Box we designed is nearly $55.
There are many virtual reality training materials designed commercially for laparoscopic and robotic surgical training apart from standard LTB, as living animal and cadaver models. It can be stated that they are still in experimental development stage due to their higher cost as new software and advanced technology are required. But as it has been learned from the studies made, easy accessibility and affordability of this technology in the future is rather important for making this skill widespread.
We think that the cost-effectiveness of the Fu-Lap T-Box approach along with its triangular prism design, self high-definition LED screen monitoring feature without any need for additional imaging device need and ease-of-use with short installation time are the important specifications which mainly discriminate this method from others.
We think that “Fu-Lap T-Box” is a training model which is less expensive, more comfortable, practical and ergonomic. We believe that models which don’t need any energy source, can be used with smartphone or tablet or are light and easy to carry in order to make the acquirement of laparoscopic surgical skills easier.
Footnotes
An editorial comment on this article is available at page 432.
Peer-review: Externally peer-reviewed.
Author Contributions: Concept - F.U.; Design - S.A.; Supervision - A.V.; Resources - S.A., B.A.; Materials - F.U., S.A., E.U.; Data Collection and/or Processing - F.U., S.A.; Analysis and/or Interpretation - F.U., S.A., B.A., E.U.; Literature Search - S.A.; Writing Manuscript - F.U., S.A.; Critical Review - F.U., S.A.; Other - B.A., E.U., A.V.
Conflict of Interest: Authors have no conflicts of interest to declare.
Financial Disclosure: The authors declared that this study has received no financial support.
References
- 1.Pope John C. Renal Dysgenesis and Cystic Disease of the Kidney, Chapter 118. In: Wein Alan J, Kavvoussi Louis R, Novick Andrew C, Partin Alan W, Peters Craig A., editors. Campbell-Walsh Urology. 10th Edition. Vol. 4. USA: Elsevier-Saunders Publication; 2012. pp. 3161–97. [Google Scholar]
- 2.Ramachandran A, Kurien A, Patil P, Symons S, Ganpule A, Muthu V, et al. A novel training model for laparoscopic pyeloplasty using chicken crop. J Endourol. 2008;22:725–8. doi: 10.1089/end.2007.0380. [DOI] [PubMed] [Google Scholar]
- 3.Frede T, Stock C, Renner C, Budair Z, Abdel-Salam Y, Rassweiler J. Geometry of laparoscopic suturing and knotting techniques. J Endourol. 1999;13:191–8. doi: 10.1089/end.2007.0380. [DOI] [PubMed] [Google Scholar]
- 4.Hoznek A, Salomon L, de la Taille A, Yiou R, Vordos D, Larre S, et al. Simulation training in video-assisted urologic surgery. Curr Urol Rep. 2006;7:107–13. doi: 10.1089/end.2007.0380. [DOI] [PubMed] [Google Scholar]
- 5.Kolla SB, Gamboa AJ, Li R, Santos RT, Gan JM, Shell C, et al. Impact of a laparoscopic renal surgery mini-fellowship program on postgraduate urologist practice patterns at 3-year follow up. J Urol. 2010;184:2089–93. doi: 10.1089/end.2007.0380. [DOI] [PubMed] [Google Scholar]
- 6.Gamboa AJ, Santos RT, Sargent ER, Louie MK, Box GN, Sohn KH, et al. Long-term impact of a robot assisted laparoscopic prostatectomy mini fellowship training program on postgraduate urological practice patterns. J Urol. 2009;181:778–82. doi: 10.1089/end.2007.0380. [DOI] [PubMed] [Google Scholar]
- 7.Lee M, Savage J, Dias M, Bergersen P, Winter M. Box, cable and smartphone: a simple laparoscopic trainer. Clin Teach. 2015;12:384–8. doi: 10.1089/end.2007.0380. [DOI] [PubMed] [Google Scholar]
- 8.Newmark J, Dandolu V, Milner R, Grewal H, Harbison S, Hernandez E. Correlating virtual reality and box trainer tasks in the assessment of laparoscopic surgical skills. Am J Obstet Gynecol. 2007;197:546.e1–4. doi: 10.1089/end.2007.0380. [DOI] [PubMed] [Google Scholar]