

Abstract
Objective
The aim of this study was to evaluate the effectiveness of the extracorporeal shock wave therapy in the subacromial impingement syndrome and its relationship with the acromion morphology.
Methods
Thirty patients (24 women, 6 men) with subacromial impingement were evaluated. The average age of patients was 53.6 ± 9.8 years (range 39–80). Patients were divided into 3 groups according to the acromion morphology. ESWT 1500 at 0.12 am mL/mm2 violence was applied once a week for 3 weeks. Shoulder pain and disability index (SPADI) was used to assess function and pain scores of the patients. The evaluations were made prior to and 12 weeks after the ESWT.
Results
Thirteen shoulders had type 1 acromion, 11 shoulders type 2 acromion and 6 shoulders type 3 acromion. After ESWT, the SPADI pain score decreased from 16.1 ± 5.1 (7–25) to 10.4 ± 4.9 (1–20); SPADI functional score decreased from 37.3 ± 19.8 (5–70) to 26.7 ± 17.5 (1–60); SPADI total score decreased from 53.4 ± 24.5 (14–95) to 37.1 ± 21.6 (2–74) (p < 0.05; paired t test). In each group better functional outcomes were achieved after ESWT (p < 0.05; paired t test). There were no differences between the groups according to functional outcome both before and after the ESWT treatment (p > 0.05, one way ANOVA test).
Conclusion
ESWT was found to be effective in the treatment of impingement syndrome both for pain and functional outcome in the early period regardless of acromion morphology.
Level of evidence
Level IV, Therapeutic study.
Keywords: Subacromial impingement syndrome, Extracorporeal shock wave therapy(ESWT), Acromion morphology
Introduction
Subacromial Impingement Syndrome (SIS) is one of the frequent reasons of shoulder pain. Nearly half of the patients who have shoulder pain have SIS.1 The pain typically appears when the patient lifts the arm and when the subacromial and subdeltoid bursa, rotator cuff tendons or biceps long head are impinged between coracoacromial arch of the scapula and the humeral head. As the reason of the pain and the limitation in movements, a widespread spectrum of pathologies may be considered from subacromial bursitis to full-layer rotator cuff rupture. This syndrome may appear due to acromion form,2 os acromiale,3 coracoacromial ligament,4 superior part of the glenoid fossa,5 hypermobility and instability of the glenohumeral joint,6 glenohumeral capsules contraction and rotator cuff pathologies.7
The relation between the SIS and rotator cuff damage is debatable. Some authors claim that external pressure leads to the development of the rotator cuff damage.7, 8, 9 On the other hand, some other authors claim that the rotator cuff weakness leads to displacement of the humeral head upwards depending on the intrinsic tendon pathologies, and the impingement appears due to this reason.10, 11 SIS is related to acromion morphology. The fact that the anatomical shape of the acromion is important has been supported by several authors.12 In the first place, spur formation in acromion anteroinferior, calcification coracoacromial ligament, anomaly in ossification or acromion structure may be observed although there is normal acromion morphology as long as the impingement continues and increases.13 Shockwave Treatment (Extracorporeal Shock Wave Therapy = ESWT) is a treatment method in which high-amplitude sound waves are focused on the desired part of the body. This method was used for destroying the kidney and biliary tract stones in 1970s. The use of this method has become widespread in various muscle-skeleton system diseases including tendinopathy, enthesopathy and calcifications.14, 15
The calcifications occurring in the adhesion area of the coracoacromial ligament influence the acromion morphology and may lead to SIS.3 The origin of the degenerative changes and bone growth happening in acromion is the calcific accumulations in coracoacromial ligament. Shockwave treatment method is influential on the resolution of the calcification and stimulating the tissue recovery.15, 16, 17
The purpose of this study is assessing the clinical and functional results of the efficiency of the extracorporeal shockwave treatment in SIS, and investigating the influences of the acromion morphology on these results. To our knowledge, no study has searched the effect of ESWT according to the acromion types in patients with SIS in the literature.
Material and method
This study was approved by the ethics committee of the Istanbul Education and Research Hospital (2013/379). The patients were informed about the procedure and the patient consents were received. The study was organized according to Helsinki Declaration. The type of the study is Case Series.
30 patients (24 women; 6 men), who were diagnosed with subacromial impingement, were assessed in this study. The average age of the patients was 53.6 ± 9.8 years (the range 39–80). The dominant extremity of all patients was the right side. The patients who had pain and function limitation in shoulder, who had pain in internal and external rotation in isometric tests, who had at least 90° active abduction, who had 90° and over pain in front elevation with the Neer Test, who had pain in internal rotation in the arm in 90° flexion with the Hawkins Test, whose glenohumeral joint range or motion was full in passive state, who were diagnosed with Subacromial Impingement Syndrome, who did not respond to conservative treatment, and who were not given any other treatments within the last 4 weeks, were included in the study.
Those patients who had previous surgical intervention in the relevant shoulder, who had pain in both shoulders, who had instability, who had rupture in rotator cuff, who had cervical syndrome findings, rheumatoid arthritis, diabetes, thyroid function disorder, glenohumeral arthritis and acromioclavicular arthritis, calcified rotator cuff tendinitis, psychiatric diseases, anticoagulant drug use history, pregnancy, tumor or infection, were not included in the study.
In order to assess the coracoacromial arch, the shoulder anterior-posterior and supraspinatus outlet graphics were assessed first. Imaging was performed with a caudal 10° angle in scapular plan from lateral in order to assess the acromion morphology with supraspinatus outlet graphics. The supraspinatus outlet graphics and the acromion morphology were assessed as defined by Bigliani.18 The patients were separated into 3 groups as ‘Type 1; Plain, ‘Type 2; Oblique, ‘Type 3; Hook’ according to the acromion type with which the supraspinatus outlet graphics were assessed (Fig. 1a, Fig. 1b). Differential diagnoses and additional pathologies were assessed with shoulder joint magnetic resonance imaging. When the shoulder joint magnetic resonance imaging was assessed, the patients who were observed as having exclusion criteria were not included in the study.
Fig. 1a.
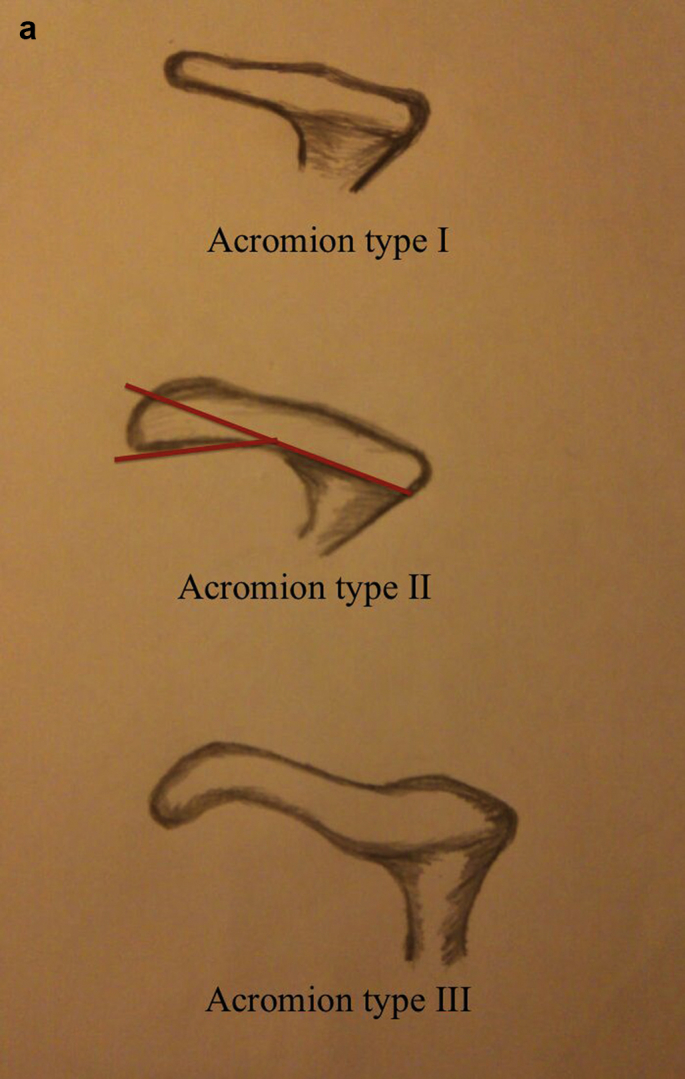
Schematic figure for acromion types.
Fig. 1b.

Type 2 acromion according to the supraspinatus outlet graphic.
3 séances once a week at a magnitude of 1500-beat ESWT (ESWT Master Plus(R) MP2000, Storz, Tagerwilen, Switzerland) 0,12 ml/mm2 focusing on the subacromial areas of the patients were applied. It was ensured that the patients did not receive any additional medical treatments before the study for at least 4 weeks and during the study.
In order to assess the functions and paint levels of the patients, Shoulder Pain and Disability Index (SPADI) was used. The pain levels (5 questions) and functional status (8 questions) were assessed with the 13 questions the index had. The assessments of the patients were performed before the treatment, and repeated 12 weeks after the ESWT application.
The SPSS Package Program was used for the statistical analyses (SPSS 17.0 for Windows, Chicago, IL, USA). This analysis revealed a standard effect size of 0.72 and at least 30 cases with a 95% confidence interval and a power of 80%. In order to assess the difference between the study groups, the one way ANOVA Test was used in continuous data which were independent from each other among the groups. The paired t test was used to assess the pre-treatment and post-treatment variables. The statistical significance value was accepted as p < 0.05.
Results
24 of the 30 patients had right shoulder complaints, and 6 of them had left shoulder complaints. At the end of the assessments of supraspinatus outlet graphics, it was determined that 13 of the patients had “Shoulder Type 1 Acromion”, 11 of the patients had “Shoulder Type 2”, and 6 of the patients had “Shoulder Type 3” Acromion. The demographic characteristics of the patients are given in Table 1.
Table 1.
Demographic features of the patients.
| Sex (n = 30) | 24 women/6 men |
|---|---|
| Acromion type 1 | 13 patient |
| Acromion type 2 | 11 patient |
| Acromion type 3 | 6 patient |
| Side | 24 right shoulder/6 left shoulder |
| Age (year) | 53.6 ± 9.8 (39–80) |
Mean ± standard deviation (minimum–maximum value).
When the patients were assessed according to the acromion types for age values, it was observed that there were no differences between the groups. The statistical assessment and the age values according to acromion types are given in Table 2 (p > 0.05, one way ANOVA test).
Table 2.
The age distribution of patients according to the type of acromion.
| Acromion type 1 | Acromion type 2 | Acromion type 3 | ||
|---|---|---|---|---|
| Age (year) | 51.2 ± 7.7 (39–64) | 57.5 ± 12.6 (41–80) | 52.0 ± 6.9 (43–76) | P = 0.47* |
Mean ± standard deviation (minimum–maximum value), * one way ANOVA test.
When all the patients were assessed after the ESWT, it was observed that the SPADI pain score regressed to 10.4 ± 4.9 (1–20) from 16.1 ± 5.1 (7–25); the SPADI functional assessment score regressed to 26.7 ± 17.5 (1–60) from 37.3 ± 19.8 (5–70); and the SPADI total score regressed to 37.1 ± 21.6 (2–74) from 53.4 ± 24.5 (14–95) (p < 0.05; paired t test). The data and the statistical assessment results are summarized in Table 3.
Table 3.
Functional evaluation results before and after ESWT for all patients.
| Before ESWT | After ESWT | ||
|---|---|---|---|
| SPADI pain score | 16.1 ± 5.1 (7–25) | 10.4 ± 4.9 (1–20) | P < 0.001* |
| SPADI functional score | 37.3 ± 19.8 (5–70) | 26.7 ± 17.5 (1–60) | P < 0.001* |
| SPADI total score | 53.4 ± 24.5 (14–95) | 37.1 ± 21.6 (2–74) | P < 0.001* |
Mean ± standard deviation (minimum–maximum value), *paired t test.
The functional assessment results of the patients were assessed separately before and after ESWT for each acromion. In each group, a recovery was determined in the functional results after the ESWT treatment. It was determined that this functional recovery level was statistically significant for each group. The distribution of the data and the statistical assessment results are given in Table 4 (p < 0.05; paired t test).
Table 4.
Functional evaluation results before and after ESWT according to acromion type.
| Acromion type 1 |
Acromion type 2 |
Acromion type 3 |
|||||||
|---|---|---|---|---|---|---|---|---|---|
| Before ESWT | After ESWT | Before ESWT | After ESWT | Before ESWT | After ESWT | ||||
| SPADI pain score | 15.1 ± 4.9 (7–22) | 9.9 ± 4.8 (1–16) | P = 0.003 | 17.0 ± 4.8 (9–25) | 10.8 ± 6.1 (3–20) | P = 0.025 | 16.8 ± 6.7 (9–22) | 11.2 ± 3.1 (8–15) | P = 0.049 |
| SPADI functional score | 32.7 ± 17.7 (8–68) | 23.2 ± 14.9 (1–48) | P = 0.006 | 40.5 ± 21.9 (5–70) | 28.5 ± 19.8 (3–60) | P = 0.026 | 42.8 ± 21.5 (17–69) | 32.4 ± 20.7 (8–60) | P = 0.031 |
| SPADI total score | 47.9 ± 22.4 (16–90) | 33.0 ± 19.2 (2–60) | p = 0.004 | 57.5 ± 26.3 (14–95) | 39.5 ± 24.6 (9–70) | P = 0.021 | 59.6 ± 27.9 (26–91) | 43.6 ± 23.4 (16–74) | P = 0.027 |
Mean ± standard deviation (minimum–maximum value), *paired t test.
When the patients were grouped according to acromion types, no difference was determined between the functional results between the groups before and after the ESWT treatment (Table 5; p > 0.05, one way ANOVA test).
Table 5.
The comparison of functional evaluation between the groups (acromion type 1, type 2 and type 3) before and after ESWT.
| Before ESWT | After ESWT | |
|---|---|---|
| SPADI pain score | P = 0.274* | P = 0.837* |
| SPADI functional score | P = 0.509* | P = 0.567* |
| SPADI total score | P = 0.529* | P = 0.602* |
*One way ANOVA test.
Discussion
Resting, activity modification, injections applied into the shoulder joint, and strengthening the muscles around the scapula are applied in conservative treatment of the SIS.19 Successful results were received with conservative treatment in most patients.8 In a prospective study, corticosteroid injection and physical treatment were applied to the shoulder joints of 100 SIS patients and the ASES values (American Shoulder and Elbow Surgeons Outcome Score) of the patients increased to 95 from 56, the pain scores regressed to 0.5 from 4.8, to 79% of the patients did not need any surgical interventions in two-year follow-up period of the patients.20 Kuhn et al determined positive effects of exercise on pain and shoulder joint functions.21 Dorrestijn et al released a compilation of studies and compared the conservative treatment and surgical treatment in SIS and reported that there were no differences between the conservative and surgical treatments.22 Conservative treatment methods preserve their popularity in the treatment of SIS.
Shockwave treatment is increasingly used for subacromial shoulder pain. It was determined in our study that the SPADI total points of patients after ESWT treatment regressed to 37.1 from 53.4; and that important recoveries were observed in functional acquisitions and in pain scores. Engebretsen et al revealed that supervised exercises were better than radial extracorporeal shockwave treatment for short term improvement of the shoulder pain and disability index in patients with subacromial shoulder pain.23 Researchers revealed that exercise therapy is an evidence-based treatment option for subacromial shoulder pain, both in short and long term.21, 24 Kvalvaag et al revealed all the patients got supervised exercises in addition to ESWT or sham for subacromial shoulder pain. They found no differences between the groups. Kvalvaag et al did not recommend shock wave treatment with subacromial pain syndrome.25 Otherwise, Santamato et al publicized that combined administration of ESWT and isokinetic exercise resulted in greater functional recovery in the short to medium term compared with ESWT alone.26 Ozturk et al concluded that ESWT treatment similarly effected physical therapy and sham ESWT treatment on shoulder pain and functional shoulder scores in patients with SIS. ESWT was assessed as an alternative method that would decrease the need for surgical interventions in rotator cuff tendinitis that was calcified and not calcified.27 Huisstede et al assessed the 17 studies, in which ESWT was applied due to rotator cuff tendinitis (calcified rotator cuff patients were included in 11 studies, and patients who did not have non-calcified tendinitis were included in 6 studies). They reported that ESWT application was efficient in the treatment of calcified tendinitis, and that it was not more efficient than the placebo and other treatment methods in non-calcified rotator cuff tendinitis.28
There are various viewpoints on the influence mechanisms of ESWT. Loew et al reported that shock waves gave increase to the pressure in the tissue they are focused, and this led to fragmentation and cavitation in calcification, and made it possible for surrounding tissues to absorb calcific particles.15 Perlick et al think that the influence mechanisms of the shock waves was not due to the physical defragmentation of the calcification, but due to the triggering of the inflammatory changes as a result of mechanical irritation caused by the shock waves.29 Wang et al on the other hand, reported that shock waves led to an increase in the blood flow in the focused tissue and stimulated recovery.30
Neer determined in a cadaver study that there were eminentia and bone growths in the front side of the acromion. He revealed that these changes were not originally in the lateral, but in the anterior with the impingement between the anterior of the humeral head of the rotator cuff and the coracoacromial ligament.3 They examined the contact between the subacromial arch and rotator cuff and the influencing load in a cadaver study, and revealed that the subacromial contact and coracoacromial ligament regression in normal shoulder appeared in all of the shoulder movements. It is expressed that this situation leads to bone eminentia and degenerative changes.31 It is considered that the eminentia and bone growths in acromion occur due to the calcifications happening in the adhesion area of the coracoacromial ligament and its effect on the acromion type.3 It was reported that these calcifications were depending especially on the tension forces in the ligament, which becomes obvious especially in shoulder abduction.32
The fact that ESWT is influential in calcific tendinitis has been demonstrated in many studies.33, 34, 35 Verstraelen et al summarized high energy shock wave therapy result in improved functional score and resorption of the deposits in their meta-analysis.36 The calcific accumulations in coracoacromial ligament cause degenerative changes and bone growth in acromion. In our study, the aim was to assess the influence of the shock waves focused on subacromial area. Recovery was observed in pain and functional assessment results of the patients with SIS after ESWT application in our study. When the patients were assessed according to the acromion types it was determined after the ESWT treatment that there was recovery in SPADI functional and paint scores. Although important recovery was determined at a significant level in the results after the treatment in each group, no difference was determined when the assessment scores of the groups before and after the treatment were compared. The acromion type ESWT treatment was not influential in the results. As a conclusion, we may suggest that the ESWT is influential in short-term follow-ups in the conservative treatment of the SIS. The limitation of our study is the fact that there is no controlled study group, and there are no long-term follow-up results.
Conclusion
It has been determined that ESWT is influential in early period in a manner that is independent from acromion morphology in recovering the pain and functional results in Subacromial Impingement Syndrome (SIS) treatment.
Footnotes
Peer review under responsibility of Turkish Association of Orthopaedics and Traumatology.
References
- 1.Roddy E., Zwierska I., Hay E.M., team St Subacromial impingement syndrome and pain: protocol for a randomised controlled trial of exercise and corticosteroid injection (the SUPPORT trial) BMC Musculoskelet Disord. 2014 Mar 14;15:81. doi: 10.1186/1471-2474-15-81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bigliani L.U., Ticker J.B., Flatow E.L., Soslowsky L.J., Mow V.C. The relationship of acromial architecture to rotator cuff disease. Clin Sports Med. 1991;10(4):823–838. [PubMed] [Google Scholar]
- 3.Neer C.S., 2nd Anterior acromioplasty for the chronic impingement syndrome in the shoulder: a preliminary report. J Bone Joint Surg Am. 1972;54(1):41–50. [PubMed] [Google Scholar]
- 4.Flatow E.L., Soslowsky L.J., Ticker J.B. Excursion of the rotator cuff under the acromion. Patterns of subacromial contact. Am J Sports Med. 1994;22(6):779–788. doi: 10.1177/036354659402200609. [DOI] [PubMed] [Google Scholar]
- 5.Edelson G., Teitz C. Internal impingement in the shoulder. J Shoulder Elbow Surg. 2000;9(4):308–315. doi: 10.1067/mse.2000.105449. [DOI] [PubMed] [Google Scholar]
- 6.Warner J.J., Micheli L.J., Arslanian L.E., Kennedy J., Kennedy R. Patterns of flexibility, laxity, and strength in normal shoulders and shoulders with instability and impingement. Am J Sports Med. 1990;18(4):366–375. doi: 10.1177/036354659001800406. [DOI] [PubMed] [Google Scholar]
- 7.Neer C.S., 2nd Impingement lesions. Clin Orthop Relat Res. 1983 Mar;(173):70–77. [PubMed] [Google Scholar]
- 8.Bigliani L.U., Levine W.N. Subacromial impingement syndrome. J Bone Joint Surg Am. 1997;79(12):1854–1868. [PubMed] [Google Scholar]
- 9.Vaz S., Soyer J., Pries P., Clarac J.P. Subacromial impingement: influence of coracoacromial arch geometry on shoulder function. Joint Bone Spine. 2000;67(4):305–309. [PubMed] [Google Scholar]
- 10.Lohr J.F., Uhthoff H.K. The microvascular pattern of the supraspinatus tendon. Clin Orthop Relat Res. 1990 May;(254):35–38. [PubMed] [Google Scholar]
- 11.Chansky H.A., Iannotti J.P. The vascularity of the rotator cuff. Clin Sports Med. 1991;10(4):807–822. [PubMed] [Google Scholar]
- 12.Toivonen D.A., Tuite M.J., Orwin J.F. Acromial structure and tears of the rotator cuff. J Shoulder Elbow Surg. 1995;4(5):376–383. doi: 10.1016/s1058-2746(95)80022-0. [DOI] [PubMed] [Google Scholar]
- 13.Neer C.S., 2nd Anterior acromioplasty for the chronic impingement syndrome in the shoulder. 1972. J Bone Joint Surg Am. 2005;87(6):1399. doi: 10.2106/JBJS.8706.cl. [DOI] [PubMed] [Google Scholar]
- 14.Ogden J.A., Alvarez R.G., Levitt R., Marlow M. Shock wave therapy (Orthotripsy) in musculoskeletal disorders. Clin Orthop Relat Res. 2001 Jun;(387):22–40. doi: 10.1097/00003086-200106000-00005. [DOI] [PubMed] [Google Scholar]
- 15.Loew M., Daecke W., Kusnierczak D., Rahmanzadeh M., Ewerbeck V. Shock-wave therapy is effective for chronic calcifying tendinitis of the shoulder. J Bone Joint Surg Br. 1999;81(5):863–867. doi: 10.1302/0301-620x.81b5.9374. [DOI] [PubMed] [Google Scholar]
- 16.Haupt G. Use of extracorporeal shock waves in the treatment of pseudarthrosis, tendinopathy and other orthopedic diseases. J Urol. 1997;158(1):4–11. doi: 10.1097/00005392-199707000-00003. [DOI] [PubMed] [Google Scholar]
- 17.Haupt G., Chvapil M. Effect of shock waves on the healing of partial-thickness wounds in piglets. J Surg Res. 1990;49(1):45–48. doi: 10.1016/0022-4804(90)90109-f. [DOI] [PubMed] [Google Scholar]
- 18.Bigliani B.U.M.E., April E.W. The morphology of the acromion and its relationship to rotator cuff tears. Orthop Trans. 1986;10:216. [Google Scholar]
- 19.Morrison D.S., Frogameni A.D., Woodworth P. Non-operative treatment of subacromial impingement syndrome. J Bone Joint Surg Am. 1997;79(5):732–737. doi: 10.2106/00004623-199705000-00013. [DOI] [PubMed] [Google Scholar]
- 20.Cummins C.A., Sasso L.M., Nicholson D. Impingement syndrome: temporal outcomes of nonoperative treatment. J Shoulder Elbow Surg. 2009;18(2):172–177. doi: 10.1016/j.jse.2008.09.005. [DOI] [PubMed] [Google Scholar]
- 21.Kuhn J.E. Exercise in the treatment of rotator cuff impingement: a systematic review and a synthesized evidence-based rehabilitation protocol. J Shoulder Elbow Surg/Am Shoulder Elbow Surg [et al] 2009;18(1):138–160. doi: 10.1016/j.jse.2008.06.004. [DOI] [PubMed] [Google Scholar]
- 22.Dorrestijn O., Stevens M., Winters J.C., van der Meer K., Diercks R.L. Conservative or surgical treatment for subacromial impingement syndrome? A systematic review. J Shoulder Elbow Surg. 2009;18(4):652–660. doi: 10.1016/j.jse.2009.01.010. [DOI] [PubMed] [Google Scholar]
- 23.Engebretsen K., Grotle M., Bautz-Holter E. Radial extracorporeal shockwave treatment compared with supervised exercises in patients with subacromial pain syndrome: single blind randomised study. BMJ. 2009;339:b3360. doi: 10.1136/bmj.b3360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Michaleff Z.A., Kamper S.J. PEDro systematic review update: the effectiveness of physiotherapy exercises in subacromical impingement syndrome. Br J Sports Med. 2013;47(14):927–928. doi: 10.1136/bjsports-2013-092750. [DOI] [PubMed] [Google Scholar]
- 25.Kvalvaag E., Brox J.I., Engebretsen K.B., Soberg H.L., Bautz-Holter E., Roe C. Is radial Extracorporeal Shock Wave Therapy (rEWST) combined with supervised exercises (SE) more effective than sham rESWT and SE in patients with subacromial shoulder pain? Study protocol for a double-blind randomised, sham-controlled trial. BMC Musculoskelet Disord. 2015;16:248. doi: 10.1186/s12891-015-0712-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Santamato A., Panza F., Notarnicola A. Is extracorporeal shockwave therapy combined with isokinetic exercise more effective than extracorporeal shockwave therapy alone for subacromial impingement syndrome? A randomized clinical trial. J Orthop Sports Phys Ther. 2016;46(9):714–725. doi: 10.2519/jospt.2016.4629. [DOI] [PubMed] [Google Scholar]
- 27.Ozturk N.S., Gelecek N., Savci S. Effects of extracorporeal shock wave therapy on subacromial impingement syndrome. Orthop J Sports Med. 2014 Nov;2(3 Suppl) [Google Scholar]
- 28.Huisstede B.M., Gebremariam L., van der Sande R., Hay E.M., Koes B.W. Evidence for effectiveness of Extracorporal Shock-Wave Therapy (ESWT) to treat calcific and non-calcific rotator cuff tendinosis–a systematic review. Man Ther. 2011;16(5):419–433. doi: 10.1016/j.math.2011.02.005. [DOI] [PubMed] [Google Scholar]
- 29.Perlick L., Luring C., Bathis H., Perlick C., Kraft C., Diedrich O. Efficacy of extracorporal shock-wave treatment for calcific tendinitis of the shoulder: experimental and clinical results. J Orthop Sci. 2003;8(6):777–783. doi: 10.1007/s00776-003-0720-0. [DOI] [PubMed] [Google Scholar]
- 30.Wang C.J., Yang K.D., Wang F.S., Chen H.H., Wang J.W. Shock wave therapy for calcific tendinitis of the shoulder: a prospective clinical study with two-year follow-up. Am J Sports Med. 2003;31(3):425–430. doi: 10.1177/03635465030310031701. [DOI] [PubMed] [Google Scholar]
- 31.Yamamoto N., Muraki T., Sperling J.W. Contact between the coracoacromial arch and the rotator cuff tendons in nonpathologic situations: a cadaveric study. J Shoulder Elbow Surg. 2010;19(5):681–687. doi: 10.1016/j.jse.2009.12.006. [DOI] [PubMed] [Google Scholar]
- 32.Chambler A.F., Bull A.M., Reilly P., Amis A.A., Emery R.J. Coracoacromial ligament tension in vivo. J Shoulder Elbow Surg. 2003;12(4):365–367. doi: 10.1016/s1058-2746(03)00031-4. [DOI] [PubMed] [Google Scholar]
- 33.Albert J.D., Meadeb J., Guggenbuhl P. High-energy extracorporeal shock-wave therapy for calcifying tendinitis of the rotator cuff: a randomised trial. J Bone Joint Surg Br. 2007;89(3):335–341. doi: 10.1302/0301-620X.89B3.18249. [DOI] [PubMed] [Google Scholar]
- 34.Gerdesmeyer L., Wagenpfeil S., Haake M. Extracorporeal shock wave therapy for the treatment of chronic calcifying tendonitis of the rotator cuff: a randomized controlled trial. JAMA. 2003;290(19):2573–2580. doi: 10.1001/jama.290.19.2573. [DOI] [PubMed] [Google Scholar]
- 35.Rompe J.D., Burger R., Hopf C., Eysel P. Shoulder function after extracorporal shock wave therapy for calcific tendinitis. J Shoulder Elbow Surg. 1998;7(5):505–509. doi: 10.1016/s1058-2746(98)90203-8. [DOI] [PubMed] [Google Scholar]
- 36.Verstraelen F.U., In den Kleef N.J., Jansen L., Morrenhof J.W. High-energy versus low-energy extracorporeal shock wave therapy for calcifying tendinitis of the shoulder: which is superior? A meta-analysis. Clin Orthop Relat Res. 2014;472(9):2816–2825. doi: 10.1007/s11999-014-3680-0. [DOI] [PMC free article] [PubMed] [Google Scholar]