

Abstract
Background:
Stroke survivors suffer from significant neuropsychiatric disturbances and these disturbances act as barrier in the motor recovery. Medication is the common treatment but it has adverse effects. Hence, there is a need to find out effective treatments with or without minimal side effects for gross motor recovery of the patient.
Objectives:
Cranial electrical stimulation (CES) and rational emotive behavior therapy (REBT) are used as treatment approaches for depression, anxiety, stress, and irrational beliefs in the general population. In the present study, the efficacy of two psycho-therapeutic modalities (CES and REBT) along with conventional physiotherapy management was evaluated on psychological illness, motor recovery, and quality of life among chronic stroke (CS) survivors.
Materials and Methods:
A total of 18 patients with CS who scored >10 on Beck Depression Inventory Scale, scored >23 on Mini–Mental state examination scale, and having stroke of duration >6 months–2 years were included in the study. They were divided into two groups, A and B. Group A received CES while Group B received REBT. Both the interventions were given 5 days in a week for 4 weeks. Conventional physiotherapy for 30 min was added to both groups as common intervention. Depression, Anxiety, Stress scale (DASS-42), Pittsburgh Sleep Quality Index (PSQI), and Shortened General Attitude and Belief Scale (SGABS) were used for measuring depression, anxiety, and stress, sleep, attitude and beliefs, respectively, 4 weeks postintervention.
Results:
Patients with CS in Group A demonstrated significant improvement, P < 0.05, in Depression, Anxiety, Stress scale-24, PSQI, and MSSI when compared to those of Group B.
Conclusion:
CES has the potential to improve psychological illness such as depression, anxiety, stress, attitudes, belief, and thereby quality of life among CS survivors than REBT.
Keywords: Anxiety, attitude, depression, electrical stimulation, quality of life
INTRODUCTION
Stroke survivors suffer from significant neuropsychiatric disturbances such as depression, anxiety, and sleep disorders. One of the most common neuropsychiatric disabilities of stroke is depression, and the National Institute of Mental Health estimated that 10%–27% of stroke survivors will experience major depression, while an additional 15%–40% will have symptoms of depression within 2 months following a stroke.[1] Moreover, poststroke depression is associated with an increased disability, increased cognitive impairment, increased mortality, and worsens the rehabilitation outcome.[2] The point prevalence rate for depression following stroke is around 31% and between 18% and 25% for significant anxiety and it likely contributes to poorer adaptive functioning and affects quality of life and relationships.[3] Other types of psychiatric morbidities which are usually seen except depression are anxiety disorders, adjustment disorders, and sexual dysfunction, which hinder the physical recovery of patients.[4]
As neuropsychiatric disturbances act as barrier in the motor recovery of stroke, it is essential to diagnose and treat these disturbances. The principal treatment which is available for depression in the general population, depressed stroke patients, and anxiety patients is anti-depressant medication, but the compliance is often compromised due to high rate of adverse effect of medicines on patient's health such as weight gain, gastrointestinal and sexual difficulties, insomnia, severe headaches, and drowsiness.[3,5] While the nondrug methods include physiotherapy, electrical stimulations such as cranial electrical stimulation (CES), transcranial direct-current stimulation, psychotherapy such as cognitive behavior therapy, rational emotive behavior therapy (REBT), and neurolinguistic programming. Due to the noncompliance issue, it is necessary to use the treatment that has minimal side effects for the management of any condition. CES has a few, mild, and self-limiting (<1%) adverse effects, which include headaches, skin irritation at electrode sites, and light-headedness may occur following treatment.[6,7] REBT is not only a set of therapeutic techniques, but also a comprehensive theory of human behavior. According to this theory, there are biological, psychological, and social factors involved in the way humans feel and behave. All human emotions and behavior are a result of what people think, assume, or believe about themselves and other people and the world in general.[8] It is an approach in psychotherapy that teaches people that their beliefs are mainly responsible for creating their emotional and behavioral reactions toward life events. People with depression have low positive emotions and high negative emotions. REBT is one of the psychotherapy approaches, which has a major role in treating psychiatric disorders, including depression.[9,10] Patients' attitudes toward their illness seem to be associated with survival after stroke and who feel that there is nothing they can do to help themselves 6 months after a stroke have a shorter survival.[11]
The relationship between the psychological illness and impairment and disability due to stroke is poorly understood by the therapist. The only goal of the physiotherapy management among stroke survivors is restoration of movement and to make person independent. Hence, in the present study, the efficacy of two psychotherapeutic modalities (CES and REBT) along with conventional physiotherapy management is evaluated on psychological illness, motor recovery, and quality of life among chronic stroke (CS) survivors.
MATERIALS AND METHODS
Recruitment and allocation
The study protocol was approved by the university research and ethics committee (PU/2016/27) and the study was done strictly in accordance with the guidelines of Helsinki declaration, revised 2013. This study was a randomized controlled trial in which efficacy of CES along with conventional physiotherapy is compared with REBT along with conventional physiotherapy. All participants signed informed consent form prior to participating in the study. The study included 18 patients with CS of duration >6 months to 2 years. The included participants were both males and females in the age range of 40–70 years. Participants who scored >10 on Beck Depression Inventory Scale were included in the study. The participants who scored ≤23 on Mini–Mental State Examination scale and who are blind, deaf, not able to speak, and had dementia were excluded from the study. After the demographics, the patients who met the inclusion criteria were allocated into two groups, CES + conventional physiotherapy (Group A) and REBT + conventional physiotherapy (Group B) by block randomization method. There were three blocks, with the matrix design of 6 × 3, where 6 being rows. Each block contained six chits (three chits for each group). The participants were allotted to the group based on the randomly chosen chit. Once the block was allotted, the next row block was opened. Thus, an equal number of participants were assigned to each group over time. Participants were blinded to their treatment allocation using sequentially numbered, opaque-sealed, envelopes. Written informed consent was obtained before commencing the study. The Consolidated Standards of Reporting Trials flow chart describing the blueprint of the study is displayed in Figure 1.
Figure 1.

Consolidated Standards of Reporting Trials diagram describing the study flow
Intervention in Group A
Patients with CS in Group A received CES along with conventional physiotherapy. CES was given by means of the pulsed, low-amplitude electrical current to the head through electrodes placed on the earlobes, usually <1 mA at 0.5 Hz from either a 9 V, AAA or AA battery.[5] CES was in lying or sitting position (as comfortable for patient) and electrodes were placed on earlobes. The CES was administered for 30 min. After the completion of CES, the conventional physiotherapy was given for rehabilitating motor impairment and each session lasted for another 30 min.
Intervention in Group B
Patients with CS in Group B received REBT and conventional physiotherapy. REBT was administered by means of counseling session by changing irrational beliefs associated with their ailment and recovery. After the completion of REBT session, conventional physiotherapy was given for 30 min to treat motor impairment.
Outcome measures
Baseline and follow-up measurements included the Depression, Anxiety, Stress scale (DASS-42), the Pittsburgh Sleep Quality Index (PSQI), and Shortened General Attitude and Belief Scale (SGABS), for measuring depression, anxiety, and stress, sleep, attitude, and beliefs, respectively. Follow-up was taken on the 11th day and on the 21st day after intervention. Both the interventions were given 5 days in a week for 4 weeks. The treatment duration was ½ h. Conventional physiotherapy was given to both the groups for another ½ h.
Data analysis
The collected demographic and outcome measures were assessed for their normality using Shapiro–Wilk test. As the data follow normal distribution, all the descriptive statistics were expressed in mean ± standard deviation. Repeated measures ANOVA was adopted to find out the differences within Group A (CES) and Group B (REBT) for pre- and post-interventional changes at baseline, 11th day, and 21st day, while independent t-test was used to compare the changes in mean values of DASS-42, PSQI, and SGABS between Group A and Group B at baseline, 11th day, and 21st day of 4-week training session. The data were analyzed using statistical software, Statistical Package for the Social Sciences (SPSS) version 20.0 (IBM Corp., Armonk, New York, USA). P ≤ 0.05 was considered to be statistically significant.
RESULTS
Eighteen patients with CS of duration >6 months to 2 years were recruited for the study. The mean age of the patients was 56.06 ± 6.10 years. Between the session and group comparison at baseline, 11th day, and 21st day of 4-week training session for the outcome measures, DASS [Figures 2–4], PSQI [Figure 5], and SGABS [Figure 6] were displayed. In all the outcome measures, Group A (CES) showed significant (P < 0.05) improvement when compared to Group B (REBT).
Figure 2.
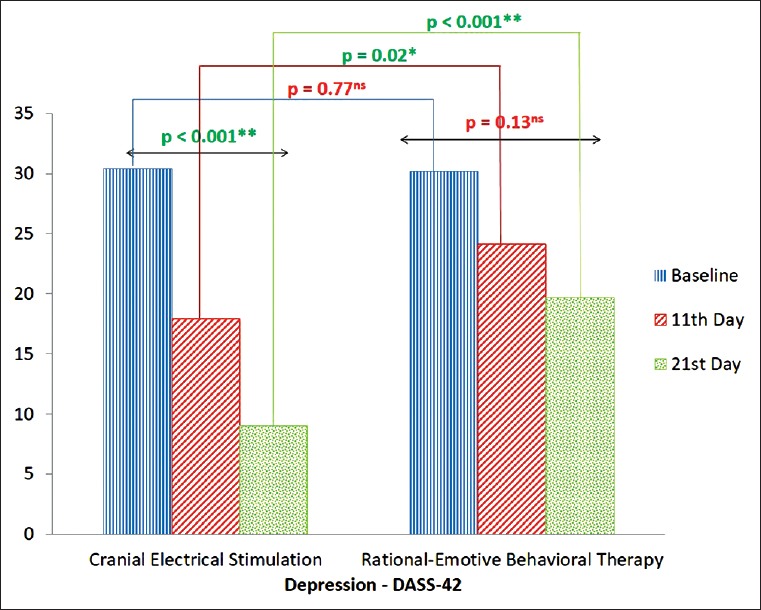
Depression, Anxiety, Stress scale-24 for depression at baseline, 11th day, and 21st day postintervention between Group A and Group B
Figure 4.
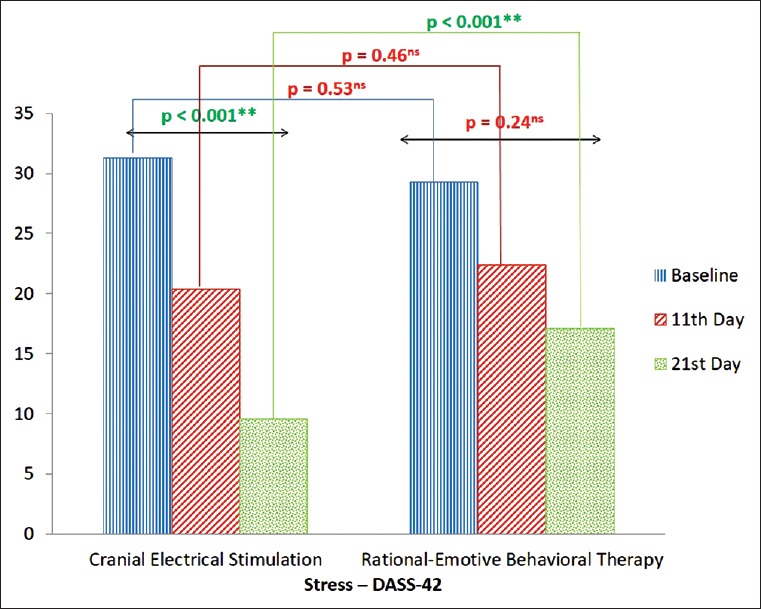
Depression, Anxiety, Stress scale-24 for stress at baseline, 11th day, and 21st day postintervention between Group A and Group B
Figure 5.
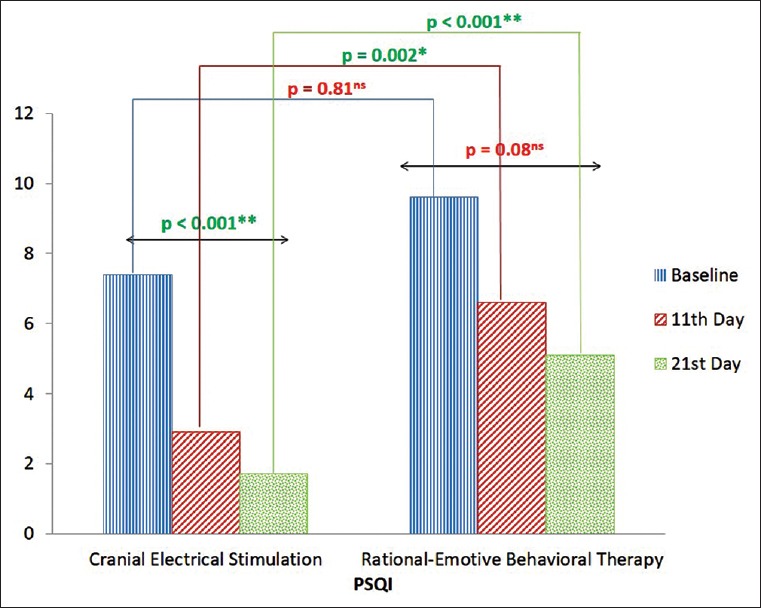
Pittsburgh Sleep Quality Index at baseline, 11th day, and 21st day postintervention between Group A and Group B
Figure 6.
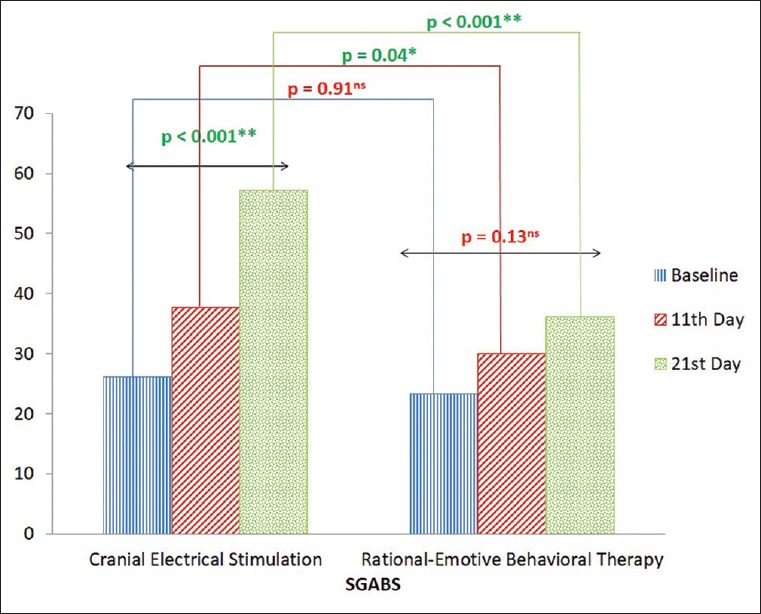
Shortened General Attitude and Belief Scale at baseline, 11th day, and 21st day postintervention between Group A and Group B
Figure 3.
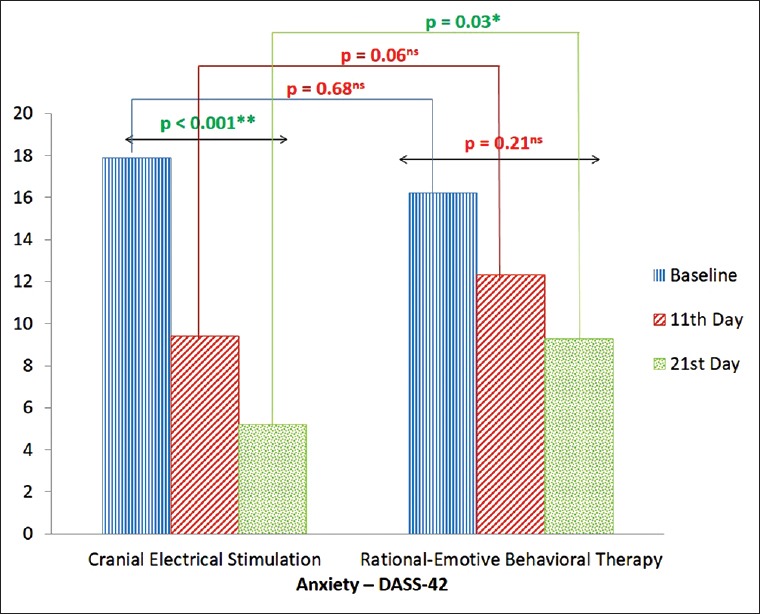
Depression, Anxiety, Stress scale-24 for anxiety at baseline, 11th day, and 21st day postintervention between Group A and Group B
DISCUSSION
Stroke causes long-term disability and the survivor may be facing further losses of his/her employment and premorbid living environment when stroke is complicated by cognitive loss.[12] As a result, the increased understanding of the brain's plasticity and the ability of rehabilitation to influence neurological recovery using different interventions are most exciting areas in stroke rehabilitation research.[13] The CES and REBT were used as intervention strategies in the present study to treat the psychological illness among stroke survivors.
The CES and REBT were administered for 21 days (4 days a week) among the patients with CS. The comparison between Group A (CES) and Group B (REBT) was done at the 95% level of significance at 0th day, 11th day, and 21st day for depression, anxiety, stress, suicidal ideation, attitude and belief, and quality of life of CS survivors. Both the interventions were showing improvement in psychological illness present among stroke survivors, but it was observed that the CES was more effective than REBT.
The total mean difference between Group A and Group B for depression, anxiety, and stress on DASS-42 at 0th day, 11th day, and 21st day was 4.33, 2.61, and −3.64 (P < 0.05) which signifies that the Group A has been showing more improvement than Group B. In sleep quality, attitude and belief, and suicidal thought, the total mean difference between Group A and Group B on PSQI, SGABS, and Modified Scale for Suicidal Ideation (MSSI) at 0th day, 11th day, and 21st day was 0.91, −0.291, and 2.519, which also indicates that the CES has been more effective than REBT.
CES is a noninvasive brain stimulation and a nondrug method used by psychiatrists for the treatment of depression and anxiety. Neurophysiologically, CES is believed to affect the subcortical brain structures known to regulate emotions such as the reticular activating system, thalamus, and hypothalamus as well as the limbic system. Furthermore, CES may stimulate regions that regulate pain messages, neurotransmitter function, and hormone production through the hypothalamic–pituitary axis. A 20-min single treatment session by CES causes cortical brain deactivation in the midline frontal and parietal regions of the brain with a similar pattern for high- and low-frequency stimulation and alters connectivity in the default mode network.[6,14] This is in line with our findings.
Only REBT was effective in improving the attitude and belief of patients toward their illness. The high effectiveness of CES than REBT was not understood but it may be because in CES group patients the electric current was delivered through ear electrodes which causes some placebo effect, while in REBT, only counseling session was given by the researcher. In REBT group, the researcher found that the patients get easily irritated by repeated questioning by the researcher, even their caregivers were also get agitated, while CES group patients experienced soothing and calming effect and they believe that something was given to them which can modulate their brain activity and they will be recovered soon.
CONCLUSION
There is sufficient evidence to prove that CES is better than REBT in improving psychological illness such as depression, anxiety, stress, attitudes, belief, and quality of life among CS survivors.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
The authors are very thankful to Mr. Asir John Samuel, BSc (Psychology), BPT, MPT (Neurosciences and Paediatric neurology), DYScEd (PhD), Associate Professor, Maharishi Markandeshwar Institute of Physiotherapy and Rehabilitation, Maharishi Markandeshwar University, Mullana, India, for providing technical support.
REFERENCES
- 1.Oladiji JO, Akinbo SR, Aina OF, Aiyejusunle CB. Risk factors of post-stroke depression among stroke survivors in Lagos, Nigeria. Afr J Psychiatry (Johannesbg) 2009;12:47–51. doi: 10.4314/ajpsy.v12i1.30278. [DOI] [PubMed] [Google Scholar]
- 2.Paolucci S. Epidemiology and treatment of post-stroke depression. Neuropsychiatr Dis Treat. 2008;4:145–54. doi: 10.2147/ndt.s2017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kneebone II, Neffgen LM, Pettyfer SL. Screening for depression and anxiety after stroke: Developing protocols for use in the community. Disabil Rehabil. 2012;34:1114–20. doi: 10.3109/09638288.2011.636137. [DOI] [PubMed] [Google Scholar]
- 4.Joy Singh A, Lenin R, Nilachandra Singh L. Post stroke psychiatric morbidity among hemiplegics in stroke. [Last accessed on 2017 Nov 23];IJPMR. 2006 17:8–10. Available from: https://www.pdfs.semanticscholar.org/4320/c39d506e1ee6cf56da10ed2c367152446907.pdf . [Google Scholar]
- 5.Barclay TH, Barclay RD. A clinical trial of cranial electrotherapy stimulation for anxiety and comorbid depression. J Affect Disord. 2014;164:171–7. doi: 10.1016/j.jad.2014.04.029. [DOI] [PubMed] [Google Scholar]
- 6.Kirsch DL, Nichols F. Cranial electrotherapy stimulation for treatment of anxiety, depression, and insomnia. Psychiatr Clin North Am. 2013;36:169–76. doi: 10.1016/j.psc.2013.01.006. [DOI] [PubMed] [Google Scholar]
- 7.Bystritsky A, Kerwin L, Feusner J. A pilot study of cranial electrotherapy stimulation for generalized anxiety disorder. J Clin Psychiatry. 2008;69:412–7. doi: 10.4088/jcp.v69n0311. [DOI] [PubMed] [Google Scholar]
- 8.Froggatt W. A brief introduction to rational emotive behaviour therapy. Behav Cogn Psychother. 2005;33:1–15. [Google Scholar]
- 9.Iftene F, Predescu E, Stefan S, David D. Rational-emotive and cognitive-behavior therapy (REBT/CBT) versus pharmacotherapy versus REBT/CBT plus pharmacotherapy in the treatment of major depressive disorder in youth; a randomized clinical trial. Psychiatry Res. 2015;225:687–94. doi: 10.1016/j.psychres.2014.11.021. [DOI] [PubMed] [Google Scholar]
- 10.Turner MJ. Rational emotive behavior therapy (REBT), irrational and rational beliefs, and the mental health of athletes. Front Psychol. 2016;7:1423. doi: 10.3389/fpsyg.2016.01423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lewis SC, Dennis MS, O'Rourke SJ, Sharpe M. Negative attitudes among short-term stroke survivors predict worse long-term survival. Stroke. 2001;32:1640–5. doi: 10.1161/01.str.32.7.1640. [DOI] [PubMed] [Google Scholar]
- 12.Ward N. Assessment of cortical reorganisation for hand function after stroke. J Physiol. 2011;589:5625–32. doi: 10.1113/jphysiol.2011.220939. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Teasell R. Stroke recovery and rehabilitation. Stroke. 2003;34:365–6. doi: 10.1161/01.str.0000054630.33395.e2. [DOI] [PubMed] [Google Scholar]
- 14.Feusner JD, Madsen S, Moody TD, Bohon C, Hembacher E, Bookheimer SY, et al. Effects of cranial electrotherapy stimulation on resting state brain activity. Brain Behav. 2012;2:211–20. doi: 10.1002/brb3.45. [DOI] [PMC free article] [PubMed] [Google Scholar]