

Abstract
Context:
Exercise-associated hyponatremia (EAH) is a potentially fatal condition that can be prevented by avoiding excessive fluid intake. Running has become more popular in recent years, so it is important to assess the safety of runners' hydration strategies.
Objective:
(1) To explore the intended hydration strategies of a sample of marathon runners before the 2014 London Marathon, (2) to examine their sources of information and knowledge about fluid intake and their understanding of EAH, and (3) to compare these findings with the results of a similar study carried out before the 2010 London Marathon.
Design:
Cross-sectional study.
Setting:
The 2014 London Marathon.
Patients or Other Participants:
A total of 298 runners (148 males, 150 females), 0.83% of all race finishers.
Main Outcome Measure(s):
Planned frequency, type, and volume of hydration; sources of information about appropriate drinking; and understanding of hyponatremia were explored. Comparisons were made with data collected from a sample of participants at the 2010 London Marathon. Data relating to the 2014 cohort are presented in descriptive form. Comparisons of the 2010 and 2014 cohorts were conducted using parametric and nonparametric methods.
Results:
A total of 48.7% of the 2014 cohort listed drinking to thirst as the most important factor affecting their hydration strategy during the race. This compared with 25.3% of runners from the 2010 cohort and represented an increase (χ2 = 29.1, P = .001); 5.8% of the 2014 cohort planned on drinking more than 3.5 L, compared with 12% of the 2010 cohort (χ2 = 4.310, P = .038).
Conclusions:
The number of sampled individuals using thirst to guide hydration strategies in the 2014 London Marathon increased from 2010. However, more than half of the 2014 cohort was not planning to drink to thirst. Runners still need to be educated about the risks of overdrinking as they continue to demonstrate a lack of knowledge and understanding.
Key Words: physical endurance, fluid intake, thirst
Key Points
Since the 2010 London Marathon, education led to improvements in runners' intended fluid strategies for the 2014 London Marathon.
Exercise-associated hyponatremia remains a medically significant problem for marathon runners.
More runners currently had safer intended hydration strategies, but a distinct lack of understanding persisted. Therefore, further education of runners about appropriate fluid intake is still required.
Over the last 2 decades, marathon running has become an increasingly popular sport.1,2 Exercise-associated hyponatremia (EAH) is a concerning and serious medical complication in endurance athletes.3 Worldwide, a number of marathon deaths due to EAH have been recorded, including a young runner in the 2007 London Marathon; 15 runners in the 2003 London Marathon were admitted to the hospital with EAH.4
Exercise-associated hyponatremia is defined as a serum sodium concentration of less than 135 mmol/L during or up to 24 hours after prolonged physical activity.4 The main cause is believed to be excessive fluid intake.5,6 A low serum sodium concentration can be associated with a range of signs and symptoms, such as nausea, headaches, and seizures. A sodium concentration of less than 135 mmol/L will often not result in any physical signs or symptoms but may still lead to the development of more serious, life-threatening complications, such as pulmonary or cerebral edema, unconsciousness, and death. Additional risk factors for EAH include inappropriate antidiuretic hormone release and metabolism and extreme environmental conditions.7
Studies carried out at the 2002 Boston Marathon8 and the 2006 London Marathon4 indicated that up to 13% of finishers had asymptomatic hyponatremia; however, the point at which asymptomatic athletes become symptomatic has not been established. Guidance has varied over time as more research has been undertaken. Previous suggestions were to base hydration strategies on the sweat rate9; the authors of a 2017 update10 advised drinking to thirst and using body weight to guide hydration. The use of thirst as a guide to hydration strategies was widely recommended by consensus statements and other publications.6,11–13 An earlier investigation by members of our group14 explored the hydration strategies of 217 runners attending registration for the 2010 London Marathon (0.6% of the total finishers15). The runners lacked knowledge about safe drinking and prevention of EAH on race day: 12% planned to drink in excess of 3500 mL during the marathon, a volume that could have put them at significantly higher risk of developing EAH.4,8,14 A total of 55 runners (25.3%) planned to drink according to their thirst. Only 35.5% had a basic understanding of EAH.
The London Marathon, held in the spring over a flat city course, is a full 26.2-mi (42.2-km) marathon. Water bottles (250 mL) were available at 23 water stations situated at 1-mi (1.6-km) intervals from miles 3 to 25. In addition, stations at 5, 10, 15, 19, and 23 miles distributed 380-mL sachets of sports energy drinks (Lucozade Sport, Uxbridge, United Kingdom).
Since 2010, efforts have been made to raise awareness of the risks of overdrinking and EAH. Specific information is now provided in the prerace material, which is supplied to every runner.16 We aimed to explore the intended hydration strategies of a sample of marathon runners before the 2014 London Marathon, to examine their sources of information and knowledge about fluid intake and their understanding of EAH, and to compare these findings with those of a similar study carried out before the 2010 London Marathon.
METHODS
Prior ethical approval for the study was obtained from the Queen Mary University of London Research Ethics Committee. Any athlete scheduled to run in the 2014 London Marathon was eligible to be invited to take part at the event registration. Consistent with the 2010 research protocol,14 every ninth runner attending was approached at staggered intervals throughout the 4 registration days and invited to participate. Runners were given an information sheet outlining the study. They were excluded if they had any problems understanding the questionnaire (ie, language barriers or learning difficulty).
Those who agreed to participate were given the study questionnaire, which was validated in 2010 (see the Appendix),10 and asked to complete it at the research station.
The questionnaire comprised the following sections:
Background demographics
Drinking strategies
Sources of information about fluid intake
Knowledge of EAH
Statistical Analysis
We used SPSS (version 21.0; IBM Corp, Armonk, NY) for analysis. Data from the questionnaire were presented descriptively. Chi squared, independent t, and Mann-Whitney U tests were used to assess the differences in proportions between data collected in 2010 and 2014.
Findings related to the sources of EAH knowledge were explored using descriptive statistical methods. A P value of <.05 was defined as statistically significant.
RESULTS
Sample Characteristics
A total of 315 runners were invited to be part of the study (0.9% of all finishers17); 17 of these runners did not take part in the study due to language barriers or lack of time. The final sample was 298 participants (0.83% of all finishers17). Sample demographics are described in Table 1. The mean finishing time of the cohort was 4.66 ± 0.49 hours versus 4.50 hours for all the runners in the 2014 London Marathon.17
Table 1.
Characteristics of the Study Samples
| Variable |
2010 Data14 |
2014 Data |
Statistical Test Valuea |
P Value |
| Sample size | 217 | 298 | ||
| No. declined to take part | 15 | 17 | ||
| Mean age, y | 38.6 | 37.5 | t = −1.189 | .235 |
| Mean ± SD |
||||
| Finishing time, h | 4.36 ± 0.55 | 4.66 ± 0.49 | t = 2.961 | .003 |
| No. (%) |
||||
| Females | 66 (30.4) | 150 (50.3) | U = 25 892.00 | .001 |
| Males | 151 (69.6) | 148 (49.7) | ||
| First marathon | 117 (54) | 162 (54.4) | U = 32 328.00 | .997 |
| Member of a running club | 56 (25.8) | 83 (27.9) | U = 32 994.50 | .606 |
Independent-samples t test or Mann-Whitney U test.
Consumption Volume
Runners were asked to estimate the total milliliters of fluid they planned to consume over the course of the race. Those planning to drink more than 3.5 L were deemed to be at increased risk of EAH. This volume guideline is based on the findings of previous studies, which suggested a higher risk of developing EAH,4,8 and was used in the 2010 study.14 The total volume the runners planned to drink during the race is shown in the Figure.
Figure.
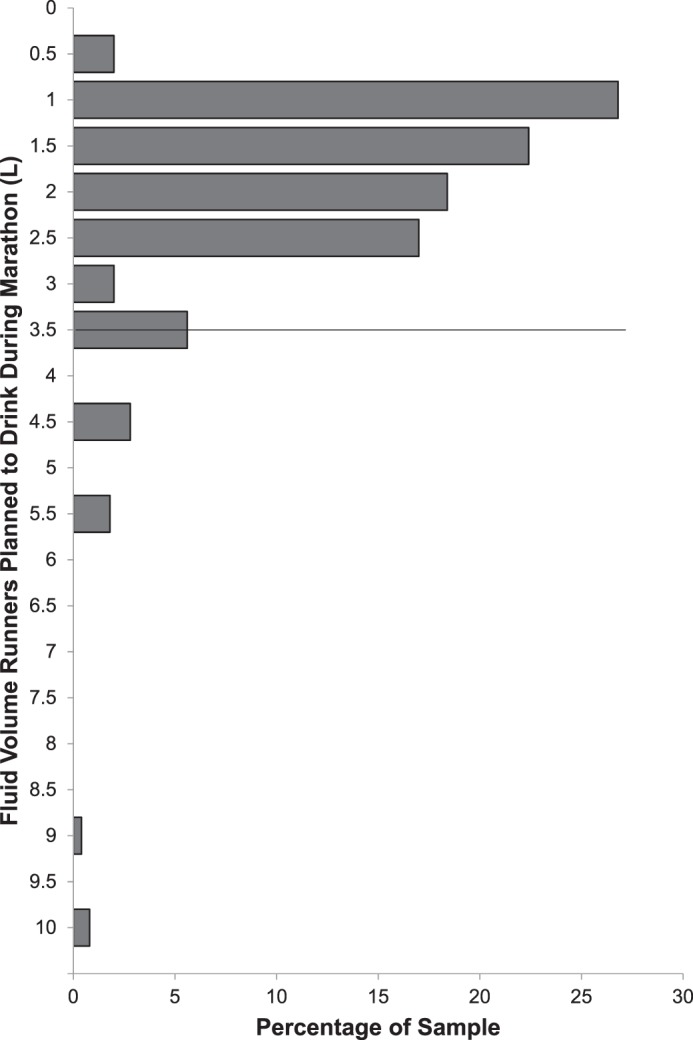
Volume of fluid (L) runners planned to drink during the marathon. The horizontal line represents the volume that previous research has shown may put runners at greater risk of hyponatremia.
Overall, 241 (81%) of the 2014 participants specified the volume they intended to consume. The median (interquartile range) volume these runners planned to consume was 1.0 (0.4–1.6) L. Of these 241 runners, 14 (5.8%) planned to drink more than the 3.5-L threshold compared with 26 runners (12%) in the 2010 cohort (χ2 = 4.310, P = .038; Table 2).
Table 2.
Comparison of 2010 and 2014 Data for Race Strategies
| Variable |
2010 Data14 |
2014 Data |
Statistical Test Valuea |
P Value |
| Hydration strategy during race? No. (%) | 208 (95.8) | 277 (93) | U = 31 108.00 | .1050 |
| Median (interquartile range) planned volume consumption during race, L | 1.2 (0.6–2.2) | 1.0 (0.4–0.6) | t = 2.421 | .0161 |
| No. of runners intending to drink >3.5 L (%) | 26 (12) | 14 (5) | Z = 3.216 | .0006 |
Independent-samples t test, Mann-Whitney U test, or Z ratio.
Frequency of Drinking
Runners in the 2014 marathon planned to drink at a median of 8 (4–11) water stations compared with a median of 10 (5–24) stations for the runners in the 2010 marathon (t = 3.353, P = .001), indicating a reduction in consumption frequency. Furthermore, a median of 3 (2–5) stations dispensing sports drinks were intended stops for the 2014 runners compared with a median of 4 (2–5) for the 2010 runners (t = 3.869, P = .0001; Table 3).
Table 3.
Comparison of 2010 and 2014 Data for Frequency of Hydration Attemptsa
| Variable |
Median No. (Interquartile Range) |
Independent- Samples t Test Value |
P Value |
|
| 2010 Data14 |
2014 Data |
|||
| Planned water- station visits | 10 (5–24) | 8 (4–11) | 3.353 | .0010 |
| Planned sports- sachet–station visits | 4 (2–5) | 3 (2–5) | 3.869 | .0001 |
Water bottle = 250 mL, sports sachets = 380 mL.
Drinking to Thirst
Thirst was reported as the main factor influencing the intended hydration strategy by 145 (48.7%) runners in 2014, which was more than the 55 (25.3%) of runners in 2010 (χ2 = 29.113, P = .001; Table 4).
Table 4.
Comparison of 2010 and 2014 Data for Those Planning to Drink to Thirst
| Variable |
No. (%) |
Independent- Samples t Test Value |
P Value |
|
| 2010 Data14 |
2014 Data |
|||
| Drinking to thirst | 55 (25.3) | 145 (48.7) | 29.1131 | .0010 |
The proportions of female and male runners who planned on drinking to thirst differed (55% and 43%, respectively; χ2 = 4.365, P = .037). We found no difference between the proportions of experienced and nonexperienced runners (χ2= 0.256, P = .613) planning on drinking to thirst.
Education
Absolute Knowledge
In 2014, 190 (63.8%) runners claimed to have heard of hyponatremia. However, in response to the question exploring their knowledge of EAH, only 70 (40%) demonstrated a basic understanding, as qualified by the criteria in Table 5.
Table 5.
Comparison of 2010 and 2014 Data for Runners' Knowledge of Exercise-Associated Hyponatremia (EAH)a
| Variable |
No. (%) |
Mann- Whitney U Test Value |
P Value |
|
| 2010 Data14 |
2014 Data |
|||
| Heard of EAH | 141 (65) | 190 (63.8) | 31 582.50 | .756 |
| Basic understanding of EAH | 77 (37) | 70 (40) | 18 620 | .865 |
| Runners felt they knew enough | 182 (83.9) | 258 (86.6) | 33 155.50 | .249 |
Those who mentioned overdrinking, or dilution effects, etc, were deemed to have a basic understanding of EAH. Understanding of EAH was deemed “basic” if their answer in free text identified a cause such as drinking too much fluid or signs and symptoms included words associated with malaise, collapse, or death, as per the 2010 study.14
Runners' Self-Perceptions of Their Knowledge
In total, 258 (86.6%) of the 2014 runners perceived that they knew enough about safe drinking on marathon day.
Sources of Knowledge
A total of 282 (94.6%) runners claimed to have either read or been told about appropriate hydration strategies on marathon day. Most had gained their information from reading the official prerace information magazine (66.4%), talking to running friends (40.4%), or reading other running magazines (30.9%). Most runners had identified more than 1 source of information. All sources of information are shown in Table 6.
Table 6.
2014 Sources of Information for Runners About Fluid Intake on Marathon Day Compared With 2010 Data
| Variable |
No. (%) |
Mann-Whitney U Test Value |
P Value |
|
| 2010 Data14 |
2014 Data |
|||
| Read or told about drinking | 202 (93.1) | 282 (94.6) | 32 542.00 | .596 |
| Virgin Money London Marathon Magazine | 152 (70) | 198 (66.4) | 30 821.00 | .311 |
| Running friends | 97 (44.7) | 121 (40.4) | 30 589.50 | .308 |
| Running magazinea | 75 (34.6) | 92 (30.9) | 30 750.00 | .339 |
| Virgin Money London Marathon Web site | 57 (26.3) | 71 (23.8) | 31 174.00 | .488 |
| Running club | 36 (16.6; 64% of club runners) | 49 (16.4; 59% of club runners) | 31 765.00 | .801 |
| Information from charity | 51 (23.5; 29.1% of charity runners) | 62 (20.8; 26.4% of charity runners) | 30 741.00 | .400 |
| Running coach | 30 (13.8) | 54 (18.1) | 34 413.00 | .020 |
| Running book | 23 (10.6) | 46 (15.4) | 32 510.00 | .641 |
| Other sources of informationb | 34 (15.7) | 26 (8.7) | 29 764.00 | .014 |
Mostly Runner's World magazine.
Mainly Internet, social media, or health professional.
DISCUSSION
Exercise-associated hyponatremia is a multifactorial condition in which consumption of a large amount of fluid is a recognized risk factor.4,8,14 Consuming a volume of 3.5 L has been associated with a higher risk of developing EAH.4,8,14 Recent deaths attributed to EAH4,18,19 have highlighted the importance of avoiding overdrinking.
Data collected in 2014 showed that 14 (5%) of the runners planned to drink more than 3.5 L during the race. Compared with the previous data from 2010, when 26 runners (12%) planned to drink in this range, this decrease demonstrated a change in runners' behavior 4 years later. This is further highlighted by the reduction in the number of water stations from which the runners intended to drink during the race. Both intentions correlated with 2 associated risk factors for developing EAH.
The current guidance is for a runner to guide fluid intake based on thirst. It was important to examine what proportion of the runners planned to use their own thirst as guidance. In this study, 48.7% of runners listed drinking to thirst as the most important factor affecting their hydration strategy throughout the race. Although this was an increase from 4 years previously, more than half of the runners in our sample were still not aware of current guidance regarding thirst as the main indicator for hydration. This change suggests that messages regarding hydration are beginning to reach a larger proportion of the running population.
Race inexperience is a known risk factor for EAH.20,21 However, we noted no statistical difference observed between the numbers of experienced and nonexperienced runners planning on drinking to thirst. More race experience does not always equate to a better understanding of the science underlying conditions such as EAH. This affirms the importance of directing messages and education about this topic at runners of all experience levels.
We found that 94.6% of runners had read or been told about hydration on marathon day, and 86.6% perceived they knew enough about drinking, which might imply that a similar proportion would plan to drink an appropriate and safe amount. Yet only 48% planned on drinking to thirst and only 40% of runners had a basic understanding of EAH, indicating that the message to runners about appropriate hydration and EAH still requires further dissemination.
A total of 66.4% of runners in our sample listed the official prerace information magazine as a source of information regarding fluid intake. The 2014 official magazine contained more prominently placed, detailed, and specific advice about appropriate and safe drinking, including the potential hazards of drinking too much and EAH. The magazine gave clear instructions to avoid drinking too much: “Drinking too much can be very dangerous and lead to hyponatraemia (water intoxication), fits [seizures], and even death.”16 Sent to each runner as part of the final preparation before the race, the magazine is the single most important London Marathon educational resource. No other specifically directed information is given to all runners. Interestingly, the data gathered on sources of information showed that most runners consulted more than 1 source, including a wide range from magazines to the Internet and discussions with peers. This fact highlights how broadly information can be distributed throughout a community: runners in this case. The message about safe fluid intake and EAH still needs to be reinforced, and perhaps more targeted attempts to dispense the information through the running community would affect runners' future behavior.
The main limitations of this study were using a questionnaire and predictive measures and comparing them with biological factors and outcomes. Exercise-associated hyponatremia is a multifactorial biological process affecting the dilution effects of fluids within the body. A 3.5-L volume was used as a guideline; however, it is not possible to say that this volume of water should be used as a definitive cutoff, as many other factors can contribute to the development of EAH. The runners in the 2014 study had a difference of approximately 20 minutes in their average finishing time, which may have influenced the results. Although a low percentage of total finishers completed the questionnaire, the numbers were comparable across the 2010 and 2014 studies; we invited every ninth runner to ensure an equal distribution of runners across the signup days at the marathon. Results of the questionnaires depended on the honesty of the respondents, and accuracy cannot be determined; such recall bias is a general limitation when using questionnaires. The questionnaire was the same for both studies, and it was previously validated for the 2010 study, allowing valid comparisons to be made. The risks and consequences of EAH are known, but many runners remain unaware of how much they should drink. More education of runners is needed.
As discussed earlier, information is slowly disseminating through the running community, but further improvement is still needed. The most frequently consulted source of information was the prerace magazine, and this publication should continue to be used to inform runners. Perhaps a more targeted approach starting at the grassroots level would help to increase the understanding of this subject area among the running community; recommendations have already been made to broadly target these athletes and to focus on certain roles within a running community.10
CONCLUSIONS
Exercise-associated hyponatremia remains a medically significant problem for marathon runners. Education has led to certain improvements in runners' intended fluid strategies at the London Marathon, with a statistically significant reduction in the proportion of our cohort planning to drink greater than 3.5 L and a higher proportion of these runners now planning on drinking to thirst, as recommended by the current medical guidelines for endurance athletes. Among our cohort, 94.6% felt they had enough information and 86.6% perceived they knew enough about safe hydration strategies. However, only 48% of these runners intended to drink to thirst, indicating a persistent and distinct lack of understanding of the topic. More effective education of runners about appropriate fluid intake and EAH is required to further reduce the risk and ultimately the incidence of EAH.
ACKNOWLEDGMENTS
We thank the participants in this study, the marathon officials who assisted with logistics, and the students from Queen Mary University of London.
Appendix.
Questionnairea Continued on Next Page
|
Many thanks for taking part in this questionnaire. If you are not clear about any of the questions, please feel free to ask the researcher. Please answer the questions in order by putting a tick in the box or writing an answer on the line. | |
| Background information about you as a runner: | |
| 1) | Is this your first marathon? |
| Yes _____ (and if Yes, please go to question 3) | |
| No _____ | |
| If this is not your first marathon, how many previous marathons have you run? (please tick) | |
| 1 _____ | |
| 2–4 _____ | |
| 5–9 _____ | |
| 10 or more marathons _____ | |
| 2) | What is your fastest time? _____h _____min |
| 3) | What is your estimated finishing time? _____h _____min |
| 4) | Are you running on behalf of a charity? |
| Yes _____ | |
| No _____ | |
| If Yes, which charity? ___________________________________________ | |
| 5) | Are you a member of a Running club? |
| Yes _____ | |
| No _____ | |
| 6) | Gender: |
| Male _____ | |
| Female _____ | |
| 7) | Age: _____y |
| 8) | How tall are you? _____ |
| 9) | What is your weight? _____ |
| Information on drinking on marathon day: | |
| 10) | Have you read about or been told about drinking fluids on marathon day? |
| Yes _____ | |
| No _____ (if No, please go to question 11) | |
| If Yes, where have you received this information from? (please tick all that apply) | |
| London Marathon magazine _____ | |
| London Marathon Web site _____ | |
| Running club _____ | |
| Running coach _____ | |
| Running friends _____ | |
| Running magazine _____ (if so, which magazine?) ___________________ | |
| Running book _____ (if so, which book?) _______________________ | |
| From the charity for which you are running _____ | |
| Other sources of information (please specify; eg, other online source, smartphone app, library book etc) __________________________________ | |
| Before the marathon: | |
| 11) | Do you have any plans about drinking in the morning before the start of the marathon? |
| Yes _____ | |
| No _____ (if No, please go to question 15) | |
| 12) | If Yes, what are you planning to drink? _____________________________ |
| 13) | How much are you planning to drink? _______________________________ |
| 14) | When are you planning to drink this? _______________________________ |
| During the marathon: | |
| 15) | Do you have any plans about drinking during the race? |
| Yes _____ | |
| No _____ (if No, please go to question 19) | |
| 16) | If Yes, what are you planning to drink? _____________________________ |
| 17) | How much are you planning to drink? ____________________________ |
| 18) | At what stages of the race are you planning to drink? |
| ______________________________________________________________________ | |
| ______________________________________________________________________ | |
| 19) | Some people carry their own drinks from the start of the race – do you intend to do that? |
| Yes _____ | |
| No _____ (if No, please go to question 25) | |
| 20) | If Yes, what drink will you carry? _______________________________ |
| 21) | What volume will you carry? __________________________________ |
| 22) | Do you plan to drink water provided in bottles at water stations during the race? |
| Yes _____ | |
| No _____ (if No, please go to question 25) | |
| 23) | If yes, at how many water stations will you take bottles of water? _____ |
| 24) | How much of each bottle do you anticipate that you will drink? |
| A few sips _____ | |
| Several mouthfuls _____ | |
| Half the bottle _____ | |
| Most or all of the bottle _____ | |
| 25) | Do you plan to drink the sports drink (Lucozade) provided at the drink stations during the race? |
| Yes _____ | |
| No _____ (if No, please go to question 28) | |
| 26) | If Yes, at how many drink stations will you take a sports drink? _____ |
| 27) | How much of each pack do you anticipate that you will drink? |
| A few sips _____ | |
| Several mouthfuls _____ | |
| Half the pack _____ | |
| Most or all of the pack _____ | |
| 28) | What is the volume of each water bottle given out on the course? |
| (please estimate if you don't know exactly) _____mls | |
| 29) | What is the volume of each pack of sports drinks given out on the course? |
| (please estimate if you don't know exactly) _____mls | |
| 30) | What factors may affect how much you drink in order of importance? |
| (please mark '1′ for the most important for you, '2′ for the second, '3′ for the third most important and '4′ for the least important) | |
| My plan _____ | |
| How thirsty I feel _____ | |
| The temperature on race day _____ | |
| Other (please specify) _____________________________ | |
| 31) | Have you practised drinking water during your training? |
| Yes _____ | |
| No _____ | |
| 32) | Have you practised drinking a sports drink during your training? |
| Yes _____ | |
| No _____ | |
| After the marathon: | |
| 33) | Do you have any plans about drinking in the 6 hours after the marathon? |
| Yes _____ | |
| No _____ (if No, please go to question 37) | |
| 34) | If Yes, what are you planning to drink? _____________________________ |
| 35) | How much are you planning to drink? _____________________________ |
| 36) | How often are you planning to drink? _____________________________ |
| Information about fluids: | |
| 37) | Do you feel that you know enough about what and how much to drink on marathon day? |
| Yes _____ | |
| No _____ | |
| If No, what would help you to be better informed for future races? | |
| ______________________________________________________________________ | |
| ______________________________________________________________________ | |
| 38) | Have you heard of the term 'hyponatraemia' (low salt or sodium levels) |
| Yes _____ | |
| No _____ | |
| If Yes, what is your understanding of its causes and effects? | |
| ______________________________________________________________________ | |
| ______________________________________________________________________ | |
| 39) | Do you have any other comments about drinking fluids on marathon day? |
| ______________________________________________________________________ | |
| ______________________________________________________________________ | |
| Many thanks for completing this questionnaire. Please return it to the researcher. | |
The questionnaire is reproduced in its original form except that underlined spaces replaced boxes for answers.
REFERENCES
- 1.Fredericson M, Misra AK. Epidemiology and aetiology of marathon running injuries. Sports Med. 2007;37(4–5):437–439. doi: 10.2165/00007256-200737040-00043. [DOI] [PubMed] [Google Scholar]
- 2.Rasmussen CH, Nielsen RO, Juul MS, Rasmussen S. Weekly running volume and risk of running-related injuries among marathon runners. Int J Sports Phys Ther. 2013;8(2):111–120. [PMC free article] [PubMed] [Google Scholar]
- 3.Speedy DB, Noakes TD, Schneider C. Exercise-associated hyponatremia: a review. Emerg Med (Fremantle) 2001;13(1):17–27. doi: 10.1046/j.1442-2026.2001.00173.x. [DOI] [PubMed] [Google Scholar]
- 4.Kipps C, Sharma S, Tunstall Pedoe D. The incidence of exercise-associated hyponatraemia in the London Marathon. Br J Sports Med. 2011;45(1):14–19. doi: 10.1136/bjsm.2009.059535. [DOI] [PubMed] [Google Scholar]
- 5.Draper SB, Mori KJ, Lloyd-Owen S, Noakes T. Overdrinking-induced hyponatraemia in the 2007 London Marathon. BMJ Case Rep. 2009;2009 doi: 10.1136/bcr.09.2008.1002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Noakes TD. Is drinking to thirst optimum? Ann Nutr Metab. 2010;57(suppl 2):9–17. doi: 10.1159/000322697. [DOI] [PubMed] [Google Scholar]
- 7.Noakes TD, Sharwood K, Speedy D, et al. Three independent biological mechanisms cause exercise-associated hyponatremia: evidence from 2, 135 weighed competitive athletic performances. Proc Natl Acad Sci U S A. 2005;102(51):18550–18555. doi: 10.1073/pnas.0509096102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Almond CS, Shin AY, Fortescue EB, et al. Hyponatremia among runners in the Boston Marathon. N Engl J Med. 2005;352(15):1550–1556. doi: 10.1056/NEJMoa043901. [DOI] [PubMed] [Google Scholar]
- 9.Convertino VA, Armstrong LE, Coyle EF, et al. American College of Sports Medicine position stand. Exercise and fluid replacement. Med Sci Sports Exerc. 1996;28(1):i–vii. doi: 10.1097/00005768-199610000-00045. [DOI] [PubMed] [Google Scholar]
- 10.Hew-Butler T, Loi V, Pani A, Rosner MH. Exercise-associated hyponatremia: 2017 update. Front Med (Lausanne) 2017;4:21. doi: 10.3389/fmed.2017.00021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hew-Butler T, Ayus JC, Kipps C, et al. Statement of the Second International Exercise-Associated Hyponatremia Consensus Development Conference, New Zealand, 2007. Clin J Sport Med. 2008;18(2):111–121. doi: 10.1097/JSM.0b013e318168ff31. [DOI] [PubMed] [Google Scholar]
- 12.Hew-Butler T, Almond C, Ayus JC, et al. Consensus statement of the 1st International Exercise-Associated Hyponatremia Consensus Development Conference, Cape Town, South Africa, 2005. Clin J Sport Med. 2005;15(4):208–213. doi: 10.1097/01.jsm.0000174702.23983.41. [DOI] [PubMed] [Google Scholar]
- 13.Hew-Butler T, Verbalis JG, Noakes TD. International Marathon Medical Directors Association. Updated fluid recommendation: position statement from the International Marathon Medical Directors Association (IMMDA) Clin J Sport Med. 2006;16(4):283–292. doi: 10.1097/00042752-200607000-00001. [DOI] [PubMed] [Google Scholar]
- 14.Williams J, Tzortziou Brown V, Malliaras P, Perry M, Kipps C. Hydration strategies of runners in the London Marathon. Clin J Sport Med. 2012;22(2):152–156. doi: 10.1097/JSM.0b013e3182364c45. [DOI] [PubMed] [Google Scholar]
- 15.London Marathon Race Results 2010. MarathonGuide.com Web site. http://www.marathonguide.com/results/browse.cfm?MIDD=16100425 Accessed April 11, 2018.
- 16.Sharma S. London Marathon medical advice. Virgin Money London Marathon Web site. www.virginmoneylondonmarathon.com/en-gb/training/staying-healthy/medical-advice Published April 2014. Accessed February 22, 2018.
- 17.London Marathon race results 2014. MarathonGuide.com Web site. http://www.marathonguide.com/results/browse.cfm?MIDD=16140413 Accessed February 22, 2018.
- 18.Gardner JW. Death by water intoxication. Mil Med. 2002;167(5):432–434. [PubMed] [Google Scholar]
- 19.Severac M, Orban JC, Leplatois T, Ichai C. A near-fatal case of exercise-associated hyponatremia. Am J Emerg Med. 2014;32(7):813. doi: 10.1016/j.ajem.2013.12.041. [DOI] [PubMed] [Google Scholar]
- 20.Chorley J, Cianca J, Divine J. Risk factors for exercise-associated hyponatremia in non-elite marathon runners. Clin J Sport Med. 2007;17(6):471–477. doi: 10.1097/JSM.0b013e3181588790. [DOI] [PubMed] [Google Scholar]
- 21.Hew TD, Chorley JN, Cianca JC, Divine JG. The incidence, risk factors, and clinical manifestations of hyponatremia in marathon runners. Clin J Sport Med. 2003;13(1):41–47. doi: 10.1097/00042752-200301000-00008. [DOI] [PubMed] [Google Scholar]