

Abstract
Small Incision Lenticule Extraction (SMILE) is a relatively new one-step refractive procedure that has recently been approved by the FDA for the treatment of myopia. It is anticipated myopic astigmatism will be FDA-approved in 2019. The SMILE procedure is shown to have similar efficacy, safety, predictability, and stability as current surgical options, such as LASIK, but has been gaining popularity due to fewer potential complications, such as dry eye incidence and greater biomechanical stability, and faster recovery time. This article discusses the SMILE procedure, its benefits, risks, uncertainties, and potential future in the world of refractive surgery.
Introduction
More than 35 million eyes have undergone excimer laser vision correction (PRK & LASIK) worldwide, with over 14 million being performed in the US since its inception. LASIK has been the bulk of these procedures. So, is there room for improvement? The answer is a resounding “yes” if we consider the never-ending drive of man’s ingenuity to improve the human condition. Engineers at Zeiss in Jena, Germany about nine years ago felt that they might be able to make corneal refractive surgery even better. (Figures 1–3).
Figure 1.

Carl Zeiss Meditec VisuMax Femtosecond Laser
Figure 2.

Disposable Curved Patient Interface
Figure 3.
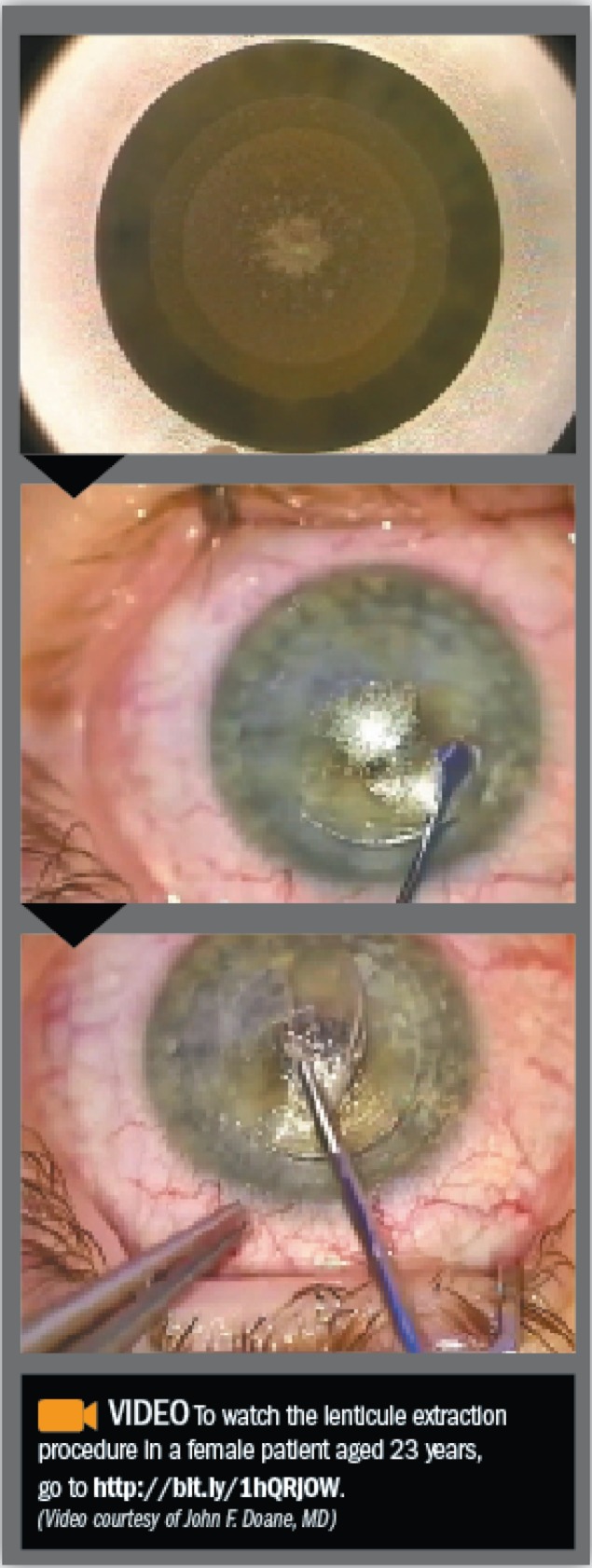
Pictures from a SMILE procedure performed. (JFD). The top frame shows the femtosecond laser creating a lenticule of tissue and an access incision. The middle image demonstrates dissection between tissue planes anterior and posteriorly of the lenticule. The bottom image shows the lenticule being placed on the front of the corneal epithelium for inspection.
What is SMILE?
SMILE is an intrastromal keratomileusis technique that requires a single laser, femtosecond, to create a 3 dimensional lenticule that is extracted through a small corneal incision ranging from 2–5 mm. (Figure 4) There is no corneal flap and there is preservation of the anterior-most stromal lamella and Bowman’s layer, excluding the region of the incision. As an analogy SMILE could be compared to other forms of corneal refractive surgery as modern small incision operative techniques (abdominal, orthopedic, etc.) would be to older larger incision operative techniques. SMILE provides several benefits for patients as it does not require moving from one laser platform to another, has no risk for traumatic flap displacement, offers better biomechanical corneal stability, and reduces postoperative dry eye symptoms as fewer corneal nerves are interrupted.1–4
Figure 4.

Image demonstrating the difference in corneal incision in LASIK vs. SMILE.
Source: http://www.premiumeyes.de/de/augenlasern/relex-versus-lasik/
Although SMILE may be a new refractive surgical option in the US it has had extensive study. Over 300 peer-reviewed articles have been published on SMILE to date.5–13 Discover Vision Centers was one of five clinical investigation sites involved in the Spherical and the Compound Myopic Astigmatism US FDA clinical trial study arms. Both studies are complete at this point. Commercial spherical myopia SMILE procedures began in the US in early March 2017. The FDA is reviewing the astigmatic results at present and expect myopic astigmatic SMILE to be approved in the first half of 2019. We expect the 1,000,000 SMILE procedure to be performed world-wide before the end of 2017. More than 1,000 SMILE procedures are being performed world-wide. The last time a refractive procedure had such a rapid uptake was in the middle 1990s when excimer laser vision correction overtook incisional keratotomy. As before, patients and surgeons alike migrate to what they perceive to be the best procedure in a given situation. I do not think excimer laser vision correction will disappear completely. It is still the majority of the cases we do (65% Excimer and 35% SMILE). But as more indications are approved for SMILE we anticipate it will likely be 90% of the corneal refractive procedures we perform. The lack of a flap is attractive to those in the military and those involved in contact physical activities. Also, the lower likelihood of dry eye issues and greater residual tensile strength seems to resonate with patients.
There are still considerations that remain unknown. At this point, we have limited data that extends beyond five years. But, like LASIK the SMILE patients we treated five years ago in the FDA study are tracking just like LASIK patients so we do not expect any surprises. At present, we expect SMILE candidacy to mirror LASIK candidacy.
SMILE, The Future of Refractive Surgery?
As with most things, time will tell if SMILE can compete on the open playing field in a post-approval commercial refractive practice. More than 1,000 surgeons, at 600-plus laser centers in over 60 countries regularly perform the procedure and the number of trained US surgeons is continuing to expand since the FDA approval of SMILE.
From a clinician’s standpoint, it is quite clear that if designed properly, a femtosecond laser is a breakthrough device for corneal microsurgery. As more data becomes available, we will know what level of impact a femtosecond laser can achieve as a stand-alone refractive surgical device.
Biography
Clockwise, John F. Doane, MD, FACS, is a board-certified ophthalmologist and LASIK surgeon in Kansas City with Discover Vision Centers. Jae E. Cauble, BS, and J. Quinten Tuckfield, BS, are medical students at Kansas City University of Medicine and Biosciences. Jace J. Rickstrew, BS, is a medical student at Kansas University School of Medicine.
Contact: jdoane@discovervision.com

Footnotes
Disclosure
None Reported.
References
- 1.Seven I, Vahdati A, Pedersen IB, Vestergaard A, Hjortdal J, Roberts CJ, Dupps WJ. Contralateral Eye Comparison of SMILE and Flap-Based Corneal Refractive Surgery: Computational Analysis of Biomechanical Impact. Journal of Refractive Surgery. 2017;33:444–453. doi: 10.3928/1081597X-20170504-01. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Xia L, Zhang J, Wu J, Yu K. Comparison of Corneal Biological Healing After Femtosecond LASIK and Small Incision Lenticule Extraction Procedure. Current Eye Research. 2016;41:1202–1208. doi: 10.3109/02713683.2015.1107590. [DOI] [PubMed] [Google Scholar]
- 3.Cai WT, Liu QY, Ren CD, Wei QQ, Liu JL, Wang QY, Du YR, He MM, Yu J. Dry eye and corneal sensitivity after small incision lenticule extraction and femtosecond laser-assisted in situ keratomileusis: a Meta-analysis. International Journal of Ophthalmology. 2017;10:632–638. doi: 10.18240/ijo.2017.04.21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mohamed-Noriega K, Riau AK, Lwin NC, Chaurasia SS, Tan DT, Mehta JS. Early Corneal Nerve Damage and Recovery Following Small Incision Lenticule Extraction (SMILE) and Laser In Situ Keratomileusis (LASIK). Investigative Ophthalmology & Visual Science. 2014;55:1823–1834. doi: 10.1167/iovs.13-13324. [DOI] [PubMed] [Google Scholar]
- 5.Kamiya K, Shimizu K, Igarashi A, Kobashi H. Visual and Refractive Outcomes of Femtosecond Lenticule Extraction and Small-Incision Lenticule Extraction for Myopia. American Journal of Ophthalmology. 2014;157:128–134. doi: 10.1016/j.ajo.2013.08.011. [DOI] [PubMed] [Google Scholar]
- 6.Xu Y, Yang Y. Small-Incision Lenticule Extraction for Myopia. Optometry and Vision Science. 2015;92:123–131. doi: 10.1097/OPX.0000000000000451. [DOI] [PubMed] [Google Scholar]
- 7.Torky MA, Alzafiri YA. Visual and refractive outcomes of small-incision lenticule extraction in mild, moderate, and high myopia: Six-month results. Journal of Cataract & Refractive Surgery. 2017;43:459–465. doi: 10.1016/j.jcrs.2017.01.015. [DOI] [PubMed] [Google Scholar]
- 8.Ivarsen A, Asp S, Hjortdal J. Safety and Complications of More Than 1500 Small-Incision Lenticule Extraction Procedures. Ophthalmology. 2014;121:822–828. doi: 10.1016/j.ophtha.2013.11.006. [DOI] [PubMed] [Google Scholar]
- 9.Liu YC, Rosman M, Mehta JS. Enhancement after Small-Incision Lenticule Extraction. Ophthalmology. 2017;124:813–821. doi: 10.1016/j.ophtha.2017.01.053. [DOI] [PubMed] [Google Scholar]
- 10.Kling S, Spiru B, Hafezi F, Sekundo W. Biomechanical Weakening of Different Re-treatment Options After Small Incision Lenticule Extraction (SMILE) Journal of Refractive Surgery. 2017;33:193–198. doi: 10.3928/1081597X-20161221-01. [DOI] [PubMed] [Google Scholar]
- 11.Blum M, Kunert KS, Voßmerbäumer U, Sekundo W. Femtosecond lenticule extraction (ReLEx®) for correction of hyperopia — first results. Graefes Archive for Clinical and Experimental Ophthalmology. 2013;251:349–355. doi: 10.1007/s00417-012-2064-y. [DOI] [PubMed] [Google Scholar]
- 12.Sekundo W, Reinstein DZ, Blum M. Improved lenticule shape for hyperopic femtosecond lenticule extraction (ReLEx® FLEx): a pilot study. Lasers in Medical Science. 2016;31:659–664. doi: 10.1007/s10103-016-1902-2. [DOI] [PubMed] [Google Scholar]
- 13.Reinstein DZ, Pradhan KR, Carp GI, Archer TJ, Gobbe M, Sekundo W, Khan R, Dhungana P. Small Incision Lenticule Extraction (SMILE) for Hyperopia: Optical Zone Diameter and Spherical Aberration Induction. Journal of Refractive Surgery. 2017;33:370–376. doi: 10.3928/1081597X-20170331-01. [DOI] [PubMed] [Google Scholar]