

Abstract
Objective: To update the 2004 American Academy of Neurology (AAN) guideline for treating new-onset focal or generalized epilepsy (GE) with second- and third-generation antiepileptic drugs (AEDs). Methods: The 2004 AAN criteria was used to systematically review literature (January 2003 to November 2015), classify pertinent studies according to the therapeutic rating scheme, and link recommendations to evidence strength. Results: Several second-generation AEDs are effective for new-onset focal epilepsy. Data are lacking on efficacy in new-onset generalized tonic–clonic seizures, juvenile myoclonic epilepsy, or juvenile absence epilepsy, and on efficacy of third-generation AEDs in new-onset epilepsy. Recommendations: Lamotrigine (LTG) should (Level B) and levetiracetam (LEV) and zonisamide (ZNS) may (Level C) be considered in decreasing seizure frequency in adults with new-onset focal epilepsy. LTG should (Level B) and gabapentin (GBP) may (Level C) be considered in decreasing seizure frequency in patients ≥60 years with new-onset focal epilepsy. Unless there are compelling adverse-effect–related concerns, ethosuximide (ETS) or valproic acid (VPA) should be considered before LTG to decrease seizure frequency in treating absence seizures in childhood absence epilepsy (Level B). No high-quality studies suggest clobazam, eslicarbazepine, ezogabine, felbamate, GBP, lacosamide, LEV, LTG, oxcarbazepine, perampanel, pregabalin, rufinamide, tiagabine, topiramate, vigabatrin, or ZNS is effective in treating new-onset epilepsy because no high-quality studies exist in adults of various ages. A recent FDA strategy allows extrapolation of efficacy across populations; therefore, for focal epilepsy, eslicarbazepine and lacosamide (oral only for pediatric use) as add-on or monotherapy in persons ≥4 years old and perampanel as monotherapy received FDA approval.
Glossary
- AAN
American Academy of Neurology
- AE
adverse events
- AED
antiepileptic drug
- CBZ
carbamazepine
- CBZ-CR
controlled-release carbamazepine
- CBZ-IR
immediate-release carbamazepine
- CLB
clobazam
- ESL
eslicarbazepine
- ETS
ethosuximide
- EZG
ezogabine
- FBM
felbamate
- GBP
gabapentin
- GE
generalized epilepsy
- GTC
generalized tonic–clonic
- JME
juvenile myoclonic epilepsy
- LCM
lacosamide
- LEV
levetiracetam
- LTG
lamotrigine
- OXC
oxcarbazepine
- PER
perampanel
- PGB
pregabalin
- PHT
phenytoin
- RCT
randomized controlled trial
- RFN
rufinamide
- TGB
tiagabine
- TPM
topiramate
- VGB
vigabatrin
- VPA
valproic acid
- VPA-ER
extended-release valproic acid
- ZNS
zonisamide
INTRODUCTION
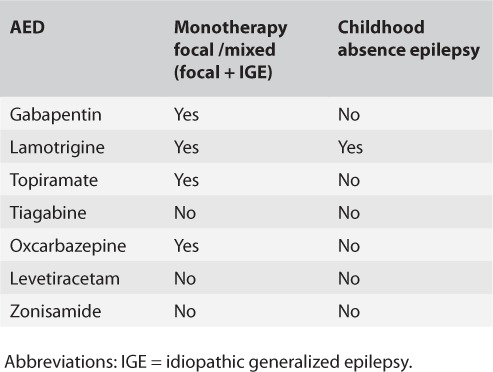
In 2004, the American Academy of Neurology (AAN) and the American Epilepsy Society (AES) published the first evidence-based guidelines on use of 7 second-generation antiepileptic drugs (AEDs) (table 1 shows principal findings).1,2 A separate guideline on felbamate (FBM) in intractable epilepsy was published (last reaffirmed July 16, 2016).
TABLE 1.
Summary of the 2004 AAN guideline Level A or B recommendations regarding the use of new AEDs in treatment of new-onset epilepsy
Since the 2004 publications, new studies emerged in the 8 second-generation and 6 newer (third-generation) AEDs (eslicarbazepine [ESL], ezogabine [EZG], lacosamide [LCM], perampanel [PER], pregabalin [PGB], rufinamide [RFN]). The US Food and Drug Administration has since approved 2 older AEDs (clobazam [CLB], vigabatrin [VGB]; in use for decades in Canada, Europe, and Latin America), for treating certain epileptic disorder types in the United States.
This update reviews new evidence for efficacy, safety, and tolerability of CLB, VGB, and the 8 second-generation and 6 third-generation AEDs. The 2004 guidelines examine the mechanisms of action, common and serious adverse events (AEs), and pharmacokinetic properties of the second-generation AEDs.1–3
A companion guideline update examines the evidence in treatment-resistant epilepsy.4
This article summarizes the guideline findings, conclusions, and recommendations. The complete guideline, including appendices e-1 through e-6 and tables e-1 and e-2, is available as a data supplement at Neurology.org.
DESCRIPTION OF THE ANALYTIC PROCESS
The AAN and AES convened an expert panel to develop this guideline in accordance with the 2004 AAN process manual.5 The complete guideline (data supplement) describes the literature search strategy and evidence review process. Recommendations are based on Class I, II, and III studies; Class IV studies are not discussed.
ANALYSIS OF EVIDENCE
For adults and children with newly diagnosed epilepsy, are CLB, ESL, EZG, FBM, gabapentin (GBP), lamotrigine (LTG), levetiracetam (LEV), LCM, oxcarbazepine (OXC), PER, PGB, RFN, tiagabine (TGB), topiramate (TPM), VGB, and zonisamide (ZNS) effective as monotherapy, and how does their efficacy and tolerability compare with those of older AEDs?
The original practice guidelines included studies that enrolled patients with a mixed group of syndromes.1 With the 2004 criteria, ratings were lowered from Class I to Class II for the 3 LTG studies and the 1 GBP study, and from Class I to Class III for the 2 TPM studies. The 4 OXC studies remain Class I. Thus, GBP and TPM are considered possibly effective (Level C) and LTG probably effective (Level B); the OXC recommendation level remains unchanged (Level A).
Monotherapy in adults with new-onset epilepsy with focal epilepsy or unclassified tonic–clonic seizures
Since the 2004 publications, 2 Class I, 5 Class II, and 2 Class III studies have been published. One study was conducted in patients aged ≥60 years and one in patients aged ≥65 years.
GBP vs LTG vs carbamazepine
A Class II double-blind randomized study compared efficacy and tolerability of GBP (≤1,500 mg/d), LTG (≤150 mg/d), and immediate-release carbamazepine (CBZ-IR) (≤600 mg/d) in patients aged ≥60 years6; the primary outcome was retention in the trial for 12 months on the basis of seizure recurrence or AEs despite dose adjustments. Drug discontinuation was less frequent among patients randomized to LTG than to GBP or CBZ-IR because of better LTG tolerability. The most frequently occurring AEs included a higher occurrence of weight gain and water retention with GBP than with LTG or CBZ, of rash with CBZ than with LTG, and of hyponatremia with CBZ than with GBP. The 3 AEDs did not differ with respect to neurologic AEs.
LTG vs controlled-release carbamazepine
The differences between LTG and CBZ-IR identified in the study just described were not reproduced in a Class I study comparing LTG efficacy and tolerability (100–500 mg/d) and controlled-release carbamazepine (CBZ-CR) (400–2,000 mg/d) in treating focal epilepsy among patients ≥65 years.7 Retention in the trial was the primary outcome and was based on seizure recurrence and AE occurrence. In the trial's final 20 weeks, the seizure-free rates were the same (52% for LTG vs 57% for CBZ-CR). AE occurrence leading to withdrawal was higher for CBZ-CR (14% for LTG vs 25% for CBZ-CR), but this difference did not reach statistical significance. The most common AEs included dizziness, headache, and fatigue with LTG use and rash, headache, dizziness, somnolence, and fatigue with CBZ use.
LEV vs CBZ-CR
A Class II study compared the efficacy and tolerability of LEV 1,000–3,000 mg/d and CBZ-CR 400–1,200 mg/d.8 Seizure-free rates were almost identical for LEV and CBZ-CR at 6 months and 1 year. Depression and insomnia occurred significantly more frequently with LEV use and back pain and weight gain with CBZ-CR use. For both AEDs, headache, fatigue, somnolence, and dizziness were the most frequent AEs.
ZNS vs CBZ-CR
A double-blind Class II study compared efficacy and tolerability of ZNS 300–500 mg/d and CBZ-CR 600–1,200 mg/d in patients with focal-onset (74%) or unknown (26%) epilepsy.9 Primary outcome was percentage of patients achieving seizure freedom for 26 weeks. Seizure-free rates for 26 weeks were nearly identical for ZNS and CBZ-CR. Decreased appetite and weight loss occurred more frequently with ZNS use and dizziness with CBZ-CR use. Headache, dizziness, and somnolence were the most frequent AEs in both AEDs.
LTG vs GBP vs TPM vs OXC vs carbamazepine
Standard and New Antiepileptic Drugs (SANAD)-Arm A is a Class III randomized unblinded trial in children and adults, of whom 89% had focal epilepsy.10 The clinician chose initial doses, formulation, and titration rate. Primary outcomes were time to treatment failure and time to 12-month remission. For former outcome, LTG outperformed carbamazepine (CBZ), GBP, and TPM and had a nonsignificant advantage over OXC. For the latter outcome, CBZ outperformed GBP and had a nonsignificant advantage over LTG, OXC, and TPM. LTG was noninferior to CBZ for 12-month remission at 2 and 4 years (secondary outcomes). AE intolerability leading to discontinuation was less frequent with GBP and LTG than with OXC and TPM. Although the frequency of tiredness and fatigue was comparable across the AEDs, rash was more frequent with CBZ and OXC; weight gain, dizziness, and ataxia were more frequent with GBP; and psychiatric symptoms, weight loss, and paresthesia were more frequent with TPM.
VGB vs CBZ-IR
One Class I study11 and 1 Class III study12 compared the safety and efficacy of CBZ-IR and VGB. The primary outcome of the Class I study was time to withdrawal due to lack of efficacy or AEs; secondary outcomes included time to 6-month seizure remission, time to first seizure after reaching the initial target dose (≤600 mg/d CBZ-IR and ≤2 g/d VGB), and AE development. Although there were no differences between the 2 AEDs regarding time to withdrawal due to lack of efficacy, time to 6-month remission was significantly shorter and time to first seizure significantly longer for CBZ-IR than for VGB. VGB was more frequently associated with psychiatric symptoms and weight gain; rash occurred more frequently with CBZ-IR.
In the Class III study, there were significantly more patients seizure free on CBZ-IR than VGB. Serious rash occurred with CBZ-IR; VGB was associated with a significantly higher frequency of scintillating visual disturbances and myoclonic jerks.
PGB vs LTG
In a Class II double-blind study,13 the primary outcome was the proportion of patients seizure free for 6 continuous months during the efficacy phase. Doses could be adjusted for the first 24 weeks and then were fixed. A majority of patients received PGB 150 mg/d or LTG 100 mg/d when doses were fixed. Secondary outcomes included withdrawal due to lack of efficacy, time to first seizure, and time to seizure freedom after dose escalation. Seizure freedom was achieved by significantly more patients taking LTG than PGB, as LTG use saw a comparatively greater reduction in patients experiencing only secondarily generalized tonic–clonic (GTC) seizures. Weight gain occurred more often among patients receiving PGB. Other frequent AEs did not differ in frequency between the 2 AEDs and included headaches, dizziness, somnolence, and fatigue. Moreover, the 2 AEDs differed only slightly in frequency of AE-related withdrawal (8% of those taking PGB vs 7% of those taking LTG).
TPM vs phenytoin
One Class II double-blind study compared TPM 100 mg/d followed by phenytoin (PHT) (1,000 mg/d load, 300 mg/d maintenance) for preventing seizure recurrence over 28 days.14 The primary endpoint was time to recurrence of a first focal seizure with altered awareness or GTC seizure (or both) by study day 28, which occurred in 18.9% of patients on TPM and 9.7% on PHT. However, the study could not establish noninferiority. The most frequent AEs included dizziness and somnolence. PHT use saw a higher incidence of rash leading to discontinuation; paresthesia was more common with TPM use. Cognitive AEs occurred more frequently among patients on TPM; these led to only 1.5% of such patients withdrawing from the study. Of note, the data from this study apply only to efficacy over 28 days and cannot be generalized to long-term treatment.
Conclusions
LTG is probably effective in patients aged ≥60 years with new-onset focal epilepsy (1 Class I study, 1 Class II study). In these 2 studies, LTG was better tolerated than CBZ-IR but not CBZ-CR.
GBP is possibly as effective and better tolerated than CBZ-IR in patients aged ≥60 years with new-onset focal epilepsy (1 Class II study).
LEV is possibly as effective as CBZ-CR in patients with new-onset focal epilepsy (1 Class II study). AEs were comparable between the 2 AEDs. Not enough patients experienced unclassified GTC seizures to identify differences between CBZ-CR and LEV.
ZNS is possibly as effective as CBZ-CR in patients with new-onset focal epilepsy (1 Class II study). The 2 AEDs had comparable AE frequency. Not enough patients had unclassified GTC seizures to identify differences between CBZ-CR and ZNS.
Evidence is insufficient to compare the efficacy of GBP, OXC, and TPM with that of CBZ-IR or CBZ-CR in patients with new-onset or relapsing focal epilepsy or unclassified GTC seizures (1 Class III study).
VGB is probably less efficacious than CBZ-IR in new-onset focal epilepsy (a secondary endpoint of 1 Class I study and of 1 Class III study). Not enough patients experienced unclassified GTC seizures to identify differences between VGB and CBZ-IR. Moreover, VGB is associated with increased risk of serious AEs.
PGB is possibly less effective than LTG at the study doses, but the PGB dose was lower than typically used for patients with epilepsy (1 Class II study). Data from this study and the 3 LTG studies15–17 examined in the 2004 guideline suggest that LTG is probably effective in treating new-onset focal epilepsy.
It is not possible to determine whether TPM is equivalent to PHT in urgent treatment of new-onset or recurrent focal epilepsy, unclassified GTC seizures, or GE presenting with GTC seizures (1 Class II study).
No high-quality studies suggest CLB, ESL, EZG, FBM, GBP, LCM, LEV, LTG, OXC, PER, PGB, RFN, TGB, TPM, VGB, or ZNS is effective in treating new-onset epilepsy.
Evidence is insufficient to demonstrate AED efficacy in unclassified GTC seizures (no study had enough patients with this seizure type).
Recommendations
In patients with new-onset focal epilepsy or unclassified GTC seizures
LTG use should be considered to decrease seizure frequency (Level B)
LTG use should be considered (Level B) and GBP use may be considered (Level C) to decrease seizure frequency in patients aged ≥60 years
LEV use may be considered to decrease seizure frequency (Level C)
ZNS use may be considered to decrease seizure frequency (Level C)
VGB use appears to be less efficacious than CBZ-IR use and may not be offered (Level C); furthermore, toxicity profile precludes VGB use as first-line therapy
PGB use at 150 mg/d is possibly less efficacious than LTG use at 100 mg/d (Level C)
Evidence is insufficient to consider GBP, OXC, or TPM instead of CBZ (Level U)
Evidence is insufficient to consider TPM instead of PHT in urgent treatment of new-onset or recurrent focal epilepsy, unclassified GTC seizures, or GE presenting with GTC seizures (Level U)
Data are lacking to support or refute use of third-generation AEDs, CLB, FBM, or VGB in treating new-onset epilepsy (Level U)
Data are lacking to support or refute use of newer AEDs in treating unclassified GTC seizures (Level U)
Monotherapy in children with new-onset epilepsy with either focal epilepsy or unclassified GTC seizures
High-dose vs low-dose TPM
In 1 Class II study of children and adolescents,18 the Kaplan-Meier survival analyses for time to next seizure favored the higher dose (400 mg/d), and the probability of seizure freedom was significantly higher among patients randomized to high-dose than low-dose TPM (50 mg/d) (90% and 78%, respectively, at 6 months; 85% and 62%, respectively, at 12 months). AEs occurred in 4% of children taking 50 mg/d and in 14% of those taking 400 mg/d. The most frequent AEs included headache, decreased appetite, weight loss, somnolence, dizziness, paresthesia, and problems with concentration or attention (or both).
Conclusions
TPM monotherapy at 400 mg/d is possibly more effective than at 50 mg/d in treating children and adolescents with new-onset focal seizures or generalized-onset GTC seizures (1 Class II study). The higher dose is associated with more AEs and is not used in these patients in clinical practice. Of note, this study was done for regulatory and not clinical purposes, and the doses used are not clinically relevant. Therefore, the study data are nonapplicable to clinical practice.
Recommendation
Although the data from this study would suggest that TPM monotherapy is possibly more efficacious at 400 mg/d than at 50 mg/d for treating children and adolescents with new-onset focal epilepsy or generalized-onset GTC seizures (1 Class II study), no recommendations can be made regarding TPM use at the studied doses, particularly in new-onset epilepsy and pediatric patients.
Monotherapy in adults and children with new-onset GE or unclassified GTC seizures
LTG vs TPM vs valproic acid
A Class III multicenter, randomized, open-label, parallel study, SANAD-Arm B, was conducted in 716 outpatient children and adults with seizure disorders (of which almost 90% had focal epilepsy) in whom a clinician “regarded valproate the better standard treatment option than carbamazepine.”10 The clinician chose initial doses and formulations. Patients had to have been diagnosed with new-onset epilepsy (87.7% of patients enrolled), have a seizure disorder failing to remit with a previous monotherapy regimen (excluding the AEDs studied in this trial [8.4%]), or have a seizure disorder that was in remission but relapsed after AED discontinuation (3.9%). GE was diagnosed in 63% of patients and focal epilepsy in 7.3%; 27% had unclassified epilepsy. Patients were randomized to LTG, TPM, or valproic acid (VPA); the treating clinician determined the target doses according to everyday practice doses.19 Primary outcomes were time to treatment failure (defined as AED discontinuation because of seizures or AEs, or both) and time to 1-year remission. VPA outperformed TPM for time to treatment failure but was comparable with LTG. When the analysis was restricted to GE, VPA was superior to LTG and TPM. For time to 1-year remission, VPA was superior to LTG when all patients were included or when analysis was restricted to only those with GE, but VPA did not differ from TPM in either analysis. Weight gain was the most frequent AE leading to treatment failure with VPA, and fatigue and psychiatric and cognitive symptoms were the most common AEs associated with TPM. Rash was the most common AE leading to LTG discontinuation (4%).
Conclusion
Evidence is insufficient to compare efficacy of LTG and TPM with that of VPA in children and adults with new-onset or relapsing GE (1 Class III study).
Monotherapy in adults and adolescents with new-onset focal, GE, or unclassified GTC seizures
LEV vs extended-release VPA or CBZ-CR
KOMET, a Class III multicenter, randomized, open-label parallel study, compared effectiveness of LEV with that of extended-release VPA (VPA-ER) or CBZ-CR in 1,688 outpatient adolescents (aged ≥16 years) and adults with new-onset epilepsy.20 GE was diagnosed in 34.8% of patients and focal epilepsy in 64.7%; 2.1% had unclassified epilepsy. The clinician was allowed to choose VPA-ER or CBZ-CR as the better standard treatment option, and patients were then randomized (1:1) to treatment with LEV or 1 of the 2 standard AEDs. Initial target doses were reached over 2 weeks (LEV 1,000 mg/d, VPA-ER 1,000 mg/d, CBZ-CR 600 mg/d), and with seizure occurrence, the clinician could increase the dose to 3,000 mg/d for LEV, 2,000 mg/d for VPA-ER, and 1,600 mg/d for CBZ-CR. Of the patients randomized to standard AEDs, 65.8% treated with VPA-ER had only GE, and 86.5% treated with CBZ-CR had only focal epilepsy. Primary outcomes were time to treatment failure (defined as AED discontinuation caused by seizures or AEs, or both), and LEV was compared with VPA-ER and with CBZ-CR. Time to treatment withdrawal was similar for LEV and VPA-ER; a nonsignificantly longer time to treatment withdrawal occurred with LEV than with CBZ-CR. The 3 drugs were comparable regarding frequency of drug-related AEs and AEs leading to drug discontinuation. The most frequent AEs were weight gain and tremor with VPA, depression with LEV, and rash with CBZ-CR. Headache, fatigue, and dizziness were equally frequent across these AEDs.
Conclusion
Evidence is insufficient to compare efficacy of CBZ-CR, LEV, and VPA-ER in adolescents and adults with new-onset GE and focal epilepsy (1 Class III study).
Childhood absence epilepsy
A Class I study compared the efficacy, tolerability, and neuropsychological effects of LTG (12 mg/kg/d), ethosuximide (ETS) (60 mg/kg/d), and VPA (60 mg/kg/d).21 Study outcomes included freedom from treatment failure after 16 weeks (which could be extended to 20 weeks if necessary) and attention disturbances measured with objective tests (e.g., continuous performance test). Children randomized to ETS and VPA had comparable freedom-from-failure rates, which were significantly higher than the LTG rates. Attention disturbances were significantly more common with VPA than with ETS. These seizure control and cognitive AE differences were maintained at a 12-month follow-up evaluation study.22
Conclusion
LTG is probably not as effective as ETS or VPA for treating absence seizures in children with childhood absence epilepsy (1 Class I study). Attention disturbances are more common with VPA use.
Clinical context
ETS use is limited to patients with childhood absence epilepsy without associated GTC seizures.
Recommendation
Unless there are compelling reasons based on AE profile, ETS or VPA use should be considered before LTG use to decrease seizure frequency in treating absence seizures in childhood absence epilepsy (Level B).
No high-quality studies suggest CLB, ESL, EZG, FBM, GBP, LCM, LEV, LTG, OXC, PER, PGB, RFN, TGB, TPM, VGB, or ZNS is effective in treating new-onset epilepsy.
CLINICAL CONTEXT
The studies examined here on treating new-onset epilepsy were limited to comparisons between first- and second-generation AEDs (and VGB). Therefore, recommendations can be made related only to those medications and cannot be generalized to comparisons involving other AEDs. The data reviewed apply to treatment of focal epilepsy and limit the ability to make recommendations regarding these drugs for unclassified GTC seizures.
The single study wherein the majority of patients had GTC seizures secondary to GE was Class III, so no recommendations can be made regarding the second-generation AEDs (LTG, TPM) used in treating this epilepsy type. The Class I study of children with absence epilepsy suggested that LTG is probably not as effective in this epilepsy type as the 2004 guideline suggests.
A recent FDA strategy allows extrapolation of efficacy across populations and granted approval of eslicarbazepine and lacosamide (oral only for pediatric age group) as add-on or monotherapy for focal epilepsy in persons ≥4 years old and perampanel as monotherapy for focal epilepsy.
FBM and VGB are not recommended in new-onset epilepsy for clinical use due to serious AEs, as there are other agents that are both safe and efficacious.
RECOMMENDATIONS FOR FUTURE RESEARCH
GBP, LEV, LTG, OXC, and ZNS are second-generation AEDs that can be considered for new-onset focal epilepsy. Change from Class I to Class III of 2 TPM studies reviewed in the 2004 guideline23,24 suggests that TPM may be possibly effective and its efficacy should be reinvestigated in a randomized controlled trial (RCT) with doses commonly used in clinical practice.
No data are available on efficacy and tolerability of TGB or any third-generation AEDs and CLB in treating new-onset focal epilepsy. The trial with PGB should be repeated using higher doses to determine whether PGB can be considered efficacious.
Among second-generation AEDs, only OXC has evidence from a Class I study suggesting efficacy in new-onset focal epilepsy.25 No studies exist on efficacy of second-generation AEDs in new-onset GE with GTC seizures in children or adolescents with juvenile absence epilepsy or juvenile myoclonic epilepsy (JME). Data are unavailable about efficacy of third-generation AEDs in new-onset epilepsy in children. The need is clear for RCTs in pediatric patients with new-onset epilepsy.
No data exist on use of second- and third-generation AEDs, CLB, or VGB in treating adults with new-onset GE with GTC seizures or in JME. Such studies should be included in future research.
Third-generation AEDs found equivalent to LTG or to CBZ-CR or VPA (or both CBZ-CR and VPA) for treating new-onset focal epilepsy and GE, respectively, should undergo head-to-head comparisons with third-generation AEDs in double-blind, controlled, parallel studies for efficacy.
DISCLAIMER
Clinical practice guidelines, practice advisories, systematic reviews and other guidance published by the American Academy of Neurology and its affiliates are assessments of current scientific and clinical information provided as an educational service. The information: 1) should not be considered inclusive of all proper treatments, methods of care, or as a statement of the standard of care; 2) is not continually updated and may not reflect the most recent evidence (new evidence may emerge between the time information is developed and when it is published or read); 3) addresses only the question(s) specifically identified; 4) does not mandate any particular course of medical care; and 5) is not intended to substitute for the independent professional judgment of the treating provider, as the information does not account for individual variation among patients. In all cases, the selected course of action should be considered by the treating provider in the context of treating the individual patient. Use of the information is voluntary. AAN provides this information on an “as is” basis, and makes no warranty, expressed or implied, regarding the information. AAN specifically disclaims any warranties of merchantability or fitness for a particular use or purpose. AAN assumes no responsibility for any injury or damage to persons or property arising out of or related to any use of this information or for any errors or omissions.
CONFLICT OF INTEREST
The American Academy of Neurology (AAN) and the American Epilepsy Society (AES) committed to producing independent, critical, and truthful clinical practice guidelines (CPGs). Significant efforts are made to minimize the potential for conflicts of interest to influence the recommendations of this CPG. To the extent possible, the AAN and AES keep separate those who have a financial stake in the success or failure of the products appraised in the CPGs and the developers of the guidelines. Conflict of interest forms were obtained from all authors and reviewed by an oversight committee prior to project initiation. The AAN and AES limit the participation of authors with substantial conflicts of interest. The AAN and AES forbid commercial participation in, or funding of, guideline projects. Drafts of the guideline have been reviewed by at least three AAN committees, three AES committees, a network of neurologists, Neurology peer reviewers, and representatives from related fields. The AAN Guideline Author Conflict of Interest Policy can be viewed at www.aan.com. For complete information on this process, access the 2004 AAN process manual.5
AUTHOR CONTRIBUTIONS
Dr. Kanner: study concept and design, acquisition of data, analysis or interpretation of data, drafting/revising the manuscript, critical revision of the manuscript for important intellectual content, study supervision.
Dr. Ashman: study concept and design, acquisition of data, analysis or interpretation of data, drafting/revising the manuscript, critical revision of the manuscript for important intellectual content, study supervision.
Dr. Gloss: acquisition of data, analysis or interpretation of data, drafting/revising the manuscript, critical revision of the manuscript for important intellectual content, study supervision.
Dr. Harden: analysis or interpretation of data, drafting/revising the manuscript, critical revision of the manuscript for important intellectual content, study supervision.
Dr. Bourgeois: study concept and design, acquisition of data, analysis or interpretation of data.
Dr. Bautista: study concept and design, acquisition of data, analysis or interpretation of data.
Dr. Abou-Khalil: study concept and design, acquisition of data, analysis or interpretation of data.
Dr. Burakgazi-Dalkilic: study concept and design, acquisition of data, analysis or interpretation of data.
Dr. Llanas Park: study concept and design, acquisition of data, analysis or interpretation of data.
Dr. Stern: study concept and design, acquisition of data, analysis or interpretation of data.
Dr. Hirtz: study concept and design, acquisition of data, analysis or interpretation of data.
Dr. Nespeca: study concept and design, acquisition of data, analysis or interpretation of data.
Dr. Gidal: study concept and design, acquisition of data, analysis or interpretation of data.
Dr. Faught: study concept and design, acquisition of data, analysis or interpretation of data.
Dr. French: study concept and design, analysis or interpretation of data, drafting/revising the manuscript, critical revision of the manuscript for important intellectual content, study supervision.
STUDY FUNDING
This practice guideline was developed with financial support from the American Academy of Neurology (AAN). Authors who serve or served as AAN subcommittee members or methodologists (A.M.K., E.A., D.G., C.H., D.H., and J.F.) were reimbursed by the AAN for expenses related to travel to subcommittee meetings where drafts of manuscripts were reviewed.
DISCLOSURES
A. Kanner has served on a scientific advisory board for UCB but the honorarium was transferred to the Department of Neurology at the University of Miami, Miller School of Medicine; receives royalties from Psychiatric Aspects of Epilepsy, Treatment of Depression in Neurological Disorders, and Psychiatric Controversies in Epilepsy, and received honoraria from Medscape and as a consultant for Neuropace.
E. Ashman receives funding from the American Academy of Neurology (AAN) for travel; has served as associate editor, level of evidence, for Neurology; has performed imaging studies that include MRI, electrophysiology, and electroencephalography in patients who are comatose; and has provided medical reviews and consultations for lawsuits and medical claims as part of his role in the US Air Force.
D. Gloss serves as an evidence-based medicine consultant for the AAN.
C. Harden receives royalties from UpToDate and Wiley; serves on the speakers bureau for UBC; and has received research support from the National Institute of Neurological Disorders and Stroke (NINDS) of the NIH and the Epilepsy Therapy Project.
B. Bourgeois serves on the data and safety monitoring board for a clinical trial conducted by Pfizer Pharmaceuticals, for which he receives honoraria; and receives royalties for The Epilepsy Prescriber's Guide to Antiepileptic Drugs.
J. Bautista serves on the National Quality Forum Neurology Steering Committee and the Neurology Endorsement Maintenance Committee and has received research funding from the NIH and NINDS.
B. Abou-Khalil has served on but declined honoraria from scientific advisory boards for Sunovion and GlaxoSmithKline; served on the editorial board for Epilepsy Research and Clinical Neurophysiology; and received royalties for Atlas of EEG & Seizure Semiology. His institution received research support from UCB, GlaxoSmithKline, Valeant, Sunovion, Upsher-Smith, Pfizer, Cyberonics, and SK Life Science, from the NIH for the Epilepsy Phenome/Genome Project and from the Human Epilepsy Project.
E. Burakgazi-Dalkilic serves on a speakers bureau for Eisai Pharmaceuticals.
E. Llanas Park reports no relevant disclosures.
J. Stern serves on the scientific advisory board for Sunovion and Lundbeck; serves as an editor for MedLink Neurology; receives royalties for Atlas of EEG Patterns and Atlas of Video-EEG Monitoring; receives honoraria from and serves on the speakers bureaus of UCB, Lundbeck, Eisai, Cyberonics, and Sunovion; and performs clinical practice in epilepsy (50% of his time).
D. Hirtz reports no relevant disclosures.
M. Nespeca serves on the Scientific Advisory Committee of the Angelman Syndrome Foundation; is a co-investigator for a US Food and Drug Administration–funded trial on levetiracetam vs phenobarbital in neonatal seizures and for industry-sponsored trials on everolimus (Novartis) for epilepsy in persons with tuberous sclerosis and on fenfluramine (Zogenix) in Dravet syndrome.
B. Gidal serves on scientific advisory boards and speakers bureaus for UCB, Eisai, and Sunovion, for which he receives honoraria; performs clinical practice in epilepsy (20% of his time); and has provided expert testimony, prepared an affidavit, and acted as a witness in the legal proceeding of Activis v Depomed.
E. Faught serves on the scientific advisory boards of Eisai, Lundbeck, SK Life Science, Supernus, Sunovion, and UCB; has received research support from Brain Sentinel, UCB, the Centers for Disease Control and Prevention, University of Alabama at Birmingham, and the Epilepsy Consortium; and has acted as a witness in legal proceedings for Rushton Stakley.
J. French receives New York University salary support from the Epilepsy Foundation and for consulting work on behalf of the Epilepsy Study Consortium for Eisai, GlaxoSmithKline, Novartis, Pfizer, Sunovion, UCB, and Upsher Smith; has received research grants from Eisai Medical Research, Lundbeck, Pfizer, Sunovion, and UCB; has received grants from the Epilepsy Research Foundation, Epilepsy Study Consortium, Epilepsy Therapy Project, and the NINDS of the NIH; serves on the editorial boards of Lancet Neurology, Neurology Today, and Epileptic Disorders; serves as scientific officer for the Epilepsy Foundation for which New York University receives salary support; and has received travel reimbursement related to research, advisory meetings, or presentation of results at scientific meetings from the Epilepsy Study Consortium, the Epilepsy Foundation, Eisai, GlaxoSmithKline, Pfizer, UCB, and Upsher-Smith.
References
- 1.French JA, Kanner AM, Bautista J et al. Efficacy and tolerability of the new antiepileptic drugs I: treatment of new-onset epilepsy. Neurology. 2004;62:1252–1260. doi: 10.1212/01.wnl.0000123693.82339.fc. [DOI] [PubMed] [Google Scholar]
- 2.French JA, Kanner AM, Bautista J et al. Efficacy and tolerability of the new antiepileptic drugs II: treatment of refractory epilepsy. Neurology. 2004;62:1261–1273. doi: 10.1212/01.wnl.0000123695.22623.32. [DOI] [PubMed] [Google Scholar]
- 3.French J, Smith M, Faught E, Brown L. Practice advisory: the use of felbamate in the treatment of patients with intractable epilepsy: report of the Quality Standards Subcommittee of the American Academy of Neurology and the American Epilepsy Society. Neurology. 1999;52:1540–1545. doi: 10.1212/wnl.52.8.1540. [DOI] [PubMed] [Google Scholar]
- 4.Kanner AM, Ashman E, Gloss D Practice guideline update: Efficacy and tolerability of the new antiepileptic drugs I: Treatment of new-onset epilepsy. .; on behalf of the American Academy of Neurology and American Epilepsy Society. Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology and the American Epilepsy Society. In development.
- 5.American Academy of Neurology Clinical Practice Guidelines Process Manual. 2004 ed. St. Paul, MN: The American Academy of Neurology; 2004. https://www.aan.com/Guidelines/Home/UnderDevelopment Published 2004. Accessed January 30, 2010. [Google Scholar]
- 6.Rowan AJ, Ramsay RE, Collins JF et alNew onset geriatric epilepsy: a randomized study of gabapentin, lamotrigine, and carbamazepine. Neurology. 2005;64:1868–1873. doi: 10.1212/01.WNL.0000167384.68207.3E. .; VA Cooperative Study 428 Group. [DOI] [PubMed] [Google Scholar]
- 7.Saetre E, Perucca E, Isojärvi J, Gjerstad L, LAM 40089 Study Group An international multicenter randomized double-blind controlled trial of lamotrigine and sustained-release carbamazepine in the treatment of newly diagnosed epilepsy in the elderly. Epilepsia. 2007;48:1292–1302. doi: 10.1111/j.1528-1167.2007.01128.x. [DOI] [PubMed] [Google Scholar]
- 8.Brodie MJ, Perucca E, Ryvlin P, Ben-Menachem E, Meencke HJ, Levetiracetam Monotherapy Study Group Comparison of levetiracetam and controlled-release carbamazepine in newly diagnosed epilepsy. Neurology. 2007;68:402–408. doi: 10.1212/01.wnl.0000252941.50833.4a. [DOI] [PubMed] [Google Scholar]
- 9.Baulac M, Brodie MJ, Patten A, Segieth J, Giorgi L. Efficacy and tolerability of zonisamide versus controlled-release carbamazepine for newly diagnosed partial epilepsy: a phase 3, randomised, double-blind, non-inferiority trial. Lancet Neurol. 2012;11:579–588. doi: 10.1016/S1474-4422(12)70105-9. [DOI] [PubMed] [Google Scholar]
- 10.Marson AG, Al-Kharusi AM, Alwaidh M et al. The SANAD study of effectiveness of carbamazepine, gabapentin, lamotrigine, oxcarbazepine, or topiramate for treatment of partial epilepsy: an unblinded randomised controlled trial. Lancet. 2007;369:1000–1015. doi: 10.1016/S0140-6736(07)60460-7. ; SANAD Study Group. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chadwick D. Safety and efficacy of vigabatrin and carbamazepine in newly diagnosed epilepsy: a multicentre randomised double-blind study. Vigabatrin European Monotherapy Study Group. Lancet. 1999;354:13–19. doi: 10.1016/s0140-6736(98)10531-7. [DOI] [PubMed] [Google Scholar]
- 12.Kälviäinen R, Aikiä M, Saukkonen AM, Mervaala E, Riekkinen PJ Sr. Vigabatrin vs carbamazepine monotherapy in patients with newly diagnosed epilepsy. A randomized, controlled study. Arch Neurol. 1995;52:989–996. doi: 10.1001/archneur.1995.00540340081016. [DOI] [PubMed] [Google Scholar]
- 13.Kwan P, Brodie MJ, Kälviäinen R, Yurkewicz J, Weaver J, Knapp LE. Efficacy and safety of pregabalin versus lamotrigine in patients with newly diagnosed partial seizures: a phase 3, double-blind, randomised, parallel-group trial. Lancet. 2011;10:881–890. doi: 10.1016/S1474-4422(11)70154-5. [DOI] [PubMed] [Google Scholar]
- 14.Ramsay E, Faught E, Krumholz A et alEfficacy, tolerability, and safety of rapid initiation of topiramate versus phenytoin in patients with new-onset epilepsy: a randomized double-blind clinical trial. Epilepsia. 2010;51:1970–1977. doi: 10.1111/j.1528-1167.2010.02670.x. .; CAPSS-272 Study Group. [DOI] [PubMed] [Google Scholar]
- 15.Brodie MJ, Overstall PW, Giorgi L. Multicentre, double-blind, randomised comparison between lamotrigine and carbamazepine in elderly patients with newly diagnosed epilepsy. The UK Lamotrigine Elderly Study Group. Epilepsy Res. 1999;37:81–87. doi: 10.1016/s0920-1211(99)00039-x. [DOI] [PubMed] [Google Scholar]
- 16.Brodie MJ, Richens A, Yuen AW. Double-blind comparison of lamotrigine and carbamazepine in newly diagnosed epilepsy. UK Lamotrigine/Carbamazepine Monotherapy Trial Group. Lancet. 1995;345:476–479. doi: 10.1016/s0140-6736(95)90581-2. [DOI] [PubMed] [Google Scholar]
- 17.Steiner TJ, Dellaportas CL, Findley LJ et al. Lamotrigine monotherapy in newly diagnosed untreated epilepsy: a double-blind comparison with phenytoin. Epilepsia. 1999;40:601–607. doi: 10.1111/j.1528-1157.1999.tb05562.x. [DOI] [PubMed] [Google Scholar]
- 18.Glauser TA, Dlugos DJ, Dodson WE, Grinspan A, Wang S, Wu SC, EPMN-106/INT-28 Investigators Topiramate monotherapy in newly diagnosed epilepsy in children and adolescents. J Child Neurol. 2007;22:693–699. doi: 10.1177/0883073807303997. [DOI] [PubMed] [Google Scholar]
- 19.Marson AG, Al-Kharusi AM, Alwaidh M et alThe SANAD study of effectiveness of valproate, lamotrigine, or topiramate for generalised and unclassifiable epilepsy: an unblinded randomised controlled trial. Lancet. 2007;369:1016–1026. doi: 10.1016/S0140-6736(07)60461-9. .; SANAD Study Group. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Trinka E, Marson AG, Van Paesschen W et alKOMET: an unblinded, randomized, two parallel-group, stratified trial comparing the effectiveness of levetiracetam with controlled-release carbamazepine and extended-release sodium valproate as monotherapy in patients with newly diagnosed epilepsy. J Neurol Neurosurg Psychiatry, 2013;84:1138–1147. doi: 10.1136/jnnp-2011-300376. .; KOMET Study Group. [DOI] [PubMed] [Google Scholar]
- 21.Glauser TA, Cnaan A, Shinnar S et alEthosuximide, valproic acid, and lamotrigine in childhood absence epilepsy. N Engl J Med. 2010;362:790–799. doi: 10.1056/NEJMoa0902014. .; Childhood Absence Epilepsy Study Group. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Glauser TA, Cnaan A, Shinnar S et alEthosuximide, valproic acid, and lamotrigine in childhood absence epilepsy: initial monotherapy outcomes at 12 months. Epilepsia. 2013;54:141–155. doi: 10.1111/epi.12028. .; Childhood Absence Epilepsy Study Team. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Gilliam FG, Veloso F, Bomhof MA et al. A dose-comparison trial of topiramate as monotherapy in recently diagnosed partial epilepsy. Neurology. 2003;60:196–202. doi: 10.1212/01.wnl.0000048200.12663.bc. [DOI] [PubMed] [Google Scholar]
- 24.Privitera MD, Brodie MJ, Mattson RH et alTopiramate, carbamazepine and valproate monotherapy: double-blind comparison in newly diagnosed epilepsy. Acta Neurol Scand. 2003;107:165–175. doi: 10.1034/j.1600-0404.2003.00093.x. .; EPMN 105 Study Group. [DOI] [PubMed] [Google Scholar]
- 25.Guerreiro MM, Vigonius U, Pohlmann H et al. A double-blind controlled clinical trial of oxcarbazepine versus phenytoin in children and adolescents with epilepsy. Epilepsy Res. 1997;27:205–213. doi: 10.1016/s0920-1211(97)00025-9. [DOI] [PubMed] [Google Scholar]