

Abstract
Objectives:
To explore beliefs, attitudes, and barriers associated with uptake of the seasonal influenza vaccine among visitors to primary healthcare clinics.
Methods:
This was a cross-sectional, self-administered questionnaire-based study of 300 people visiting Family Medicine Centers, King Abdulaziz Medical City, Riyadh, Saudi Arabia, between May 2017 and October 2017.
Results:
Most respondents reported that they never get vaccinated (63.3%), but most intend to get the vaccination in future. Only 7.7% of respondents had ever experienced side-effects from the influenza vaccine. Reported barriers to vaccination include :a desire to avoid medication, the fact that the Ministry of Health has not made vaccination obligatory, concerns about the side-effects of the vaccine, the belief that one is at low risk of acquiring influenza, and the idea that influenza is a simple disease with no need for prevention. The rate of vaccination was higher among males than females. More females than males said they refused the influenza vaccine because of concerns about side effects or having a phobia of injections.
Conclusion:
Although most respondents said they were concerned about influenza and believed the vaccine to be effective, this study revealed a low rate of influenza vaccination. More public education and better arrangements for vaccination are required in the healthcare setting to overcome several reported barriers to vaccination.
Influenza is a highly contagious respiratory viral illness that occurs in certain seasons of the year. The 2 main types of human influenza viruses are influenza virus A and influenza virus B, both of which are easily spread between people, and are responsible for seasonal influenza epidemics each year, with a significant disease burden and significant morbidity and mortality.1,2 Vaccination against influenza is the main way to reduce the substantial health burden that seasonal influenza causes, and is the primary tool to prevent influenza infection.3 The Advisory Committee on Immunization Practices at the US Centers for Disease Control and Prevention (CDC) recommended that all people above age 6 months receive the influenza vaccination annually unless contraindicated.4 There are marked differences in seasonal influenza vaccination rates between different countries, and between different times of the year.5-7 In Arab countries, the vaccination rates are variable. For example, according to a study carried out in Lebanon in 2015, the overall vaccination rate was 27.6%,8 while in Jordan, 2 studies reported a low vaccination rate between 9.9 and 20% of adults.9,10 Locally, a study carried out in Makkah, western Saudi Arabia, found a low seasonal flu vaccination rate, with only 18.5% of people receiving the vaccine.11 Another study of military personnel in central Saudi Arabia revealed an influenza vaccine coverage rate of 17.8%.12 A person’s decision to receive the seasonal influenza vaccine depends on several factors, including beliefs and attitudes about influenza and the influenza vaccine.5,13 In Slovenia, unvaccinated people cited 2 main reasons for not getting the seasonal influenza vaccine: the perception that they were in good health and therefore did not need the vaccine, and a fear of side effects. Many of those who did get the vaccine said they felt it was important to be vaccinated by their family physicians since they had confidence in them.10 In a German study in 2010, ‘fear of side effects’ and the opinion that ‘vaccination was not necessary’ were the major reasons cited for receiving a pandemic vaccination.13 In the study carried out in Lebanon in 2015, the only factor that was found associated significantly with the abstinence form annual vaccination is ‘thinking that the vaccine was not needed’,8 while in the study carried out in Jordan, the most reported critical barrier to vaccination was the concern about the safety and efficacy of the vaccine.9 Studies exploring the factors associated with public acceptance and refusal of the seasonal influenza vaccine remain lacking in Saudi Arabia.
The aim of this study was to explore beliefs, attitudes and barriers towards uptake of the seasonal influenza vaccine among visitors to primary healthcare clinics at King Abdulaziz Medical City (KAMC), Riyadh, Saudi Arabia.
Methods
Prior to research conduction, manual search of English-language journals for similar articles regarding influenza and influenza vaccine was conducted in Medline and Google Scholar. This was a cross-sectional study conducted at 3 primary healthcare centers at KAMC between May and Oct 2017 (the Health Care Specialty Center, HCSC; King Abdulaziz Housing Clinics, Iskan; and the National Guard Comprehensive Specialized Clinic, NGCSC).
All 3 centers provide primary curative and preventive health services, and have both walk-in and booking appointment systems for patients to receive treatment and advice for acute and chronic medical conditions.
Study participants were male and female adult visitors to the centers aged 18 years and above. Exclusion criteria include illiterate people, sick patients and mentally ill patients. The sample size was calculated using Openepi, an epidemiologic calculator, based on the 18.5% uptake of the influenza vaccine found among participants of similar study by Korani. Using a 95% confidence interval and 5% margin of error, the calculated minimum sample size was estimated to be 232, which was adjusted to 300 to compensate for incomplete questionnaires.
The proportion of participants from each of the 3 centers was based on the clinic catchment area as follows: HCSC serves a population of approximately 200,000 people, thus accounts for approximately 57.1% of the sample size, equal to 171 participants; Iskan serves approximately 50,000 people, accounting for approximately 14.3% of the sample size, equal to 43 participants; and NGCSC serves approximately 100,000 people, accounting for approximately 28.6% of the sample size, equal to 86 participants.
Study data was collected using a self-administered questionnaire. The questionnaire used was developed by Korani15 (used with permission), which was modified by the investigator after a literature review of similar studies to meet the study objectives.
The questionnaire was written in simple Arabic language, and included the following sections: demographic data; questions about knowledge, attitudes and beliefs towards the seasonal influenza vaccine; and questions related to factors affecting vaccine acceptance. Two research experts reviewed the questionnaire, and a pilot study was conducted with 10 participants to verify the clarity of the tool.
Participants were recruited via a random convenient sampling method. Visitors of the 3 primary care centers were approached while sitting in the waiting area. All visitor to the 3 centers who meet the inclusion criteria and agreed to participate were included until the sample size was reached. No participants who meet the inclusion criteria and agree to participate were excluded. The investigator explained the purpose of the study to each participant and obtained verbal consent to participate before administering the questionnaire.
All data were coded, entered and analyzed using Statistical Package for the Social Sciences software, version 23 (Armonk, NY: IBM Corp.). Continuous variables were reported in terms of means and standard deviation, while categorical variables were described using frequencies and percentages. Analytic statistics were carried out using the Chi-square (x2) test for associations and/or the difference between 2 categorical variables. A p-value ≤0.05 was considered statistically significant.
Ethical considerations
Study approval was obtained from King Abdullah International Medical Research Center (KAIMRC), Ministry of National Guard, Saudi Arabia. Verbal consent was obtained from participants at the time of questionnaire distribution. Privacy and confidentiality of the data was considered, completely protected and used only for research purposes. The study was carried out according to principles of Helsinki Declaration.
Results
Three hundred people took part in the study. Among the study group, 164 (54.7%) were 30 years old or younger and 134 (44.7%) were older than 30. The mean age was 32.66±11.141 years, ranging from 18 to 75 years. One hundred and fifty-five participants (51.7%) were male, 196 (65.3%) were married, and only 45 participants (18%) had chronic disease. In terms of educational level, 162 participants (54%) had completed school-level education, and 138 (46%) had an university education. More than half of participants were working (53.3%), and of these, 44.4% had military jobs. Most study subjects had not been vaccinated against seasonal influenza (63.3%).
Participants reported that they received most of their information about the seasonal influenza vaccine from mass media (37.7%), family and friends (30%), healthcare providers (26.7%) and other sources (6.3%).
In regard to knowledge about the seasonal influenza vaccine, more than half of participants (n=162, 54%) knew how often they should receive the vaccine, 128 (42.7%) knew how the vaccine was administered, and only 73 (24.3%) knew that the influenza vaccine is appropriate for all people, particularly the elderly and those with chronic illnesses.
Approximately 60% (n=181, 60.3%) of participants knew that hospitals offer free influenza vaccinations. Most study participants were concerned about the risk of seasonal influenza infection (74.3%), and 249 (83%) said they thought the seasonal influenza vaccine was useful. Two-thirds (n=198, 66%) of participants said they intended to get the vaccination again, and 259 (68.3%) thought that greater awareness of the seasonal influenza vaccine was needed in the community (Table 1).
Table 1.
Knowledge and attitude about influenza vaccine.

Only 23 participants (7.7%) had ever experienced side effects from the influenza vaccine. The most commonly reported side effects were a slight rise in temperature (3%), sore throat (2.7%), mild redness or swelling at the vaccine site (2.3%), and minor body aches (1%).
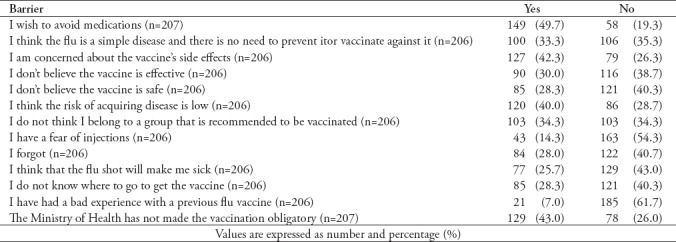
Table 2 summarizes the reported barriers to having the influenza vaccine. The most common reason to refuse the influenza vaccine was a desire to avoid medications (n=149, 49.7%). Other reported barriers included: the fact that the Ministry of Health has not made influenza vaccination obligatory (43%), concerns about the side effects of the vaccine (42.3%), the perception that patients’ are at low risk of influenza infection (40%), the belief that patients’ are in a group of the population that is not recommended to receive the vaccination (34.3%), and the belief that influenza is a simple disease that does not require prevention (33.3%). The least often cited barriers to vaccination were a fear of injection (14.3%) and a previous bad experience with a vaccination (7%).
Table 2.
Barriers to seasonal influenza vaccination.
Bivariate analysis
The results in Table 3 show the relationships between participants’ characteristics and their history of seasonal influenza vaccination. The rate of vaccination among males was statistically significantly higher than in females (p=0.050), but there was no statistically significant difference between other demographic variable and history of influenza vaccination. Participants who knew that hospitals offer free vaccinations get vaccinated more than those who did not (p=0.000). There was a statistically significant relationship between having a vaccination history and greater knowledge about the seasonal influenza vaccine (p=0.000) (Table 4). Participants with a university education knew about the recommended frequency of vaccination, and the vaccination route more often than those with a lower level of education, (p=0.001, p=0.018, respectively) (Table 5). No statistically significant difference was found between knowledge of the seasonal influenza vaccine and participants’ age, gender, marital status or employment status.
Table 3.
Relationship between participant’s characteristics and history of seasonal Influenza vaccination.

Table 4.
Relationship between history of vaccination and knowledge about Influenza vaccine.

Table 5.
Relationship between educational level and knowledge about influenza vaccine.

Results showed that participants who have previously had a influenza vaccination, and those who experienced side effects from a previous influenza vaccine, were significantly less inclined to get the vaccine again (both p=0.000). Older participants reported significantly more often than younger participants that they were concerned about seasonal influenza infection (81.3% versus 69.5%, p=0.019). Participants employed in a non-military profession were significantly more likely to trust in the effectiveness of the influenza vaccine than those in military employment (p=0.031). Otherwise, no statistically significant differences were found to correlate concern about influenza infection or beliefs about the seasonal influenza vaccine with participants’ characteristics. Females were significantly more likely to report not getting the influenza vaccination because of concerns about side effects, or because of the misconception that they are not in a population group that is recommended to get the vaccine (p=0.019 and p=0.025). Females were also more likely than males to report fear of injection as a barrier to getting the vaccination (p=0.038), as were participants with a low educational level (p=0.038). Married participants were more likely to hold the misconception that the influenza vaccine is unsafe (p=0.070), and were more likely to believe that influenza is a simple disease that does not require a vaccination (p=0.006). People employed in military professions were more likely that people in other professions to report that they did not know where to obtain a influenza vaccine (p=0.026). Participants with a history of chronic disease more often reported concerns about vaccine side effects (p=0.007).
Discussion
The aim of this study was to explore public knowledge of and attitude towards the seasonal influenza vaccine, and to understand the barriers that might prevent people from getting this vaccination. The study population comprised visitors to Family Medicine centers at 3 National Guard health facilities in Riyadh, Saudi Arabia. This community included National Guard employees, both military and nonmilitary, and their dependents.
Subgroups of participants were almost similar in number in terms of age, gender, marital and employment status, and educational level. Less than one-fifth of participants (18%) had a chronic disease such as diabetes mellitus, hypertension, asthma or hypothyroidism. This was expected, since 54.7% of all participants were younger than 30 years of age.
As found in a similar local study,11 most participants (63.3%) had never had an influenza vaccination. In fact, poor uptake of the influenza vaccine is a problem around the world, as reported in studies conducted in Lebanon,8 Jordan,9,10 and European countries.5,6,14 In our study, the rate of vaccination is insufficient to achieve a coverage that offers community-wide protection from the disease and its complications. This indicates a need for greater efforts to educate people about the vaccination, and to provide the necessary health facilitation and involvement of multidisciplinary teams to promote the seasonal influenza vaccination. This need was clearly demonstrated in this study since participants with a better knowledge of the influenza vaccine had a significantly higher rate of vaccine uptake. Participants themselves (86.6%) also reported that more public campaigns are needed to increase awareness of influenza vaccination.
The only demographic characteristic that was found to make a significant difference in vaccination rate was gender: fewer females were vaccinated than males (p=0.050). As was also reported in Makkah11 and Lebanon,8 most of the participants in our study who had a chronic disease had not received the influenza vaccine. This is surprising, since those with chronic disease are potentially more likely than medically free people to develop complications from influenza infection. They also usually visit a clinic more regularly, thus have more opportunities to receive the vaccine. Further exploration of this alarming result is required to determine whether the factors related to low uptake of the influenza vaccine in this group are patient-related, related to healthcare providers, or to the healthcare system.
Most of the participants in our study did not know that the influenza vaccine is recommended for everybody over the age of 6 months. Furthermore, almost half did not know how often the vaccine should be given, or how it was administered. This indicates poor knowledge, and was clearly reflected in our findings by the low rate of vaccine uptake. Conversely, knowledge of the influenza vaccine was considerably higher in the Jordanian population.10
As in the study by Korani,11 the participants in our study reported that they mostly obtain information about the influenza vaccine from mass media, followed by friends and family (30%) and healthcare providers (26.7%). Participants’ knowledge of the influenza vaccine is possibly influenced by the main source of information from which they learn about it; it is known that many misconceptions about the influenza vaccine are publicized, which might affect people’s knowledge of the vaccine and their attitudes towards it. Despite that almost one-third of participants said that their health care provider was their main source of information, it seems that more education is needed at this level to disseminate correct information about the influenza vaccine, and hence improve uptake. In comparison, in the Lebanese study, participants most frequently reported that their physician was their main source of information about the influenza vaccine.5 Similarly, in the Slovenian study,5 most participants said they received their information about the influenza vaccine from their family physician. It is interesting that most participants in our study said they were concerned about influenza infection and believe that the vaccine is useful to prevent it, yet the majority never get vaccinated. This can be understood in the context of possible barriers that prevent uptake despite a recognized need.
The 3 barriers most often reported as preventing people from getting the influenza vaccine were a desire to avoid medication, the fact that the Ministry of Health has not made vaccination obligatory, and a fear that the vaccine would cause side effects. Other reported barriers were the beliefs that the vaccine is ineffective and/or unsafe. In the Makkah study, most participants believed the seasonal influenza vaccine to be unsafe, and reported a fear of possible side effects.11 In the 2016 Jordanian study, concerns about the safety and efficacy of the vaccine were cited as the most critical barriers to vaccination among adults and children,9 while in Lebanon, thinking that the vaccine was not needed was the only correlate found to be significantly associated with abstinence from regular vaccination.8
In Slovenia, unvaccinated people reported 2 major reasons for not getting the seasonal influenza vaccination: the perception that they had good health and therefore did not need the vaccination, and a fear of side effects. Conversely, many vaccinated people felt it was important to be vaccinated by their family physicians since they had confidence in them.5 In a German study conducted in 2010, ‘fear of side effects’ and the opinion that ‘vaccination was not necessary’ were the 2 main reasons identified for refusing a pandemic vaccination.13
Many obstacles mean that it may not be possible for the Saudi Arabian Ministry of Health to make the influenza vaccine obligatory, but much can be carried out to correct the misconception that the influenza vaccine is unnecessary, and that it has side effects to the degree that it should be avoided. A considerable percentage of participants (28.3%) did not know where they could get the vaccine. This is a barrier that can be easily solved if appropriate arrangements were made a family medicine and primary healthcare facilities during the influenza season. For example, the vaccine could be made available in the screening room, with nurses offering it to every attending patient or patient’s relative (after ensuring no contraindication). Reported barriers to influenza vaccination differ between countries, and these differences may be associated with differences in participants’ characteristics.5,10
Participants of our study were more likely to report feeling concerned about side effects of the vaccine if they had a history of chronic disease. This may be caused by am is conception that having a chronic disease makes them more vulnerable to vaccine side effects. In fact, several studies have demonstrated that patients with chronic diseases such as diabetes mellitus and asthma need the vaccination more than others, since they might suffer more from the complications of influenza infection.15-17
Among unvaccinated participants of our study, males more frequently reported than females that they intended to get the vaccination in future. This difference might be explained by the fact that more female than male participants reported being afraid of injections and being concerned about side effects.
Study limitations
This study was geographically limited, and only included visitors to primary healthcare clinics. Therefore, it may not be possible to generalize the results. Recall bias is also possible.
In conclusion, although most participants said they were concerned about influenza infection, and believed that the influenza vaccine is effective, our study revealed low uptake of the seasonal influenza vaccine. Participants reported several barriers to the vaccine, the most common being a desire to avoid medications, the fact that the Ministry of Health has not made vaccination obligatory, and concerns about the side effects of the vaccine.
Acknowledgment
We would like to thank eScienta (www. eScienta.com) for English language editing.
Footnotes
References
- 1.Treanor JJ. Influenza viruses. In viral infections of humans. Boston (MA): Springer; 2014. pp. 455–478. [Google Scholar]
- 2.World Health Organization. Global Influenza Programme. A manual for estimating disease burden associated with seasonal influenza. [[Updated 2015; Accessed 2017 October 21]]. Available from URL: http://www.who.int/influenza/resources/publications/manual_burden_of_disease/en/
- 3.Zeitouni MO, Al Barrak AM, Al-Moamary MS, Alharbi NS, Idrees MM, Al Shimemeri AA, et al. The Saudi Thoracic Society guidelines for Influenza vaccinations. Ann Thorac Med. 2015;10:223–230. doi: 10.4103/1817-1737.167065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Grohskopf LA, Sokolow LZ, Broder KR, Walter EB, Bresee JS, Fry AM, et al. Prevention and control of seasonal influenza with vaccines: recommendations of the Advisory Committee on Immunization Practices-United States, 2017-18 influenza season. Am J Transplant. 2017;17:2970–2982. doi: 10.15585/mmwr.rr6602a1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kravoskravos A, Kračun L, Kravos K, Iljaž R. The impact of patient's sociodemographic characteristics, comorbidities and attitudes on influenza vaccination uptake in family practice settings. Slovenian Journal of Public Health. 2015;54:204–211. doi: 10.1515/sjph-2015-0029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Mereckiene J, Cotter S, Nicoll A, Lopalco P, Noori T, Weber J, et al. Venice project gatekeepers group. Seasonal influenza immunizations in Europe. Overview of recommendations and vaccination coverage for three seasons: pre-pandemic (2008/09), pandemic (2009/10) and post-pandemic (2010/11) Euro Surveill. 2014;19:20780. doi: 10.2807/1560-7917.es2014.19.16.20780. [DOI] [PubMed] [Google Scholar]
- 7.World Health Organization. Global Influenza Programme. Seasonal influenza vaccine use in low and middle income countries in the tropics and sub tropics. A Systematic Review. [[Updated 2015; Accessed 2017 October 21]]. Available from URL: http:// www.who.int/influenza/resources/publications/9789241565097/en/
- 8.El Khoury G, Salameh P. Attitude and practices among the Lebanese adult population. Int J Environ Res Public Health. 2015;12:15486–15497. doi: 10.3390/ijerph121215000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Abu-Rish EY, Elayeh ER, Mousa LA, Butanji YK, Albsoul-Younes AM. Knowledge awareness and practices towards seasonal Influenza and its vaccine: implications for future vaccination campaigns in Jordan. Fam Pract. 2016;33:690–697. doi: 10.1093/fampra/cmw086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Assaf AM, Hammad EA, Haddadin RN. Influenza Vaccination Coverage Rates, Knowledge, Attitudes, and Beliefs in Jordan: A Comprehensive Study. Viral Immunol. 2016;29:516–525. doi: 10.1089/vim.2015.0135. [DOI] [PubMed] [Google Scholar]
- 11.Korani MF. Assessment of seasonal flu immunization status among adult patients visiting al-Sharaee Primary Health Care Center in Makkahal-Mokarramah. Int J Med Sci Public Health. 2015;4:117–123. [Google Scholar]
- 12.Al-Khashan HI, Selim MA, Mishriky AM, Binsaeed AA. Meningitis and seasonal Influenza vaccination coverage among military personnel in central Saudi Arabia. Saudi Med J. 2011;32:159–165. [PubMed] [Google Scholar]
- 13.Bödeker B, Remschmidt C, Schmich P, Wichmann O. Why are older adults and individuals with underlying chronic diseases in Germany not vaccinated against flu?A population-based study. BMC Public Health. 2015;15:618. doi: 10.1186/s12889-015-1970-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Giese C, Mereckiene J, Danis K, O'Donnell J, O'Flanagan D, Cotter S. Low vaccination coverage for seasonal influenza and pneumococcal disease among adults at-risk and health care workers in Ireland, 2013: The key role of GPs in recommending vaccination. Vaccine. 2016;34:3657–3662. doi: 10.1016/j.vaccine.2016.05.028. [DOI] [PubMed] [Google Scholar]
- 15.Wang IK, Lin CL, Chang YC, Lin PC, Liang CC, Liu YL, et al. Effectiveness of influenza vaccination in elderly diabetic patients: a retrospective cohort study. Vaccine. 2013;31:718–724. doi: 10.1016/j.vaccine.2012.11.017. [DOI] [PubMed] [Google Scholar]
- 16.Moghadam MD. A new discussion for “effects of annual influenza vaccination on mortality and hospitalization in elderly patients with ischemic heart disease: a nationwide population-based study”. Prev Med. 2013;56:163. doi: 10.1016/j.ypmed.2012.12.006. [DOI] [PubMed] [Google Scholar]
- 17.Lee WJ, Chen LK, Tang GJ, Lan TY. The impact of influenza vaccination on hospitalizations and mortality among frail older people. Journal of the American Medical Directors Association. 2014;15:256–260. doi: 10.1016/j.jamda.2013.12.003. [DOI] [PubMed] [Google Scholar]