

Abstract
Objectives:
To provide an overview of the extent of hyperlipidemia in very high-risk patients, and how lipid-lowering therapy (LLT) is used in a real-world setting.
Methods:
In this multicenter observational study, data were collected from LLT-treated patients with stable CHD or an ACS in Saudi Arabia between 2013 and 2014. Individuals were included if they were >18 years and had a full lipid profile available, recorded either prior to the baseline physician visit (CHD patients) or within 24-hours of admission to hospital (ACS patients).
Results:
A total of 737 patients were included in the study, 597 with stable CHD and 140 with ACS. Few patients in either group had an LDL-C level of <70 mg/dl, which is advocated for very high-risk patients (24.3% and 11.4%, respectively). The median distances to this value were 19.0 mg/dl (CHD) and 25.0 mg/dl (ACS). Low doses of statins were being utilized (31 and 24 mg/day for CHD and ACS, respectively), with only minimal intensification for the ACS patients after hospital admission (41 mg/day at follow-up).
Conclusions:
Achievement of recommended LDL-C levels was poor for patients with stable CHD or an ACS. Statin intensity was low, indicating huge scope for intensifying the treatment of these very high-risk patients.
It is well-established that patients with coronary heart disease (CHD) are at very high risk for experiencing an adverse cardiovascular event. Such risk can be reduced by careful management of associated risk factors, including hypertension, diabetes mellitus, and dyslipidemia.1,2 Lipid abnormalities, such as high levels of low-density lipoprotein cholesterol (LDL-C) or triglycerides, and low levels of high-density lipoprotein cholesterol (HDL-C), are known to be highly prevalent in patients with CHD.3 Indeed, in a recent study of CHD patients in Saudi Arabia, 76.7% were found to have dyslipidemia.4 The benefits of reducing LDL-C levels in particular have been extensively studied in the context of decreasing the occurrence of cardiovascular events. Indeed, it has been shown that a reduction in LDL-C of approximately 39 mg/dl (1 mmol/l) could decrease the 5-year rate of major vascular events by approximately a fifth.
Evidence-based guidelines for the treatment of dyslipidemia from the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS) advocate a target LDL-C level of <70 mg/dl (1.81 mmol/l) for patients at very high cardiovascular risk, such as those with established CHD.5 Lipid-lowering therapies (LLTs) such as statins have been shown to effectively reduce levels of LDL-C; however, despite their widespread use, significant numbers of high risk CHD patients fail to achieve target levels. In the Middle Eastern cohort of the first Dyslipidemia International Study (DYSIS), only 30.5% of the statin-treated group at highest cardiovascular risk had an LDL-C level below 70 mg/dl.6 Results from the Arabian Gulf countries included in the Centralized pan-Middle East Survey on the Undertreatment of Hypercholesterolemia (CEPHEUS) showed 31.9% achievement of the same LDL-C target for the very high-risk patients being treated with LLT.7 The EUROASPIRE studies have demonstrated increasing statin use in patients with CHD over the last decades; however, in their most recent analysis, only 19.5% of patients had an LDL-C level below 70 mg/dl.8 In a single-center study in Saudi Arabia, few CHD patients had a recent lipid profile recorded in their medical notes, indicating poor monitoring of hyperlipidemia in these high-risk patients.9
In order to obtain details on the management of cholesterol in patients with CHD, and to evaluate current treatment practices, DYSIS II was initiated.10 This was a multinational, observational study investigating lipid abnormalities in patients with either stable CHD or presenting with an acute coronary syndrome (ACS). With the use of standardized methodology, the prevalence of lipid abnormalities, and predictors of LDL-C target attainment, was evaluated in patients from countries throughout the world. Here, we present the results collected in Saudi Arabia, providing an overview of the extent of hyperlipidemia in these very high-risk patients, and how LLT is used in a real-world setting.
Methods
Patients were enrolled at 4 centers within Saudi Arabia from December 2013 to October 2014. Individuals with either stable CHD or those admitted to the hospital with an ACS were included if they were over 18 years of age and had a full lipid profile available. Acute coronary syndrome was defined as an ST-segment elevation myocardial infarction (STEMI)/left bundle branch block myocardial infarction (LBBB MI), non-ST-segment elevation myocardial infarction (NSTEMI), or unstable angina (UA) at the time of hospital admission. For patients with CHD, the lipid profile was obtained from the last blood test within the 12 months prior to the baseline physician visit; for patients with an ACS, the lipid profile was recorded within 24 hours of admission to the hospital. Patients were included in the present analysis if they had been receiving LLT for at least 3 months prior to the latest lipid test. Patients were excluded if they were participating in a clinical trial at the same time as the study, and for the ACS patients, if they died during the hospital stay. For CHD patients, data were collected at the baseline physician visit. For ACS patients, data were collected on admission to the hospital and at 4 months (±15 days) post-admission.
All included patients provided written informed consent. The study received ethical approval from the relevant national and regional committees at each participating center, and was carried out in accordance with the Declaration of Helsinki and its amendments.
Data were recorded on a standardized case report form (CRF) and later entered into a central web-based database maintained at the Institut für Herzinfarktforschung, Ludwigshafen, Germany.
Demographic and clinical variables were collected at baseline, including age, gender, and body mass index (BMI); presence of hypertension or type 2 diabetes mellitus; a sedentary lifestyle or smoking; a history of CHD, peripheral artery disease (PAD), chronic renal failure (CRF), or chronic kidney disease (CKD); a prior MI or stroke (ischemic or hemorrhagic); and any family history of CHD. Obesity was defined as BMI >30 kg/m2. Diabetes was defined as current treatment for diabetes, a previous diagnosis of diabetes, or a fasting plasma glucose level of ≥126 mg/dl. Hypertension was defined as current treatment, a previous diagnosis, or having blood pressure of >140/90 mm Hg. A sedentary lifestyle was defined as <20-30 minutes of walking on <3-4 days per week. Use of cardiovascular medications (beta-blockers, calcium channel blockers, diuretics, ACE inhibitors, antiplatelet agents) and laboratory values of HbA1c and blood glucose at admission were also documented. A full lipid profile, which included measurement of serum levels of total cholesterol (TC), LDL-C, HDL-C, non-HDL-C, and triglycerides was recorded at baseline. For the ACS patients, any further lipid profiles available from the follow-up period were also collected.
For ACS patients, pre-ACS cardiovascular risk status was determined according to the ESC/EAS guidelines, and targets for LDL-C for very high-risk patients were defined as <70 mg/dL, high-risk <100 mg/dL, moderate-risk <115 mg/dL, and low-risk <130 mg/dL.5 As shown in the guidelines, very high- and high-risk patient groups have clearly set target values based on comorbidity, while additional risk factors or markers such as obesity or high C-reactive protein (CRP) are taken into account for moderate and low cardiovascular risk. Low-density lipoprotein cholesterol goal attainment was judged based on lipid values at admission, reflecting the pre-admission lipid levels. The median distance to the LDL-C target was calculated for patients who had not attained this level on the date of the lipid profile.
Details of the LLT that each patient was being treated were documented. The following classes of LLT were assessed: statin monotherapy, non-statin monotherapy, statin plus ezetimibe, and statin plus other non-statin therapy (other non-statins included nicotinic acids, fibrates, omega-3 fatty acids, and other less common agents). The statins assessed were atorvastatin, fluvastatin, lovastatin, pravastatin, pitavastatin, rosuvastatin, and simvastatin. Atorvastatin dose equivalents were based on clinical trial data regarding the LDL-C-lowering efficacy of various statins.
For ACS patients, at 4 months (±15 days) post-admission, any lipid profiles obtained since hospital discharge were collected. The median distance to the LDL-C target was calculated for patients who had not attained the LDL-C target on the date of the lipid profile. Any occurrence of cardiovascular-related adverse events (rehospitalization, MI, stroke, percutaneous coronary intervention [PCI], or coronary artery bypass grafting [CABG]) during the follow-up period was recorded. These outcomes were not mutually exclusive.
Statistics analysis
Data are presented as means with standard deviations (SD), medians with interquartile ranges (IQR), or absolute values with percentages. Statistical significance was determined using the Chi-squared test or the Mann-Whitney-Wilcoxon test.
Multivariate logistic regression was conducted in order to identify any predictors of a patient having an LDL-C level below 70 mg/dl. The covariates were age, female gender, obesity, current smoking, sedentary lifestyle, stable angina, CKD, type 2 diabetes mellitus, history of congestive heart failure [CHF], hypertension, and statin dose [atorvastatin dose equivalent]).
Data were analyzed using SAS version 9.3 (Cary, NC, USA) and a p-value <0.05 was considered statistically significant.
Results
Five hundred and ninety-seven LLT-treated patients with stable CHD were recruited (Table 1). The mean age of these subjects was 62.5 (±9.8) years and 79.2% were male. Obesity was recorded for 58.8% of the population. Other cardiovascular risk factors included current smoking (16.8%), a sedentary lifestyle (69.4%), and a family history of CHD (21.6%). Hypertension was highly prevalent, being found in 76.5% of patients. Greater than 50% stenosis was observed by coronary angiography for 45.4% of patients, and by cardiac computed tomography for 1.2%. A total of 39.5% of patients had previously undergone PCI, 20.9% had undergone CABG, and 7.2% had experienced an ACS >3 months prior to the physician visit.
Table 1.
Characteristics at baseline of 140 lipid-lowering therapies-treated patients admitted to the hospital with an ACS.
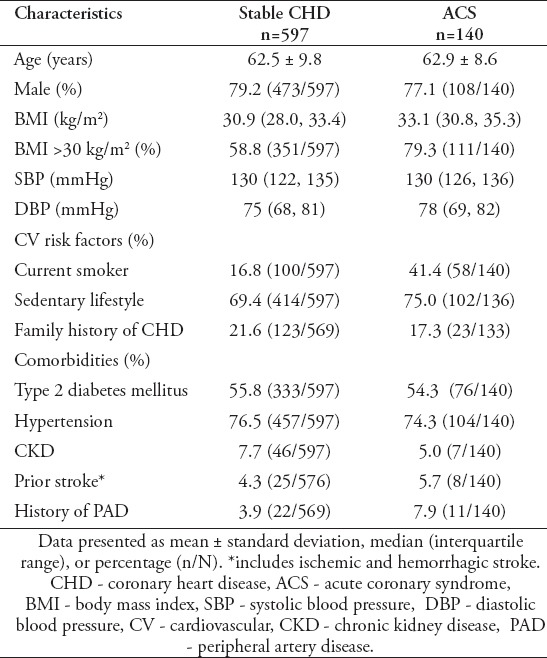
One hundred and forty LLT-treated patients admitted to the hospital with an ACS were enrolled in the study (Table 1). The mean age of these subjects was 62.9 (±8.6) years and 77.1% were male. Obesity was recorded for 79.3% of the population. A high proportion (75%) reported a sedentary lifestyle, while current smoking (41.4%) and a family history of CHD (17.3%) were also common. The majority of patients had hypertension (74.3%), and many had type 2 diabetes mellitus (54.3%). The primary ACS diagnosis was STEMI for 65% of patients and a NSTEMI for 16.4%. The remaining patients (18.6%) were diagnosed with UA.
Lipid profile at time of latest lipid test
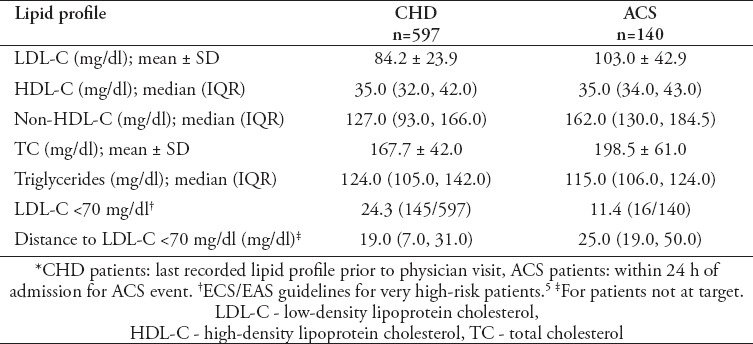
For the CHD patients, the mean LDL-C level was 84.2 (±23.9) mg/dl, with only 24.3% having a value below the ESC/EAS target of 70 mg/dl (Table 2).
Table 2.
Baseline lipid profile of both cohort of ACS and CHD enrolled in hyperlipidemia in Saudi Arabia study.
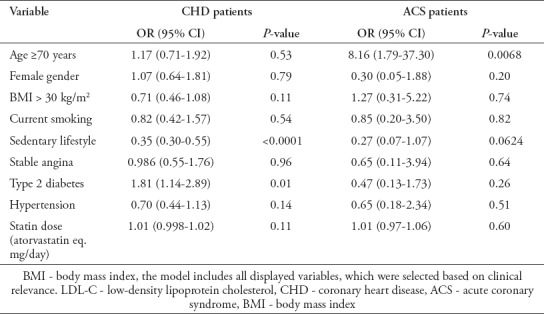
Multivariate logistic regression identified type 2 diabetes mellitus as being predictive of achieving an LDL-C level of <70 mg/dl (adjusted odds ratio (AOR): 1.81; 95% confidence interval (CI): 1.14-2.89; p=0.01), while a sedentary lifestyle (AOR: 0.35; 95% CI: 0.30-0.55, p<0.0001) lowered the likelihood of target value attainment (Table 3).
Table 3.
Multiple logistic regression model for an LDL level of <70 mg/dl at baseline in both cohort of ACS and CHD enrolled in hyperlipidemia in Saudi Arabia study.
For the ACS patients, 11.1% (15/135) of those at very high risk and 50% (1/2) of those at high risk, but none of those at moderate risk (0/3), according to pre-ACS risk level, were at their respective LDL-C target at hospital admission. As per the ESC/EAS guidelines, all patients were classed as being at very high risk on admission, owing to their presentation with an ACS.5 The mean LDL-C value for the ACS patients, measured within 24 hours of admission, was 103 (±42.9) mg/dl (Table 2).
Only 11.4% of this population had an LDL-C level of <70 mg/dl. The median distance to this value was 25.0 (19.0, 50.0) mg/dl. The median HDL-C level was 35.0 (34.0, 43.0) mg/dl, the median non-HDL-C level was 162.0 (130.0, 184.5) mg/dl, the mean TC level was 198.5 (±61.0) mg/dl, and the median triglyceride level was 115.0 (106.0, 124.0) mg/dl. Multivariate logistic regression using data collected at hospital admission, found that an age equal or greater to 70 years was associated with an increased likelihood of having an LDL-C level of <70 mg/dl (AOR: 8.16; 95% CI 1.79-37.30; p=0.0068) (Table 3).
During the 4-month follow-up period, a lipid profile was collected for 21 of the patients. Of these, none had an LDL-C level of <70 mg/dl at admission and one (4.8%) had reached this target by the follow-up point.
Lipid-lowering therapy
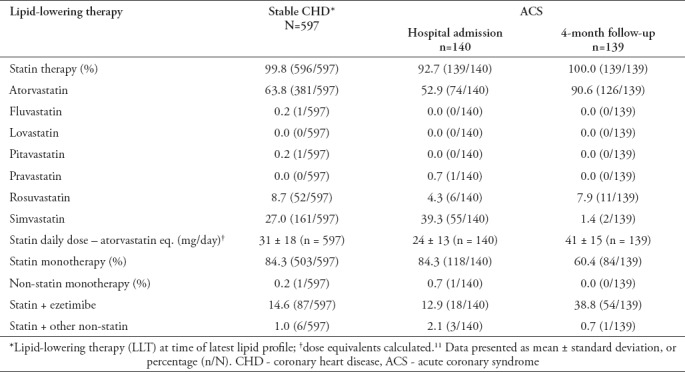
Of the stable CHD patients, 84.3% were on statin monotherapy, while 14.6% were on a combination of a statin and ezetimibe, and 1% on a combination of a statin and other non-statin (Table 4). Atorvastatin was the most commonly used statin (63.8%), followed by simvastatin (27%), and rosuvastatin (8.7%). When statin potency was normalized to Atorvastatin, the mean daily dosage was calculated to be 31 ± 18 mg. Of the ACS patients, 84.3% were on statin monotherapy, 12.9% were on a combination of a statin and ezetimibe, and 2.1% on a combination of a statin and other non-statin. Atorvastatin was the most commonly used statin (52.9%), followed by simvastatin (39.3%), and rosuvastatin (4.3%). The mean atorvastatin equivalent daily dosage was 24 ± 13 mg. At the 4-month follow-up point, 60.4% of the ACS patients were on statin monotherapy, while 38.8% were on a combination of statin and ezetimibe. The prescription patterns of the different statins differed from baseline, with a higher proportion of patients receiving Atorvastatin (52.9% versus 90.6%) and a lower proportion receiving simvastatin (39.3% versus 1.4%). The mean Atorvastatin equivalent daily statin dosage had increased from 24 ± 13 mg at admission to 41 ± 15 mg at 4 months.
Table 4.
Lipid-lowering therapy at baseline in both cohort of ACS and CHD enrolled in hyperlipidemia in Saudi Arabia study.
Events during follow-up for ACS patients
None of the ACS patients died during the 4-month follow-up period. There was no occurrence of MI or stroke, and no patients underwent PCI or CABG. Only 2 of the patients that were treated with LLT prior to admission required rehospitalization. There was no increased untoward effects reported with the increase of the statin dose over time.
Discussion
Dyslipidemia International Study II was established in order to specifically address hyperlipidemia in patients with either stable CHD or ACS, and to evaluate their treatment. Patients from Saudi Arabia, a country with alarming prevalence of cardiovascular risk factors, attainment of an LDL-C level of <70 mg/dl was poor. Furthermore, for the patients admitted to the hospital because of an ACS, LLT intensification was inadequate.
As in the rest of the world, hyperlipidemia is becoming more prevalent in Saudi Arabia as the average age and income of the population increase.12 In DYSIS, it was shown that only 26.4% of Saudi patients classed as being at very high cardiovascular risk had an LDL-C level of <70 mg/dl, despite being treated with statins.13 A high level of under-treatment of these patients was indicated, a finding that was also reported for the Arabian Gulf cohort of CEPHEUS.7
Comorbidities and cardiovascular risk factors were highly prevalent in both the patients with stable CHD and those admitted to the hospital for ACS. Obesity was extremely common, in particular for the ACS patients (79.3%). In comparison to the DYSIS II data for the Middle East and Africa region combined (Manuscript in preparation), almost 30% of the ACS patients from Saudi Arabia were classed as obese. This is in agreement with data presented by Yatsuya et al14 where Saudi Arabia was shown to have one of the highest levels of overweight and obesity in the East Mediterranean region. A sedentary lifestyle was also common (69.4% and 75% of LLT-treated CHD and ACS patients, respectively), as was smoking (16.8% and 41.4%, respectively), suggesting that better patient education would be beneficial for improving these modifiable risk factors.15 Similar to previous studies in patients at high cardiovascular risk, hypertension and diabetes mellitus were noted for large proportions of patients.4,7,8
For the CHD patients, less than a quarter (24.3%) attained LDL-C <70 mg/dl, despite the finding of a relatively low mean LDL-C value in comparison to the average values quoted in other studies.4,7 Poor LDL-C target attainment was also reported for the very high risk LLT-treated patients in the Middle East cohort of DYSIS and the Arabian Gulf countries included in CEPHEUS, with 30.5% and 31.9% of these patients, respectively, achieving a level of <70 mg/dl.6,7 We found that the distance to target for those not at goal was quite small, indicating that even small reductions in LDL-C levels would greatly increase target attainment. This is corroborated by the high proportion of CHD patients (68%) achieving a level of <100 mg/dl in a previous study in Saudi Arabia.9 After multivariable analysis, the only factors that were found to be associated with an LDL-C level below 70 mg/dl were a sedentary lifestyle, which decreased the likelihood, and type 2 diabetes, which increased the likelihood. In CEPHEUS, Arafah et al7 also identified a history of diabetes as being predictive of target achievement. A potential explanation for this finding is that patients with diabetes may be more aware of the seriousness of their health situation and so might be more adherent to pharmacological therapy and lifestyle improvements. Furthermore, they would be likely to have greater contact with physicians (cardiologists and endocrinologists). Al Shammeri et al9 found that a high proportion of the stable CHD patients included in their study did not have a recent LDL-C level documented in their medical notes. It therefore appears that increased attention to lipid testing may have a positive effect on target attainment in CHD patients.
Low-density lipoprotein cholesteroltarget attainment according to pre-ACS risk level was extremely poor for the ACS patients, reaching just over 11% for those at very high risk. In contrast to the patients with stable CHD, the only factor included in the multivariable analysis that was found to be associated with ACS patients displaying an LDL-C level of <70 mg/dl at admission was an age of 70 years or above.
The low levels of target achievement suggest highly ineffective use of LLT in these very high risk patients. While all subjects were being treated with LLT, the mean atorvastatin equivalent daily dose was only 31 mg for the stable CHD patients and 24 mg for the ACS patients at admission. While the dosage by the 4-month follow-up point had increased to 41 mg for the ACS patients, this is still only a medium intensity. Nicholls et al16 reported significant coronary plaque regression when intensive Atorvastatin (80 mg/day) or rosuvastatin (40 mg/day) therapy was prescribed to patients with CHD.16 Furthermore, in the Pravastatin or Atorvastatin Evaluation and Intensive Therapy-Thrombolysis in Myocardial Infarction-22 (PROVE IT–TIMI 22), patients with an ACS who were treated with intensive statin therapy were found to have a lower likelihood of death or a major cardiovascular event in comparison to the patients that received standard therapy.17 Similar advantages of intensive LLT were found in the GWTG database and the Translational Research Investigating Underlying Disparities in Acute Myocardial Infarction Patients’ Health Status (TRIUMPH) study.18 A number of other trials have also demonstrated advantages in terms of lipid-lowering and occurrence of cardiovascular adverse events when more intensive statin treatment is prescribed.19 The majority of these studies utilized an Atorvastatin dose of 80 mg as the intensive arm, which highlights the low average doses used for the patients in the present analysis. In the Middle Eastern CEPHEUS patients, although exact normalized statin doses were not reported, the majority of patients were being treated with the equivalent of ≤30 mg of atorvastatin per day.7 In DYSIS, which was carried out in 2011-2012, the most commonly prescribed statin dose for the very high risk patients in the Middle East countries was equivalent to 20 mg per day.6 The increase in statin dose from DYSIS to DYSIS II may indicate improvement in the way in which these drugs are used for managing LDL-C levels in CHD patients in Saudi Arabia; however, there is clearly room for treatment intensification, in particular for patients who have experienced an ACS.
The addition of a non-statin agent to statin monotherapy is an alternative method to intensify LLT for very high risk patients. In the Improved Reduction of Outcomes: Vytorin Efficacy International Trial (IMPROVE-IT), it was shown that, in patients that had suffered an ACS, LDL-C levels were reduced to a greater extent with the use of ezetimibe in combination with simvastatin (93.8 mg/dl to 53.7 mg/dl during the trial) than with simvastatin alone (93.8 mg/dl to 69.5 mg/dl during the study).20 The study also demonstrated a 2% lower rate of the primary endpoint (cardiovascular death, non-fatal MI, UA requiring hospitalization, coronary revascularization, or non-fatal stroke) achievement for the patients receiving combination therapy. In addition, increased plaque regression has been demonstrated for combination therapy (ezetimibe plus rosuvastatin) in comparison to statin monotherapy (rosuvastatin alone) in patients with CHD.21,22 In the present study, ezetimibe use was relatively uncommon at baseline (14.5% and 12.9% for CHD and ACS patients, respectively); however, by the 4-month follow-up point, 38.8% of the ACS patients were being treated with this agent. Interestingly, this is much higher than the proportions of patients in other Middle Eastern countries that participated in DYSIS II (Manuscripts in preparation). Such evidence of treatment intensification is promising, but there remains a discrepancy between optimal therapy and that used in the real-world.
One limitation to this analysis is the low number of ACS patients with a full lipid profile collected during the acute phase and the follow-up period. This prevents us from also establishing a true picture of the effects of changes that were made to the LLT after admission. Furthermore, no adverse cardiovascular events were recorded for the ACS patients during the relatively short follow-up period, and such events were not monitored in the patients with stable CHD. This prevents us from evaluating the associations between lipid levels, LLT, and long-term cardiovascular outcome.
In conclusions, despite the known benefits of achieving a low level of LDL-C, few patients had reached the recommended target for individuals with CHD. While all patients were being treated with LLT prior to enrolment in the study, the mean daily dosage was low. Treatment was intensified for the patients who were admitted to hospital owing to an ACS; however, the statin dosages remained low. The data indicate that there is a huge scope for improving the treatment of hyperlipidemia in high-risk patients in Saudi Arabia.
Acknowledgment
Authors would like to acknowledge the following DYSIS II investigators from Saudi Arabia: Saleem Al Suwaidan and Mohammed Al Hag (King Faisal National Guard Hospital, Riyadh); Mohammed B. Jajah, Innam ul Haq, and Mohammed M. Ali Haj (Al Hada Military Hospital, Taif); Abdallah M. Abu ElSukar and Pardip Nair (Saad Specialist Hospital, Khobar); and Aneela Hussain, Mohamed Shafiq, and Hussam Jnaid (King Faisal Specialist Hospital and Research Centre, Riyadh). We would like to acknowledge Katherine Smith (IPPMed, Cloppenburg, Germany) for English language editing.
Footnotes
References
- 1.Anderson TJ, Gregoire J, Hegele RA, Couture P, Mancini GB, McPherson R, et al. 2012 update of the Canadian Cardiovascular Society guidelines for the diagnosis and treatment of dyslipidemia for the prevention of cardiovascular disease in the adult. Can J Cardiol. 2013;29:151–167. doi: 10.1016/j.cjca.2012.11.032. [DOI] [PubMed] [Google Scholar]
- 2.Naito R, Kasai T. Coronary artery disease in type 2 diabetes mellitus: Recent treatment strategies and future perspectives. World J Cardiol. 2015;7:119–124. doi: 10.4330/wjc.v7.i3.119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Catapano AL, Ference BA. IMPROVE-IT and genetics reaffirm the causal role of LDL in Cardiovascular Disease. Atherosclerosis. 2015;241:498–501. doi: 10.1016/j.atherosclerosis.2015.06.008. [DOI] [PubMed] [Google Scholar]
- 4.Al-Shehri AM. Prevalence and pattern of lipid disorders in Saudi patients with angiographically documented coronary artery disease. J Family Community Med. 2014;21:166–169. doi: 10.4103/2230-8229.142970. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.European Association for Cardiovascular Prevention & Rehabilitation. Reiner Z, Catapano AL, De Backer G, Graham I, Taskinen MR, et al. ESC/EAS Guidelines for the management of dyslipidaemias: the Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS) Eur Heart J. 2011;32:1769–1818. doi: 10.1093/eurheartj/ehr158. [DOI] [PubMed] [Google Scholar]
- 6.Al Sifri SN, Almahmeed W, Azar S, Okkeh O, Bramlage P, Junger C, et al. Results of the Dyslipidemia International Study (DYSIS)-Middle East: clinical perspective on the prevalence and characteristics of lipid abnormalities in the setting of chronic statin treatment. PLoS One. 2014;9:e84350. doi: 10.1371/journal.pone.0084350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Arafah M, Al-Hinai AT, Al Mahmeed W, Al-Rasadi K, Al Tamimi O, Al Herz S, et al. Centralized pan-Middle East Survey on the undertreatment of hypercholesterolemia: results from the CEPHEUS study in Arabian Gulf countries. Angiology. 2014;65:919–926. doi: 10.1177/0003319713512414. [DOI] [PubMed] [Google Scholar]
- 8.Kotseva K, Wood D, De Bacquer D, De Backer G, Ryden L, Jennings C, et al. EUROASPIRE IV: A European Society of Cardiology survey on the lifestyle, risk factor and therapeutic management of coronary patients from 24 European countries. Eur J Prev Cardiol. 2016;23:636–648. doi: 10.1177/2047487315569401. [DOI] [PubMed] [Google Scholar]
- 9.Al Shammeri O, Stafford RS, Alzenaidi A, Al-Hutaly B, Abdulmonem A. Quality of medical management in coronary artery disease. Ann Saudi Med. 2014;34:488–493. doi: 10.5144/0256-4947.2014.488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Gitt AK, Lautsch D, Ferrieres J, De Ferrari GM, Vyas A, Baxter CA, et al. Cholesterol target value attainment and lipid-lowering therapy in patients with stable or acute coronary heart disease: Results from the Dyslipidemia International Study II. Atherosclerosis. 2017;266:158–166. doi: 10.1016/j.atherosclerosis.2017.08.013. [DOI] [PubMed] [Google Scholar]
- 11.Roberts WC. The rule of 5 and the rule of 7 in lipid-lowering by statin drugs. Am J Cardiol. 1997;80:106–107. [PubMed] [Google Scholar]
- 12.Al-Nozha MM, Arafah MR, Al-Maatouq MA, Khalil MZ, Khan NB, Al-Marzouki K, et al. Hyperlipidemia in Saudi Arabia. Saudi Med J. 2008;29:282–287. [PubMed] [Google Scholar]
- 13.Gitt AK, Lautsch D, Ferrieres J, Kastelein J, Drexel H, Horack M, et al. Low-density lipoprotein cholesterol in a global cohort of 57,885 statin-treated patients. Atherosclerosis. 2016;255:200–209. doi: 10.1016/j.atherosclerosis.2016.09.004. [DOI] [PubMed] [Google Scholar]
- 14.Yatsuya H, Li Y, Hilawe EH, Ota A, Wang C, Chiang C, et al. Global trend in overweight and obesity and its association with cardiovascular disease incidence. Circ J. 2014;78:2807–2818. doi: 10.1253/circj.cj-14-0850. [DOI] [PubMed] [Google Scholar]
- 15.Midhet FM, Sharaf FK. Impact of health education on lifestyles in central Saudi Arabia. Saudi Med J. 2011;32:71–76. [PubMed] [Google Scholar]
- 16.Nicholls SJ, Ballantyne CM, Barter PJ, Chapman MJ, Erbel RM, Libby P, et al. Effect of two intensive statin regimens on progression of coronary disease. N Engl J Med. 2011;365:2078–2087. doi: 10.1056/NEJMoa1110874. [DOI] [PubMed] [Google Scholar]
- 17.Cannon CP, Braunwald E, McCabe CH, Rader DJ, Rouleau JL, Belder R, et al. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med. 2004;350:1495–1504. doi: 10.1056/NEJMoa040583. [DOI] [PubMed] [Google Scholar]
- 18.Arnold SV, Kosiborod M, Tang F, Zhao Z, Maddox TM, McCollam PL, et al. Patterns of statin initiation, intensification, and maximization among patients hospitalized with an acute myocardial infarction. Circulation. 2014;129:1303–1309. doi: 10.1161/CIRCULATIONAHA.113.003589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Cannon CP, Steinberg BA, Murphy SA, Mega JL, Braunwald E. Meta-analysis of cardiovascular outcomes trials comparing intensive versus moderate statin therapy. J Am Coll Cardiol. 2006;48:438–445. doi: 10.1016/j.jacc.2006.04.070. [DOI] [PubMed] [Google Scholar]
- 20.Cannon CP, Blazing MA, Giugliano RP, McCagg A, White JA, Theroux P, et al. Ezetimibe added to statin therapy after acute coronary syndromes. N Engl J Med. 2015;372:2387–297. doi: 10.1056/NEJMoa1410489. [DOI] [PubMed] [Google Scholar]
- 21.Masuda J, Tanigawa T, Yamada T, Nishimura Y, Sasou T, Nakata T, et al. Effect of combination therapy of ezetimibe and rosuvastatin on regression of coronary atherosclerosis in patients with coronary artery disease. Int Heart J. 2015;56:278–285. doi: 10.1536/ihj.14-311. [DOI] [PubMed] [Google Scholar]
- 22.Wang X, Zhao X, Li L, Yao H, Jiang Y, Zhang J. Effects of combination of ezetimibe and rosuvastatin on coronary artery plaque in patients with coronary heart disease. Heart Lung Circ. 2016;25:459–465. doi: 10.1016/j.hlc.2015.10.012. [DOI] [PubMed] [Google Scholar]