

Abstract
Objectives:
To investigate the role of serum anti müllerian hormone (AMH) pre-chemotherapy treatment levels in prediction of post-chemotherapy effect on the ovarian reserve of women with breast cancer.
Methods:
This cohort prospective study was carried out at the Biochemistry Department, College of Medicine, University of Baghdad and at the Oncology Clinic, Oncology Teaching Hospital, Baghdad, Iraq. It included 58 women with regular menstrual cycle (25-45 years) who were newly diagnosed with breast cancer. The women were classified into 3 groups: GI: 30 women with breast cancer before starting chemotherapy, GII: the same 30 women of GI who finished 4 cycles of anthracycline chemotherapy (course 1) and GIII: which involved another 28 women who had finished both courses of chemotherapy, (course 1) and (course 2).
Results:
The mean (±SEM) value of AMH levels was significantly decreased in GII and GIII when compared with GI (for both, p<0.0005). However, there was no significant difference in serum AMH levels between GII and GIII.
Conclusion:
The measurement of serum AMH may be a useful biochemical marker of the chemotherapy extent induced ovarian reserve damage and the incidence of amenorrhea.
Breast cancer (BC) is the most frequent cancer in women worldwide, forming 23% of all cancer cases in women. Today, it has become the most common cancer both in developed and developing countries.1 Jemal et al noted that BC occurs at a rate of 25% before menopause and 15% during the reproductive age. It is the main cause of cancer-related deaths.2 In Iraq, breast cancer is the most common type of malignancy. It accounts for approximately one-third of the recorded female cancers.3 Adjuvant chemotherapy (CT) is important for increasing the survival rate and assists in permanent healing, but can also produce many side effects which may continue even after finishing the CT. The main side effect of CT which forms a particular concern for young women is the suppression of ovarian function and reserve. This can lead to infertility and increase the risks of premature menopause.4 Anti-mullerian hormone (AMH) is a homodimeric glycoprotein, a member of the transforming growth factor-beta (TGF-β) super family, with its molecular weight being 140 K Da. Anti-mullerian hormone is important for the development and maturation of follicles and is generated in the pre-antral and antral follicles of ovaries by the surrounding granulosa cells.5
Van Disseldorp et al6 submitted that using a single measurement of AMH may be a highly suitable predictor for measuring odds ratio (OR) and determining women’s starting age of menopause. Fertility rates depend on the levels of AMH; good fertility rates have higher levels of AMH. Anti-mullerian hormone is a relevant tool for OR assessment and follow-up during and after treatment of women with breast cancer.7
Methods
This cohort prospective study was carried out at the Biochemistry Department, College of Medicine, University of Baghdad and at the Oncology Clinic at the Oncology Teaching Hospital, Baghdad, Iraq, between September 2016 and February 2017. It included 58 women who were diagnosed by the Oncology group to have had newly breast cancer, aged range was 25-45 years. All included women that had regular menstrual cycle. These women were divided into 3 groups: group I (GI): 30 women newly diagnosed with breast cancer before starting CT, group II (GII): the same 30 women of GI who had finished 4 cycles of anthracycline and cyclophosphamide CT (course 1), and group III (GIII): another 28 women who finished both courses of CT, including (course 1) and 4 cycles of taxanes (course 2).
The stages of breast cancer of the studied women were between stage 1-3. All metastasized tumors were excluded. Formal consent were taken from each patient. We received ethical approval from the Scientific Committee of the Biochemistry Department, College of Medicine, University of Baghdad, Baghdad, Iraq. Five milliliters of peripheral venous blood was aspirated from each studied woman on day 2-4 of their menstrual cycle. The sample blood was transferred into a plain test tube and allowed to clot for 20-30 minutes, followed by centrifugation at 2500 rpm for 10-15 minutes. The separated serum was stored at -20°C until the day of assay. Investigation included serum measurements of AMH.8 Serum luteinizing hormone (LH), estradiol 17-β (E2), and prolactin were measured using Enzyme Linked Immunosorbent Assay (ELISA) technique according to the reported methods.9 All material kits for the measured parameters were provided from Human GmbH.65205 Wiesbaden, Germany. The ELISA study was performed using Biotek instrument Highland Park, USA.
The Statistical Package for Social Sciences Version 21 (IBM Corp., Armonk, NY, USA), and Minitab analysis programs were used for all statistical studies. Analysis of Variance and Student’s t-tests were used to test for statistical significance. Linear regression was utilized to test the correlation between different studied parameters, and the significance of the r-value was assessed by related t-test. A p-value of >0.05 was considered significant.
Results
The mean (±SEM) values of women age of were of GI (38.83±4.74 years) and of GIII (39.53±4.44 years), with no significant difference. Also, the mean (±SEM) values of body mass index were comparable between the women of GI (29.92± 4.88 kg/m2) and GIII (30.81± 4.81 kg/m2).
Table 1 shows the mean (±SEM) values of AMH levels of the 3 studied groups. This mean was significantly decreased in both groups of treatment. However, there was no significant difference in mean serum AMH values between GII and GIII. The mean (±SEM) value of the basal serum AMH (pre-CT women) was significantly declined in those women who had amenorrhea after the first course of CT compared to the mean AMH value of women who remain menstruated (p<0.001), Table 2.
Table 1.
The mean values of serum AMH concentrations in GI, GII, GIII.
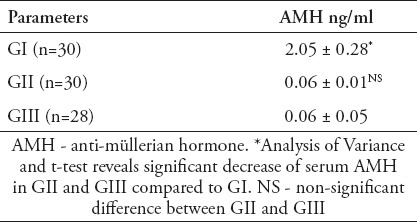
Table 2.
The relation between menstrual cycle status and the mean value of anti-müllerian hormone (AMH).
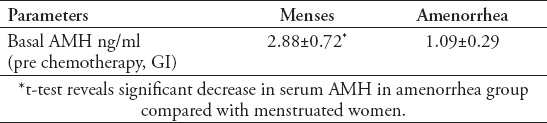
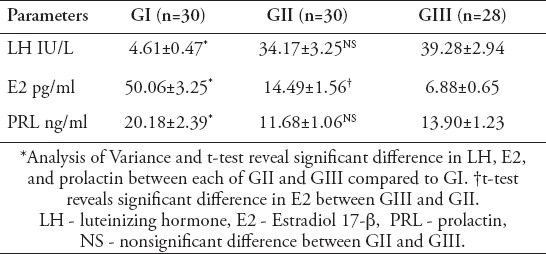
Table 3 shows significant increase in mean serum value of LH levels of GII and GIII (p<0.0005) compared to GI. However, there was no significant difference in serum mean value of LH between GII and GIII. The same table also reveals the significant decrease in mean value of serum E2 in GII and GIII in comparison with GI (for both p<0.0005), with significant difference between GII and GIII (p<0.016). The mean (±SEM) value of serum prolactin levels were significantly decreased in GII (p<0.001) and GIII (p<0.011) compared to GI. There was no significant difference between GII and GIII.
Table 3.
The mean values of serum LH, E2, PRL concentrations in GI, GII, GIII.
Discussion
The present cohort study revealed the effect of CT on OR indicated by serum AMH in women with BC. These effects included significantly decreased serum AMH in GII and GIII (CT-treated BC women groups) compared with GI, which represents women before treatment (Table 1). Chemotherapy treatment reduces the number of primordial and early growing follicles, which results in premature ovarian insufficiency, infertility, and AMH deficiency.10
The results confirmed by the present study are in agreement with D’Avila et al11 who showed a significant decline in serum AMH after completing CT compared with a group before treatment, due to damage of the ovarian stroma and effects upon oocytes at any stage.11 The results of the present study confirmed that the baseline of serum AMH is an important biomarker for menstruation status (Table 2). This means that serum levels of AMH pre-treatment may be a predictor of the OR status and the incidence of amenorrhea after CT. This result is in accordance with Anderson et al12 who found a positive correlation between serum AMH and menses status, with high level of AMH patients being less prone to amenorrhea. Also, this study agrees with the study of Dillon et al,13 which revealed a significant decrease in serum AMH after CT compared to a group before treatment.
Table 3 presents significant differences of LH and E2 levels among the studied groups. Serum LH and E2 levels changed to postmenopausal levels after the first and second course of CT. Chemotherapy induced primary hypergonadotropic hypogonadism, as confirmed by results for premature ovarian insufficiency, infertility and estrogen deficiency that were observed by low levels of E2 and high LH levels.14
These hormones are affected by feedback mechanisms on the pituitary and the hypothalamus by estrogen from the ovaries. Decreased levels of estrogen leads to an elevation in follicle-stimulating hormone and LH secretion, while high levels of estrogen have the opposite effect.14 D’Avila et al,11 found that E2 levels revealed a significant decline in postmenopausal range after the CT was finished. The present study revealed a significant decline in serum Prolactin (PRL) in GII and GIII compared with GI (Table 3). The mean value of serum PRL levels in women with BC prior to CT in the present study was higher than the normal reference range, and then decreased post CT. Tikk et al15 linked prolactin and invasive breast cancer tumors and showed that higher circulating prolactin is associated with increased risk of breast cancer.
Limitation of the present study was the inability to follow up with the same women of GI, pre-treatment of CT, until the end of complete courses of treatment, meaning both courses of 1 and 2.
In conclusion, the measurement of serum AMH may be a useful biochemical marker for measuring the extent of ovarian reserve damage and the incidence of amenorrhea; high levels of AMH prior to CT treatment may be an indicator for preservation of menstrual cycle post CT. Serum PRL measurement is a highly appropriate marker for CT follow-up in women with breast cancer.
Acknowledgment
Authors would like to thanks all staffs of Teaching Laboratories, Baghdad Teaching Hospital, and the Gastrointestinal Hospital, Medical City, Baghdad, Iraq, for their support and assistance.
Footnotes
References
- 1.Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127:2893–2917. doi: 10.1002/ijc.25516. [DOI] [PubMed] [Google Scholar]
- 2.Jemal A, Tiwari RC, Murray T, Ghafoor A, Samuels A, Ward E, et al. Cancer statistics, 2004. CA Cancer J Clin. 2004;54:8–29. doi: 10.3322/canjclin.54.1.8. [DOI] [PubMed] [Google Scholar]
- 3.Iraqi National Cancer Research Center. Brief historical introduction, establishing the breast & cervical cancer research unit and the Iraqi National Cancer Research Center/Program. Baghdad (Iraq): Iraqi National Cancer Research Center; 2013. [Google Scholar]
- 4.Partridge AH, Gelber S, Peppercorn J, Sampson E, Knudsen K, Laufer M, et al. Web-based survey of fertility issues in young women with breast cancer. J Clin Oncol. 2004;22:4174–4183. doi: 10.1200/JCO.2004.01.159. [DOI] [PubMed] [Google Scholar]
- 5.Jamil Z, Fatima SS, Ahmed K, Malik R. Anti-mullerian hormone: above and beyond conventional ovarian reserve markers. Dis Markers. 2016;2016:5246217. doi: 10.1155/2016/5246217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.van Disseldorp J, Faddy MJ, Themmen AP, de Jong FH, Peeters PH, van der Schouw YT, et al. Relationship of serum antimüllerian hormone concentration to age at menopause. J Clin Endocrinol Metab. 2008;93:2129–2134. doi: 10.1210/jc.2007-2093. [DOI] [PubMed] [Google Scholar]
- 7.Fréour T, Barrière P, Masson D. Anti-müllerian hormone levels and evolution in women of reproductive age with breast cancer treated with chemotherapy. Eur J Cancer. 2017;74:1–8. doi: 10.1016/j.ejca.2016.12.008. [DOI] [PubMed] [Google Scholar]
- 8.Groome NP, Evans LW. Does measurement of inhibin have a clinical role? Ann Clin Biochem. 2000;37:419–431. doi: 10.1177/000456320003700401. [DOI] [PubMed] [Google Scholar]
- 9.Burits CA, Ashwood ER, Bruns DE. Tietz Fundamentals of Clinical chemistry. 6th ed. Philadelphia (PA): Saunders Elsevier; 2008. pp. 373–401. and 735-801. [Google Scholar]
- 10.Bozza C, Puglisi F, Lambertini M, Osa EO, Manno M, Del Mastro L. Anti-Mullerian hormone: determination of ovarian reserve in early breast cancer patients. Endocr Relat Cancer. 2014;21:R51–R65. doi: 10.1530/ERC-13-0335. [DOI] [PubMed] [Google Scholar]
- 11.D'Avila ÂM, Capp E, Corleta HVE. Antral Follicles Count and Anti-Müllerian hormone levels after gonadotoxic chemotherapy in patients with breast cancer: cohort study. Rev Bras Ginecol Obstet. 2017;39:162–168. doi: 10.1055/s-0037-1601438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Anderson RA, Rosendahl M, Kelsey TW, Cameron DA. Pretreatment anti-Müllerian hormone predicts for loss of ovarian function after chemotherapy for early breast cancer. Eur J Cancer. 2013;49:3404–3411. doi: 10.1016/j.ejca.2013.07.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Dillon KE, Sammel MD, Prewitt M, Ginsberg JP, Walker D, Mersereau JE, et al. Pretreatment antimüllerian hormone levels determine rate of posttherapy ovarian reserve recovery: acute changes in ovarian reserve during and after chemotherapy. Fertil Steril. 2013;99:477–483. doi: 10.1016/j.fertnstert.2012.09.039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Fritz MA, Speroff L. Female infertility. Clinical Gynecologic Endocrinology and Infertility. 8th ed. Philadelphia (PA): Lippincott Williams and Wilkins; 2011. pp. 1137–1190. [Google Scholar]
- 15.Tikk K, Sookthai D, Fortner RT, Johnson T, Rinaldi S, Romieu I, et al. Circulating prolactin and in situ breast cancer risk in the European EPIC cohort: a case-control study. Breast Cancer Res. 2015;17:49. doi: 10.1186/s13058-015-0563-6. [DOI] [PMC free article] [PubMed] [Google Scholar]