

Abstract
BACKGROUND
Left ventricular function, volumes and regional wall motion provide valuable diagnostic information and are of long-term prognostic importance in patients with dilated cardiomyopathy (DCM). This study was designed to compare the effectiveness of 2D-echocardiography and gated single-photon emission tomography (SPECT) for evaluation of these parameters in patients with DCM.
PATIENTS AND METHODS
Gated SPECT and 2D-echocardiography were performed in 33 patients having DCM. Gated SPECT data, including left ventricular volumes and left ventricular ejection fraction (LVEF), were processed using an automated algorithm. Standard technique was used for 2D-echocardiography. Regional wall motion was evaluated using both modalities and was scored by two independent observers using a 16-segment model with a 5-point scoring system.
RESULTS
The overall agreement between the two imaging modalities for the assessment of regional wall motion was 56% (298/528 segments). With gated SPECT, LVEF, end-diastolic volume (EDV), and end-systolic volume (ESV) were 27±9%, 217±77 mL, and 163±73 mL, respectively, and 30±8%, 195±58 mL, and 137±48 mL with echocardiography. The correlation between gated SPECT and 2D-echocardiography was good (r=0.76, P<0.01) for the assessment of LVEF. The correlation for EDV and ESV were also good, but with wider limits of agreement (r=0.72, P<0.01 and r=0.73, P<0.01, respectively) and significantly higher values were obtained with gated SPECT (P<0.01).
CONCLUSIONS
Gated SPECT and 2D-echocardiography correlate well for the assessment of LV function and LV volumes. Like 2D-echocardiography, gated SPECT provides reliable information about LV function and dimension with the additional advantage of perfusion data.
Dilated cardiomyopathy (DCM) is the most common cardiomyopathy and has a poor prognosis.1 DCM is characterized by ventricular re-modeling producing chamber dilatation, normal or decreased wall thickness, and diminution in systolic function. Impaired systolic function causes an increase in left ventricular end-diastolic (LVEDV) and left ventricular end-systolic volume (LVESV) with reduced left ventricular ejection fraction (LVEF). Left ventricle volume, LVEF, and regional wall motion provide valuable diagnostic information and are of long-term prognostic importance in patients with DCM.2,3 Non-invasive techniques that are available to assess these parameters include two-dimensional (2D) echocardiography, magnetic resonance imaging (MRI) and radionuclide angiography (RNA).4–7 Neither these procedures nor gated SPECT matches the gold standard. Because of its excellent spatial resolution and freedom from contamination by surrounding structures, contrast angiography has been the standard to which all techniques have been compared. Of the noninvasive methods, RNA is unique because the radioactivity that is injected for the purpose of imaging the heart temporarily remains in the cardiac chambers in a concentration that is directly proportional to the volume of blood in those chambers, making the technique inherently quantitative. All the other noninvasive and invasive techniques require mathematical assumptions about the geometry of the ventricle to quantify ventricular function. Such assumptions work well some of the time, but when shape of a ventricle is distorted by localized infarction, severe hypertrophy, or marked dilatation, the accuracy of geometric approaches is questionable.8 Recently, it has become possible to assess LV perfusion, function, and volumes simultaneously using electrocardiography gating during acquisition of single photon emission tomography (SPECT) perfusion images. Both technetium 99m (Tc-99m) and thallium 201 (Tl-201), the most commonly used tracers for perfusion scintigraphy, can be used for gated SPECT purposes.9–15 However, limited data are available regarding the accuracy of gated SPECT to evaluate these parameters in patients with DCM and significantly depressed LV function.14–18 The purpose of this study was to evaluate the accuracy of gated SPECT for the assessment of LVEF, LV volumes, and regional wall motion in such patients in comparison to more routinely used echocardiography.
Patients and Methods
The study group consisted of 33 patients (25 men and 8 women) who were diagnosed with either ischemic or idiopathic DCM. The diagnosis of DCM was based on diffuse LV hypokinesis, an LVEF <45%, LVEDV >3.0 cm3m−2, and exclusion of other etiologic factors that may cause LV dysfunction. Based on patient history and coronary angiography findings, 21 patients were diagnosed with ischemic DCM and 12 patients were diagnosed with idiopathic DCM. The mean (±SD) age was 62±11 years (age range, 38–80 years).
Patients with arrhythmias, left bundle branch block, implanted pacemakers, acute myocardial infarction or unstable angina within the last month, percutaneous angioplasty, and coronary artery bypass graft surgery were excluded from the study. All patients were clinically stable and their cardiac medications were not changed during the study. The clinical research protocol was approved by the ethics committee of the Kocaeli University School of Medicine and all patients provided informed consent prior to enrollment into the study.
The study protocol included a resting gated SPECT imaging and a resting echocardiography study that were performed within a 15-day period. At resting condition, 555 MBq Tc-99m methoxyisobutyl-isonitrile (MIBI) was injected intravenously and electrocardiography gated myocardial perfusion SPECT acquisition was started 45 minutes following the injection. Data acquisition was performed with a single-head SPECT system (ADAC, Argus Epic, Milpitas, California, USA) equipped with low-energy, high-resolution collimators. A 20% window around a 140-keV energy peak of Tc-99m MIBI was used. A total of 64 projections (step-andshoot mode, 30 seconds per projection) were obtained over an 180º circular orbit. Acquisitions were gated for eight frames per cardiac cycle (acceptance window, 50%).
The gated SPECT images were reconstructed using filtered back-projection (Butterworth filter, order 10, cut-off frequency 0.55). The resulting transaxial slices were re-oriented perpendicular to the heart’s long axis, yielding long- and short-axis tomograms. Images were not corrected for attenuation. Gated SPECT images were assessed visually for regional function by two experienced observers blinded to the echocardiography results. A 16-segment model, 5-point score (1=normal, 2=mildly hypokinetic, 3=severely hypokinetic, 4=akinetic, and 5=dyskinetic) was used to enable direct comparison of the same areas for both gated SPECT and echocardiography data (Figure 1). Segments with either normal wall motion or mild hypokinesia were considered normal.
Figure 1.
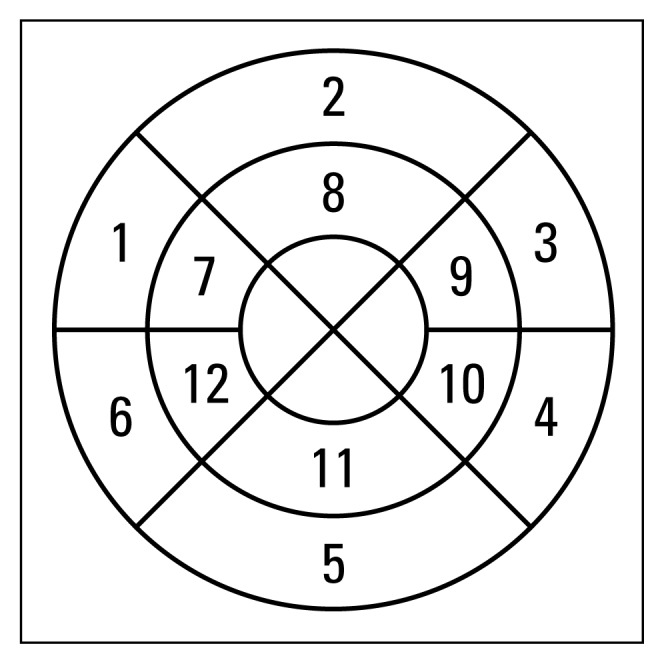
The 16-segment model used for gated SPECT and echocardiography, 1–6=six basal segments (1, anteroseptal; 2, anterior; 3, anterolateral; 4, inferolateral; 5, inferior; 6, inferoseptal), 7–12=six midventricular segment (7,anteroseptal; 8, anterior; 9, anterolateral; 10, inferolateral; 11, inferior; 12, inferoseptal) and segment 13–16 four apical segments (including 13, septal; 14, anterior; 15, lateral; 16, inferior).
The LVEF and LV volumes were calculated using previously validated and commercially available automated software (Autoquant software, Cedars- Sinai Medical Center, Los Angeles, California, USA) from the gated SPECT images. The algorithm operates in three-dimensional space. It segments the LV, estimates and displays the endo- and epicardial surfaces for every gating interval, calculates ESV and EDV, and derives the related LVEF by taking their difference (stroke volume) and dividing it by EDV.
Two dimensionally guided M-mode echocardiograms were performed with standard techniques using a Toshiba SSA-390 A echocardiograph. Images were acquired at rest with standard parasternal, short-axis and apical (two chamber and four chamber) views. EDV, ESV and LVEF were derived with the previously validated modified Simpson’s biplane discs method.19,20
For the assessment of regional wall motion similar to gated SPECT, a 16-segment model, and a 5-point score was used (same segments, same scoring system). Again, segments with normal wall motion and mild hypokinesia were considered normal, whereas the remaining segments were considered severely dysfunctional.
Continuous data were expressed as mean±SD and compared using the two-tailed Student’s t-test for paired and unpaired data when appropriate. The agreement for segmental wall motion was assessed with 3×3 tables and weighted kappa statistics. Kappa values <0.4, between 0.4 and 0.75, and >0.75 were considered to represent poor, fair to good and excellent agreement respectively, based on Fleiss’s classification. 21
The agreement between LVEF, EDV and ESV derived from gated SPECT and echocardiography data were determined with linear regression (Pearson correlation coefficient) and Bland-Altman analysis.22 For all tests, a P value <0.05 was considered significant.
Results
Of the 33 patients enrolled into the study, 21 were diagnosed with ischemic DCM and 12 patients were diagnosed with idiopathic DCM. Twenty-one patients had a history of myocardial infarction. On angiography, eight patients were found to have onevessel disease, seven patients were found to have twovessel disease, and six patients were found to have three-vessel disease. Fifteen patients had diabetes mellitus and 18 patients had systemic hypertension.
On echocardiography, 298 (56%) segments revealed normal wall motion, 195 (37%) segments showed severe hypokinesia, and 35 (7%) segments showed akinesia or dyskinesia. On gated SPECT, 289 (55%) segments showed normal wall motion, 161 (30%) segments showed severe hypokinesia and 78 (15%) segments showed akinesia or dyskinesia. The agreement on a segmental basis is shown in Table 1. An exact overall agreement of 56% was found, with a kappa value of 0.23, indicating poor agreement between the two methods.
Table 1.
Agreement for regional wall motion analysis between echocardiography and gated SPECT (n=33)
| Gated SPECT | Echocardiography | ||
|---|---|---|---|
| 1–2 | 3 | 4–5 | |
|
| |||
| 1–2 | 204 | 79 | 6 |
|
| |||
| 3 | 72 | 77 | 12 |
|
| |||
| 4–5 | 22 | 39 | 17 |
Agreement = 56%, kappa = 0.23
1–2, normal-mild hypokinesia; 3, severe hypokinesia; 4–5 akinesia-dyskinesia.
Table 2 shows LVEF measured by gated SPECT and echocardiography. The values were similar and showed good correlation by linear regression (Figure 2A). The mean difference in LVEF measured with gated SPECT and echocardiography was −3% ±6%, with large limits of agreement (9% to −15%) (P<0.01, 95% CI, −5.24 to −0.88), as shown by a Bland-Altman analysis (Figure 2B). The mean EDV by echocardiography was slightly lower than with gated SPECT (Table 2). Linear regression found a good correlation (Figure 3A). The mean difference in EDV measured with gated SPECT and echocardiography was 22±53 mL (P<0.01, 95% CI, 3.06–40.82), and with large limits of agreement (128 to −85 mL) (Figure 3B). The mean ESV on echocardiography was slightly lower than the corresponding ESV values measured with gated SPECT (Table 2). Linear regression analysis showed a good correlation (Figure 4A). The mean difference between ESV values measured with gated SPECT and echocardiography was 26±50 mL (P<0.01, 95% CI, 8.48 to 44.12), and with large limits of agreement (127 to −75 ml) (Figure 4B).
Table 2.
Measurement of left ventricular volumes and ejection fraction with echocardiography and gated SPECT.
| Gated SPECT | Echocardiography | P | |
|---|---|---|---|
| LVEF | |||
| Mean±SD (%) | 27±9 | 30±8 | <0.01 |
| Range (%) | 10–49 | 10–45 | |
| EDV | |||
| Mean±SD (mL) | 217±77 | 195±58 | <0.01 |
| Range (mL) | 98–375 | 90–331 | |
| ESV | |||
| Mean±SD (mL) | 163±73 | 137±48 | <0.01 |
| Range (mL) | 50–325 | 55–250 | |
Figure 2A.

Relation between left ventricular ejection farction (LVEF) assessed with gated SPECT and echocardiography.
Figure 2B.

Bland-Altman plot for LVEF.
Figure 3A.

Linear regression analysis demonstrating the relation between end diastolic volume (EDV) assessed with gated SPECT and echocardiography.
Figure 3B.

Bland-Altman plot for EDV.
Figure 4A.

Relation between end systolic volume (ESV) assessed with gated SPECT and echocardiography.
Figure 4B.

Bland-Altman plot for ESV.
To assess the reproducibility of the technique, 26 of the study patients were randomly selected and reprocessed by a second specialist, who was blinded to the results of the initial evaluation. There was good correlation between the values for LVEF (y=0.77 x+0.59, r=0.969, SEE, 2.71%, P<0.01, mean difference 5.76%, limits of agreements −0.78 to 9.81) that were calculated by the two different specialists with wider limits of agreement for EDVs (y=x+11, r=0.98, SEE, 12 mL, P<0.01, mean difference 12 mL, limits of agreements −11 to 35 mL) and ESVs (y=1.22 x+0.92, r=0.993, SEE, 10 mL, P<0.01, mean difference −0.73 mL, limits of agreements −19 to 21 mL).
Discussion
As DCM is the most common cardiomyopathy with a poor prognosis, assessment of regional perfusion as well as functional parameters is important for prognostic purposes.1,2,3 Gated SPECT offers the potential advantage of gathering information on both myocardial perfusion and function at the same time. Many previous studies have demonstrated the feasibility and validity of gated SPECT for evaluating myocardial perfusion as well as LV function and volumes.9–15 However, data regarding the performance of gated SPECT in patients with severely depressed LV function and dilated cardiomyopathy is still scarce.14–18 In particular, not much is known about the usefulness of gated SPECT for the assessment of regional wall motion in patients with DCM. Therefore, we focused our study solely on patients with DCM who already had depressed LV function. For comparison, 2D echocardiography was used, as it is currently one of the most widely applied and accepted non-invasive techniques to assess the LV volume, LVEF, and regional wall motion.19,20
In our study, the exact segmental agreement for assessment of regional wall motion between echocardiography and gated SPECT was 56%. This is lower than the numbers quoted in previous studies.18,23,24 The reason for this discrepancy may be two-fold: The visual analysis of wall motion by echocardiography is a subjective method that has an important inter-and intra-observer variability25 and our study group comprised a special group of patients with severely depressed LV function and remodeled (spherical) LV shape. Analysis of wall motion in these patients requires experience and may be more difficult than in patients with segmental wall motion abnormalities and relatively preserved (ellipsoid) LV shape due to the rather global hypokinesia.
Gated SPECT has a disadvantage in assessing the wall motion in a severely hypoperfused area or in an area with decreased myocardial thickness, as the obtained count may be inadequate to visualize the region of interest. As a result of this, accurate evaluation of ventricular function may be compromised. An image enhancement technique described by Nichols et al. improves the visualization of underperfused myocardium. 26 The use of this technique might improve the accuracy for the analysis of wall motion in segments with severely diminished perfusion.
Our study showed a good correlation between gated SPECT and 2D-echocardiography in determining LVEF, when LV is dilated. This technique was also highly reproducible, although there was a minor (3%) underestimation of LVEF with gated SPECT. All previous studies that validated the accuracy of gated SPECT with the quantitative gated SPECT method (QGS) have included patients with myocardial infarctions.9,15,17,18 However, few studies have focused specifically on the subgroup of patients with large earlier infarctions, in whom the ability of an automated approach would be most severely tested, because the absence or severe reduction of counts in transmural infarction or dilatation is likely to impair the ability of any approach to accurately assess endocardial borders. Germano et al developed the QGS program, and validated it against first-pass equilibrium radionuclide angiocardiography (ERNA) for LVEF. In another study, the QGS was also shown to have a high degree of reproducibility and repeatability. 9,27 Similarly good and excellent correlation between QGS and MRI was shown for measuring LV volumes.6,15 Tadamura et al. showed good correlation in LVEF between gated SPECT and 3D-MRI, although there was a small (3.5%) underestimation of LVEF with gated SPECT.28 Manrique et al. focused specifically on the accuracy of gated SPECT in 50 patients with large earlier myocardial infarctions (>20% of the left ventricle) and concluded that gated SPECT with QGS underestimated LVEF in these patients (mean difference, 4.7%).14 This was attributed to temporal under sampling and severe perfusion defects. However, their conclusion that LVEF is underestimated in patients with large perfusion defects has been challenged.29 Indeed, data from the same study showed that the presence and size of perfusion defects was not correlated with the degree of underestimation. An alternative interpretation is that a small systematic difference exist between 8 frame gated SPECT and ERNA-LVEF measurements, possibly because of a temporal under sampling (an average 4% difference) reported by Germano et al, and Manrique et al, that occurs regardless of the presence of perfusion defects. This can be overcome by systematically adding 4 ejection fraction points to 8 frame gated SPECT or by using 16 frame gating.29 Previous studies with echocardiography correlation reported similar results.18,30 Although systematic differences between different methods for LVEF measurement (such as gated SPECT and 2D-echocardiography) may be detectable, small and predictable differences should not detract from the clinical usefulness of each method, provided that the method is reproducible and repeatable and the differences are well recognized.
In our study, the correlations between LV volume measurements with gated SPECT and 2D-echocardiography were good and both EDV and ESV values measured using gated SPECT were somewhat higher compared to echocardiography. Nichols et al. compared different analysis programs to correlate gated SPECT data to echocardiography in patients with severe perfusion defects, and demonstrated an overestimation of LV volumes with gated SPECT when QGS was used, especially in those patients with large LV volumes.30 QGS relied more heavily on systolic count changes to compute endocardial offsets, and some phantom and clinical studies have suggested that gated SPECT underestimates true thickening.31,32 This method adjusted ED offsets partly based on regional myocardial counts and therefore would have smaller endocardial offsets and larger LV cavity volumes for hypoperfused data.14 Similar results were reported by Vourvori C et al.18 On the other hand, Cwaj et al. evaluated 109 patients with both 2D-echocardiography and gated SPECT (using both Tl-201 and Tc-99m MIBI), and demonstrated good correlation between the two modalities for assessing LV volumes, but with slightly larger LV volumes on echocardiography than on gated SPECT.33 It is clear that this issue needs further study.
In conclusion, gated SPECT was found to have good correlation with 2D echocardiography for measuring LV volumes and LVEF. In clinical practice, gated SPECT may be a good alternative for patients with limitations for optimal echocardiography visualization. Furthermore, it may be routinely used for patients who may also need to be assessed for myocardial viability and/or ischemia at the same time. Contrary to the labor intensive and more observer- dependent echocardiography techniques that are widely used to assess LV volumes and LVEF, gated SPECT technique is fast, nearly completely automated, and highly reproducible.
References
- 1.Rodkey SM, Ratliff NB, Young JB. Cardiomyopathy and myocardial failure. In: Topol EJ, editor. Textbook of Cardiovascular Medicine. Philadelphia: Lippincott/Raven; 1998. pp. 2217–2219. [Google Scholar]
- 2.Hammermeister KE, DeRouen TA, Dodge HT. Variables predictive of survival in patients with coronary artery disease. Selection of univariate and multivariate analyses from the clinical, electrocardiographic, exercise, arteriographic and quantitative angiographic evaluations. Circulation. 1979;59:421–30. doi: 10.1161/01.cir.59.3.421. [DOI] [PubMed] [Google Scholar]
- 3.White HD, Norris RM, Brown MA, Brandt PW, Whitlock RM, Wild CJ. Left ventricular end-systolic volume as the major determinant of survival after recovery from myocardial infarction. Circulation. 1987;76:44–51. doi: 10.1161/01.cir.76.1.44. [DOI] [PubMed] [Google Scholar]
- 4.Starling MR, Crawford MH, Sorenson SG, Levi B, Richards KL, O’Rourke RA. Comparative accuracy of apical biplane cross/sectional echocardiography and gated equilibrium radionuclide angiography for estimating left ventricular size and performance. Circulation. 1981;63:1075–84. doi: 10.1161/01.cir.63.5.1075. [DOI] [PubMed] [Google Scholar]
- 5.Van der Wall EE, Vliegen HW, De Roos A, Bruschke AVG. Magnetic resonance imaging in coronary artery disease. Selection 1. Circulation. 1995;92:2723–39. doi: 10.1161/01.cir.92.9.2723. [DOI] [PubMed] [Google Scholar]
- 6.Bavelaar-Croon CDL, Kayser HWM, Van der Waal EE, Roos A, Dibbets-Schneider P, Pauwels EKJ, et al. Left Ventricular Function: Correlation of quantitative gated SPECT and MR imaging over a wide range of values. Radiology. 2000;217:572–5. doi: 10.1148/radiology.217.2.r00nv15572. [DOI] [PubMed] [Google Scholar]
- 7.Wackers FJ, Berger HJ, Johnstone DE, Goldman L, Reduto LA, Langou RA, et al. Multiple gated cardiac blood pool imaging for left ventricular ejection fraction: validation of the technique and assessment of variability. Am J Cardiol. 1979;43:1159–66. doi: 10.1016/0002-9149(79)90148-6. [DOI] [PubMed] [Google Scholar]
- 8.Murphy PB, Port SC. Radionuclide evaluation of left ventricular function. In: Sandler MP, Coleman RE, Patton JA, Wackers FJTh, Gottschalk A, editors. Diagnostic Nuclear Medicine. Philadelphia: Lippincott Williams & Wilkins; 2003. pp. 239–71. [Google Scholar]
- 9.Germano G, Kiat H, Kavanagh PB, Moriel M, Mazzanti M, Su HT, et al. Automatic quantification of ejection fraction from gated myocardial perfusion SPECT. J Nucl Med. 1995;36:2138–47. [PubMed] [Google Scholar]
- 10.Germano G, Erel J, Kiat H, Kavanagh PB, Berman DS. Quantitative LVEF and qualitative regional function from gated thallium-201 perfusion SPECT. J Nucl Med. 1997;38:749–54. [PubMed] [Google Scholar]
- 11.Mochizuki T, Murase K, Tamaka H, Kondoh T, Hamamoto K, Tauxe WN. Assessment of left ventricular volume using ECG-gated SPECT with technetium-99m MIBI and technetium-99m tetrofosmin. J Nucl Med. 1997;38:53–7. [PubMed] [Google Scholar]
- 12.Maunoury C, Chen CC, Chua KB, Thompson CJ. Quantification of left ventricular function with thallium-201 and technetium-99m-sestamibi myocardial gated SPECT. J Nucl Med. 1997;38:958–61. [PubMed] [Google Scholar]
- 13.Germano G, Erel J, Lewin H, Kavanagh PB, Berman DS. Automatic quantitation of regional myocardial wall motion and thickening from gated technetium-99m sestamibi myocardial perfusion single-photon emission computed tomography. J Am Coll Cardiol. 1997;30:1360–7. doi: 10.1016/s0735-1097(97)00276-3. [DOI] [PubMed] [Google Scholar]
- 14.Manrique A, Faraggi M, Vera P, Vilain D, Lebtahi R, Cribier A, et al. 201 Tl and 99mTc MIBI gated SPECT in patients with large perfusion defects and left ventricular dysfunction: comparison with equilibrium radionuclide angiography. J Nucl Med. 1999;40:805–9. [PubMed] [Google Scholar]
- 15.Vaduganathan P, He ZX, Vick GW, Mahmarian JJ, Verani MS. Evaluation of left ventricular wall motion, volumes, and ejection fraction by gated myocardial tomography with technetium 99m-labeled tetrofosmin: a comparison with cine magnetic resonance imaging. J Nucl Cardiol. 1999;6:3–10. doi: 10.1016/s1071-3581(99)90058-2. [DOI] [PubMed] [Google Scholar]
- 16.Nichols K, DePuey G, Krosnow N, Lefkowitz D, Rozanski A. Reliability of enhanced gated SPECT in assessing wall motion of severely hypoperfused myocardium: echocardiographic validation. J Nucl Cardiol. 1998;5:387–94. doi: 10.1016/s1071-3581(98)90144-1. [DOI] [PubMed] [Google Scholar]
- 17.Chua T, Yin LC, Thiang TH, Choo TB, Ping DZ, Leng LY. Accuracy of the automated assessment of left ventricular function with gated perfusion SPECT in presence of perfusion defects and left ventricular dysfunction: correlation with equilibrium radionuclide ventriculography and echocardiography. J Nucl Cardiol. 2000;7:301–11. doi: 10.1067/mnc.2000.105279. [DOI] [PubMed] [Google Scholar]
- 18.Vourvouri EC, Poldermans D, Bax JJ, Sianos G, Sozzi FB, Schinkel FLA, et al. Evaluation of left ventricular function and volumes in patients with ischaemic cardiomyopathy: gated single-photon emission computed tomography versus two dimensional echocardiography. Eur J Nucl Med. 2001;28:1610–5. doi: 10.1007/s002590100624. [DOI] [PubMed] [Google Scholar]
- 19.Schiller NB, Shah PM, Crawford M, DeMaria A, Devereux R, Feigenbaum H, et al. Recommendations for quantitation of the left ventricle by two dimensional echocardiography: American Society of Echocardiography Committee on Standards Subcommittee on Quantitation of Two-Dimensional Echocardiography. J Am Soc Echocardiogr. 1989;2:358–67. doi: 10.1016/s0894-7317(89)80014-8. [DOI] [PubMed] [Google Scholar]
- 20.Otterstad JE, Froeland G, St John Sutton M, Holme I. Accuracy and reproducibility of biplane two-dimensional echocardiographic measurements of left ventricular dimensions and function. Eur Heart J. 1997;18:507–13. doi: 10.1093/oxfordjournals.eurheartj.a015273. [DOI] [PubMed] [Google Scholar]
- 21.Fleiss JL. Statistical methods for rates and proportions. 2nd ed. New York: Wiley; 1981. [Google Scholar]
- 22.Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical assessment. Lancet. 1986;1:307–10. [PubMed] [Google Scholar]
- 23.Wahba FFM, Bavelaar-Croon CDL, Baur LNB, Zwinderman AH, Van Roosmalen RPM, Pauwels EKJ, et al. Detection of residual wall motion after sustained myocardial infarction by gated Tc-99m- Tetrofosmin SPECT: a comparison with echocardiography. Nucl Med Com. 2001;22:175–82. doi: 10.1097/00006231-200102000-00009. [DOI] [PubMed] [Google Scholar]
- 24.Bacher-Stier C, Muller S, Pachinger O, Strolz S, Erler H, Moncayo R, et al. Thallium-201 gated single -photon emission tomography for the assessment of left ventricular ejection fraction and regional wall motion abnormalities in comparison with two-dimensional echocardiography. Eur J Nucl Med. 1999;26:1533–40. doi: 10.1007/s002590050491. [DOI] [PubMed] [Google Scholar]
- 25.Picano E, Lattanzi F, Orlandini A, Marini C, L’Abbate A. Stress echocardiography and the humane factor: the importance of being expert. J Am Coll Cardiol. 1991;17:666–9. doi: 10.1016/s0735-1097(10)80182-2. [DOI] [PubMed] [Google Scholar]
- 26.Nichols K, DePuey EG, Rozanski A, Salensky H, Friedman MI. Image enhancement of severely hypoperfused myocardia for computation of tomographic ejection fraction. J Nucl Med. 1997;38:1411–7. [PubMed] [Google Scholar]
- 27.Berman D, Germano G, Lewin H, Kang X, Kavanagh PB, Tapnio P, et al. Comparison of post-stress ejection fraction and relative left ventricular volumes by automatic analysis of gated myocardial perfusion single-photon computed tomography acquired in the supine and prone positions. J Nucl Cardiol. 1998;5:40–7. doi: 10.1016/s1071-3581(98)80009-3. [DOI] [PubMed] [Google Scholar]
- 28.Tadamura E, Kudoh T, Motooka M, Inubushi M, Shirakawa S, Hattori N, et al. Assessment of regional and global left ventricular function by reinjection Tl-201 and rest Tc-99m ECG-gated SPECT: Comparison with three-dimensional magnetic resonance imaging. J Am Coll Cardiol. 1999;33:991–7. doi: 10.1016/s0735-1097(98)00661-5. [DOI] [PubMed] [Google Scholar]
- 29.Germano G, Berman DS. On the accuracy and reproducibility of quantitative gated myocardial perfusion SPECT. J Nucl Med. 1999;40:810–3. [PubMed] [Google Scholar]
- 30.Nichols K, Lefkowitz D, Faber T, Folks R, Cooke D, Garcia EV, et al. A. Echocardiographic validation of gated SPECT ventricular function measurements. J Nucl Med. 2000;41:1308–14. [PubMed] [Google Scholar]
- 31.Buvat I, Barlett ML, Kitsiou AN, Dilsizian V, Bacharach SL. A ‘hybrid’ method for measuring myocardial wall thickening from gated PET/SPECT images. J Nucl Med. 1997;38:324–9. [PubMed] [Google Scholar]
- 32.Fukuchi K, Uehara T, Morozumi T, Tsujimura E, Hasegawa S, Yutani K, et al. Quantification of systolic count increase in technetium-99m MIBI gated myocardial SPECT. J Nucl Med. 1997;38:1067–73. [PubMed] [Google Scholar]
- 33.Cwajg E, Cwajg J, He ZX, Hwang WS, Keng F, Nagueh SF, et al. Gated myocardial perfusion tomography for the assessment of left ventricular function and volumes: Comparison with echocardiography. J Nucl Med. 1999;40:1857–65. [PubMed] [Google Scholar]