

Abstract
The Integrated Academic (Advanced) Information Management System (IAIMS) initiative emerged in the early 1980s to respond to trends in biomedical information, transfer and access, and to identify the implications for health sciences libraries. Three recurrent themes have emerged as being essential to the creation of IAIMSs : changing the paradigm ; redirecting expenditures to build reuseable infrastructure ; and working across cultural boundaries. An IAIMS penetrates an organization in four stages : from creating awareness ; through development of foundation infrastructure ; through integration as an extra effort ; to integration as a byproduct of organizational structure and information architecture. Extension of the IAIMS to support a regional area is a natural fifth stage that reapplies the processes of the first four stages and re-reuses the infrastructure that has been built within the cooperating organizations. Area IAIMSs have the potential to transform biomedicine by enabling new paradigms for manpower development and publication of information.
Since the Integrated Academic Information Management System (IAIMS) initiative began in the early 1980s, there have been dramatic changes in what information technology can do and in the health care market. Over the course of the initiative, we've seen equally dramatic changes in the types of things that people are doing under the umbrella of IAIMSs.
Our challenge today is to try to tease apart the lasting lessons about IAIMSs from this background of changes in technology and the marketplace. For those of you who are clinically oriented, we need to look at the evolution of IAIMSs through a process analogous to digital subtraction angiography. That process uses a plain film to subtract the background from a film taken with dye so that the vascular system becomes visible.
What are the lasting lessons from 13 years of IAIMSs ? What have we learned that we can use as a launch pad for the next decade ?
Origins of IAIMSs
IAIMSs trace their origins to a contract issued by the National Library of Medicine (NLM) to the Association of American Medical Colleges (AAMC) in 1979. That contract was to study trends in biomedical information transfer and access, and to identify the implications for health sciences libraries. The findings of the AAMC study were reported in 1982 by Nina Matheson and John Cooper. 1 They found academic health centers to have information support systems consisting of “fragmented mixtures of single function, manual, and computer-based files that can neither communicate or exchange information effectively.”
The report issued three challenges :
To academic health sciences centers and hospitals— “To implement a network that facilitates the flow of recorded knowledge throughout their institutions... strengthen the technological capabilities of libraries to serve as stage one network nodes.”
To professional associations and organizations—“To link the academic and administrative organization information bases to hospitals and to individual practitioners in an interactive information network.”
To industry, foundations, and federal and state agencies—“To support the development of prototype network systems and programs that encourage the rapid integration of information technologies in the learning and practice of the health professions... programs that attract and retain qualified people in medical information and knowledge-based development in academic centers.”
The NLM responded immediately. In a few months they issued a request for a proposal for strategic planning for information resource management within institutions. The Integrated Academic Information System (IAIMS) program was later incorporated into the long-range funding strategy for extramural programs. The first IAIMS initiative focused on academic institutions and on libraries and was a three-stage planning, model development, and implementation process. In the late 1980s, site visits to the institutions and libraries responsible for the first set of implementation proposals confirmed that the concept had been proven. The question then became, “How do we do it ? ” “How do we scale up and do it in a big way ? ” The focus of the IAIMS initiative changed from academic information management systems to advanced information management systems. 2
I want to make the case that we are ready for another major step in the evolution of the IAIMS. I would like to persuade you that we should change from advanced information management systems to area information management systems. Our challenge is to take the lessons from IAIMSs, the changes that have occurred in information technology, and the changes that have now taken place in the market to find a way to take IAIMSs beyond one institution, to provide an essential infrastructure for the integrated delivery system.
Recurrent Themes about Creating an IAIMS
Table 1 outlines the changing environment in which the IAIMS concept has evolved. Through a transition that has seen network bandwidths increase by six orders of magnitude, three recurrent themes have emerged as being essential to creation of an IAIMS.
Table 1.
IAIMS—Development against a Background of Change
| Processor | Bandwidth | Application | Market | |
|---|---|---|---|---|
| 1982 | 8088 | 0.0003 MBit modem | Library catalog | DRGs |
| 1987 | 286 | 4-10 MBit EN and TR | Emulation and gateways | Growth |
| 1992 | 486 | 100 MBit FDDI | Interface engines and repositories | Managed care |
| 1996 | Pentium Pro | >155 MBit ATM | WWW and multimedia | Integrated delivery system |
The first lesson is about the idea of a paradigm shift. To achieve an IAIMS, you must change the paradigm. Those of us who are responsible for informatics, information systems, or libraries within our institutions are faced with communities of users who are frustrated by their inability to do today's work. They want to tell us what is wrong with the tools they have, and they want us to help them. We need to help them, but if we focus on that alone we are putting all of our energy into fixing past decisions about how to use old technology. We have to help those people step past today's problems, to think with us about how they want to work in totally new ways that can be enabled by the kind of information access that we can now support. Once that vision is clear, we can see how to move from where we are to where we want to be in a way that solves today's problems incrementally. Focusing on future uses of new technology is a key piece of IAIMSs.
The best analogy is the one that Tony Gorry uses about the camera. When the camera first came out, people used it to take pictures of still life, because that was what artists had traditionally painted. The camera could not capture still life scenes that were as engaging as those the artist could paint. The new technology was being used to do something that was already done quite well with paint. Then people began to discover that the camera could catch light and motion, and a whole new art form engaged—one that could not be achieved with paint.
The second lesson is about building infrastructure. When people estimate the cost of an IAIMS infrastructure, they come up with a price tag of several million dollars. The institutional leadership says “we do not have the resources.” They are not being asked the right question. Every institution of any size is spending millions of dollars per year on information technology. Ask the following questions : “What are your current costs for information handling ?” “What is the library budget ?” “What is being spent by individual departments buying and maintaining personal computers ?” All of that money is already being spent, but it is spent through a series of individual decisions. The expenditures do not result in an infrastructure that can be shared. An IAIMS plan provides a road map so that individual investments can be made in a way that builds reuseable infrastructure.
The third lesson is about working across boundaries and cultures. In the early IAIMS efforts, the challenge was how to get one group of people to look at administrative, educational, research, and clinical needs. As the Vanderbilt strategic plan was developed, we identified over a thousand capabilities that people wanted. The job became possible as we looked at that one-thousand-item list and asked, “What are the things that these needs have in common ?” To do that, we had to open up a dialogue that had not previously existed between groups. The next step is to cross cultures by having information systems, library, and academic informatics groups share their visions. If that culture gap can be bridged, we should be able to work across organizational boundaries. The problems are the same, as are the processes that relate to them.
Strategies That Will Scale Up to Support an Enterprise
I have led and learned lessons from the IAIMS experiences at two institutions. Being in a position to compare what we are doing at Vanderbilt with what we did at Duke has been a unique learning experience. That comparison can be illustrated by reading the article that describes the Vanderbilt transition from planning to implementation, 3 and reading the parallel paper that describes Duke's position as it transitioned from model testing to implementation. 4 At a high level, the difference is that the Duke implementation grant specified in great detail what would be done in each of the user domains. At Vanderbilt, we wrote a very different proposal. We did not focus our attention on specific end-user functions. Instead, we focused on that first letter of IAIMS, the I, the “Integrated.” We asked, “What does an institution have to do to establish an environment that allows individual projects to come together to form an IAIMS ?” The change in strategy did not reflect a change in objective. We thought we could produce a better result for the user community.
The real question is, how do you produce an IAIMS that can scale up to support enterprise-wide use ? A plan is important, but a plan is not the answer. A core of planning functions should be provided by the enterprise to guide decision making at all levels of the organization. Support for organizational development, strategic planning, and envisioning the future have been critical to any IAIMS effort.
As IAIMSs move across organizational boundaries, policy formulation moves higher up the ladder of priorities that must be dealt with. The value of information relates directly to the speed with which it is delivered to the point where it can impact a decision. In an organization, information moves very slowly through the organizational structure. It is owned and controlled by the organization, or the part of the organization, that produces it. To realize the advantages of the IAIMS, we must change from a focus upon data ownership to one of data stewardship. We are forced to face difficult issues such as, “How do we bring the information together, and how do we credential people for access ?” The challenge of this change in thinking is magnified as you cross organizational boundaries.
To move toward an Integrated Area Information Management System, organizations within the area must move toward a common reference architecture. Such an architecture opens the way to building an infrastructure of components. The advantages are evident to a person who assembled a “stereo” in the 1960s. You bought an amplifier and speakers, and plugged in a turntable and a receiver. When tape decks came out, you could plug them in and reuse the amplifier and speakers. The same reuse worked with the new generation of technology represented by the CD-ROM. A component-based strategy works for data management. We can record an item in a database, such as Access, move it to a spreadsheet such as Excel to manipulate it, and finally move it to a display program such as PowerPoint to project it.
Technology forecasting is a necessary part of the IAIMS building process. Each computer user is faced with making decisions about which technology to invest in. We diverge because there are no off-the-shelf recommendations. If we are able to put recommendations on the table, people will converge around them, particularly if volume pricing provides an incentive through reduced costs. Technology forecasting can be near-term—e.g., do not buy a PC if it is less powerful than a “floor” configuration—or it can be long-term—providing a prediction of the role of a new technology, such as wireless communication.
Often, the most difficult part of creating an IAIMS is fostering the necessary strategic alliances. The IAIMS consortium, and IAIMSs in general, are built around the premise that by sharing, we can accomplish what we cannot accomplish as individuals. But sharing takes time, and people are faced with impossible demands on their time and talents. Strategic alliances, therefore, have to be built upon win-win situations that take very little added effort from the participants and still allow each to work toward his or her primary agenda items. Vanderbilt's successes in this area offer case studies of what is required.
Vanderbilt was able to succeed in a joint development partnership with a vendor. Before we entered into discussions, we had a working prototype of what we needed. We continued to build that prototype into our infrastructure while the vendor built a version that fit smoothly into its product. We did not give up control of the critical path of our implementation, but we were able to use the vendor's solution when it was delivered on time.
Our strategic alliance with the University of Pittsburgh to import the MARS technology 5 is another demonstration case. The alliance worked because we had already recruited individuals from Pittsburgh who were able to manage the Vanderbilt side of the project at little cost to Pittsburgh. Any transfer back to Pittsburgh resulted in a win-win.
Intra-institution information system projects fail because of the magnitude of the task. The concept of an area infrastructure could be daunting. The fast-tract strategy involves reducing a large project to a set of steps. As a step is completed, benefits are achieved and the course can be corrected to reflect lessons learned. A project can be segmented into layers that build on one another. Foundational elements such as a network, transaction-processing systems, intellectual capital, and facilities are put in place first. The resources that permit system integration make up a second layer. This layer leverages the foundation layer. A third layer is needed to provide new services such as just-in-time education. Each layer builds on, and reuses, elements of lower levels in a way that would not be possible if those functions were provided as intact services or information systems.
Integrated AREA Information Management Systems
As part of our vision-development process, we have produced a videotape that depicts how we might support practices that affiliate with Vanderbilt through information services. 6 This vision may not prove true. Nonetheless, it makes the point that traditional information systems, which provide limited communication between fairly isolated care processes, will not let us achieve our objectives. We need new processes that are enabled by constant communication—a very different strategy.
As we consider moving in this direction across our health care region, it is clear that we have to do more than develop information systems. We need to provide wide-area connections to the backbone network ; a means to configure and update workstations at sites around the region ; an effective end-user support mechanism ; and cost-effective training. We are following a parallel strategy outside the sphere of the Informatics Center to build expertise in practice management and case management process. Although information systems are hard to transfer, we predict that the processes that are necessary to get people to work together will be transferable to support the region.
Despite significant change in what is being worked on under the IAIMS umbrella, I think that we are not seeing a fundamental change in the effort. Rather, we are seeing certain lessons and ideas used in increasingly complex settings. We might think of IAIMS as penetrating an institution, or a region, in the same way we think about managed care penetrating a market, as depicted in Figure 1. The first stage is focused around individual applications (i.e., computer-aided instruction or clinical pathways). Committee structures begin to create awareness that integration is as important as function, but the focus is on applications. In the second stage, the organization is beginning to invest in infrastructure, such as a backbone network that creates a capability for integration. Stage three provides integration as a byproduct of separate new applications (an IAIMS menu that links different systems, or a repository that pulls together data from multiple systems). In stage four, where Vanderbilt is now, the integration is a byproduct of an architecture made up of reusable components. The integration becomes inherent with no added cost.
Figure 1.
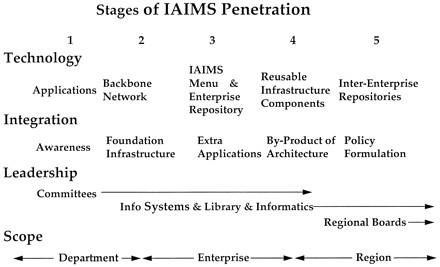
A five-stage model for assessing the degree to which IAIMS has penetrated an organization or region based upon the technology being utilized, the means for achieving integration, the locus of leadership, and the scope of the effort.
If we are to justify renaming IAIMSs Integrated Area Information Management Systems, we must move to a fifth stage. This stage would make the IAIMS an inter-enterprise strategy. The emphasis would be not on information technology or integrative resources, but on how to manage the policy issues related to shared governance. The fifth stage does not involve fundamental new processes. Instead, it involves reapplying processes from stages one through four across organizations. IAIMSs have yet to reach the fifth stage. Some programs extend across regions, but each IAIMS exists within a single enterprise. The goal is to go beyond that.
IAIMSs—The Key to Transforming Biomedicine
If we assume that a stage-five IAIMS is achievable, we can ask what its impact would be on how the health care system works and how the academic enterprise integrates with other components of the health care system. Industry experts say that the current system is nonsustainable and that it must change to survive. Let's examine one model for the health care system of the future, as depicted in Figure 2. There could be a single-entry pathway for all people interested in working in the health sciences—nurses, pharmacists, doctors, etc. They would come into the system and spend one year in “school.” They would learn vocabulary, how to use the computer, and how to interact with people. Those are a set of common skills that each must have. Next, they would serve an apprenticeship that could be in an academic medical center, in a practice across the region, or in an affiliated hospital. The apprentice phase would bring together the functions of the clerkship, the housestaff model, or the clinical portion of a physician assistant or nurse practitioner program. At that juncture, students who wanted to move into the primary care network would require no further training. Others would continue to study the basic sciences to prepare for either basic research or clinical specialties.
Figure 2.
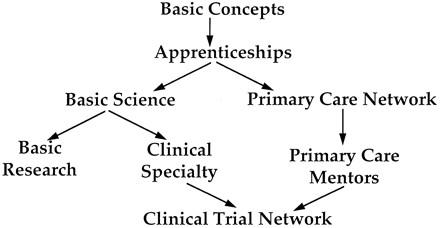
A unified model for incorporating manpower development into the ongoing processes of a regional health care delivery system through just-in-time learning.
This model is not a new idea. What is new is the information technology that would allow us to pursue the model while incorporating rigor into training. We can monitor experience, we can deliver information equally and easily to nearby and remote sites, and we can use simulation to provide just-in-time instruction. After their apprenticeships, the people who selected a primary care track would go into practice. Other individuals would go back to school for training in basic sciences and specific diseases. Supported by the right tools, they all would benefit from a lifelong learning opportunity. In this model, the health care professions would be a part of one system. The clinical specialists and the primary care mentors would provide training opportunities and perform clinical research. This model would eliminate debt ; it would eliminate continuing medical education ; it would eliminate alumni and development ; and it would offer other advantages. Certainly, there are many reasons that the model might not work. I would argue, however, that whatever emerges in the next ten years will be as different from what we do today as is this model. We are moving toward a major paradigm shift in the way we train health scientists.
Information commerce is another opportunity for a paradigm shift. Academic centers produce information, give it to publishers, and buy it back. Information producers need to assume responsibility for making the information artifacts they produce accessible. If this process were in place, and someone accessed a piece of information, the producer could get a credit to access someone else's artifacts. When someone without credits needed to access a producer's data, he or she would pay in dollars. Information producers would then have a new revenue stream to help support the academic component of their endeavor, and the global cost of access to information would be reduced. We might even shift the base of academic promotion to whether anyone reads what a researcher publishes instead of a promotion policy that encourages the production of new journals to publish material that is never read.
Conclusion
Envisioning the future is both fun and provocative, but what are the take-home lessons ? What does it take for an organization to successfully achieve an IAIMS ? First, the informatics component of the organization (information technology, information systems—there are many different names) needs to be at the leadership level of that institution. Being a part of the executive cabinet is the only way to fully understand an organization's business needs. Open, ongoing communication between the business needs and the art-of-the-possible of new technologies is essential to achieving paradigm shifts. Data are a corporate asset and must be handled as such. Different parts of the corporation produce the data, but the corporation as a whole is responsible for their accuracy, for making them accessible, for making them secure, and for credentialing people to access them.
Planning is a core function that involves visioning, consensus, and communication. The planning process has to consider how to achieve the organization's objectives in a way that leverages what has been done, and that focuses on the objectives, not the technology. Processes and systems must be able to scale up to support the enterprise. Cost issues have to be addressed from a perspective of maximizing benefit, not of minimizing cost. Technology is expensive, and inexpensive computing is generally poor computing. Start with an objective, determine the best technology to achieve that objective, and assess the predicted benefit. You then have the data necessary to decide whether it is worth the cost.
Presented at the IAIMS Consortium Symposium, Vanderbilt University, Nashville, TN, September 27, 1996.
Supported in part by National Library of Medicine Grant No. G08-LM05443.
References
- 1.Matheson NW, Cooper JAD. Academic information in the health sciences center : roles for the library in information management. Med Educ. 1982. : 57(Part 2) : 1-93. [DOI] [PubMed] [Google Scholar]
- 2.Lindberg DAB, West RT, Corn M. IAIMS : an overview from the National Library of Medicine. Bull Med Libr Assoc. 1992. : 80 ; 244-6. [PMC free article] [PubMed] [Google Scholar]
- 3.Stead WW, Borden R, Bourne J, et al. The Vanderbilt University fast track to IAIMS : transition from planning to implementation. J Am Med Informat Assoc. 1996. : 3 ; 308-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Stead WW, Bird WP, Califf RM, Elchlepp JG, Hammond WE, Kinney TR. The IAIMS at Duke University Medical Center : transition from model testing to implementation. MD Comput. 1993. : 10 ; 225-30. [PubMed] [Google Scholar]
- 5.Yount RJ, Vries JK, Council CD. The medical archival system : an information retrieval system based on distributed parallel processing. Information Processing and Management. 1991. ; 27 : 1-11. [Google Scholar]
- 6.Creating our Future in the Information Age : Seamless Healthcare Delivery, video 7 min. 26 sec., 1995, Olsen AJ, producer.