

Abstract
The purpose of this article is to investigate the association between the background characteristics of patients with severe fear of dental treatment who frequently avoid dental care and the degree of difficulty in treating them. At the time of initial presentation at a dental phobia clinic, each of 321 subjects was asked to complete the State-Trait Anxiety Inventory, the Dental Anxiety Scale, and a health questionnaire related to phobic objects. Subjects who rejected oral examination with a dental mirror were categorized as being severely difficult to treat, whereas those who were able to undergo examination were categorized as being moderately difficult to treat. In the statistical analysis, assessment items that were correlated with difficulty to treat were designated as independent variables for a logistic regression analysis. In the logistic regression analysis, significant correlations were observed for gender (male > female with adjusted odds ratio, 4.121; 95% CI, 1.96–8.65) and level of trait anxiety (2.401; 1.01–5.73). Male gender and a high trait anxiety were identified as major factors associated with severe dental fear and avoidance.
Key Words: Dental anxiety scale, Dental avoidance, Dental fear, Logistic regression analysis, State-Trait Anxiety Inventory
Individuals with fear of dental treatment (“dental fear”) frequently avoid dental care (“avoidance”) for long periods of time and have a worse oral health–related quality of life than do those without dental fear.1–3 In addition, when individuals with dental fear and avoidance do accept oral examinations, dentists frequently have difficulty performing treatment. Although many studies have investigated dental fear and avoidance,1–6 no studies have examined the background characteristics of the subgroup of patients with severe dental fear and avoidance, which we define as those who reject even intraoral examination with a dental mirror and periodontal pocket examination. Therefore, we investigated the association between the background characteristics of patients with severe dental fear and avoidance and the degree of difficulty in treating them.
METHODS
This study was registered with the Ethics Committee at Tokyo Dental College, Tokyo, Japan (approval No. 300). All patients received humane care in accordance with the ethical guidelines for clinical research published by the Ministry of Health, Labour, and Welfare of Japan. Written informed consent to participate in this study was obtained from all 321 patients. All of the patients enrolled in the study had long-term dental fear and avoidance and had been referred to the Relaxation Dental Outpatient Clinic for Dental Phobia at Tokyo Dental College Suidobashi Hospital, Tokyo, Japan, for an initial examination between April 2007 and March 2010.
At the time of the initial examination, a health questionnaire was given to each subject to complete. The survey included items related to age, gender, and duration of dental treatment avoidance, as well as to whether or not they had any “previous experience of fainting during dental treatment,” “childhood experience of forced dental treatment,” “other common phobias,” “parents or siblings with dental fear,” or “a mental disorder.” In addition, the participants were asked to respond “yes” or “no” to whether they feared “the smell of medicine,” “the sound of teeth being drilling,” “the injection of anesthetic in the mouth,” “having an impression taken,” “having tools inserted into the mouth,” or “conversing with the dentist.” In addition, the State-Trait Anxiety Inventory (STAI)7 was used to measure the degrees of state and trait anxiety, and the Dental Anxiety Scale (DAS)8 was used to measure the extent of dental anxiety. Males with STAI trait and state anxiety scores of at least 44 and 41, and females with STAI trait and state anxiety scores of at least 45 and 42, respectively, or subjects who scored at least 15, irrespective of gender, on the DAS were categorized as having high anxiety.
At the initial consultation, an intraoral examination was carried out and grade of dental fear determined by 2 dentists and 1 dental hygienist. Difficult to treat was determined on the basis of the participants' capability to appropriately open their mouths and cooperate with oral examination using a dental mirror and periodontal pocket measurement with a periodontal probe. Patients who rejected oral examination, periodontal pocket examination, or both were classified as being severely difficult to treat. It was expected these patients' desensitization treatment would become more difficult.9 Those who were cooperative for both types of examination were classified as being moderately difficult to treat.
SPSS statistical software (version 19) was used to analyze the data. Age and duration of dental avoidance are expressed as mean ± standard deviation, gender as male or female, trait and state anxiety as high anxiety or not, and DAS score as at least 15 or not. First, statistical differences between patients with difficulty to treat in the severe group and moderate group on the 17 items were tested. Student's t test was used to assess the comparison between 2 groups in age and duration of dental avoidance, and the chi-square test was used to assess the comparison between all other assessment items. Next, the items with p values greater than .05 were rejected. Assessment items with p values less than .05 were used as independent variables in a logistic regression analysis. The logistic regression analysis was carried out with the significant assessment items as the independent variables and difficulty to treat (severe or moderate) as the dependent variable.
RESULTS
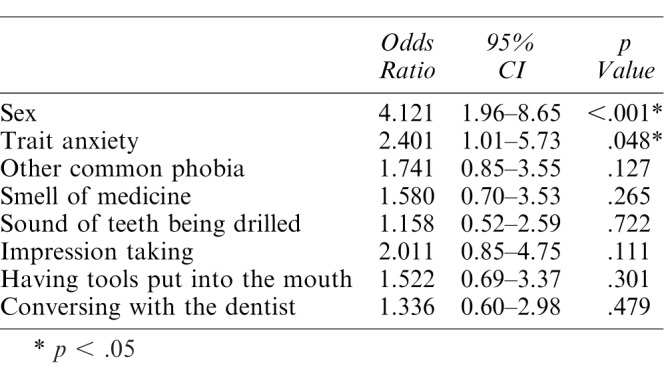
Forty-eight patients (15.0%) were classified as being severely difficult to treat, and 273 patients (85.0%) were classified as being moderately difficult to treat. The differences between 2 groups are shown in Tables 1, 2, and 3. Nine items were rejected for further analysis. Eight assessment items were found to be statistically different between the severely and moderately difficult to treat groups: gender (Table 1); presence or absence of another common phobia, fear of the smell of medicine, fear of the sound of teeth being drilled, fear of having an impression taken, fear of having tools inserted into the mouth, and fear of conversing with the dentist (Table 2); and level of trait anxiety (Table 3). Logistic regression analysis was performed with these 8 items as the independent variables and difficult to treat (severe or moderate) as the dependent variable, and significant correlations were observed for gender and level of trait anxiety (Table 4). The adjusted odds ratios for gender and level of trait anxiety were 4.121 (95% CI: 1.96–8.65) and 2.401 (95% CI: 1.01–5.73), respectively.
Table 1.
Comparison of the Severe Group and the Moderate Group: Background of the Patients

Table 2.
Comparison of the Severe Group and the Moderate Group: Questionnaire
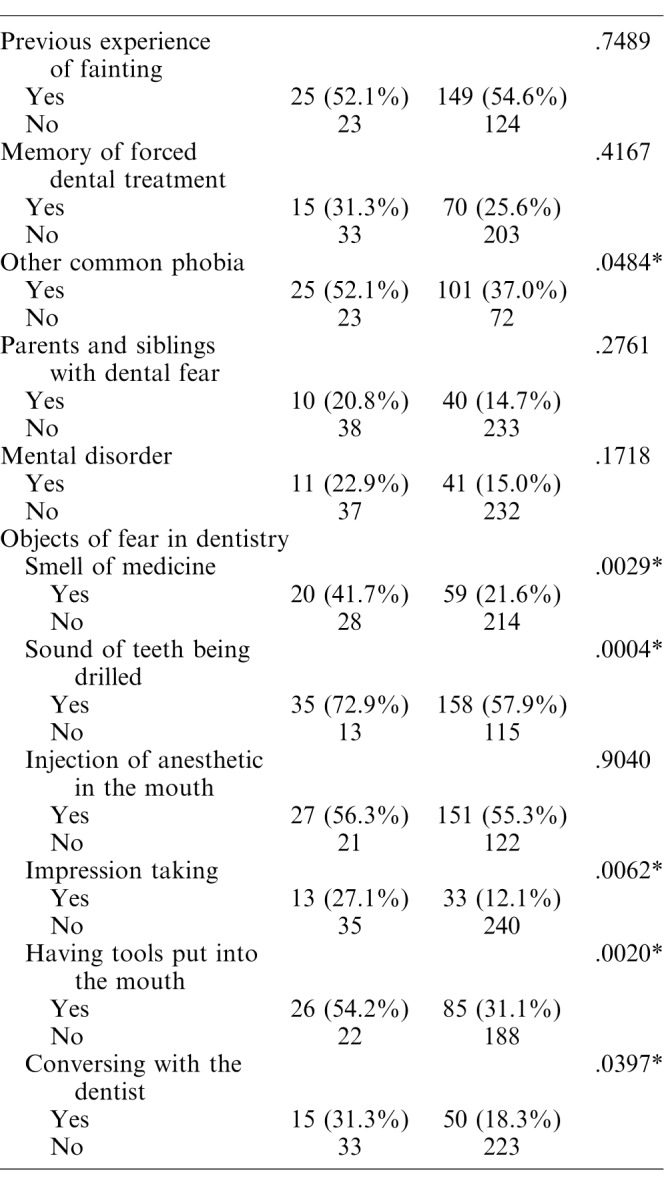
Table 3.
Comparison of the Severe Group and the Moderate Group: STAI and DAS†
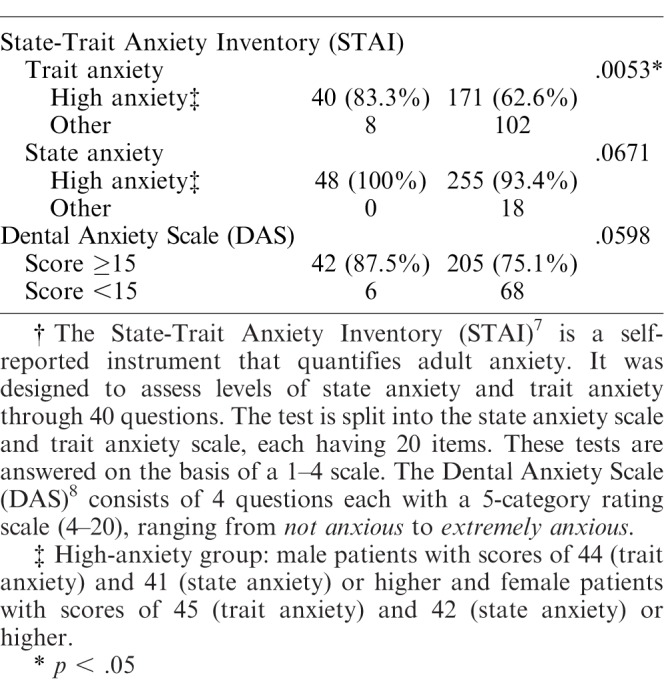
Table 4.
Factors Analyzed for Severe Dental Fear and Avoidance (Logistic Regression Analysis)
DISCUSSION
The results of the present study revealed that male gender (adjusted odds ratio: 4.121) and high trait anxiety (adjusted odds ratio: 2.401) were major factors underlying severe dental fear and avoidance in the study cohort.
It has been estimated that approximately 30% of the population has some kind of dental fear.4,5 When a score of 15 or higher on the DAS is set as the diagnostic criteria for identifying dental fear and avoidance, incidence rates of 5.4%4 and 4.2%6 have been reported. Dental phobia has been reported as the most prevalent phobia.10 In terms of gender, dental fear is reported to be more common in women than in men.10–12 In fact, women accounted for 76% of the participants in the present study. Although women represent a large majority of the total population of patients with dental fear, a greater proportion of men than women were classified as being severely difficult to treat in the present study, which is presumably the result of factors unique to males. Generally, compared with women, men pay fewer visits to the dentist to receive dental care13 and have fewer opportunities to visit clinics. Therefore, more men than women may be classified as being severely difficult to treat because few male patients visit dental clinics for more easily treated conditions.
An unpleasant experience during dental treatment may trigger dental fear, which is then expressed as dental avoidance.12–14 However, Armfield15 reported that cognition (rather than past experience) is a greater causal factor underlying dental fear. Eli et al16 also pointed out the significance of trait anxiety as well as of environmental factors for the development of dental fear. Furthermore, Pohjola et al17 postulated that the development of dental fear is an intrinsic problem and that many patients with dental fears also have psychological disorders such as depression and anxiety. In other words, in addition to the effects of past emotional traumas, heritable and endogenous factors are also suggested as causal factors for the development of dental fear and avoidance. The results of the present study revealed that having high trait anxiety, which is a congenital factor,18 is associated with more severe dental avoidance. Therefore, intrinsic factors, in addition to past experiences, should be considered not only as causes of dental fear and avoidance but also as factors affecting the degree of dental fear.
No significance was observed for the level of state anxiety and DAS score in the present study. If the present study had a larger sample size, level of state anxiety and DAS scores might have reached significance.
Psychological treatments such as cognitive behavioral therapy have been recommended as treatments for dental fear and avoidance.19,20 The efficacies of these treatments, which attempt to help the participant understand and overcome past inappropriate coping patterns, have been confirmed in comparisons with drug-based methods of behavioral control.20,21 However, cognitive behavioral therapy is unsuccessful in 25% of cases and is therefore an incomplete solution.22 In severe dental fear and avoidance, although past emotional trauma may be involved, a complex range of other factors of both heritable and endogenous causes is highly likely to be involved. Therefore, the treatment of severe dental fear and avoidance requires more advanced solutions such as the combination of behavioral and drug therapies in some patients.
The present study was an assessment conducted only at the time of initial presentation at the clinic. In future studies, the details of the treatment progress and desensitization should be investigated. Results may suggest which patients are most suited to behavioral versus pharmacologic treatment.
CONCLUSIONS
Male gender and high trait anxiety were identified as major factors underlying severe dental fear and avoidance in a Japanese population.
ACKNOWLEDGMENTS
We thank all of the staff at the Relaxation Dental Outpatient Clinic for Dental Phobia at Tokyo Dental College Suidobashi Hospital for their assistance in this study.
REFERENCES
- 1.McGrath C, Bedi R. The association between dental anxiety and oral health-related quality of life in Britain. Community Dent Oral Epidemiol. 2004;32:67–72. doi: 10.1111/j.1600-0528.2004.00119.x. [DOI] [PubMed] [Google Scholar]
- 2.Mehrstedt M, John MT, Tonnies S, Micheelis W. Oral health-related quality of life in patients with dental anxiety. Community Dent Oral Epidemiol. 2007;35:357–363. doi: 10.1111/j.1600-0528.2007.00376.x. [DOI] [PubMed] [Google Scholar]
- 3.Ng SKS, Leung WK. A community study on the relationship of dental anxiety with oral health status and oral health-related quality of life. Community Dent Oral Epidemiol. 2008;36:347–356. doi: 10.1111/j.1600-0528.2007.00412.x. [DOI] [PubMed] [Google Scholar]
- 4.Hakeberg M, Berggren U, Carlsson SG. Prevalence of dental anxiety in an adult population in a major urban area in Sweden. Community Dent Oral Epidemiol. 1992;20:97–101. doi: 10.1111/j.1600-0528.1992.tb00686.x. [DOI] [PubMed] [Google Scholar]
- 5.Wisoff TE, Vassend O, Asmyhr O. Dental anxiety, utilization of dental services, and DMFS status in Norwegian military recruits. Community Dent Health. 1995;12:100–103. [PubMed] [Google Scholar]
- 6.Moore R, Birn H, Kirkegaard E, Brodsgaard I, Scheutz F. Prevalence and characteristics of dental anxiety in Danish adults. Community Dent Oral Epidemiol. 1993;21:292–296. doi: 10.1111/j.1600-0528.1993.tb00777.x. [DOI] [PubMed] [Google Scholar]
- 7.Spielberger CD, Gorsuch RL, Lushene RE. State-Trait Anxiety Inventory: Manual for the State-Trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologists Press;; 1970. [Google Scholar]
- 8.Corah NL. Development of a Dental Anxiety Scale. J Dent Res. 1969;48:596. doi: 10.1177/00220345690480041801. [DOI] [PubMed] [Google Scholar]
- 9.Saita N, Fukuda K, Koukita Y, Ichinohe T, Yamashita S. Relationship between gagging severity and its management in dentistry. J Oral Rehabil. 2013;40:106–111. doi: 10.1111/joor.12014. [DOI] [PubMed] [Google Scholar]
- 10.Oosterink FMD, de Jongh A, Hoogstraten J. Prevalence of dental fear and phobia relative to other fear and phobia subtypes. Eur J Oral Sci. 2009;117:135–143. doi: 10.1111/j.1600-0722.2008.00602.x. [DOI] [PubMed] [Google Scholar]
- 11.Weinstein P, Smith TA, Bartlett RC. A study of the dental student-patient relationship. J Dent Res. 1973;52:1287–1292. doi: 10.1177/00220345730520062201. [DOI] [PubMed] [Google Scholar]
- 12.Domoto PK, Weinstein P, Melnick S, et al. Result of a dental fear survey in Japan: implications for dental public health in Asia. Community Dent Oral Epidemiol. 1988;16:199–201. doi: 10.1111/j.1600-0528.1988.tb01753.x. [DOI] [PubMed] [Google Scholar]
- 13.Skaret E, Raadal M, Kvale G, Berg E. Gender-based differences in factors related to non-utilization of dental care in young Norwegians: a longitudinal study. Eur J Oral Sci. 2003;111:377–382. doi: 10.1034/j.1600-0722.2003.00072.x. [DOI] [PubMed] [Google Scholar]
- 14.De Jongh A, Aartman IHA, Brand N. Trauma-related phenomena in anxious patients. Community Dent Oral Epidemiol. 2003;31:52–58. doi: 10.1034/j.1600-0528.2003.00025.x. [DOI] [PubMed] [Google Scholar]
- 15.Armfield JM. Towards a better understanding of dental anxiety and fear: cognitions vs. experiences. Eur J Oral Sci. 2010;118:259–264. doi: 10.1111/j.1600-0722.2010.00740.x. [DOI] [PubMed] [Google Scholar]
- 16.Eli I, Uziel N, Baht R, Kleinhauz M. Antecedent of dental anxiety learned responses versus personality traits. Community Dent Oral Epidemiol. 1997;252:33–37. doi: 10.1111/j.1600-0528.1997.tb00932.x. [DOI] [PubMed] [Google Scholar]
- 17.Pohjola V, Mattila AK, Joukamaa M, Lahti S. Anxiety and depressive disorders and dental fear among adults in Finland. Eur J Oral Sci. 2011;119:55–60. doi: 10.1111/j.1600-0722.2010.00795.x. [DOI] [PubMed] [Google Scholar]
- 18.Fuentes D, Gorenstein C, Hu L.W. Dental anxiety and trait anxiety: an investigation of their relationship. Br Dent J. 2009;206:E17. doi: 10.1038/sj.bdj.2009.253. [DOI] [PubMed] [Google Scholar]
- 19.Kvale G, Berggren U, Milgrom P. Dental fear in adults: a meta-analysis of behavioral interventions. Community Dent Oral Epidemiol. 2004;32:250–264. doi: 10.1111/j.1600-0528.2004.00146.x. [DOI] [PubMed] [Google Scholar]
- 20.Wide Boman U, Carlsson V, Westin M, Hakeberg M. Psychological treatment of dental anxiety among adults: a systematic review. Eur J Oral Sci. 2013;121:225–234. doi: 10.1111/eos.12032. [DOI] [PubMed] [Google Scholar]
- 21.Berggren U. Linde A. Dental fear and avoidance: a comparison of two modes of treatment. J Dent Res. 1984;63:1223–1227. doi: 10.1177/00220345840630101201. [DOI] [PubMed] [Google Scholar]
- 22.Smith TA, Kroeger RF, Lyon HE. Evaluating a behavioral method to manage dental fear. J Am Dent Assoc. 1990;121:525–539. doi: 10.14219/jada.archive.1990.0197. [DOI] [PubMed] [Google Scholar]