

Abstract
INTRODUCTION:
The main aim of this study was to explore the socioeconomic determinants of health-care and emotional needs among older adults.
MATERIALS AND METHODS:
In this cross-sectional study, 350 older adults were randomly selected from five geographical regions in Isfahan, 2016. A self-administered checklist was employed to collect health-care and emotional need data among older adults residing day-care centers. Data were analyzed using logistic regression through STATA/SE (version 14).
RESULTS:
The highest proportion of older adults lived with income 285–855 USD monthly and insured by social security insurance. Illiteracy, loneliness, and low level of income were more prevalent among female older adults than male ones. The emotional needs of single/widow (odds ratio [OR] = 0.299), divorced (OR = 0.133) older people, not having children (OR = 0.811) or grandchildren (OR = 0.684), and illiterates (OR = 0.689) were discovered to be lower than their counterpart groups. As the elderly got older, their health-care needs were met more. Older adults covered by military insurance have their health-care needs met as much as 21% (OR = 1.215) greater than social security insurance.
CONCLUSIONS:
Regarding health-care needs, economic and monetary factors are still important in meeting this type of needs as well as education and social insurance. While regarding emotional needs, nonmonetary and noneconomic factors, including social network, are important determinants for the satisfaction of emotional needs.
Keywords: Needs assessment, older adults, socioeconomic determinants
Introduction
Need has been defined as an essential factor in normal development and operation of human being,[1] with various meanings in different populations. One population is the older adults, whose needs have been considered significantly.[2] Since aging is a process with psychological and social aspects,[3,4] the older adults can have various needs. Health, economic, emotional, spiritual, and educational cares are some of their most important needs. A study investigating the needs of the older adults in Isfahan using the multimethod has listed theses needs as their essential needs: health, emotional, cultural, recreational, and supportive needs.[5]
Population aging is a phenomenon resulting in some health-related problems all over the world, and consequently, the prediction and preparation of health services for them requires a comprehensive measurement of their care needs.[6] As such, since aging is accompanied by several diseases and chronic disabilities such as cardiovascular diseases, various cancers, cognitive deficiencies, and Alzheimer's diseases,[7,8] health care has always been considered as an essential need for older people. Cohen considers health care as an essential need for older people, the absence of which can cause suffering.[9] On the other hand, meeting their health-care needs is a teleological objective and can make life better.[10] Park et al. stated that low socioeconomic level can play an important role in health-care needs of older people, especially in the deteriorating health situation.[11]
Researches have indicated that different factors such as socioeconomic status,[12] age, nationality,[13] education, marital status, economic status, emotional support,[14] transformation of extended family to nuclear family, women participation in workforce, and tendency toward living alone[15] can affect their health-care needs.
On the other hand, factors such as somatic risks and reduction in social relationships can affect the older people's emotional welfare[16] so that an older people's social network – having relationships with spouses, friends, and relatives – affects their emotional life. In Ghasemi et al. study of Tehran elderly's perception of their needs, the lack of spouse and children for reasons such as death or independence of them can lead to a reduction in social relationships of the elderly, which results in deprivation of emotional and mental support and ultimately loneliness in the elderly.[17] It should also be considered that paying attention to emotional needs plays an important role in taking care of older adults.[18]
Compared to the western societies, Iran has a younger population, but the phenomenon of population aging has begun in Iran since a few decades ago.[4] Older individuals represent the fastest growing segment of the population in Iran.[17,18] It is estimated that the population of people aged >60 years in Iran will have increased from 9.3 in 2016 to 20% by 2020. Isfahan is one of the largest urban areas in Iran, with a population of around 5.2 million within the city and metropolitan area. There was approximately 10.3% of people in Isfahan aged >60 years in 2016.[19] In general, it seems that in developing countries, health system accompanied with three challenges, i.e. disease, loneliness, and how old people lives.[20] “Therefore, preparedness of policy makers to meet older adults issues, moving from hospitalized care to home care as well as increased responsibility of community and government towards elderly, are among the necessity of addressing the healthcare and emotional needs”. Regarding the continuing attention to the role of the social determinants of health in health of communities, this study was conducted to determine the main socioeconomic factors of health-care and emotional needs of older people. Namely, we tried to consider other social and emotional needs beyond the merely focusing on economic needs of the older adults.
Materials and Methods
Study design
This cross-sectional study was conducted in Isfahan older population from September to November 2016.
Setting and sample
The sample consisted of 340 participants admitted to Isfahan's day-care centers, who were selected through stratified random sampling. Day-care centers in Isfahan were divided into five geographical regions (north, south, east, west, and central) in which older adults were randomly selected. All the participants were interviewed by trained investigators from 15 municipal regions in Isfahan which were randomly selected from 5 geographical regions of north, south, east, west, and central. The inclusion criterion was age 60 years and older. According to the medical records of older adults, individuals with severe and moderately severe dementia were excluded from the study due to difficulty in filling checklist.
Measurements
A self-structured checklist about older adults' needs was developed based on five focus group discussions with older people. The checklist was derived from five focus groups and contained 20 questions which covered 4 dimensions of older people's needs, including emotional needs, health-care needs, cultural and recreational needs, and supportive needs. This checklist was reviewed by experts and its face and content validity were proven by a panel of experts from 10 various disciplines (gerontology, health psychology, medical sociology, and social worker). The Cronbach's α was 0.87 that showed a high degree of internal consistency and homogeneity between items. The mean of series technique was used for handling 21 missing cases of emotional needs' variable.
Definition of variables
In the current study, we selected health-care and emotional needs as binary variables that have been derived from above-mentioned checklist. Health-care needs' domain consists of 5 questions including(1) access to general physician, (2) access to specialist physician, (3) purchasing required medicine, (4) purchasing rehabilitation devices, and (5) access to diagnostic or laboratory services. Moreover, emotional domain consists of three questions including (1) relation with spouses, (2) relation with children and grandchild, and (3) relation with relatives. Each of the questions was rated in two categories describing met need (=1) and unmet need (=0). Then, five and three questions in terms of health-care and emotional needs were added together, respectively. Finally, to infer about met or unmet need, median was used as a cutoff point. This way, we had a binary variable for health-care and emotional needs comprising of above median as a “met need” and below median as an “unmet need” of health-care and emotional needs, and all the subsequent analyses were conducted on the first category (met need).
To determine the factors that affect older adult's health-care and emotional needs, potential socioeconomic factors were extracted from several related studies,[21,22,23] including aging phases (the young-old [aged 65–74], the middle-old [aged 75–84], and the old-old [aged over 85],[24] marital status, educational level, monthly family income, place of residence (central, north, east, west, and south districts), type of insurance (social security, Iranian health, and others), number of children, and number of grandchild.
Data analysis
Descriptive analyses were calculated in terms of frequencies with percentages. Responses were tabulated for the level of needs rated by older adults. Considering the fact that, in this study, the health-care and emotional needs were binary variable (whether the needs were met or not), we used binary logistic regression. The distribution of data was parametric according to the Kolmogorov–Smirnov test. The odds ratio (OR) and 95% confidence intervals were calculated for each determinant variable with a significant level of 0.05. Pearson's χ2, log-likelihood, and pseudo R2 were used to assess logistic regression goodness-of-fit. All data were analyzed by STATA/SE (version 14; Stata Corporation, College Station, TX, USA).
Ethical consideration
This study received the required ethics approval from Research Ethics Committee with this number: IR. MUI. REC.1395.2.029.
Results
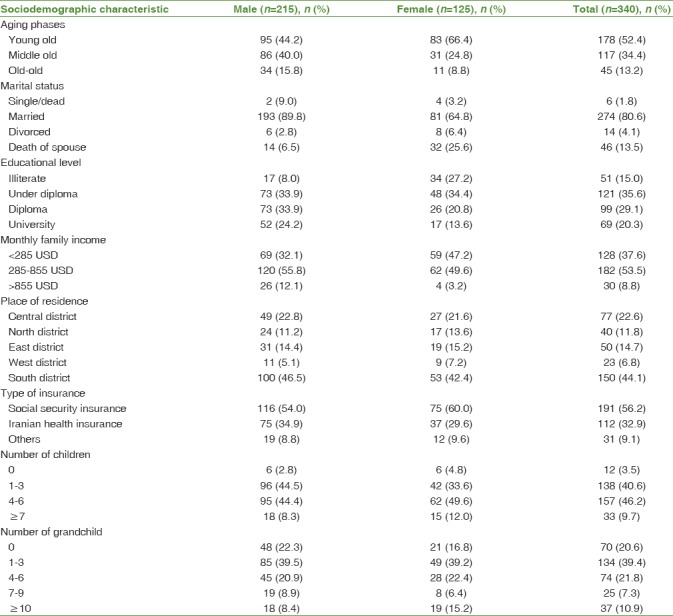
The sociodemographic features of older adults have been shown in Table 1. Out of 340 older adults, 49.5% have had diploma and higher educational level. Illiteracy (34%) and loneliness (4%) were more prevalent among female older adults than male ones. Regarding income, 53.5% of older adults lived with income between 285 and 855 USD monthly. In comparison to females, male older adults have had higher level of income. The most of studied older adults were residence in south district (44%). One hundred and ninety-one older adults were insured by social security insurance, representing the highest proportion. The most of older adults have had 4–6 (46%) and 1–3 (39%) children and grandchildren, respectively.
Table 1.
Sociodemographic features of the study population
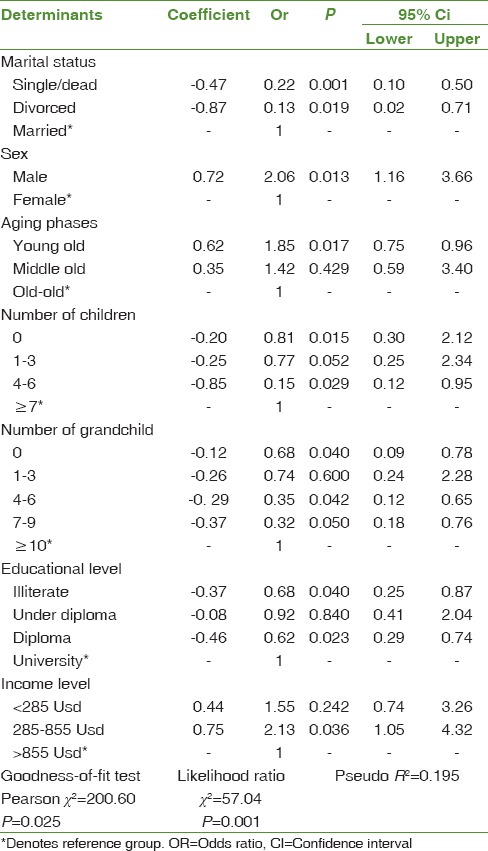
According to the significance of OR, single/widow and divorced older adults have had lower ratio of met emotional needs than married older adults as much as 23% and 13%, respectively. The emotional needs of older men have been met almost twice higher than older women. The probability of meeting emotional needs among younger elderly people was 85% higher than the oldest. Those without children and without grandchildren have had lower ratios of meeting their emotional needs (81% and 68%) in comparison to older adults with ≥7 children and ≥10 grandchildren, respectively. In fact, the higher the number of children and grandchildren the higher level of met emotional needs. Moreover, emotional needs in illiterate older adults were been met as much as 68% and 63% lower than the older adults with university level and diploma, respectively. The emotional needs of older adults with 285–855 USD income were been met almost twice higher than older adults with >855 USD. Pearson's χ2 goodness-of-fit test and likelihood ratio proposed no evidence of lack of fit (P > 0.05). Regarding pseudo R2, 19.5% of the variance of emotional needs can be explained by included variables in the logistic model [Table 2].
Table 2.
Logistic regression of met emotional needs and related determinants in older people in isfahan in 2016
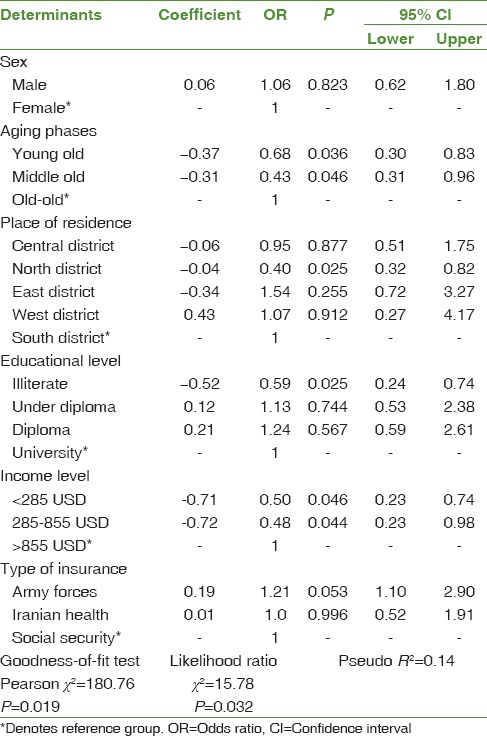
As Table 3 shows, the health-care needs of young and middle-aged people have been met 68% and 43% lower than much older ones, respectively. Result demonstrated that older adults living in north districts of Isfahan have had 40% lower ratio of health-care needs in comparison with older adults where reside in south districts. Moreover, health-care needs in illiterate older adults had been met as much as 60% lower than the older adults with university level. The health-care needs of older people' income <285 USD and income 285–855 USD have been met 50% and 48% lower than older adults with >855 USD, respectively. Finally, older adults covered by military insurance have met their health-care needs as much as 21% greater than social security insurance. Pearson's χ2 test and likelihood ratio indicated the goodness-of-fit of the model (P < 0.05). Regarding pseudo R2, about 15% of the variance of health-care needs can be explained by included variables in the logistic model.
Table 3.
Logistic regression of met health-care needs and related determinants in older people in Isfahan in 2016
Discussion
Understanding the needs of older adults is among their health and emotional care needs, and the factors affecting the provision of services and health care are of utmost importance. According to the findings of the present study, health-care needs among much older people who are living in regions with higher socioeconomic status, have received academic education, have a monthly income higher than 855 USD, and are insured by the social insurances of the military are met in a higher level. Wastesson et al. found that the level of education related with outpatient and dental services.[25] Health-care needs among high-income and educated groups shows that these groups, as a result of the higher accessibility of health services and their higher level of education[26] are met higher than other groups.
In Iran, the needs of people who are insured by the military, because of the health-care facilities provided by the organization including complementary insurances and exclusive hospitals and clinics, have a higher probability to be met in comparison with the people insured by other insurance companies. Afzali and Pourreza found that only about 4% of the total social security contributions of Tehran are elderly, accounting for >37% of total health-care costs.[27] Bahadori et al. studied the quality of services provided to veterans referred to a branch of the armed forces and their analysis revealed that exception-related staffs in whole dimensions were upward on the current situation. The highest mean of scores in expectation sector was related to the assurance of service warranty.[28]
Ghasemi et al. demonstrated that emotional need is the most demanded by Iranian elderly.[17] The emotional needs in young old, male, married, having children and grandchildren with academic education, and a monthly income between 270$ and 540$ are met more effectively. Alice et al. showed that mental needs of women are more likely to be met than that of men.[29] Since the nature of emotional needs is related to social relationships, supports, and networks, it seems that in Iran, the wideness of familial networks and relationships, as a result of the increased quantity of relationships through more children and grandchildren, leads to a higher level of satisfaction in terms of emotional needs. Due to the special cultural characteristics dominant in Iran, men enjoy a wider and more comprehensive communicative range, and as compared to women, the intra- and inter-group relationships are more available for them, so it seems that their emotional needs are also met more effectively. Furthermore, young old as compared to older elders, due to their bodily and physical conditions, are more prone to communicate with their family and relatives and can participate in social ceremonies, so their emotional needs are met more effectively.
In comparison with other studies, the present study showed that there are differences among various age groups of older people, and it seems that as they age, the rate of diseases and disabilities increases. Although we found that the health-care needs of very older adults are met more effectively than younger elders, this was not confirmed in Li et al.[30] The reason for this result can be that health-care services are not specialized in Iran and the only elders whose needs are met are those with an obvious disease. It seems that elders with higher education can satisfy their health-care needs more effectively. This has been pointed out in the related literature and has been confirmed in the present study.[31,32] Since the elders with higher education have better access to information resources and have a higher purchase power to meet their health-care needs, generally it seems that higher socioeconomic status is accompanied with higher level of needs met.[12] In confirming Bookman and Kimbrel study,[33] the present study showed that people living in richer regions of Isfahan who earn more income have their needs met more effectively. As such, military insurance, because of their higher health-care service coverage and their lower prices, can meet more health-care needs.
Regarding emotional needs, the present study showed that this need in men is estimated to be higher than women (about two-fold). It seems that, according to the Iranian subculture about the older people, generally male elders, as compared to female ones, are consumers rather than givers and marital status plays an important role here. As you may know, older women are an important resource for providing health-care services for their husbands because they are younger and have a longer life expectancy.[34] While men, due to several chronic diseases, are dependent on their wives. This leads to fulfill their emotional needs. It should also be taken into consideration that because of cultural reasons, older men, compared to older women, have a higher chance to get married after the death of their wives. Since a wife can increase the chances of emotional need satisfaction, older women have to spend their widowhood period in solitude. According to social exchanges theory, people must reach a harmony in social interactions.[35] When a person gets old, his/her participation in the social network decreases. Our study showed that older elders, as compared to other younger elders, have a lower chance to satisfy their emotional needs. It seems that when one's partner dies, he/she will withdraw from the social network. On the other hand, an increase in the possibility to have chronic diseases can affect their communication in the social network.
Iran community features special cultural characteristics and families that are transferring from extended families to nuclear families. Given the growth rate of births during the last decades in Iranian families, a number of children and consequently grandchildren are high and their education and income level are low. It seems that the older people, due to their agricultural knowledge, customs, traditions, and religion, enjoy an elevated status in their family. On the other hand, they are dependent on the financial aids from their children. This can pave the way for the satisfaction of their emotional needs significantly.
Conclusions
In total, according to the findings obtained from this research, it can be said that the policies related to meeting the older people's needs should consider different programs and policies given the type of their needs. More specifically, in terms of health-care needs, economic and monetary factors are still important in meeting this type of needs as well as education and social insurance. While regarding the emotional needs, nonmonetary and noneconomic factors, including the width of the social networks, are important determinants for the satisfaction of their needs. Therefore, by considering the type of needs (i.e., health care or emotional) and their related determinants, social planners who are trying to meet the older people's needs can adopt appropriate economic, social support, and social security policies.
Limitation and strength
The present work had one main limitation: difficulty in accessing and communicating with the older people. We tried to interview the older adults patiently and in an appropriate time. To the best of our knowledge, no study has taken the need assessment as we did in this study to reveal health-care and emotional needs within Iranian older adults.
Financial support and sponsorship
This study was financially supported by the Social Determinants of Health Research Center, Isfahan University of Medical Sciences, IR.MUI.REC.1395.2.295029.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We would like to that all older adults for participating to this study.
References
- 1.Brewster-Smith M, Fitzgerald R. Rushcutters Bay, Australia: Pergamon Press; 1977. Metapsychology, Politics and Human Needs. Hum Needs Politice; pp. 124–41. [Google Scholar]
- 2.Wijk H, Grimby A. Needs of elderly patients in palliative care. Am J Hosp Palliat Care. 2008;25:106–11. doi: 10.1177/1049909107305646. [DOI] [PubMed] [Google Scholar]
- 3.Inui TS. The need for an integrated biopsychosocial approach to research on successful aging. Ann Intern Med. 2003;139:391–4. doi: 10.7326/0003-4819-139-5_part_2-200309021-00002. [DOI] [PubMed] [Google Scholar]
- 4.Rashedi V, Gharib M, Yazdani AA. Social participation and mental health among older adults in Iran. IRJ. 2014;12(1):9–13. [Google Scholar]
- 5.Amini Rarani M, Nosratabadi M. Age Int. Isfahan University of Medical Sciences: Social Determents of Health Research Center, 2017 Contract No: 295029; 2017. Assessing the met and unmet needs among elderly people in Isfahan, Iran: A mixed method. [Google Scholar]
- 6.Girling LM, Morgan LA. Older women discuss planning for future care needs: An explanatory framework. J Aging Health. 2014;26:724–49. doi: 10.1177/0898264314529330. [DOI] [PubMed] [Google Scholar]
- 7.Hayes N. Hazzard's Geriatric Medicine and Gerontology. McGraw-Hill; 2010. pp. 10–1. [DOI] [PubMed] [Google Scholar]
- 8.Rashedi V, Asadi-Lari M, Foroughan M, Delbari A, Fadayevatan R. Prevalence of disability in Iranian older adults in Tehran, Iran: A population-based study. J Health Soc Sci. 2016;1:251–62. [Google Scholar]
- 9.Beran D. Needs and needs assessments: A gap in the literature for chronic diseases. SAGE Open. 2015;5:1–10. [Google Scholar]
- 10.Asadi-Lari M, Packham C, Gray D. Need for redefining needs. Health Qual Life Outcomes. 2003;1:34. doi: 10.1186/1477-7525-1-34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Park S, Kim B, Kim S. Poverty and working status in changes of unmet health care need in old age. Health Policy. 2016;120:638–45. doi: 10.1016/j.healthpol.2016.03.004. [DOI] [PubMed] [Google Scholar]
- 12.Lindstrӧm C, Rosvall M, Lindstrӧm M. Socioeconomic status, social capital and self-reported unmet health care needs: A population-based study. Scand J Public Health. 2017;45:212–21. doi: 10.1177/1403494816689345. [DOI] [PubMed] [Google Scholar]
- 13.Axén E, Lindström M. Ethnic differences in self-reported lack of access to a regular doctor: A population-based study. Ethn Health. 2002;7:195–207. doi: 10.1080/1355785022000042024. [DOI] [PubMed] [Google Scholar]
- 14.Ahs AM, Westerling R. Health care utilization among persons who are unemployed or outside the labour force. Health Policy. 2006;78:178–93. doi: 10.1016/j.healthpol.2005.10.010. [DOI] [PubMed] [Google Scholar]
- 15.Liu YH, Chang HJ, Huang CC. The unmet activities of daily living (ADL) needs of dependent elders and their related factors: An approach from both an individual-and area-level perspective. Inter J Gerontol. 2012;6:163–8. [Google Scholar]
- 16.Hahn J, Oishi S. Psychological needs and emotional well-being in older and younger Koreans and Americans. Pers Individ Differ. 2006;40:689–98. [Google Scholar]
- 17.Ghasemi S, Mohammadi NK, Shahboulaghi FM, Ramezankhani A. Older adults' perception of their needs in Tehran: A cry for emotional and social support. Global J Health Sci. 2016;9:134. [Google Scholar]
- 18.McCabe MP, Davison T, Mellor D, George K. Barriers to care for depressed older people: Perceptions of aged care among medical professionals. Int J Aging Hum Dev. 2009;68:53–64. doi: 10.2190/AG.68.1.c. [DOI] [PubMed] [Google Scholar]
- 19.Afshar PF, Asgari P, Shiri M, Bahramnezhad F. A review of the Iran's elderly status according to the census records. Galen Med J. 2016;5:1–6. [Google Scholar]
- 20.Mousavi SM, Haghi M, Manshadi MG. Iran's health system and readiness to meet the aging challenges. Iran J Public Health. 2015;44:1716–7. [PMC free article] [PubMed] [Google Scholar]
- 21.Keyvanara M, Hosseini SM, Emami P. Social support and diabetes control: A study among patients admitted to specialized clinic of Dr. Gharazi hospital in Isfahan. Med Arh. 2012;66:24–7. doi: 10.5455/medarh.2012.66.24-27. [DOI] [PubMed] [Google Scholar]
- 22.Miller WR, Bakas T, Buelow JM. Problems, needs, and useful strategies in older adults self-managing epilepsy: Implications for patient education and future intervention programs. Epilepsy Behav. 2014;31:25–30. doi: 10.1016/j.yebeh.2013.11.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Charles ST, Carstensen LL. Social and emotional aging. Annu Rev Psychol. 2010;61:383–409. doi: 10.1146/annurev.psych.093008.100448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Rhee H, Jang KS, Park JM, Kang JS, Hwang NK, Kim IY, et al. Short- and long-term mortality rates of elderly acute kidney injury patients who underwent continuous renal replacement therapy. PLoS One. 2016;11:e0167067. doi: 10.1371/journal.pone.0167067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Wastesson JW, Fors S, Parker MG, Johnell K. Inequalities in health care use among older adults in sweden 1992-2011: A repeated cross-sectional study of swedes aged 77 years and older. Scand J Public Health. 2014;42:795–803. doi: 10.1177/1403494814557150. [DOI] [PubMed] [Google Scholar]
- 26.van Doorslaer E, Wagstaff A, van der Burg H, Christiansen T, De Graeve D, Duchesne I, et al. Equity in the delivery of health care in Europe and the US. J Health Econ. 2000;19:553–83. doi: 10.1016/s0167-6296(00)00050-3. [DOI] [PubMed] [Google Scholar]
- 27.Afzali A, Pourreza A. Tehran: Social Security Organization Research Institute; 2000. The Combination of Disease, Average Length of Stay and Cost Estimates of Treatment Among Elderly of Social Security, Tehran. [Google Scholar]
- 28.Bahadori M, Zaboli R, Ghanbari A. Quality of services provided to veterans referred to a branch of the armed forces in Hamadan. Iran J War Public Health. 2013;6:44–50. [Google Scholar]
- 29.Villatoro AP, Mays VM, Ponce NA, Aneshensel CS. Perceived need for mental health care: The intersection of race, ethnicity, gender, and socioeconomic status. Soc Mental Health. 2018;8:2–7. doi: 10.1177/2156869317718889. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Li IC, Fann SL, Kuo HT. Predictors of the utilization of long-term care (LTC) services among residents in community-based LTC facilities in Taiwan. Arch Gerontol Geriatr. 2011;53:303–8. doi: 10.1016/j.archger.2010.11.009. [DOI] [PubMed] [Google Scholar]
- 31.Chen C. National Chung-Cheng University, Department of Social Work Thesis; 2006. The Long-Term Care Policy in Taiwan: From The Perspectives of Elderly Living Arrangement and Unmet Needs. [Google Scholar]
- 32.Otero A, de Yébenes MJ, Rodríguez-Laso A, Zunzunegui MV. Unmet home care needs among community-dwelling elderly people in spain. Aging Clin Exp Res. 2003;15:234–42. doi: 10.1007/BF03324504. [DOI] [PubMed] [Google Scholar]
- 33.Bookman A, Kimbrel D. Families and elder care in the twenty- first century. Future Child. 2011;21:117–40. doi: 10.1353/foc.2011.0018. [DOI] [PubMed] [Google Scholar]
- 34.Smith PR. Elder care, gender, and work: The work-family issue of the 21st century. Berkeley J Employ Labor Law. 2004;25:351–99. [Google Scholar]
- 35.Bengtson VL, Burgess EO, Parrott TM. Theory, explanation, and a third generation of theoretical development in social gerontology. J Gerontol B Psychol Sci Soc Sci. 1997;52:S72–88. doi: 10.1093/geronb/52b.2.s72. [DOI] [PubMed] [Google Scholar]