

Abstract
Background:
Phantom sensations like phantom vibration (PV) and phantom ringing (PR)— the sensations of vibration and ringing of the phone when they are not, respectively—are among the latest in the category of “techno-pathology” to receive global attention. This study was conducted with the aim to estimate the prevalence of such sensations among medical interns and their association with perceived stress levels and smartphone usage pattern.
Materials and Methods:
Ninety-three medical interns using smartphone were recruited for the study. Data were collected anonymously using semi-structured questionnaire, perceived stress scale (PSS), and smartphone addiction scale-short version (SAS-SV). Data were analyzed using descriptive statistics, Chi-square test, independent t-test, ANOVA, and Pearson's correlation coefficient.
Results:
Fifty-nine percent students had a high level of stress, whereas 40% had problematic smartphone use. Sixty percent students experienced PV, whereas 42% experienced PR and both were significantly associated with higher frequency of phone use and the use of vibration mode. Mean SAS-SV score was significantly lower in students who did not perceive PR/PV, whereas mean PSS score was significantly lower in students who did not perceive PV.
Conclusion:
This study confirms findings from other national and international researches about the experience of cell phone phantom sensations and their relationship with the pattern of phone use and stress level. It also brings to light high levels of stress and problematic smartphone use among medical students during the internship.
Key words: India, phantom, ringing, smartphone, stress, vibration
INTRODUCTION
Necessity is the mother of invention, it is said. Invention, we say, is the mother of modern diseases! This could be true of conditions that are being categorized as “techno-pathology”—disorders resulting from the overuse or misuse of technology.[1] Phantom sensations like phantom vibration (PV) and phantom ringing (PR)—the sensation of vibration and ringing of the phone when it is not, respectively—are one of the latest in this category to receive global attention. This may be attributed to the rising use of smartphones among people of all ages, especially the youth. The Telecom Regulatory Authority of India (TRAI) recently revealed that until December 2017, 1,167.44 million people in India used mobile phones.[2] A similar trend has been observed all over the world.[3] Not surprisingly, problem behaviors associated with mobile phone use have also seen an increasing trend.[4] Among the disturbances seen are behavioral addictions (mobile phones, Internet, etc.), emotional disturbances reportedly due to excessive smartphone use, and phantom vibration syndrome (PVS).[5,6] PVS, although termed a “syndrome,” is not really a disease or disorder. It is more a “normal phenomenon” with possible misinterpretation of stimuli.[6] The same holds true for PR.
Rothberg et al. (2010) led one of the earliest studies in this regard.[6] They evaluated the prevalence of PV among medical personnel. Approximately two thirds of their subjects reported having experienced PV. A large number (93%) of subjects found this to be “slightly” or “not at all” bothersome. With regard to the frequency of the experience, approximately 88% of the subjects reported it “weekly” or “monthly.” In another, prospective, study of 74 medical interns, it was found that subjects with severe PV/PR had higher subjective somatic anxiety and somatic depressive scores at any given time during their internship.[7] This leads us to believe that stress must have some role to play in the phenomenon of phantom sensations. There is also a possibility that the phenomena may be attributable to a prodrome of clinical burnout syndrome. Chen et al. (2014) did not find any association of PV/PR with anxiety or depression but found that work-related burnout was significantly associated with phantom sensations.[8] This makes PV/PR a potential predictor of occupational burnout. In India, Goyal (2015) studied PV and PR among 300 postgraduate students and found that 74% of students had experienced both phenomena, whereas 17% experienced PV exclusively and 4% experienced PR exclusively.[9]
Across the globe, internship during medical studies has been found to be a stressful period with a declining quality of life.[10,11,12,13] Among the possible causes for such findings are the increasing sense of responsibility and uncertainty in this period as well as the transition from being an observer of medicine to a practitioner.[10]
Young adults have been found to cope with such stressful experiences by increasing their time spent on mobiles. The mobile phone offers several advantages like portability, accessibility, and privacy even in a public setting, among others, thereby offering a small “security blanket” effect, lowering the initial negative reactions to stress. However, pervasive use of this coping strategy is unlikely to remain beneficial in the long-run, with resultant adverse mental health impact.[14] Further, both high levels of stress and smartphone use have been found to be associated with higher PV/PR sensations as described earlier.[6,7] Phantom perceptual experiences cannot be explained by stress alone. A multitude of factors such as personality traits of anxiety and avoidance, and situational ones like expecting a call or message and being concerned about an issue that one may be contacted about at a given time may also influence the experience.[15]
With this background, we set out with the aim to estimate the prevalence of phantom perceptual experiences of smartphone ringing/vibrating among medical students at a private university in western India. We also attempted to examine the association of these with perceived stress levels and smartphone usage pattern.
MATERIALS AND METHODS
This was a cross-sectional study conducted after obtaining clearance from the Institutional Ethics Committee (IEC). Our sample consisted of medical interns from the institute—a private university located in western India. Initial screening of the interns was done by a qualified psychiatrist. Interns who were smartphone users and consented to the study were recruited. We chose smartphone users specifically, as these are the most commonly used devices these days, especially among younger populations, and one of the tools used was specifically designed for smartphone users. Hence, traditional basic or feature phone users were not included. Further, those with a present or past history of mental illness or alcohol/substance dependence were also excluded to minimize the impact of abnormal perceptual experience related to mental illness on normal phantom sensations.
Sampling method
Students belonging to only one particular year—internship—were recruited. This would have helped in minimizing the potential variation in stress levels among students belonging to different levels of seniority.[16] The sample size was 118 (all students doing the internship), out of which data from 25 interns could not be included due to incomplete data or refusal to participate, resulting in a total recruited sample of 93 students.
Method of data collection
Data were collected by a qualified psychiatrist using the following instruments: (1) semi-structured questionnaire in English for documenting details about the PV/PR sensations over the last 1 month anonymously and confidentially; (2) perceived stress scale (PSS)[17]—PSS is the most widely used psychological instrument for measuring the perception of stress. It is a measure of the degree to which situations in one's life are appraised as stressful. The questions are of a general nature and hence relatively free of content specific to any subpopulation group. PSS has 10 items where each item is rated on a 5-point Likert scale ranging from never (0) to almost always (4). Positively worded items are reverse scored and the ratings are summed, with higher scores indicating more perceived stress. The questions in the PSS ask about feelings and thoughts during the last month. This scale has been found to be a substantially reliable measurement tool (i.e., coefficient of reliability = 0.84, 0.85, and 0.86, in three test samples) with high reliability (a = 0.78) and acceptable validity; (3) smartphone addiction scale-short version (SAS-SV)[18]—the SAS-SV is a validated scale originally constructed in South Korea, but published in English. It contains 10 items rated on a dimensional scale (1 “strongly disagree” to 6 “strongly agree”). The total score ranges from 10 to 60, with the highest score being the maximum presence of “smartphone addiction” in the past year. The original SAS-SV showed content and concurrent validity and internal consistency (Cronbach's alpha: 0.91).
Ethical aspects
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent was obtained from all individual participants included in the study.
Statistical analysis
Demographic details and information about the experience of phantom sensations were assessed using frequency distribution tables. Chi-square test was used to assess the relationship between the experience of phantom sensations with other smartphone use characteristics like the use of the phone in vibration mode and the average number of calls/messages received in a day. The relationship between PSS/SAS-SV scores and gender was assessed using independent t-test. The relationship between PSS/SAS-SV scores and experience of phantom sensations was assessed using analysis of variance (ANOVA). Karl Pearson correlation coefficient was used to assess the relationship between PSS and SAS-SV scores.
RESULTS
Of 93 recruited students, almost 63% (n = 59) were females. Eighty-seven percent (n = 81) of the students carried only one mobile phone. Almost 51% (n = 47) of the students kept phones in their side pockets (e.g., apron) whereas 47% (n = 44) kept them in their front pocket (e.g., trouser). Ninety-six percent (n = 89) students used the “vibration” function irrespective of whether the phone was on silent or ringing mode. About 70% (n = 65) of the students reported receiving an average of more than 10 calls/messages per day.
On evaluating the scores on PSS, 59% (n = 55) had a score of greater than 20, indicating high levels of stress. Further, on taking a cutoff score of 31 for males and 33 for females in SAS-SV, almost 40% (n = 37) of the students had a high level of smartphone usage pattern possibly approaching addiction. Males were found to have a significantly higher SAS-SV score as compared to females. On assessing Karl Pearson correlation coefficient, a weak positive relationship (r = 0.297) was found between PSS and SAS-SV scores, indicating 29.7% students with higher PSS score had a significantly higher SAS-SV score, which was more significant among females as compared to males. The students who showed high levels of stress and smartphone usage were further evaluated psychologically and offered appropriate treatment interventions, which was not part of the study.
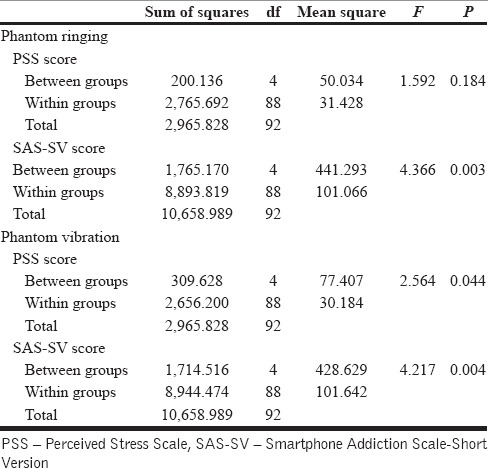
Sixty percent (n = 56) of the students reported having experienced PV, and 42% (n = 39) had experienced PR. There was a significant relationship between the prevalence of phantom sensations with use of the phone in vibration mode and the average number of calls/messages received per day [Table 1]. Mean SAS-SV score was significantly lower in students who did not experience PR as compared to those who did. There was no difference in their mean PSS score. On the other hand, both mean PSS score and SAS-SV score were significantly lower in students who did not perceive PV as compared to those who did [Table 2].
Table 1.
Relationship between “use of phone in vibration mode” and “approximate number of calls received per day” with experience of “phantom sensations”

Table 2.
Relationship between experience of “phantom sensations” with PSS and SAS-SV scores (ANOVA)
DISCUSSION
PV and PR are common forms of pseudo-hallucination in the general population, especially the teenagers and adolescents.[7] Prevalence of phantom sensations shows wide variability. An Iranian study involving medical students found the prevalence of 54.3% and 49.3% for PV and PR, respectively, which is close to our findings of 60% and 49%, respectively.[19] On the other hand, baseline prevalence among Taiwanese medical interns was found to be 78.1% and 27.4% for PV and PR, respectively, which spiked to a maximum of 95.9% and 87.7% respectively during the period of internship.[7] Similar high prevalence of PV (93%) was reported among Pakistani medical students.[20] An Indian study involving 300 students found the prevalence to be around 74%.[9] Such wide variation could be accounted for by different geographical and sociodemographic characteristics along with varied levels of stress and emotional responses among different populations.[21]
Similar to our findings, previous studies too have reported higher prevalence of phantom sensations when using the phone in vibration mode and among those who spend more time using their mobile phone.[7,9] On the subjective evaluation of the extent of phone use based on the approximate number of calls/messages attended per day, we found a significant relationship with experience of phantom sensations [Table 1]. Further, on an objective evaluation of the extent of phone use by applying SAS-SV scale, lower scores were significantly associated with lower chances of experiencing phantom sensations [Table 2]. Thus, we found a possible relationship between the extent of smartphone use and experience of PV/PR. This phenomenon could have three possible explanations: (1) higher smartphone use emanates from differing needs like productivity-enhancement, information-seeking, social information, and interaction, diversion and relaxation, entertainment, monetary compensation, and personal status.[4] Individuals are reliant on messages/calls/alerts to navigate their personal, professional, and social relationships and hence more likely to receive more messages, keep their phone in vibration mode to be alerted to those messages, and thus develop heightened sensitivity to mobile phone vibrations because of repeated exposure.[19] (2) Higher smartphone use is often considered as a risk factor for developing anxiety, stress, and depression, indicating higher stress levels among such individuals leading to heightened sensitivity and predisposition to misinterpretation of sensory stimuli or imagined vibrations.[14] Mobile phones may also be used as a coping method to deal with negative emotion, suggesting a bidirectional relationship.[22] Our finding of lower PSS scores being significantly associated with a lower experience of PV also supports the latter possibility. (3) Certain psychological attributes, as explained earlier, could have interacted with contextual factors like emergency duties, which are common during the internship, leading to higher chances of PV and PR experiences.[15]
On assessing the PSS scores independently, the majority of our subjects (59%) were found to have a high level of stress, with a mean score of 20.85 (+5.39) among males and 19.44 (+5.82) among females. This is similar to the findings among students affiliated to a medical college in Orissa, India where 53% were found to be suffering from stress, with females suffering significantly more than males.[16] We did not find any gender difference in PSS scores. They also found higher morbidity among senior students. Similar results were observed among medical students in Bangladesh[23] and the United States of America.[24]
On assessing the SAS-SV scores independently, 40% of our students had a score above the cutoff recommended by Kwon et al. (2013),[18] with males having a significantly higher score. A recent study utilizing the full version of SAS found 33.3% adolescents were high users of the smartphone with males having significantly higher scores as compared to females, similar to our finding.[25] An interesting term, nomophobia, has been coined depicting an irrational fear of being without one's phone or of being unable to use one's phone for some reason. An Indian study involving medical students from Bengaluru found 39.5% of their subjects to be suffering from nomophobia, suggesting high mobile phone use.[26] They also found the prevalence of nomophobia to be higher in males, though not statistically significant. Another study utilizing a different scale found a high prevalence rate of mobile phone dependence (85.1%) among medical students in Nanded, India.[27]
A weak positive correlation was found (r = 0.297) between PSS and SAS-SV scores, suggesting a reciprocal relationship between stress and smartphone addiction. A recent systematic review found stress to be somewhat consistently related to problematic mobile phone use, with small to medium effect size.[4] Bidirectional relationship between negative emotion and mobile phone use has been observed, as explained earlier.[22]
CONCLUSION
This study confirms findings from other national and international research about the experience of cell phone phantom sensations and their relationship with the pattern of phone use and stress level. It also brings to light high levels of stress and problematic smartphone use among medical students during their internship period. Although the experience of phantom sensations does not indicate psychopathology per se, it could be considered as a sign indicating problematic mobile phone usage and possibly clinically high levels of stress warranting further investigation. This study also has its own limitations. Considering the fact that the study population involved only medical students doing the internship, our findings cannot be generalized to the public or even the students in different phases of medical education. Personality attributes of these students were not accounted for and provide an opportunity for further research.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Varela JE. Technopathology: The New Epidemic of the 21st Century. Rev Enferm. 2016;39:31–6. [PubMed] [Google Scholar]
- 2.Telecom Regulatory Authority of India (TRAI), Telecom Subscription Data December 2017. [Last accessed on 2018 Mar 12]. Available from: http://www.trai.gov.in/sites/default/files/PR_No23_TSD_Eng_16022018.pdf .
- 3.International Telecommunication Union, World Telecommunication/ICT Development Report and database. 2016. [Last accessed on 2018 Mar 12]. Available from: https://data.worldbank.org/indicator/IT.CEL.SETS.P2?end=2016&name_desc=false&start=2007&view=chart .
- 4.Elhai JD, Dvorak RD, Levine JC, Hall BJ. Problematic smartphone use: A conceptual overview and systematic review of relations with anxiety and depression psychopathology. J Affect Disord. 2017;207:251–9. doi: 10.1016/j.jad.2016.08.030. [DOI] [PubMed] [Google Scholar]
- 5.De-Sola Gutierrez J, Rodriguez de Fonseca F, Rubio G. Cell-Phone Addiction: A Review. Front Psychiatry. 2016;7:175. doi: 10.3389/fpsyt.2016.00175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rothberg MB, Arora A, Hermann J, Kleppel R, St Marie P, Visintainer P. Phantom vibration syndrome among medical staff: A cross sectional survey. BMJ. 2010;341:c6914. doi: 10.1136/bmj.c6914. [DOI] [PubMed] [Google Scholar]
- 7.Lin YH, Chen CY, Li P, Lin SH. A dimensional approach to the phantom vibration and ringing syndrome during medical internship. J Psychiatr Res. 2013;47:1254–8. doi: 10.1016/j.jpsychires.2013.05.023. [DOI] [PubMed] [Google Scholar]
- 8.Chen CP, Wu CC, Chang LR, Lin YH. Possible association between phantom vibration syndrome and occupational burnout. Neuropsychiatr Dis Treat. 2014;10:2307–14. doi: 10.2147/NDT.S73038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Goyal AK. Studies on Phantom Vibration and Ringing Syndrome among Postgraduate Students. Indian J Comm Health. 2015;1:35–40. [Google Scholar]
- 10.Liu CH, Tang WR, Weng WH, Lin YH, Chen CY. The process of coping with stress by Taiwanese medical interns: A qualitative study. BMC Med Educ. 2016;16:10. doi: 10.1186/s12909-016-0534-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Abdulghani HM, Irshad M, Al Zunitan MA, Al Sulihem AA, Al Dehaim MA, Al Esefir WA, et al. Prevalence of stress in junior doctors during their internship training: A cross-sectional study of three Saudi medical colleges' hospitals. Neuropsychiatr Dis Treat. 2014;10:1879–86. doi: 10.2147/NDT.S68039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Chandramouleeswaran S, Edwin NC, Braganza D. Job stress, satisfaction, and coping strategies among medical interns in a South Indian tertiary hospital. Indian J Psychol Med. 2014;36:308–11. doi: 10.4103/0253-7176.135387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Susmita C, Edwin N, Braganza D. Quality of life among medical interns in a South Indian tertiary hospital. Natl Med J India. 2014;27:214–6. [PubMed] [Google Scholar]
- 14.Panova T, Lleras A. Avoidance or boredom: Negative mental health outcomes associated with use of Information and Communication Technologies depend on users' motivations. Comput Human Behav. 2016;58:249–58. [Google Scholar]
- 15.Kruger DJ, Djerf JM. High Ringxiety: Attachment Anxiety Predicts Experiences of Phantom Cell Phone Ringing. Cyberpsychol Behav Soc Netw. 2016;19:56–9. doi: 10.1089/cyber.2015.0406. [DOI] [PubMed] [Google Scholar]
- 16.Iqbal S, Gupta S, Venkatarao E. Stress, anxiety & depression among medical undergraduate students and their socio-demographic correlates. Indian J Med Res. 2015;141:354–7. doi: 10.4103/0971-5916.156571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health SocBehav. 1983;24:385–96. [PubMed] [Google Scholar]
- 18.Kwon M, Kim DJ, Cho H, Yang S. The smartphone addiction scale: Development and validation of a short version for adolescents. PLoS One. 2013;8:e83558. doi: 10.1371/journal.pone.0083558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mohammadbeigi A, Mohammadsalehi N, Moshiri E, Anbari Z, Ahmadi A, Ansari H. The prevalence of phantom vibration/ringing syndromes and their related factors in Iranian students of medical sciences. Asian J Psychiatr. 2017;27:76–80. doi: 10.1016/j.ajp.2017.02.012. [DOI] [PubMed] [Google Scholar]
- 20.Alam M, Qureshi S, Sarwat A, Haque Z, Masroor S, Makki A, et al. Prevalence of Phantom Vibration Syndrome and Phantom Ringing Syndrome (Ringxiety): Risk of Sleep Disorders and Infertility among Medical Students. Int J Adv. 2014;2 [Google Scholar]
- 21.Drouin M, Kaiser DH, Miller DA. Phantom vibrations among undergraduates: Prevalence and associated psychological characteristics. Comput Human Behav. 2012;28:1490–6. [Google Scholar]
- 22.Kim J, Seo M, David P. Alleviating depression only to become problematic mobile phone users: Can face-to-face communication be the antidote? Comput Human Behav. 2015;51:440–7. [Google Scholar]
- 23.Eva EO, Islam Z, Mosaddek AS, Rahman F, Rozario RJ, Iftekhar AF, et al. Prevalence of stress among medical students: A comparative study between public and private medical schools in Bangladesh. BMC Res Notes. 2015;8:327. doi: 10.1186/s13104-015-1295-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Ludwig AB, Burton W, Weingarten J, Milan F, Myers DC, Kligler B. Depression and stress amongst undergraduate medical students. BMC Med Educ. 2015;15:141. doi: 10.1186/s12909-015-0425-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Soni R, Upadhyay R, Jain M. Prevalence of smart phone addiction, sleep quality and associated behaviour problems in adolescents. Int J Res Med Sci. 2017;5:515. [Google Scholar]
- 26.Pavithra MB, Madhukumar S, Murthy M. A Study on Nomophobia-Mobile Phone Dependence, Among Students of a Medical College in Bangalore. Natl J Community Med. 2015;6:340–4. [Google Scholar]
- 27.Domple VK, Wadde SK, Gattani PL. Mobile phone dependence among undergraduate medical students in Nanded city. Ann Trop Med PH. 2017;10:27. [Google Scholar]