

Abstract
Background:
The flood disaster of 9th–10th September 2014 wreaked havoc in the Jammu and Kashmir region of India. Incessant rains and deluge claimed 283 lives and damaged 2.53 lakh houses. This article presents the findings of the psychosocial care team from the National Institute of Mental Health and Neuro Sciences, Bengaluru, India, during the early phase of disaster.
Materials and Methods:
The team assessed posttraumatic stress symptoms of 64 child survivors from six villages of two districts struck by floods using Children's Revised Impact of Event Scale (CRIES)-8 and qualitative narrations.
Results:
Children showed high levels of intrusion and avoidance in the aftermath of floods. Both boys and girls showed moderate to severe level of psychological impact on the domains of CRIES-8. The narrations by the children centred on the theme of “water” and “enjoyment in seeing lots of water;” followed by “fearing of the parent's life,” later on “fear of their own life,” and subsequently to avoidance to go near the river and nightmares like “floating in the water.”
Conclusion:
Disasters immensely impact children because of their particular stage of psychological and social development. This highlights the need for psychosocial interventions to minimize the impact of disasters on children at the earliest using simple psychosocial care techniques by employing available community-based manpower.
Key words: Children, flood disaster, Kashmir, posttraumatic stress symptoms
INTRODUCTION
A disaster is an event causing severe disruption to normal functioning of a society, leaving a profound trail of human, material, or environmental losses which exceed the natural ability of the affected society to cope with its own resources.[1] Disasters, depending on their sources, have been classified as either natural disasters, such as floods, droughts, earthquakes, and epidemics, or human-made disasters such as fire, conflicts, and terrorism. In recent years, global reports suggest a significant increase in the occurrence of natural disasters, especially those related to global warming.[2,3] Disasters are always coupled with psychosocial reactions, and research indicates that natural disasters have an immense impact on the psychological health of children, including symptoms of fear, depression, anxiety, self-blame, guilt, loss of interest in school and other activities, regressive behavior, sleep and appetite disturbance, night terrors, aggressiveness, poor concentration, and separation anxiety.[4] Almost half of the surveys conducted on children after a natural disaster report some level of PTSD symptoms.[5] In a disaster such as traumatic events, children exhibit symptoms that vary from minimum to severe based on a child's developmental level, personal experiences, emotional or physical health, and parental response to the incident.[6] India is highly prone to natural disasters caused by recurrence of floods, droughts, cyclones, earthquakes, and landslides. Out of the 602 districts in the country, 125 have been identified as most hazard-prone areas.[7]
The state of Jammu and Kashmir has been engulfed in a cycle of armed conflict for the past six decades, affecting nearly everybody living in the region. Housen et al.[8] reported that mental distress in Kashmir Valley was experienced by 45% of their sample, with 41% suffering from depression, 26% with anxiety, and 19% with probable posttraumatic stress disorder (PTSD). Besides experiencing the brunt of prolonged armed violence, the state has also been declared a multi-hazard-prone region in India. Owing to its unique geopolitical and geographical setting, the state has suffered a lot due to natural disasters.[9] One such disaster occurred in September 2014, leading to devastating physical and psychological damage in the state in the wake of floods caused by incessant rains. According to official estimates, the deluge resulted in the loss of 283 lives, displacement, and damage to 2.53 lakh houses. The districts of Srinagar, Budgam, Anantnag, Pulwama, and Kulgam were the worst affected.[10]
The Government of India designated National Institute of Mental Health and Neurosciences (NIMHANS), Bengaluru, as the nodal agency for assessment and coordination of psychosocial relief work for the affected population following flood disaster. Hence, a multidisciplinary team was deputed to the Kashmir Valley to identify various psychosocial issues of the affected populace and to provide immediate interventions and psychosocial care. This article reflects the part of community assessment and intervention carried out in the region during the early phase of disaster by the psychosocial care team.
MATERIALS AND METHODS
Setting and sample
The state of Jammu and Kashmir is the northernmost state of India which comprises three regions, namely, Jammu, Kashmir, and Ladakh, with a total population of 10.14 million. It is divided into 22 districts – 2 districts in Ladakh region and 10 each in Jammu and Kashmir.[11] This study was conducted between 10th and 25th September 2014 in six villages of two flood-struck districts (Anantnag and Pulwama) of Kashmir region. The study sample consisted of 64 child survivors from six villages affected by floods who had resumed schooling in their respective communities and agreed to participate in the study.
Instruments
The psychological impact was assessed using Urdu version of Children's Revised Impact of Event Scale (CRIES)-8.[12] It is a screening instrument for children at risk of developing PTSD after experiencing a traumatic event.[13] It has eight items that constitute two subscales, Intrusion and Avoidance. Statements are scored as follows: 0 (not at all), 1 (rarely), 3 (sometimes), and 5 (often), with scores ranging from 0 to 40. Higher scores on scale reflect the presence of more posttraumatic stress symptoms (PTSS). Internal consistencies of CRIES-8 range from 0.75 to 0.84.[13,14,15] The validity of CRIES-8 has been reported satisfactory with a cut-off score of 17.[16,17] To gain an in-depth understanding of children's reactions to the disaster, interviews were conducted focusing on their experience of fear, immediate responses, and coping strategies.
Procedure
The psychosocial care team visited the affected villages once the water receded and they became accessible through roads. The team approached six schools that had resumed work after floods and contacted the principals with the request to make an announcement in the schools and in the surrounding area about the availability of mental health professionals and that the needy could avail mental health services. Information, education, and communication materials in the form of manuals, booklets, and pamphlets on psychosocial care of children and adults affected by disasters, developed by NIMHANS, were distributed among teachers in all six schools. The team had both individual interviews using CRIES-8 and group discussions with children who joined school after floods and agreed to participate in the study by giving written informed assent. In group discussions, the children were motivated to share their experiences of flood disaster. The principal investigator moderated the group discussions, while coinvestigators took notes of the experiences expressed by the children. Later, transcripts were read several times to develop categories and themes. Different categories were compared for underlying meanings and relationship at the interpretation level to form themes which are discussed under “qualitative narrations.” Post hoc approval was obtained from NIMHANS Ethics Committee (vide ref. No. NIMHANS/IEC/2018).
RESULTS
Characteristics of informants
A total of 64 children were interviewed, whose age ranged from 13 to 18 years (mean age 14.61 ± 1.06 years) [Table 1].
Table 1.
Sociodemographic characteristics of the children
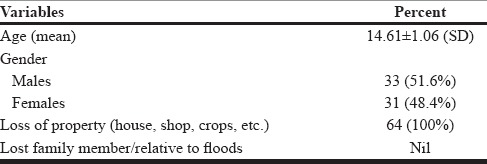
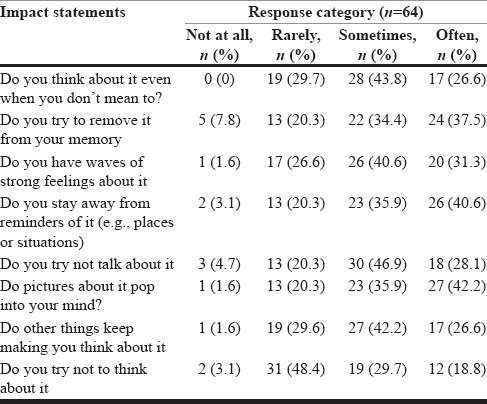
All participants lost property in floods. To assess the impact of flood disaster on psychological health [Table 2], respondents were asked to rate their impact with eight statements of CRIES-8 using a Likert scale. More than half of the respondents (70.4%) reported that sometimes or often they think about the event even when they do not mean to do so. On another statement, most of the respondents (71.9%) reported that sometimes or often they try to remove memories of the event. In similar manner, responses to statement “Do you have waves of strong feelings about it?” received an endorsement on sometimes or often from 71.9% of the respondents. Most of the respondents (70.6%) affirmed that sometimes or often they stay away from the remaining event, against 23.4% who responded not at all or rarely. A majority of the respondents (75%) sometimes or often try not talk about the event. A stronger majority of the sample (78.1%) sometimes or often concurred that pictures about the event come into their mind. Also, 69.1% of the respondents reported that sometimes or often other things make them think about the event. Interestingly, 48.5% of the participants reported that sometimes or often they do not try to think about the event, against 48.4% who reported rarely and 3.1% who denied the same.
Table 2.
Impact of a flood disaster on the psychological health of children
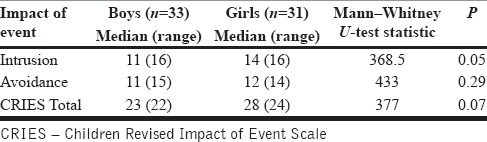
Mann–Whitney U-test [Table 3] revealed no significant differences (P > 0.05) of the impact of disaster on boys and girls on intrusion, avoidance, or CRIES-8 total scores.
Table 3.
Differences of impact of event on psychological health based on gender
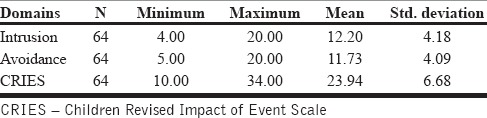
The descriptive analysis [Table 4] shows the mean score of intrusion level of children (n = 64) at 12.20 ± 4.18 and avoidance level at 11.73 ± 4.09. The total mean score of CRIES is 23.93 ± 6.68 with a cut-off score reported at 17. Therefore, the results showed the presence of higher levels of PTSSs in children post disaster.
Table 4.
Overall impact of disaster on psychological health of children
Qualitative narrations
Disasters cause traumatic experiences which often surpass the coping ability of an individual. Expression of trauma by children helps them understand traumatic experiences in more detailed form and understand their context and meaning and facilitates ways of addressing their belief systems.[18] The following section presents the experiences of children under different themes:
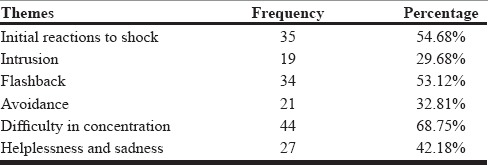
Initial reactions to shock
“I heard announcements on loudspeakers of mosque of immediate evacuation, and a few minutes later, I saw water flowing from all sides. Initially I was excited to see lots of water, but, as water began destroying houses around us, I started fearing for myself and my parents' lives.”
“In the beginning, I was unable to understand what is happening around me.”
“I saw my mother and aunt crying; my sisters and I were terrified.”
Intrusion
“Sometimes, all of a sudden, images of people pleading for help and rescue pop in my mind; I feel like crying and sad.”
“Whenever I pass by the river of our village, I start recollecting the events of the flood, the shouting, and the crying. My heart begins to beat fast. I close my eyes and run as fast as I could to save myself.”
“I am unable to sleep in nights – Even the sound of rain or wind reminds me of the floods.”
Flashbacks
“I get dreams of water entering my room, and I start floating on it. I feel caught inside. When the whole room gets filled with water, I start drowning and water enters my mouth and nose. I wake up, with whole of my body sweating and shivering; after that I don't get sleep.”
“During nights, when I go to sleep, I get thoughts and images of water surrounding me. I am not able to sleep peacefully.”
Avoidance
“We are scared to go near the stream; it also reminds of the floods. I do not go near as it may flood again.”
Difficulty in concentrating
“Floods have occupied my mind. I am not able to do my homework properly, and I keep on forgetting my lessons or homework given at school.”
“During classes, I keep looking out through the window to check whether floods might have again entered our village.”
Helplessness and sadness
“Floods destroyed our newly constructed house. We lost almost everything. Now I don't know whether we may be able to live a normal life again.”
“My father didn't speak to anyone for days. He remained aloof in a corner, and I saw him crying silently. It was very painful for me.”
“I feel helpless as I was not able to help my family to save some of the belongings during floods” [Table 5].
Table 5.
Themes reported by children
DISCUSSION
Natural disasters cause widespread loss of life and property. This study found all the children who lost property in flood disaster. High levels of psychological impact were seen in children. Studies using mixed methods while exploring the impact of disasters on children help in developing appropriate result-oriented interventions as compared to conducting separate qualitative and quantitative studies.[19,20] Psychological health of children is affected largely by the nature of disaster, the level of exposure to disaster, personal loss, and individual characteristics of children, including their age, gender, and stage of development. After disaster, children manifest psychological distress in forms of anxiety, fear, sadness, hostility and aggressive behavior, apathy, withdrawal, sleep disturbances, somatization, and pessimistic thoughts.[7,21] In this study, children reported psychological symptoms in the form of increased palpitation, panic, sadness, inability to sleep, fear when they think of flood, and difficulty in concentrating.
Our study reports the presence of PTSSs in children. However, elevating them to the construct of PTSD requires a minimum of three avoidance symptoms, two hyper-arousal symptoms, one re-experiencing symptom, and clinically significant distress or impairment in social, occupational, or other areas of functioning as per Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition.[22,23] None of the participants with PTSS satisfied these criteria for PTSD, especially functional impairment. This study reports the presence of equal levels of PTSS in both boys and girls. This finding contradicts previous research which suggests that women always tend to suffer more from the impact of disasters than men, due to gender inequalities involving lack of access to resources that allow people to cope with negative impacts of a disaster such as income, education, health, and social networks.[24]
Many tools have been developed to assess the impact of psychological distress such as Trauma Screening Questionnaire,[25] Depression Self-Rating Scale, and Child Posttraumatic Stress Disorder Reaction Index.[26] However, most of the research have focused on the effectiveness of the Impact of Event Scale[27] that has a modified version for children as CRIES, having 8 and 13-items. The 8-item CRIES, the most commonly used shorter version, is found useful in children age 8 years and older.[28] The same tool (CRIES-8) has been used in this study to analyze and explore the impact of a flood disaster on children. The strength of this study is using a mixed methodology that gives a complete picture of the impact of disaster on health and well-being in complex emergencies and helps improve the quality of services for affected populations.[29]
This study has a few limitations. The study was cross-sectional and could only include children who returned to school and agreed to participate in the study. However, children who are yet to join and those who refused to be part of the study form a significant number. Hence, it can be inferred that the study population is not an accurate representation of the total magnitude of the affected children. Such studies in future should adopt door-to-door survey than a school-based survey.
The data for the study were collected predominantly during field visits to affected villages for carrying out psychosocial assessment and interventions in the early phase of the disaster, rather than as a research project; therefore, rigorous sampling methods could not be carried out.
Implications for social work practice
Provide psychological first aid and support to children and families
Identify needs of children and resources and help them to access resources
Prevent severe physical and mental problems in children by making referrals
Prevent individuals, families, groups, organizations, and communities from breaking down, through psychosocial intervention aimed at developing coping and resilience among the affected population.
CONCLUSION
Disasters immensely impact children because of their particular stage of psychological and social development. PTSSs were seen to be common in children. However, in the absence of functional impairment, elevating them to a psychiatric diagnosis of PTSD is questionable.[23] The need to intervene to minimize the impact on children at the earliest, using simple psychosocial care by the available community resources, is important.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
“Authors are thankful to the Emergency Medical Relief division, Ministry of Health and Family Welfare, Government of India for providing all possible support for carrying out relief work. We are grateful to Director, NIMHANS Bengaluru, National Disaster Management Authority, New Delhi and Directorate of health services Kashmir for providing necessary support.” We are also thankful to Dean Behavioural Sciences, NIMHANS Bengaluru for providing post hoc ethical clearance for manuscript.
REFERENCES
- 1.International Strategy for Disaster Reduction. Basic Terms of Disaster Risk Reduction. Living with Risk: A Global Review of Disaster Reduction Initiatives. United Nations Publications. 2004. [Last accessed on 2017 Aug 26]. Available from: https://www.unisdr.org/we/inform/terminology .
- 2.Helmer M, Hilhorst D. Natural disasters and climate change. Disasters. 2006;30:1–4. doi: 10.1111/j.1467-9523.2006.00302.x. [DOI] [PubMed] [Google Scholar]
- 3.Van Aalst MK. The impacts of climate change on the risk of natural disasters. Disasters. 2006;30:5–18. doi: 10.1111/j.1467-9523.2006.00303.x. [DOI] [PubMed] [Google Scholar]
- 4.Baggerly J, Exum HA. Counseling children after natural disasters: Guidance for family therapists. Am J Fam Ther. 2007;36:79–93. [Google Scholar]
- 5.Saylor CF, Cowart BL, Lipovsky JA, Jackson C, Finch AJ., Jr Media exposure to September 11: Elementary school students' experiences and posttraumatic symptoms. Am Behav Sci. 2003;46:1622–42. [Google Scholar]
- 6.Vogel JM, Vernberg EM. Part 1: Children's psychological responses to disasters. J Clin Child Psychol. 1993;22:464–84. [Google Scholar]
- 7.Vranda MN, Sekar K. Assessment of psychosocial impact of flood on children: Indian experience. J Indian Acad Appl Psychol. 2012;38:19–22. [Google Scholar]
- 8.Housen T, Lenglet A, Ariti C, Shah S, Shah H, Ara S, et al. Prevalence of anxiety, depression and post-traumatic stress disorder in the Kashmir Valley. BMJ Glob Health. 2017;2:e000419. doi: 10.1136/bmjgh-2017-000419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.National Disaster Management Authority. Jammu and Kashmir State Disaster Management Policy. Govt. of Jammu and Kashmir (n.d) [Last accessed on 2017 Aug 26]. Available from: http://www.ifrc.org/docs/IDRL/DM_POLICY0_J%26K_IMPA.pdf .
- 10.Rajya Sabha TV. 282 people died, 2.53 lakh houses damaged in JK floods. Govt. of India 2014. [Last accessed on 2017 Aug 26]. Available from: http://rstv.nic.in/282-people-died-2-53-lakh-houses-damaged-jk-floods-govt.html .
- 11.Election Commission of India. Comprehensive SVEEP Plan of J&K State. Govt. of India. 2004. [Last accessed on 2017 Aug 26]. Available from: http://eci.nic.in/eci_main1/SVEEP/Jammu%20&%20Kashmir19092014.pdf .
- 12.Children and War Foundation. Children's Revised Impact of Event Scale. 2011. [Last accessed on 2017 Jul 12]. Available from: http://www.childrenandwar.org/measures/
- 13.Smith P, Perrin S, Dyregrov A, Yule W. Principal components analysis of the impact of event scale with children in war. Pers Individ Dif. 2003;34:315–22. [Google Scholar]
- 14.Lau JT, Yeung NC, Yu XN, Zhang J, Mak WW, Lui WW. Validation of the Chinese version of the Children's Revised Impact of Event Scale (CRIES) among Chinese adolescents in the aftermath of the Sichuan Earthquake in 2008. Compr Psychiatry. 2013;54:83–90. doi: 10.1016/j.comppsych.2012.06.007. [DOI] [PubMed] [Google Scholar]
- 15.Zhang N, Zhang Y, Wu K, Zhu Z, Dyregrov A. Factor structure of the Children's Revised Impact of Event Scale among children and adolescents who survived the 2008 Sichuan earthquake in China. Scand J Psychol. 2011;52:236–41. doi: 10.1111/j.1467-9450.2010.00867.x. [DOI] [PubMed] [Google Scholar]
- 16.Perrin S, Meiser-Stedman R, Smith P. The Children's Revised Impact of Event Scale (CRIES): Validity as a screening instrument for PTSD. Behav Cogn Psychother. 2005;33:487–98. [Google Scholar]
- 17.Deeba F, Rapee RM, Prvan T. Psychometric properties of the Children's Revised Impact of Events Scale (CRIES) with Bangladeshi children and adolescents. Peer J. 2014;2:e536. doi: 10.7717/peerj.536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Pynoos RS, Steinberg AM, Goenjian A. Traumatic stress in childhood and adolescence: Recent developments and current controversies. In: Van der Kolk BA, McFarlane AC, Weisaeth L, editors. Traumatic Stress: The Effects of Overwhelming Experience on Mind, Body, and Society. New York: Guilford Press; 1996. pp. 331–58. [Google Scholar]
- 19.Boeije H, Slagt M, van Wesel F. The contribution of mixed methods research to the field of childhood trauma: A narrative review focused on data integration. J Mix Methods Res. 2013;7:347–69. [Google Scholar]
- 20.O'Cathain A, Murphy E, Nicholl J. Integration and publications as indicators of “yield” from mixed methods studies. J Mix Methods Res. 2007;1:147–63. [Google Scholar]
- 21.Schonfeld DJ. Supporting adolescents in times of national crisis: Potential roles for adolescent health care providers. J Adolesc Health. 2002;30:302–7. doi: 10.1016/s1054-139x(02)00382-8. [DOI] [PubMed] [Google Scholar]
- 22.Peters L, Slade T, Andrews G. A comparison of ICD10 and DSM-IV criteria for posttraumatic stress disorder. J Trauma Stress. 1999;12:335–43. doi: 10.1023/A:1024732727414. [DOI] [PubMed] [Google Scholar]
- 23.Rajkumar AP, Mohan TS, Tharyan P. Lessons from the 2004 Asian tsunami: Epidemiological and nosological debates in the diagnosis of post-traumatic stress disorder in non-Western post-disaster communities. Int J Soc Psychiatry. 2013;59:123–9. doi: 10.1177/0020764011423468. [DOI] [PubMed] [Google Scholar]
- 24.Neumayer E, Plümper T. The gendered nature of natural disasters: The impact of catastrophic events on the gender gap in life expectancy, 1981–2002. Ann Assoc Am Geogr. 2007;97:551–66. [Google Scholar]
- 25.Brewin CR, Rose S, Andrews B, Green J, Tata P, McEvedy CH, et al. Brief screening instrument for post-traumatic stress disorder. Br J Psychiatry. 2002;181:158–62. doi: 10.1017/s0007125000161896. [DOI] [PubMed] [Google Scholar]
- 26.Goenjian AK, Walling D, Steinberg AM, Roussos A, Goenjian HA, Pynoos RS. Depression and PTSD symptoms among bereaved adolescents 6½ years after the 1988 Spitak earthquake. J Affect Disord. 2009;112:81–4. doi: 10.1016/j.jad.2008.04.006. [DOI] [PubMed] [Google Scholar]
- 27.Horowitz M, Wilner N, Alvarez W. Impact of Event Scale: A measure of subjective stress. Psychosom Med. 1979;41:209–18. doi: 10.1097/00006842-197905000-00004. [DOI] [PubMed] [Google Scholar]
- 28.Mondal R, Sarkar S, Banerjee I, Hazra A, Majumder D, Sabui T, et al. Acute stress-related psychological impact in children following devastating natural disaster, the Sikkim earthquake (2011), India. J Neurosci Rural Pract. 2013;(Suppl 1):S19. doi: 10.4103/0976-3147.116434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Bolton P, Tol WA, Bass J. Combining qualitative and quantitative research methods to support psychosocial and mental health programs in complex emergencies. Intervention. 2009;7:181–6. [Google Scholar]