

Abstract
Background:
Physical inactivity during adolescence and youth has been considered as potential risk factor for future mental health problems. The present study was conducted with the aim to examine whether an association exists between leisure-time physical activity (PA) and depression among the youth of Kangra district, studying in professional or degree colleges.
Methodology:
A cross-sectional study was conducted among the students of Medical College (MC), Central University (CU) and Industrial Training Institute (ITI) of Kangra district. 370 adolescents and youth of age <25 years, who consented to participate, were recruited. The sample size was divided into three parts among all the three institutes. Only one question regarding leisure time PA (LTPA) was asked, as to how many hours spent in the last week; and Center for Epidemiologic Studies Depression Scale for Children (CES-DC) was used.
Results:
There were 124 participants from ITI, 126 from CU and 120 from MC. The mean score of CES-DC was highest among CU students 22.7 (±11.0) and lowest among MC students; 13.6 (±9.2). Low LTPA (<4 h) was significantly associated with higher depressive symptoms among all students (odds ratio [95% confidence interval]; 3.34 [1.41–7.92]).
Conclusion:
LTPA was associated with lower rates of depression.
Key words: Depression, physical activity, young adult
INTRODUCTION
Depression, according to WHO, is a common illness worldwide, with an estimated 350 million people affected. The burden of depression and other mental health conditions is on the rise globally. The World Mental Health Survey conducted in 17 countries found that on average about 1 in 20 people reported having an episode of depression in 2011.[1]
The onset of depressive disorders occurs at a young age hence reducing people's functioning. This is one of the reasons that depression is the leading cause of disability worldwide regarding total years lost due to disability.[1]
It has been demonstrated that along with socioeconomic status (SES), gender, body mass index (BMI), smoking, alcohol, and psychological health, a reduced level of physical activity (PA) during adolescence and youth is also among the most important potential risk factors for the future mental health problems.[2,3,4]
It has generally been accepted that regular exercise confers medical health benefits on participants through increased cortical blood flow, endorphins, and epinephrine. Some cross-sectional studies in the field show that a higher level of PA is associated with a lower level of depressive symptoms.[5,6,7,8] Some prospective studies show a weak association between a higher level of PA during adolescence and lower risk of future depression/symptoms of depression, but others do not.[9] There is no consensus among the studies as to whether levels of PA may act as a preventive factor in the development of the future depression. In a developing country like India, the statistics on depression are still underestimating the true burden due to poor healthcare seeking behavior, less faith on primary healthcare and more on traditional healers, and the social stigma attached. There is a paucity of literature from the northern states of India on mental health or PA among youth. Hence, this study was designed to examine whether an association exists between leisure-time PA and poor mental health among the youth of Kangra district studying in professional or degree colleges.
District Kangra of Himachal Pradesh is situated in foothills of the Western Himalayas. The population of the district according to census 2011 was 1,507,223.[10] Around 20% of the population comprises of young people in the of age group 15–24 years.[11] In the district, there are 22 government colleges, two universities, six professional training institutions, and two postsecondary schools.[12]
METHODOLOGY
A cross-sectional study was conducted over a period of 3 months in three major institutes in the vicinity of the town of Kangra, in Himachal Pradesh. We selected one university, one professional training institution, and one post higher secondary school with vocational courses according to our convenience. A Government Medical College (MC), the Central University (CU) and an Industrial Training Institute (ITI) were selected.
To assess the mental health, we used Center for Epidemiologic Studies Depression Scale for Children (CES-DC), which is a depression scale designed in 1980 and is also used to measure current levels of depressive symptoms in a general population (CES-D).[13] The tool, although initially used for research purposes, is also used as a screening tool to identify persons at risk for clinical depression. The scale has been translated into several languages and validated for both young people and adults.[14,15] Higher CES-DC scores indicate increasing levels of depression. The cutoff score of 15 as being suggestive of depressive symptoms has been used in the current study.
PA has been defined as “any bodily movement produced by skeletal muscle and resulting in energy expenditure.” Leisure time PA (LTPA) is defined as “PA performed during exercise, recreation, or any time other than those associated with one's regular occupation, housework, or transportation.”[16,17]
Only one question regarding LTPA was asked. The variable LTPA had six possible answers, where each participant is asked in a single item, “How many hours a week do you usually exercise or play sports where you become breathless or have to sweat?” The answer categories of LTPA were, respectively: None, ½, 1, 2–3, 4–6, and 7 h or more. The selected cutoff values were based on studies by Holstein et al., McKercher et al., and The Danish Health and Medicines Authority's Health Profile.[4,18,19] The questionnaire used included CES-DS, to which we added questions regarding LTPA and demographic details. To validate the questionnaire, we conducted a prepiloting session with 25 individuals (18–25 year age group). During the session, all difficulties and shortcomings were noted by each of the authors and amendments were done with a unanimous decision of the authors. This was followed by a pilot study conducted on 50 individuals (18–25 year of age) taking an equal number of subjects from each institution.
A sample size of 359 was calculated considering the prevalence of poor mental health (as shown in previous studies)[9] to be 37.3%, at 95% confidence interval with a design effect of 1 using Epi Info v7. However, to account for nonresponse, 390 students were approached. All students who had acquired formal education up to 12th standard and were <25 years of age were included in the study. Those with a diagnosed mental health problem or with chronic morbidity were excluded. Twenty of the 390 students approached were not included as seven did not give their consent to participate and 13 did not satisfy all the inclusion criteria. Hence, the study was finally conducted on 370 students. The entire sample of 370 students was then divided into three parts; hence, the participants included were 124 from ITI, 126 from CU, and 120 from MC. In all the colleges, the total number of participants was equally divided among all the classes, i.e., from first to final year. The first roll number in each class was picked using the last digit on a currency note, and then, we picked the next student by adding the digit three to that number and so on till the required sample size was attained. The data collection was conducted from March to May 2016. Ethical approval was sought from Institute's Ethical Committee. Data were collected by the investigators after narrating the purpose of the study and taking prior consent.
Weight and height were measured using standard procedures. Weight was measured using a standardized portable scale. The individuals removed their shoes and heavy clothing while weighing. Height was measured using a stature meter. To record the height, the subjects stood with their scapula, buttocks and heels resting against a wall, the neck was held in a natural not stretched position, the heels were touching each other, the toe tips formed a 45° angle and the head was held straight such that Frankfurt plane was horizontal.
BMI was determined using the Quetlet's equation (ratio of weight in kilograms and square of height in meters). The cutoff values for defining obesity are in accordance with the guidelines given by the WHO, and these were further compared with the values calculated according to the consensus statement for Indians (i.e., 18–22.9 kg/m2 normal, 23–24.9 kg/m2 overweight, >25 kg/m2 obese) for comparison.[20]
Data presented as means and proportions were tested using Chi-square test, Fischer exact test, and ANOVA for mean using Epi Info 7 (CDC, Clifton Rd, Atlanta, GA, USA). Multiple regression analysis was applied, taking outcome variable as positive screen for depression and exposure variable as leisure-time PA, and the potential confounders were sex, native area of residence, type of institution, and BMI. P < 0.05 was considered statistically significant.
RESULTS
The sociodemographic profile of the students at the three institutes shows that 99.2% of the participants from the ITI were male, whereas the proportion of males in the samples from CU and MC were 62.7% and 42%, respectively [Table 1]. Majority of the students from ITI (100%) and CU (77%) were from rural areas, and 65% of students in the MC had an urban native background. The anthropometry of the participants showed that 8.9% of ITI students were overweight, while 25.6% of CU students and 25.8% of MC students were obese. LTPA in the week before the interview was reported to be high (≥4 h) in 18.3% MC students, 10.3% CU students, and 4% of ITI students.
Table 1.
Sociodemographic profile of study participants
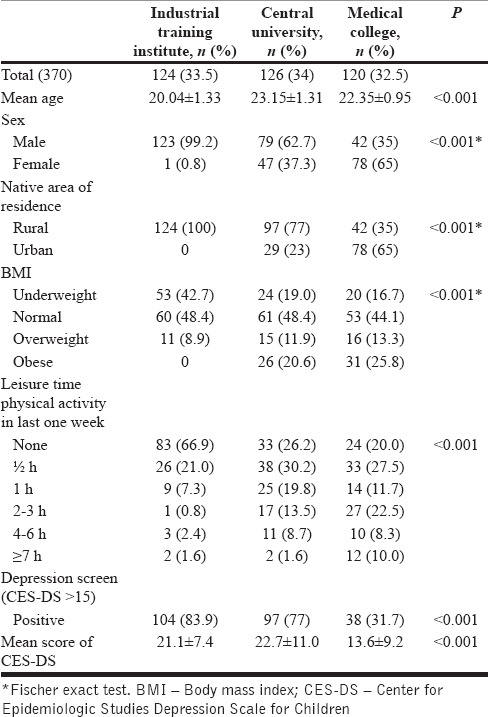
Higher CES-DC scores indicate increasing levels of depression. The cutoff score of 15 was used as suggestive of depressive symptoms. The mean CES-DC score was highest among CU students 22.7 (±11.0) and lowest among MC students 13.6 (±9.2). The difference in the mean scores across the three groups was found to be statistically significant (P < 0.001). Using this cutoff for the depression screen, it was observed that 83.9% of ITI, 77% of CU, and 31.7% of MC students were positive (had depressive symptoms) and the difference in proportion was statistically significant across the three groups (P < 0.001) [Table 1].
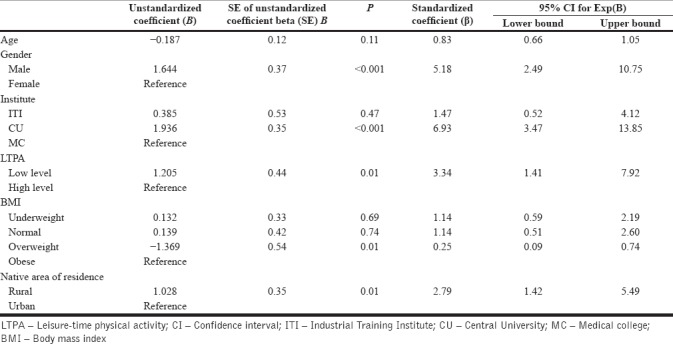
Overall low level of LTPA was reported by around 98% of females as compared to 84% males. Among males, a high proportion of low-level LTPA performing subjects screened positive for depression. Multiple logistic regression analysis showed that the odds of depression were three times higher in low-level LTPA group as compared to the high-level LTPA group (odds ratio [OR] [95% confidence interval [CI]; 3.34 [1.41–7.92]). Male sex, rural native background, underweight, and overweight were observed to be positively associated with risk of depression. Around 1.5 times higher risk of having a positive screen for depression was observed among ITI (OR [95% CI]; 1.47 [0.52–4.12]) and seven times higher in CU (OR [95% CI); 6.93 [3.47–13.85]) students as compared to MC students [Table 2].
Table 2.
Multiple logistic regression analysis showing association of leisure time physical activity with positive depression screen among all the study participants
DISCUSSION
The current community-based analysis on young people attending three different institutions used CES-DC scale to screen for depression and revealed an overall 64.6% positive screen for depression. According to the WHO, at least 20% of young people are likely to experience some form of mental illness such as depression, mood disturbances, substance abuse, suicidal behaviors, eating disorders, and others.[21] Global burden of disease study says that in India, 30% of the mental, neurological and substance abuse disorders are attributable to depressive disorder.[22] Youth is a critical phase of life, with major physical, physiological, psychological and behavioral changes. These changes are also accompanied by significant stress on young people, which influence and affect their relationship with their peers and adults.[23] In the current study, a major proportion of depression was reported from the students of ITI. Least was among medical graduate students. Type of education plays an important part. Probable reason could be that professional courses such as medicine are likely to provide more security and job satisfaction than vocational courses or nonprofessional degree.[24]
Around 40% of all participants reported no LTPA in last week, and high level (>4 h) was reported by 10% only. Globally, around 31% of adults aged 15 and over were insufficiently active in 2008.[25] It is recommended that adults aged 18–64 should do at least 150 min of moderate-intensity aerobic PA or do at least 75 min of vigorous-intensity aerobic PA throughout the week or an equivalent combination of moderate and vigorous-intensity activity.[26] The current study, however, did not measure the intensity of PA. The emerging public health issue of physical inactivity is mainly due to easy life due to access to technology and economic incentives which tend to discourage activity. The energy released during activity of daily living has been reduced over time due to the boon of technology. Majority of highly paid jobs are sedentary as compared to active work.[27]
Further stratification shows that inactivity was highest among students of ITI and less among medical graduates and CU students. One of the reasons in this scenario is awareness about PA, which tends to be higher among medical graduates and university students, who also get an opportunity for co-curricular activities on campus.
Positive screen for depression was higher among low LTPA performing students across all the institutes. A significant positive association was observed between low LTPA and depression, and after adjustment, the association persisted and strengthened. This suggests that relation of LTPA to depression is complex. It derives from a variety of other characteristics of an individual or his circumstances, yet it is not wholly attributable to the influence of any of these covariates or even the combination of all of them together. Bremnes et al.[6] examined the association between PA and depressive symptoms in adolescents. They found cross-sectional evidence that PA was inversely associated with depressive symptoms.
Male gender and rural area of residence were strong predictors in this study. The gender difference in our study population with regard to being physically active has been supported by previous studies, which have reported that boys (15.6%) are more physically active than girls (1.6%),[7,28,29,30,31] but that the girls more often report their mental health to be poor is not found in our analysis.[7,32,33,34,35] This divergent finding in our study could be due to a high proportion of male participants as very few female students attend ITI, different ages of the studies' populations, different cutoff values for levels of PA and different contexts. Majority of the participants belonged to a rural area. Hence, those with the risk of depression was also high for rural area.
Being overweight was also positively associated with a positive screen for depression. Increased sedentary behavior contributes to worsening depression and obesity, as well as directly links these two conditions. Vice versa, depression may cause increased sedentary activity secondary to depressed mood, fatigue, and decreased motivation. The combination of decreased PA and/or increased appetite can lead to unhealthy weight gain.[36] Obesity in the current analysis was, however, negatively associated with depression. The obese youth may have a tendency of giving socially desirable answers which could be one of the reasons for this contradictory finding. Among the obese, none of the medical graduate students screened positive for depression, hinting that single variable does not predict depression and that it is a complex phenomenon. Underweight was also positively associated with risk of depression, indicating toward body dissatisfaction which is a reliable predictor of depression.[37]
The association between PA and depression may be bidirectional: Depression may lead to decreased levels of exercise due to low motivation and energy and decreased exercise may be a risk factor for depression. A recent review of the literature showed that regular physical exercise significantly decreased the risk for developing depression in adult populations.[38]
Cross-sectional analyses have given evidence in favor of higher LTPA and low risk of depression among young adults. The causality has been proven by some population-based longitudinal studies,[38,39,40] but was absent in other studies.[31,41,42,43,44] De Moor et al., in their population-based analysis, hypothesized that one-third factor, that is, personality, influences PA behavior which has a direct causal effect on depression and anxiety. In addition, SES affects the biology of the above three variables simultaneously.[45] As per a review published by Mayo Clinic, regular exercise probably helps ease depression in a number of ways, which may include releasing feel-good brain chemicals (neurotransmitters, endorphins, and endocannabinoids) that may ease depression, reducing immune system chemicals that can worsen depression, and increasing body temperature, which may have calming effects.[46]
A onetime analysis does not give us evidence on causality, dose-response relationship, or the temporal association. In addition, the indicator of depression was based on self-reported symptoms, which may have reflected a variety of heterogeneous mood states. This only screens for depression and does not differentiate among subjects experiencing mild-to-severe dysphoric mood and those suffering from diagnosable episodes of clinical depression. This could also be the reason for the higher prevalence of depression in the current study. The intensity and frequency of PA have not been accounted for in the current analysis. In addition, measurement error could have occurred in the self-report measure of LTPA because of potential over-reporting of PA. This cohort will be followed up again for 1–3 years (depending on the batch/semester of the students enrolled) with these variables of PA and depression to establish causation.
Community-based studies are needed to generate baseline data using standard criteria for depression and anxiety and their predictors. The Mental Health Programme in India, through its school mental health services and college counseling services as a platform, can be used to incorporate moderate and vigorous forms of aerobic PA in the curriculum. In addition, motivation from teachers and counselors are an important part.
CONCLUSION
Leisure Time Physical Activity was found to be associated with lower rates of depression.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.World Health Organization. The Global Burden of Disease: 2011 Update (Data and Statistics) Geneva: World Health Organization; 2012. [Last accessed on 2016 Sep 19]. Available from: http://www.who.int/healthinfo/global_burden_disease/GBD_report_2004update_full.pdf?ua=1 . [Google Scholar]
- 2.Ammouri AA, Kaur H, Neuberger GB, Gajewski B, Choi WS. Correlates of exercise participation in adolescents. Public Health Nurs. 2007;24:111–20. doi: 10.1111/j.1525-1446.2007.00615.x. [DOI] [PubMed] [Google Scholar]
- 3.Jerstad SJ, Boutelle KN, Ness KK, Stice E. Prospective reciprocal relations between physical activity and depression in female adolescents. J Consult Clin Psychol. 2010;78:268–72. doi: 10.1037/a0018793. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.McKercher C, Sanderson K, Schmidt MD, Otahal P, Patton GC, Dwyer T, et al. Physical activity patterns and risk of depression in young adulthood: A 20-year cohort study since childhood. Soc Psychiatry Psychiatr Epidemiol. 2014;49:1823–34. doi: 10.1007/s00127-014-0863-7. [DOI] [PubMed] [Google Scholar]
- 5.Moksnes UK, Moljord IE, Espnes GA, Byrne DG. Leisure time physical activity does not moderate the relationship between stress and psychological functioning in Norwegian adolescents. Ment Health Phys Act. 2010;3:17–22. [Google Scholar]
- 6.Bremnes AJ, Martinussen M, Laholt H, Bania EV, Kvernmo S. The association between mental health and physical activity among high-school students. Tidsskr Nor Psykol Foren. 2011;48:332–8. [Google Scholar]
- 7.Motl RW, Birnbaum AS, Kubik MY, Dishman RK. Naturally occurring changes in physical activity are inversely related to depressive symptoms during early adolescence. Psychosom Med. 2004;66:336–42. doi: 10.1097/01.psy.0000126205.35683.0a. [DOI] [PubMed] [Google Scholar]
- 8.Kremer P, Elshaug C, Leslie E, Toumbourou JW, Patton GC, Williams J, et al. Physical activity, leisure-time screen use and depression among children and young adolescents. J Sci Med Sport. 2014;17:183–7. doi: 10.1016/j.jsams.2013.03.012. [DOI] [PubMed] [Google Scholar]
- 9.Hoegh Poulsen P, Biering K, Andersen JH. The association between leisure time physical activity in adolescence and poor mental health in early adulthood: A prospective cohort study. BMC Public Health. 2016;16:3. doi: 10.1186/s12889-015-2658-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Government of India. Registrar General and Census Commissioner, India, Population Totals. New Delhi: Government of India; 2011. [Google Scholar]
- 11.Park K. Textbook of Preventive and Social Medicine. 23rd ed. India: Banarsidas Bhanot Publishers; 2015. p. 482. Ch. 8. [Google Scholar]
- 12.List of Government Colleges in Himachal Pradesh. Department of Higher Education. Himachal Pradesh. 2011. [Last accessed on 2016 Sep 24]. Available from: http://www.educationhp.org/colleges.html .
- 13.Carleton RN, Thibodeau MA, Teale MJ, Welch PG, Abrams MP, Robinson T, et al. The center for epidemiologic studies depression scale: A review with a theoretical and empirical examination of item content and factor structure. PLoS One. 2013;8:e58067. doi: 10.1371/journal.pone.0058067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Fendrich M, Weissman MM, Warner V. Screening for depressive disorder in children and adolescents: Validating the center for epidemiologic studies depression scale for children. Am J Epidemiol. 1990;131:538–51. doi: 10.1093/oxfordjournals.aje.a115529. [DOI] [PubMed] [Google Scholar]
- 15.Smarr KL, Keefer AL. Measures of depression and depressive symptoms: Beck depression inventory-II (BDI-II), center for epidemiologic studies depression scale (CES-D), geriatric depression scale (GDS), hospital anxiety and depression scale (HADS), and patient health questionnaire-9 (PHQ-9) Arthritis Care Res (Hoboken) 2011;63(Suppl 11):S454–66. doi: 10.1002/acr.20556. [DOI] [PubMed] [Google Scholar]
- 16.Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985;100:126–31. [PMC free article] [PubMed] [Google Scholar]
- 17.Kandula NR, Lauderdale DS. Leisure time, non-leisure time, and occupational physical activity in Asian Americans. Ann Epidemiol. 2005;15:257–65. doi: 10.1016/j.annepidem.2004.06.006. [DOI] [PubMed] [Google Scholar]
- 18.Christensen AI, Davidsen M, Ekholm O, Pedersen PV, Juel K. Danskernes Sundhed: Den Nationale Sundhedsprofil 2013. Copenhagen: Danish Health and Medicines Authority; 2014. [Google Scholar]
- 19.World Health Organization. Physical Activity and Young People: Global Strategy on Diet, Physical Activity and Health. Geneva: WHO; 2011. [Google Scholar]
- 20.Misra A, Chowbey P, Makkar BM, Vikram NK, Wasir JS, Chadha D, et al. Consensus statement for diagnosis of obesity, abdominal obesity and the metabolic syndrome for Asian Indians and recommendations for physical activity, medical and surgical management. J Assoc Physicians India. 2009;57:163–70. [PubMed] [Google Scholar]
- 21.World Health Organization. Young People: Health Risks and Solutions. Fact Sheet No 345. World Health Organization. 2011. [Last accessed on 2016 Sep 18]. Available from: http://www.who.int/mediacentre/factsheets/fs345/en/index.html .
- 22.Charlson FJ, Baxter AJ, Cheng HG, Shidhaye R, Whiteford HA. The burden of mental, neurological, and substance use disorders in China and India: A systematic analysis of community representative epidemiological studies. Lancet. 2016;388:376–89. doi: 10.1016/S0140-6736(16)30590-6. [DOI] [PubMed] [Google Scholar]
- 23.Singh S, Gopalkrishna G. Health behaviours & problems among young people in India: Cause for concern & call for action. Indian J Med Res. 2014;140:185–208. [PMC free article] [PubMed] [Google Scholar]
- 24.Jamil H, Kanno SS, Abo-Shasha R, AlSaqa MM, Fakhouri M, Arnetz BB, et al. Promoters and barriers to work: A comparative study of refugees versus immigrants in the United States. New Iraqi J Med. 2012;8:19–28. [PMC free article] [PubMed] [Google Scholar]
- 25.World Health Organization. Physical Activity: Fact Sheet. Geneva: World Health Organization; 2016. [Last accessed on Sep 18]. Available from: http://www.who.int/mediacentre/factsheets/fs385/en/ [Google Scholar]
- 26.Haskell WL, Lee IM, Pate RR, Powell KE, Blair SN, Franklin BA, et al. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Circulation. 2007;116:1081–93. doi: 10.1161/CIRCULATIONAHA.107.185649. [DOI] [PubMed] [Google Scholar]
- 27.Rothon C, Edwards P, Bhui K, Viner RM, Taylor S, Stansfeld SA, et al. Physical activity and depressive symptoms in adolescents: A prospective study. BMC Med. 2010;8:32. doi: 10.1186/1741-7015-8-32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Sund AM, Larsson B, Wichstrøm L. Role of physical and sedentary activities in the development of depressive symptoms in early adolescence. Soc Psychiatry Psychiatr Epidemiol. 2011;46:431–41. doi: 10.1007/s00127-010-0208-0. [DOI] [PubMed] [Google Scholar]
- 29.Rangul V, Holmen TL, Bauman A, Bratberg GH, Kurtze N, Midthjell K, et al. Factors predicting changes in physical activity through adolescence: The Young-HUNT study, Norway. J Adolesc Health. 2011;48:616–24. doi: 10.1016/j.jadohealth.2010.09.013. [DOI] [PubMed] [Google Scholar]
- 30.Holstein BE, Henriksen PE, Krølner R, Rasmussen M, Due P. Trends in vigorous physical activity versus physical inactivity among 11-15 year olds from 1988 to 2002. Ugeskr Laeger. 2007;169:37–42. [PubMed] [Google Scholar]
- 31.Toseeb U, Brage S, Corder K, Dunn VJ, Jones PB, Owens M, et al. Exercise and depressive symptoms in adolescents: A longitudinal cohort study. JAMA Pediatr. 2014;168:1093–100. doi: 10.1001/jamapediatrics.2014.1794. [DOI] [PubMed] [Google Scholar]
- 32.Hume C, Timperio A, Veitch J, Salmon J, Crawford D, Ball K, et al. Physical activity, sedentary behavior, and depressive symptoms among adolescents. J Phys Act Health. 2011;8:152–6. doi: 10.1123/jpah.8.2.152. [DOI] [PubMed] [Google Scholar]
- 33.Desha LN, Ziviani JM, Nicholson JM, Martin G, Darnell RE. Physical activity and depressive symptoms in American adolescents. J Sport Exerc Psychol. 2007;29:534–43. doi: 10.1123/jsep.29.4.534. [DOI] [PubMed] [Google Scholar]
- 34.Skrove M, Romundstad P, Indredavik MS. Resilience, lifestyle and symptoms of anxiety and depression in adolescence: The Young-HUNT study. Soc Psychiatry Psychiatr Epidemiol. 2013;48:407–16. doi: 10.1007/s00127-012-0561-2. [DOI] [PubMed] [Google Scholar]
- 35.Reeves GM, Postolache TT, Snitker S. Childhood obesity and depression: Connection between these growing problems in growing children. Int J Child Health Hum Dev. 2008;1:103–14. [PMC free article] [PubMed] [Google Scholar]
- 36.Cash TF, Morrow JA, Hrabosky JI, Perry AA. How has body image changed? A cross-sectional investigation of college women and men from 1983 to 2001. J Consult Clin Psychol. 2004;72:1081–9. doi: 10.1037/0022-006X.72.6.1081. [DOI] [PubMed] [Google Scholar]
- 37.Teychenne M, Ball K, Salmon J. Physical activity and likelihood of depression in adults: A review. Prev Med. 2008;46:397–411. doi: 10.1016/j.ypmed.2008.01.009. [DOI] [PubMed] [Google Scholar]
- 38.Camacho TC, Roberts RE, Lazarus NB, Kaplan GA, Cohen RD. Physical activity and depression: Evidence from the Alameda county study. Am J Epidemiol. 1991;134:220–31. doi: 10.1093/oxfordjournals.aje.a116074. [DOI] [PubMed] [Google Scholar]
- 39.Farmer ME, Locke BZ, Mościcki EK, Dannenberg AL, Larson DB, Radloff LS, et al. Physical activity and depressive symptoms: The NHANES I epidemiologic follow-up study. Am J Epidemiol. 1988;128:1340–51. doi: 10.1093/oxfordjournals.aje.a115087. [DOI] [PubMed] [Google Scholar]
- 40.Strawbridge WJ, Deleger S, Roberts RE, Kaplan GA. Physical activity reduces the risk of subsequent depression for older adults. Am J Epidemiol. 2002;156:328–34. doi: 10.1093/aje/kwf047. [DOI] [PubMed] [Google Scholar]
- 41.Allison KR, Adlaf EM, Irving HM, Hatch JL, Smith TF, Dwyer JJ, et al. Relationship of vigorous physical activity to psychologic distress among adolescents. J Adolesc Health. 2005;37:164–6. doi: 10.1016/j.jadohealth.2004.08.017. [DOI] [PubMed] [Google Scholar]
- 42.Cooper Patrick L, Ford DE, Mead LA, Chang PP, Klag MJ. Excercise and depression in midlife: A prospective study. Am J Public Health. 1997;87:670–3. doi: 10.2105/ajph.87.4.670. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Kritz-Silverstein D, Barrett-Connor E, Corbeau C. Cross-sectional and prospective study of exercise and depressed mood in the elderly: The Rancho Bernardo Study. Am J Epidemiol. 2001;153:596–603. doi: 10.1093/aje/153.6.596. [DOI] [PubMed] [Google Scholar]
- 44.Weyerer S. Physical inactivity and depression in the community. Evidence from the Upper Bavarian Field Study. Int J Sports Med. 1992;13:492–6. doi: 10.1055/s-2007-1021304. [DOI] [PubMed] [Google Scholar]
- 45.De Moor MH, Beem AL, Stubbe JH, Boomsma DI, De Geus EJ. Regular exercise, anxiety, depression and personality: A population-based study. Prev Med. 2006;42:273–9. doi: 10.1016/j.ypmed.2005.12.002. [DOI] [PubMed] [Google Scholar]
- 46.Depression and Anxiety: Exercise Eases Symptoms – Mayo Clinic. [Last accessed on 2017 Jan 12]. Available from: http://www.mayoclinic.org/diseases..../depression/in-depth/depression....exercise/art-2004649 .