

Abstract
Objective:
Borderline personality disorder affects up to 2% of the population and is associated with poor functioning, low quality of life and increased mortality. Psychotherapy is the treatment of choice, but it is unclear whether specialized psychotherapies (dialectical behavior therapy, mentalization-based treatment, transference-focused therapy and schema therapy) are more effective than non-specialized approaches (e.g. protocolized psychological treatment, general psychiatric management). The aim of this systematic review is to investigate the effectiveness of these psychotherapies.
Methods:
PubMed, PsycINFO, CINAHL, EMBASE and CENTRAL were searched from inception to November 2017. Included randomized controlled trials were assessed on risk of bias and outcomes were meta-analyzed. Confidence in the results was assessed using the Grading of Recommendations Assessment, Development and Evaluation method. The review has been reported following Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
Results:
A total of 20 studies with 1375 participants were included. Specialized psychotherapies, when compared to treatment as usual or community treatment by experts, were associated with a medium effect based on moderate quality evidence on overall borderline personality disorder severity (standardized mean difference = –0.59 [95% confidence interval: –0.90, –0.28]), and dialectical behavior therapy, when compared to treatment as usual, with a small to medium effect on self-injury (standardized mean difference = –0.40 [95% confidence interval: –0.66, –0.13]). Other effect estimates were often inconclusive, mostly due to imprecision.
Conclusion:
There is moderate quality evidence that specialized psychotherapies are effective in reducing overall borderline personality disorder severity. However, further research should identify which patient groups profit most of the specialized therapies.
Keywords: Review, meta-analysis, psychotherapy, borderline personality disorder
Introduction
Borderline personality disorder (BPD) is the most common personality disorder and affects approximately 0.7–2% of the population (Torgersen, 2012). The disorder has a substantial negative impact on people’s lives, demonstrated by poor functioning, high (attempted) suicide rate, and high mental and physical comorbid problems (Samuels, 2011; Tomko et al., 2014). Pharmacotherapy is usually not advised to address general BPD severity (Lieb et al., 2004; NICE, 2009), yet psychological treatments have been examined and some have shown benefit (Cristea et al., 2017; NICE, 2009; Stoffers et al., 2012). Among these psychological treatments, four were designed to specifically address BPD, and these may be superior to others (Bloom et al., 2012; Cristea et al., 2017; Kliem et al., 2010; Stoffers et al., 2012). We have called these ‘specialized psychotherapies’ and they are dialectical behavior therapy (DBT), mentalization-based treatment (MBT), transference-focused therapy (TFP) and schema therapy (ST; formerly schema-focused therapy, SFT). Specialized psychotherapies share several commonalities: they are all are based on theories about the etiology and maintaining factors of BPD and have published detailed protocols on the treatment of BPD and therapeutic techniques, as well as on managing the therapeutic relationship. In other words, only specialized psychotherapies specifically designed as a ‘complete therapy’ for BPD were included, but generic treatments as cognitive behavioral therapy (CBT), and adjunct treatments as systems training for emotional predictability and problem solving (STEPPS) are not.
A comprehensive meta-analysis on non-pharmacological interventions by Stoffers et al. (2012) investigated the effectiveness of individual specialized psychotherapies for BPD and found low certainty of the evidence due to the small number of studies for each specialized psychotherapy separately. Since then, the number of randomized controlled trials (RCTs) and follow-up of existing studies has increased. A recent meta-analysis by Cristea et al. (2017) included all specialized and other psychotherapies. Cristea et al. pooled psychotherapies together on a high aggregated level (standalone vs add-on) and grouped the outcomes in categories to create a strong evidence base. However, their review does not focus on the effectiveness of specialized psychotherapies and did not include studies in which one psychotherapy was compared to another psychotherapy (head-to-head trials) to examine the comparative effectiveness.
Aims
The aim of our meta-analysis was to investigate whether specialized psychotherapies are effective for adults with BPD on overall BPD severity, single BPD symptoms (e.g. avoidance of abandonment, dysfunctional interpersonal patterns, identity disturbance, impulsivity, suicidal ideation, suicidal behavior, self-injurious behavior, affective instability, feelings of emptiness, anger and dissociative symptoms) and dropout. By pooling all specialized psychotherapies together we aim to create a more solid and clinically useful evidence base. In addition, we investigated the comparative effectiveness of individual specialized psychotherapies.
Methods
The review is reported following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2009).
Eligibility criteria
We included RCTs on four specialized psychotherapies (DBT, MBT, TFP and ST) for adults (18 years and older) with BPD, which included an individual psychotherapy component and had a duration of 16 weeks or more. Eligible comparison groups were other protocolized and specialized psychotherapies, or control groups, for example, treatment as usual (TAU), waiting list, attention control or community treatment by experts (CTBE). In studies that also included participants with other personality disorders (e.g. antisocial), we contacted the authors and requested disaggregated data. Studies were excluded with an arbitrary cut-off of <66% of the participants having BPD, unless disaggregated data were provided. Also, studies were excluded that tested incomplete versions of specialized treatment, for example, studies that investigated only skills training instead of the full DBT program.
Search strategy
We searched PubMed, PsycINFO, CINAHL, EMBASE and CENTRAL from inception to the 13 November 2017 using terms for BPD, psychotherapy and RCTs (Supplementary Material A). Subsequently, we searched the World Health Organization (WHO) International Clinical Trials Registry, reference lists of the included studies, excluded studies and previous reviews. We also contacted authors of (ongoing) studies to request additional data.
Assessment of bias
Included studies were assessed independently by two authors (M.O., R.V.) using the Cochrane Collaboration Risk of Bias Assessment Tool (Higgins and Green, 2008). Disagreements were discussed and resolved by consensus. Each study was rated for risk of bias due to sequence generation, allocation concealment, masking of participants, assessors and providers, selective outcome reporting, incomplete data and allegiance effect. Risk of bias for each domain was rated as high (seriously weakens confidence in the effect estimate), low (unlikely to seriously alter the effect estimate) or unclear. Inter-rater reliability (IRR) of the initial risk of bias rating was examined with a two-way mixed model, absolute agreement and average-measures intra-class correlations (ICCs). Inter-rater agreement was satisfactory, with ICCs ranging from 0.545 to 0.770 with a mean of 0.649, median of 0.643 and standard deviation of 0.08.
Data management
Service user outcomes included overall BPD severity, single BPD symptoms (e.g. avoidance of abandonment, dysfunctional interpersonal patterns, identity disturbance, impulsivity, suicidal ideation, suicidal behavior, self-injurious behavior, affective instability, feelings of emptiness, anger and dissociative symptoms) and dropout. Continuous measures are listed in Supplementary Material B. We also extracted treatment format, number and length of sessions, age, sex, setting and study location. For each study, the important study characteristics are reported in Table 1. If data were missing or could not be meta-analyzed, authors were contacted and additional data were requested.
Table 1.
Characteristics of the included studies.
| Study | Country | Setting | Mean age | % Female | Intervention | N total per arm | Treatment completers % | Hours of contact per week | Duration (weeks) | Follow-up (weeks) |
|---|---|---|---|---|---|---|---|---|---|---|
| Priebe et al. (2012) | UK | Outpatients | 32.2 | 87.5 | DBT vs TAU | 40, 40 | 47.5, 100 | 3 | 52 | – |
| Feigenbaum et al. (2012) | UK | Outpatients | 35.1 | 73 | DBT vs TAU | 26, 16 | 42.3, 93.8 | 3.5 | 52 | – |
| Linehan et al. (1991)a | US | Outpatients | 18–45 | 100 | DBT vs TAU | 30, 31 | 73.3, 71 | NR | 52 | – |
| Linehan et al. (1994)b | US | Outpatients | 26.7 | 100 | DBT vs TAU | 13, 13 | 100, 100 | NR | 52 | – |
| Van Den Bosch et al. (2005) | NL | Outpatients | 34.9 | 100 | DBT vs TAU | 31, 33 | 77.4, 51.5 | 3.5 | 52 | – |
| Linehan et al. (2006) | US | Outpatients | 29.3 | 100 | DBT vs CTBE | 52, 49 | 80.8, 57.1 | 3.5 | 52 | 104 |
| McMain et al. (2009) | CA | Outpatients | 30.4 | 86.8 | DBT vs PPT (GPM) | 90, 90 | 62.2, 61.1 | 5, 1 | 52 | 156 |
| US | Outpatients | 22.0 | 79.2 | DBT vs PPT (CCT) | 12, 12 | 75, 50 | NR | 52 | – | |
| Carter et al. (2010) | AUS | Outpatients | 42.5 | 100 | DBT vs TAU | 38, 35 | 52.6, 88.6 | NR | 26 | – |
| Koons et al. (2001) | US | Outpatients | 35.0 | 100 | DBT vs TAU | 14, 14 | 71.4, 71.4 | 3 | 26 | – |
| Steil et al. (2011)/Bohus et al. (2013) | DE | Hospitalized patients | 35.9 | 100 | DBT-PTSD vs TAU | 17, 16 | 82, 81 | 5.9 | 20 | – |
| Linehan et al. (2015) | US | Outpatients | 30.3 | 100 | DBT vs DBT-S vs DBT-I | 33, 33, 33 | 75.8, 51.5, 60.6 | 1,a 0.7,a 0.6a | 52 | 104 |
| Harned et al. (2014) | US | Outpatients | 32.6 | 100 | DBT vs DBT-PEP | 9, 17 | 55.6, 59.9 | 3.5, 5.8 | 52 | 65 |
| Doering et al. (2010) | DE/AT | Outpatients | 27.3 | 100 | TFP vs CTBE | 52, 52 | 86.5, 75 | 1.7 | 52 | – |
| Clarkin et al. (2007) | US | Outpatients | 30.9 | 92.2 | TFP vs DBT vs SPT | 31, 30, 29 | 74.1, 46.7, 75.9 | 1.7, 2.5, 0.8 | 52 | – |
| Bateman and Fonagy (1999b) | UK | Partially hospitalized patients | 31.8 | 57.9 | MBT-PH vs TAU | 22, 22 | 31.8, 86.4 | 6.5 | 78 | – |
| Jorgensen et al. (2013) | DK | Outpatients | 29.2 | 95.5 | MBT vs CTBE (SGP) | 74, 37 | 52.7, 51.4 | 1.9 | 104 | – |
| Bateman and Fonagy (2009) | UK | Outpatients | 31.3 | 79.9 | MBT-out vs PPT (SCM) | 71, 63 | 73.2, 74.6 | 6.5 | 78 | – |
| Giesen-Bloo et al. (2006) | NL | Outpatients | 30.6 | 93.0 | ST vs TFP | 45, 43 | 73.3, 48.8 | 1.7, 1.7 | 156 | – |
| Farrell et al. (2009) | US | Outpatients | 35.6 | 100 | ST vs TAU | 16, 16 | 100, 75 | 1.5 | 35 | – |
| Nadort et al. (2009) | NL | Outpatients | 32.0 | 96.8 | ST vs ST + TTA | 32, 30 | 78.1, 80 | 1.5, 1.5 | 78 | – |
TAU: treatment as usual; CCT: client-centered therapy; CTBE: community treatment by experts; PPT: protocolized psychological treatment; GPM: general psychiatric management according to APA guidelines; DBT: dialectical behavior therapy; MBT: metallization-based therapy; out: outpatient; PH: partially hospitalized; PTSD: post-traumatic stress disorder; SCM: structured clinical management; ST: schema(-focused) therapy; SGP: supported group psychotherapy; SPT: supportive psychotherapy; TTA: therapist telephone availability; TAU; treatment as usual; TFP: transference focused psychotherapy; I: individual therapy plus activities group; S: skills training plus case management; PEP: prolonged exposure protocol; NR: not reported; AUS: Australia; CA: Canada; DE: Germany; DK: Denmark; ES: Spain; UK: United Kingdom; NL: Netherlands; US: United States; AT: Austria.
Patients from the same trial
True amount of contact per week (mean for the whole group).
Statistical analysis
For continuous outcomes, we calculated the standardized mean difference (SMD), Hedges’ g, for between-group differences. SMDs were considered small (0.2 ⩽ SMD < 0.5), medium (0.5 ⩽ SMD < 0.8) or large (SMD ⩾ 0.8) (Cohen, 1988). For dichotomous outcomes, we calculated the risk ratio (RR) for events. If continuous and dichotomous effect estimates were reported for an outcome, we transformed RRs into SMDs so that effect estimates could be pooled. All outcomes are reported with 95% confidence intervals (CIs). Overall effects were calculated using random effects models. Continuous effects were weighted by the inverse of variance; dichotomous effects were weighted using the Mantel–Haenszel method (Higgins and Green, 2008).
Statistical heterogeneity was assessed by visual inspection of forest plots, by performing the χ2 test (assessing the p value), and by calculating the I2 statistic, which describes the percentage of observed heterogeneity that would not be expected by chance. If the p value was less than 0.10 and I2 exceeded 50%, we considered heterogeneity to be substantial. Meta-analyses of comparisons and subgroups were conducted using Review Manager (RevMan) 5.3 (Nordic Cochrane Centre, 2014). Confidence in the effect estimates were assessed by M.O. and M.L.M.H. using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) method (Guyatt et al., 2011), which is a structured assessment of the quality of evidence attending to the following factors: risk of bias, inconsistency, indirectness, imprecision and publication bias. Outcomes can be ‘downgraded’ on the basis of these factors resulting in ‘high’, ‘moderate’, ‘low’ or ‘very low’ confidence in the effect estimate.
Results
Study flow
Of 1013 potentially relevant citations, we retrieved papers of 29 distinct studies, which were assessed for inclusion (Figure 1). Of these, nine studies were excluded due to several reasons: the duration of the intervention was not sufficient (<16 weeks of therapy), no individual treatment component was present to be regarded as a specialized psychotherapy, <66% of the participants were diagnosed with BPD, and no RCT. In total, 63 papers of 20 studies were, therefore, included, which were published between 2014 and 2015.
Figure 1.

Study selection.
Study characteristics
Characteristics of each study are presented in Table 1. Included studies randomized 1375 participants, ranging from 24 to 180 per study. Studies were conducted in North America (k = 10), United Kingdom (k = 4), continental Europe (k = 5) and Australia (k = 1). Participants were mostly treated in outpatient settings (k = 18); only one study was conducted in an inpatient setting, and in another participants were partially hospitalized. In almost all studies a structured diagnostic interview was used to assess and establish the presence of BPD, most commonly with a version of the Structured Clinical Interview for DSM Personality Disorders (SCID-II), one study (Farrell et al., 2009) did not and used the diagnostic interview for borderline patients–revised (DIB-R; Zanarini et al., 1990). Only 4 of the 20 studies had follow-up data, ranging from 65 to 156 weeks. Across all studies, the median of the mean age of participants was 32 years (range, 22–43) and almost all participants were female (mean = 93%, range = 58–100%).
Interventions
The included studies investigated a variety of interventions (Supplementary Material C). A team of four clinical experts independently classified treatments, and disagreements were resolved in a consensus meeting. This process resulted in 10 comparisons for meta-analysis. Specialized psychotherapies were compared with TAU, with CTBE and with protocolized psychological treatment, which comprised general psychiatric management (GPM), structured clinical management (SCM) and client-centered therapy (CCT). The other seven comparisons were head-to-head comparisons, of which two compared different types of specialized therapies (DBT vs TFP and ST vs TFP). Two other comparisons investigated the efficacy of add-on interventions (ST with or without therapist telephone availability; DBT with or without prolonged exposure). Finally, in three comparisons, DBT was compared with two interventions containing DBT elements (one with only individual therapy plus group activities and the other with only group skills training and case management); these semi-DBT interventions were compared with each other in the final comparison.
Risk of bias
Risk of bias per study is presented in Figure 2, and two references are on the same study (Linehan et al., 1991, 1994). No studies were at high risk of bias for random sequence generation; however, the method of randomization was not reported in four studies. Allocation concealment was unclear in 7 studies and had a low risk in 14 studies. Masking of participants and providers in studies of psychological interventions is impossible and therefore all were at high risk of bias. Four of the studies did not have masked assessors and these were considered to be at high risk of bias. Regarding incomplete outcome data, seven were at high risk of bias because of the number (more than 10%) of missing cases or because missing cases were excluded from the analyses. Six studies were at high risk of allegiance bias, because the developers of the treatment protocol were also involved in the research investigating the efficacy.
Figure 2.
Risk of bias summary.
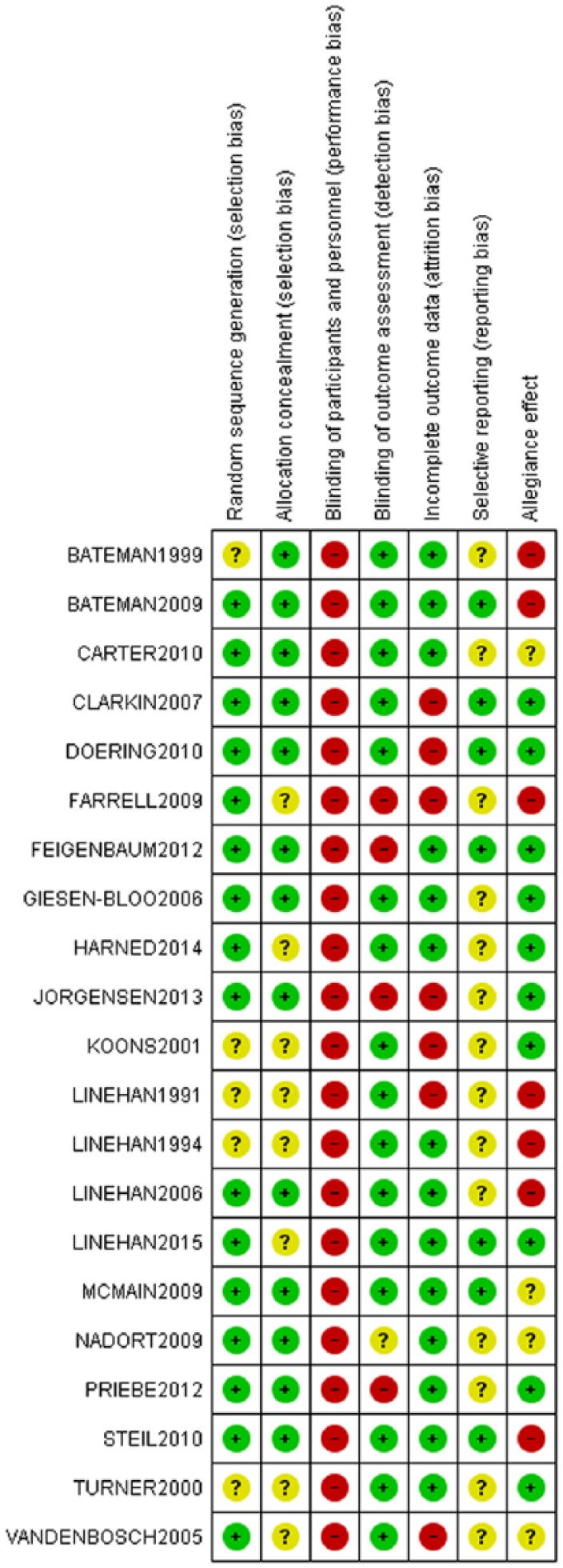
Risk of bias was rated as low (+), high (–) or unclear (?) using the Cochrane Risk of Bias Tool (Higgins and Green, 2008).
Reporting bias
There was no high risk of selective outcome reporting. Only four studies were prospectively registered; all others were at unclear risk of bias. Risk of publication bias could not be assessed by means of funnel plots because there were too few studies for all comparisons.
Overall quality of the evidence
All outcomes were downgraded due to imprecision of the effect estimates (wide CIs because of few participants or events). Effect estimates for overall BPD severity and self-injury following specialized therapy were of moderate quality, as rated with the GRADE method. Most other evidence was rated low or very low. A small number of studies also reported follow-up data; overall these outcomes were of low quality.
Quantitative data synthesis
Effect estimates of the meta-analyses suggest that specialized therapies are associated with improvement in overall BPD severity and with a reduction in self-injury (Tables 2 and 3). All outcomes are summarized for each comparison and subgroup in Supplementary Material D and E, including reasons for downgrading. Very low quality outcomes can be found in the supplementary material, too, but we will not report on all of these in the treatment results described below.
Table 2.
Outcomes at post-treatment.
| Outcome | Sub-analysis | Trials (reference) | N | Effect size | [95% CI] | Heterogeneity (I²) | Intervention length (weeks) | Quality (GRADE) |
|---|---|---|---|---|---|---|---|---|
| SMD below zero or a RR below 1 means the treatment (condition) was more effective than the comparator (condition) | ||||||||
| 1. Specialized psychotherapy versus treatment as usual (TAU) | ||||||||
| Overall BPD severity | Total | 4 | 151 | SMD = –0.75 | [–1.30, –0.19] | 58% | 20–52 | Lowb,d |
| DBT | (Priebe et al., 2012; Koons et al., 2001) | 90 | SMD = –0.36 | [–0.78, 0.05] | 0% | 26–52 | ||
| DBT-PTSD | (Steil et al., 2011) | 33 | SMD = –0.85 | [–1.57, –0.13] | N/A | 20 | ||
| SFT-Group | (Farrell et al., 2009) | 28 | SMD = –1.66 | [–2.54, –0.78] | N/A | 35 | ||
| Self-injury | Total | 7 | 314 | SMD = –0.33 | [–0.57, –0.09] | 0% | 26–78 | Moderated |
| DBT | (Feigenbaum et al., 2012; Koons et al., 2001; Linehan et al., 1991; Priebe et al., 2012; Van Den Bosch et al., 2005) | 225 | SMD = –0.40 | [–0.66, –0.13] | 0% | 26–52 | Moderated | |
| (Carter et al., 2010) | 51 | RR = 1.11 | [0.78, 1.57] | N/A | 26 | |||
| MBT-PH | (Bateman and Fonagy, 1999a) | 38 | RR = 0.44 | [0.24, 0.81] | N/A | 78 | ||
| Dropout | Total | 10 | 486 | RR = 1.54 | [0.70, 3.38] | 76% | 20–78 | Lowb,d |
| 2. Specialized psychotherapy versus community treatment by experts (CTBE) | ||||||||
| Overall BPD severity | Total | 2 | 170 | SMD = –0.47 | [–0.78, –0.16] | 0% | 52–104 | Moderated |
| MBT | (Jorgensen et al., 2013) | 66 | SMD = –0.33 | [–0.84, 0.17] | N/A | 104 | ||
| TFP | (Doering et al., 2010) | 104 | SMD = –0.55 | [–0.95, –0.16] | N/A | 52 | ||
| Self-injury | TFP | (Doering et al., 2010) | 104 | RR = 1.09 | [0.84, 1.40] | N/A | 52 | Lowd |
| Dropout | Total | 3 | 316 | RR = 0.62 | [0.39, 0.99] | 73% | 52–104 | Lowb,d |
| 3. Specialized psychotherapy versus protocolized psychological treatment | ||||||||
| Overall BPD severity | DBT vs GPM | (McMain et al., 2009) | 180 | SMD = –0.04 | [–0.33, 0.25] | N/A | 52 | Lowd |
| Self-injury | Total | 2 | 122 | RR = 0.80 | [0.42, 1.55] | 80% | 52–78 | Very lowb,c,d |
| DBT vs GPM | (McMain et al., 2009) | 177 | RR = 1.09 | [0.79, 1.50] | N/A | 52 | Lowd | |
| MBT-PH or out vs SCM | (Bateman and Fonagy, 1999b) | 134 | RR = 0.56 | [0.34, 0.92] | N/A | 78 | Moderated | |
| Self-injury | DBT vs CCT | (Turner, 2000) | 24 | SMD = –1.28 | [–2.17, –0.38] | N/A | 52 | Lowd |
| Dropout | Total | 4 | 265 | RR = 1.06 | [0.81, 1.40] | 0% | 52–78 | Lowc,d |
| 4. Dialectical behavior therapy vs transference-focused psychotherapy (TFP) | ||||||||
| Suicidal behavior | DBT vs TFP | (Clarkin et al., 2007) | 39 | SMD = 0.13 | [–0.51, 0.76] | N/A | 52 | Very lowa,d |
| Dropout | DBT vs TFP | (Clarkin et al., 2007) | 39 | RR = 2.07 | [1.04, 4.10] | N/A | 52 | Very lowa,d |
| 5. Schema(-focused) therapy (ST) vs transference-focused psychotherapy (TFP) | ||||||||
| Overall BPD severity | ST vs TFP | (Giesen-Bloo et al., 2006) | 86 | SMD = –0.45 | [–0.87, –0.02] | N/A | 156 | Lowd |
| Dropout | ST vs TFP | (Giesen-Bloo et al., 2006) | 88 | RR = 0.52 | [0.30, 0.92] | N/A | 156 | Lowd |
| 6. Schema(-focused) therapy (ST) vs ST + TTA | ||||||||
| Overall BPD severity | ST vs ST + TTA | (Nadort et al., 2009) | 61 | SMD = 0.13 | [–0.51, 0.76] | N/A | 78 | Lowd |
| Dropout | ST vs ST + TTA | (Nadort et al., 2009) | 62 | RR = 0.91 | [0.35, 2.41] | N/A | 78 | Lowd |
| 7. DBT vs DBT prolonged exposure protocol (DBT-PEP) | ||||||||
| Self-injury | DBT vs DBT-PEP | (Harned et al., 2014) | 18 | SMD = 0.05 | [–0.93, 1.03] | N/A | 52 | Lowd |
| Dropout | DBT vs DBT-PEP | (Harned et al., 2014) | 18 | RR = 1.35 | [0.60, 3.05] | N/A | 52 | Lowd |
| 8. DBT vs DBT-S (skills training plus case management) | ||||||||
| Self-injury | DBT vs DBT-S | (Linehan et al., 2015) | 66 | SMD = 0.02 | [–0.47, 0.50] | N/A | 52 | Lowd |
| Self-injury | DBT vs DBT-S | (Linehan et al., 2015) | 66 | RR = 1.06 | [0.69, 1.62] | N/A | 52 | Lowd |
| Dropout | DBT vs DBT-S | (Linehan et al., 2015) | 66 | RR = 0.50 | [0.25, 1.01] | N/A | 52 | Lowd |
| 9. DBT vs DBT-I (individual therapy plus activities group) | ||||||||
| Self-injury | DBT vs DBT-I | (Linehan et al., 2015) | 66 | SMD = –0.39 | [–0.88, 0.09] | N/A | 52 | Lowd |
| Self-injury | DBT vs DBT-I | (Linehan et al., 2015) | 66 | RR = 0.90 | [0.61, 1.34] | N/A | 52 | Lowd |
| Dropout | DBT vs DBT-I | (Linehan et al., 2015) | 66 | RR = 0.62 | [0.29, 1.29] | N/A | 52 | Lowd |
| 10. DBT-I vs DBT-S | ||||||||
| Self-injury | DBT-I vs DBT-S | (Linehan et al., 2015) | 66 | SMD = 0.39 | [–0.10, 0.88] | N/A | 52 | Lowd |
| Self-injury | DBT-I vs DBT-S | (Linehan et al., 2015) | 66 | RR = 1.17 | [0.78, 1.75] | N/A | 52 | Lowd |
| Dropout | DBT-I vs DBT-S | (Linehan et al., 2015) | 66 | RR = 0.81 | [0.47, 1.41] | N/A | 52 | Lowd |
GRADE: Grading of Recommendations Assessment, Development and Evaluation; BPD: borderline personality disorder; DBT: dialectical behavior therapy; PTSD: post-traumatic stress disorder; SFT: schema-focused therapy; MBT: mentalization-based treatment; PH: partially hospitalized; GPM: general psychiatric management according to APA guidelines; SCM: structured clinical management; CCT: client-centered therapy; TTA: therapist telephone availability; N/A: not applicable; SMD: standardized mean difference; RR: risk ratio.
Risk of bias.
Inconsistency.
Indirectness.
Imprecision.
Publication/reporting bias.
Table 3.
Outcomes at follow-up.
| Outcome | Sub-analysis | Trials (reference) | N | Effect Size | [95% CI] | Heterogeneity (I2) |
Intervention length (weeks) | Quality (GRADE) |
|---|---|---|---|---|---|---|---|---|
| SMD below zero or a RR below 1 means the treatment (condition) was more effective than the comparator (condition) | ||||||||
| 2. Specialized psychotherapy vs community treatment by experts (CTBE) | ||||||||
| Overall BPD severity | MBT | (Jorgensen et al., 2013) | 54 | SMD = –0.12 | [–0.70, 0.47] | N/A | 182 | Very lowa,d |
| 3. Specialized psychotherapy vs protocolized psychological treatment | ||||||||
| Overall BPD severity | DBT vs GPM | (McMain et al., 2009) | 180 | SMD = 0.27 | [–0.02, 0.57] | N/A | 156 | Lowd |
| Self-injury | DBT vs GPM | (McMain et al., 2009) | 177 | RR = 0.81 | [0.50, 1.30] | N/A | 156 | Lowd |
| 7. DBT vs DBT prolonged exposure protocol (DBT-PEP) | ||||||||
| Self-injury | DBT vs DBT-PEP | (Harned et al., 2014) | 18 | SMD = –0.28 | [–1.26, 0.71] | N/A | 65 | Lowd |
| 8. DBT vs DBT-S (skills training plus case management) | ||||||||
| Self-injury | DBT versus DBT-S | (Linehan et al., 2015) | 66 | SMD = –0.09 | [–0.58, 0.39] | N/A | 104 | Lowd |
| Self-injury | DBT versus DBT-S | (Linehan et al., 2015) | 66 | RR = 1.00 | [0.59, 1.70]] | N/A | 104 | Lowd |
| 9. DBT vs DBT-I (individual therapy plus activities group) | ||||||||
| Self-injury | DBT vs DBT-I | (Linehan et al., 2015) | 66 | SMD = –0.34 | [–0.82, 0.15] | N/A | 104 | Lowd |
| Self-injury | DBT vs DBT-I | (Linehan et al., 2015) | 66 | RR = 1.15 | [0.66, 2.03] | N/A | 104 | Lowd |
| 10. DBT-I vs DBT-S | ||||||||
| Self-injury | DBT-I vs DBT-S | (Linehan et al., 2015) | 66 | SMD = 0.24 | [–0.24, 0.72] | N/A | 104 | Lowd |
| Self-injury | DBT-I vs DBT-S | (Linehan et al., 2015) | 66 | RR = 0.87 | [0.49, 1.52] | N/A | 104 | Lowd |
GRADE: Grading of Recommendations Assessment, Development and Evaluation; BPD: borderline personality disorder; MBT: metallization-based therapy; DBT: dialectical behavior therapy; GPM: general psychiatric management according to APA guidelines; N/A: not applicable; SMD: standardized mean difference; RR: risk ratio.
Risk of bias.
Inconsistency.
Indirectness.
Imprecision.
Publication/reporting bias.
Specialized psychotherapies versus TAU
Nine RCTs (n = 524) compared specialized psychotherapies with TAU. Studies investigated DBT (Carter et al., 2010; Feigenbaum et al., 2012; Koons et al., 2001; Linehan et al., 1991, 1994; Priebe et al., 2012; Van Den Bosch et al., 2005), DBT with trauma focused interventions (DBT-PTSD; Bohus et al., 2013; Steil et al., 2011), MBT (Bateman and Fonagy, 1999a) and ST (Farrell et al., 2009).
Low-quality evidence was found for specialized psychotherapies being associated with a medium effect on reducing the overall severity of BPD (k = 4; n = 151; SMD = –0.75 [95% CI: –1.30, –0.19]; for forest plot see Supplementary Material F; Bohus et al., 2013; Farrell et al., 2009; Koons et al., 2001; Priebe et al., 2012; Steil et al., 2011) and a large effect on suicidal behavior (k = 1; n = 38; RR = 0.08 [95% CI: 0.01, 0.58]) at post-treatment (Bateman and Fonagy, 1999a). Seven studies (n = 314) reported moderate quality evidence that specialized psychotherapies were associated with a small effect on a reduction in self-injury at post-treatment (SMD = –0.33 [95% CI −0.57, −0.09]; Feigenbaum et al., 2012; Koons et al., 2001; Linehan et al., 1991, 1994; Priebe et al., 2012; Van Den Bosch et al., 2005). However, for effects on anger (Feigenbaum et al., 2012; Koons et al., 2001; Linehan et al., 1991, 1994) and risk of dropout, the data were inconclusive (Bateman and Fonagy, 1999a; Bohus et al., 2013; Carter et al., 2010; Farrell et al., 2009; Feigenbaum et al., 2012; Koons et al., 2001; Linehan et al., 1991, 1994; Priebe et al., 2012; Steil et al., 2011; Van Den Bosch et al., 2005). For all other outcomes (e.g. dysfunctional interpersonal patterns, dissociations, affective instability and impulsivity), the quality was very low. The undertaken studies did not report follow-up results.
Specialized psychotherapies versus CTBE
Three RCTs (n = 391) compared specialized psychotherapies with CTBE. Studies investigated DBT (Linehan et al., 2006), MBT (Jorgensen et al., 2013) and TFP (Doering et al., 2010).
Two studies (n = 170) reported moderate quality evidence that specialized psychotherapies were associated with a medium effect on reducing the overall severity of BPD at post-treatment (SMD = –0.47 [95% CI: –0.78, –0.16]; for forest plot see Supplementary Material F; Doering et al., 2010; Jorgensen et al., 2013). Also, there was a 38% lower risk of dropout from the specialized psychotherapies group (k = 3; n = 326; Doering et al., 2010; Jorgensen et al., 2013; Linehan et al., 2006). There was low-quality evidence of no difference in effect between specialized psychotherapies and CTBE on suicidal behavior (k = 2; n = 193; SMD = –0.18 [95% CI: –0.52, 0.15]; Doering et al., 2010; Linehan et al., 2006) and self-injury (k = 1; n = 104; RR = 1.09 [95% CI: 0.84, 1.40]), although the CI was compatible with both a reduction and increase in effect (Doering et al., 2010). For the outcome of dysfunctional interpersonal patterns, the quality was very low (Jorgensen et al., 2013). Only the study of MBT (Jorgensen et al., 2013) reported follow-up results on overall BPD severity and dysfunctional interpersonal patterns, but the quality of effect estimates was considered very low.
Specialized psychotherapies versus protocolized psychological treatment
Four RCTs (n = 401) compared specialized psychotherapies with protocolized psychological treatment (Bateman and Fonagy, 2009; Clarkin et al., 2007; McMain et al., 2009; Turner, 2000); one compared MBT with SCM (Bateman and Fonagy, 2009), one compared DBT with CCT (Turner, 2000), one compared DBT with GPM (McMain et al., 2009) and one compared DBT and TFP with supportive psychotherapy (SPT) (Clarkin et al., 2007).
At post-treatment the data were of low quality and inconclusive on the outcomes of overall severity of BPD (for forest plot see Supplementary Material F), suicidal behavior, dissociation, anger, affective instability and dropout. For all other outcomes (e.g. self-injury, dysfunctional interpersonal patterns and impulsivity), the quality was very low.
At follow-up, moderate quality evidence was found for a small effect of protocolized psychological treatment on anger (k = 1; N = 180; SMD = 0.37 [95% CI: 0.07, 0.66]). Low-quality evidence was inconclusive for the following outcomes: overall BPD severity, suicidal behavior, self-injury, dysfunctional interpersonal patterns, affective instability and impulsivity.
Head-to-head comparison of specialized psychotherapies
Two RCTs (n = 178) compared two specialized psychotherapies. TFP was compared with DBT in one study (Clarkin et al., 2007) and with ST in another (Giesen-Bloo et al., 2006).
At post-treatment one study (n = 86) reported low-quality results of a medium effect of ST (compared with TFP) on reducing the overall severity of BPD (SMD = –0.45 [95% CI: –0.87, –0.02]), and there was also 48% less risk of dropout (Giesen-Bloo et al., 2006). In another study (n = 39), there were very low quality and inconclusive effect estimates on suicidal behavior, anger and impulsivity when DBT was compared with TFP. However, participants treated with TFP had a two times lower risk of dropout (Clarkin et al., 2007).
Adjusted specialized psychotherapies versus the original intervention
Three RCTs (n = 187) compared modified versions of a specialized psychotherapy to an original version. The following modified psychotherapies were investigated: DBT with a prolonged exposure protocol (Harned et al., 2014), DBT consisting only of individual therapy plus an activities group (DBT-I; Linehan et al., 2015), DBT consisting only of group skills training and case management (DBT-S; Linehan et al., 2015) and ST with therapist telephone availability (Nadort et al., 2009).
At post-treatment, the effect estimates were of low quality and inconclusive in all comparisons. This was also the case at follow-up, except for the outcome of suicidal behavior where a medium effect was found for DBT compared with DBT-I (k = 1; N = 66; SMD = –0.64 [95% CI: –1.14, –0.14]; Linehan et al., 2015).
Specialized psychotherapies versus TAU and CTBE combined (post hoc analysis)
As CTBE can be seen as a special form of TAU (i.e. psychotherapy-as-usual provided by community experts), and due to the similarities of the two meta-analyses involving TAU and CTBE, we conducted a post hoc analysis on BPD severity (see Figure 3) by combining results of the six studies comparing specialized psychotherapies with TAU or CTBE (N = 321; I² = 39%; Doering et al., 2010; Farrell et al., 2009; Jorgensen et al., 2013; Koons et al., 2001; Priebe et al., 2012; Steil et al., 2011). A medium effect with moderate quality evidence (SMD = –0.59 [95% CI: –0.90, –0.28]) on reducing the severity of BPD was found in favor of specialized psychotherapies.
Figure 3.

Forest plot of post hoc analysis on overall BPD severity at post-treatment.
Discussion
To our knowledge, this is the first comprehensive review (N = 1375) of specialized psychotherapies (DBT, MBT, TFP and ST) for the treatment of BPD in adults since Stoffers et al. (2012) reviewed the literature up to 2010. Although Cristea et al. (2017) updated the evidence until the end of 2015, the review did not focus on the specific effectiveness of specialized psychotherapies and did not investigate the comparative effectiveness of psychotherapies. Moreover, they did not GRADE the outcomes, whereas the certainty of evidence per outcome influences the relevance for clinical practice. Our review included some relevant studies (Bohus et al., 2013; Clarkin et al., 2007; Feigenbaum et al., 2012; Giesen-Bloo et al., 2006; Harned et al., 2014; Linehan et al., 2015; Nadort et al., 2009; Steil et al., 2011) that were missing in the meta-analysis of Cristea et al. (2017) and, by pooling the studies on specialized psychotherapies together and GRADEing the evidence on treatment outcomes, we created a stronger and transparent evidence base for treatment effects. In addition, we investigated the effectiveness of individual specialized psychotherapies by including studies with head-to-head comparisons.
The evidence suggests that these specialized psychotherapies, which have been designed for people with BPD, are more effective than TAU and CTBE. The post hoc analysis in which studies comparing specialized psychotherapies with TAU or CTBE were combined (N = 321; I2 = 39%) confirms this and moderate quality evidence of a medium effect on reducing the severity of BPD was found in favor of specialized psychotherapies. Furthermore, moderate quality effects were found for specialized psychotherapies on reducing self-injury. Another important benefit of specialized psychotherapies is that they are generally well tolerated. Participants had 38% less chance of dropout when compared with CTBE and there was no significant difference in dropout when compared with TAU.
Interestingly, specialized psychotherapies compared to protocolized psychological treatment show no significant differences on almost any outcome, although the quality of the evidence was mostly low to very low due to a significant amount of heterogeneity. Subgroup analysis provided moderate quality positive effects of MBT on suicidal behavior, self-injury and dysfunctional interpersonal patterns in comparison with SCM. In the second subgroup, DBT was superior to CCT on reducing suicidal behavior, self-injury and dissociation/psychoticism, but the quality of the evidence was low. However, DBT was not superior when compared with GPM. Moderate quality evidence also showed that GPM was statistically more effective on anger at follow-up. In another comparison, when specialized therapies were compared with each other (head-to-head), the results were mostly inconclusive. Only one statistically significant difference of low-quality evidence was found: ST was more effective than TFP on overall BPD severity and on treatment dropout.
It is possible to criticize our approach of aggregating specialized psychotherapies because of the differences between these psychotherapies. However, the specialized therapies share commonalities, including a theoretical framework connecting etiological and maintenance factors to therapeutic techniques, a BPD-specific rationale for patients and therapists, advice for therapists (e.g. how to respond to problematic behaviors) and a structured program for patients. By meta-analyzing the results of all specialized psychotherapies, the result could have been inconsistent (statistical heterogeneity), but this was not the case for most outcomes.
In conclusion, specialized therapies are more effective than TAU and CTBE, but it is not clear which one works better for whom and if they are more effective than protocolized psychological treatment. Moreover, it cannot be concluded from this analysis whether there might be a difference in effectiveness or dropout between specialized psychotherapies, let alone whether they are statistically equivalent (for which large Ns are needed).
Implications for practice
The current meta-analysis leads us to recommend the provision of specialized psychotherapies in the treatment of outpatients with BPD to reduce their symptoms. The findings of our review are important because in actual practice most patients are not often treated with prolonged specialized psychotherapies (Hermens et al., 2011). Pharmacological treatment has not been found to be effective in reducing the overall severity of BPD (Lieb et al., 2010).
Although we cannot conclude this directly from the meta-analysis, we hypothesize that protocolized psychological treatment (e.g. GPM) could be more feasible in community health teams for less complex BPD. For more severe patients, specialized psychotherapies are warranted (Barnicot et al., 2012). Service users could be informed about the different specialized psychotherapies that are available at a center to help choose between them. Service user preference should be a priority because, in general, patient-preferred treatment leads to better outcomes and lower dropout (Mergl et al., 2011; Swift et al., 2011). In addition, it could improve the therapeutic alliance, also a contributor to positive treatment outcomes (Barnicot et al., 2012). A decision about which specialized psychotherapy to provide could be made on the basis of costs. In a recent economic evaluation (Brettschneider et al., 2014), it was concluded that most specialized psychotherapies (DBT and ST) were cost saving when compared with TAU, and there were also indications that ST was more cost-saving than TFP.
Directions for future research
First, the evidence base should be strengthened by undertaking more well-powered RCTs into existing treatments (e.g. replication studies) instead of (underpowered) (R)CTs of new treatments. Furthermore, there are indications that the difference in effectiveness between protocolized and specialized psychotherapies is spurious for people with less severe BPD. Thus, future research should focus on testing this issue further, preferably using a large RCT comparing these two types of treatments and deducing the difference in effect on service users with severe or less severe BPD problems, also investigating the relative cost effectiveness. Second, it remains unclear which specialized psychotherapy is more effective and whether there are differences on individual BPD outcomes between the specialized treatments. This should therefore be investigated. Further research should be undertaken to investigate the effects of specialized therapies for inpatients, because providing these interventions in this setting is common in some countries and treating people with BPD in hospital for a long period of time may do more harm than good (Linehan, 1993). Another important point to potentially improve effectiveness and reduce costs is that further research should support the development of tailored specialized therapies for specific BPD profiles. This could be achieved by delineating the effective ingredients from these interventions. Nadort et al. (2009) and Linehan et al. (2015) have investigated effective elements by eliminating certain aspects of specialized therapies and comparing the ‘stripped’ version with the original protocol. No differences in effect were found, although the quality of the evidence was low. Also a recent meta-analysis on the treatment of BPD found that psychological interventions that were offered more than once a week and those that included group sessions had significantly greater improvements in social functioning and reduction in self-injury and depression than those that consisted of one session per week or only individual sessions (Omar et al., 2014).
We have some methodological recommendations that can be made to help build solid, reliable and transparent (meta-analytic) evidence. First, considering that the majority of the RCTs were not registered, the risk of bias in the overall body of evidence could and should be reduced by prospective registration of future studies in established trial registers. Moreover, this advice applies to the whole field of research into non-pharmacological interventions, because unregistered studies are not uncommon (Cybulski et al., 2016). Risk of bias should also be reduced by studies performed by independent investigators; in our review, we noticed that some study authors were founders of the study protocols, which could lead to allegiance bias (Dragioti et al., 2015) and thus to an overestimation of the results. Further steps to prevent bias are mixed model analyses to account for study dropouts, and independent replication studies. Second, with regard to the measured outcomes, we noticed that overall BPD severity and some individual outcomes were not always measured. Therefore, it would be very helpful if future studies incorporated assessments with the Zanarini Rating Scale for BPD (ZAN-BPD), the Borderline Symptom List (BSL), the BPD Severity Index (BPDSI) or the Borderline Evaluation of Severity over Time (BEST) (Zanarini et al., 2010). Also, more attention should be paid to some individual BPD outcomes, for example, results on ‘identity disturbance’ and ‘feelings of emptiness’ outcomes have not been meta-analyzed because they were not reported or were not extractable in the included studies. A third point that could lead to a stronger evidence base is the way results are meta-analyzed. In a post hoc analysis, we showed that the evidence base could be stronger when data are aggregated on the highest possible level, that is, when combined studies compared specialized psychotherapies with TAU and CTBE. Fourth and finally, it might be worthwhile to undertake a network meta-analysis, thereby enlarging the power of the study data and enabling a comparison of interventions that have not yet been compared directly in RCTs.
Supplemental Material
Supplemental material, Supplementary_Material for Specialized psychotherapies for adults with borderline personality disorder: A systematic review and meta-analysis by Matthijs Oud, Arnoud Arntz, Marleen LM Hermens, Rogier Verhoef and Tim Kendall in Australian & New Zealand Journal of Psychiatry
Acknowledgments
The authors thank the Dutch guideline development group for personality disorders and specifically the members of the psychotherapy topic group. They also thank Angita Peterse of Trimbos Institute for design and implementation of the literature searches.
Footnotes
Declaration of Conflicting Interests: A.A. is author on two studies included in this review. All other authors have no competing interests. The views of the authors expressed in this paper do not necessarily reflect the views of NCCMH, Royal College of Psychiatrists, Trimbos Institute or NHS England.
Funding: Funding for this study was provided by a grant from Netwerk Kwaliteitsontwikkeling GGz. Netwerk Kwaliteitsontwikkeling GGz (grant number PV130006) had no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.
Supplementary material: Supplementary material is available at journals.sagepub.com/doi/suppl/10.1177/0004867418791257.
ORCID iD: Matthijs Oud  https://orcid.org/0000-0001-8194-3614
https://orcid.org/0000-0001-8194-3614
References
- Barnicot K, Katsakou C, Bhatti N, et al. (2012) Factors predicting the outcome of psychotherapy for borderline personality disorder: A systematic review. Clinical Psychology Review 32: 400–412. [DOI] [PubMed] [Google Scholar]
- Bateman A, Fonagy P. (1999. a) Effectiveness of partial hospitalization in the treatment of borderline personality disorder: A randomized controlled trial. American Journal of Psychiatry 156: 1563–1569. [DOI] [PubMed] [Google Scholar]
- Bateman A, Fonagy P. (2009) Randomized controlled trial of outpatient mentalization-based treatment versus structured clinical management for borderline personality disorder. American Journal of Psychiatry 166: 1355–1364. [DOI] [PubMed] [Google Scholar]
- Bateman AW, Fonagy P. (1999. b) Psychotherapy for severe personality disorder. Article did not do justice to available research data. BMJ 319: 709–710. [PubMed] [Google Scholar]
- Bloom JM, Woodward EN, Susmaras T, et al. (2012) Use of dialectical behavior therapy in inpatient treatment of borderline personality disorder: A systematic review. Psychiatric Services 63: 881–888. [DOI] [PubMed] [Google Scholar]
- Bohus M, Dyer AS, Priebe K, et al. (2013) Dialectical behaviour therapy for post-traumatic stress disorder after childhood sexual abuse in patients with and without borderline personality disorder: A randomised controlled trial. Psychotherapy and Psychosomatics 82: 221–233. [DOI] [PubMed] [Google Scholar]
- Brettschneider C, Riedel-Heller S, Konig HH. (2014) A systematic review of economic evaluations of treatments for borderline personality disorder. PLoS ONE 9: e107748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carter GL, Willcox CH, Lewin TJ, et al. (2010) Hunter DBT project: Randomized controlled trial of dialectical behaviour therapy in women with borderline personality disorder. Australian and New Zealand Journal of Psychiatry 44: 162–173. [DOI] [PubMed] [Google Scholar]
- Clarkin JF, Levy KN, Lenzenweger MF, et al. (2007) Evaluating three treatments for borderline personality disorder: A multiwave study. American Journal of Psychiatry 164: 922–928. [DOI] [PubMed] [Google Scholar]
- Cohen J. (1988) Statistical Power Analysis for the Behavioral Sciences. Hillsdale, NJ: Lawrence Erlbaum Associates. [Google Scholar]
- Cristea IA, Gentili C, Cotet CD, et al. (2017) Efficacy of psychotherapies for borderline personality disorder: A systematic review and meta-analysis. JAMA Psychiatry 74: 319–328. [DOI] [PubMed] [Google Scholar]
- Cybulski L, Mayo-Wilson E, Grant S. (2016) Improving transparency and reproducibility through registration: The status of intervention trials published in clinical psychology journals. Journal of Consulting and Clinical Psychology 84: 753–767. [DOI] [PubMed] [Google Scholar]
- Doering S, Horz S, Rentrop M, et al. (2010) Transference-focused psychotherapy v. treatment by community psychotherapists for borderline personality disorder: Randomised controlled trial. British Journal of Psychiatry 196: 389–395. [DOI] [PubMed] [Google Scholar]
- Dragioti E, Dimoliatis I, Fountoulakis KN, et al. (2015) A systematic appraisal of allegiance effect in randomized controlled trials of psychotherapy. Ann Gen Psychiatry 14: 25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Farrell JM, Shaw IA, Webber MA. (2009) A schema-focused approach to group psychotherapy for outpatients with borderline personality disorder: A randomized controlled trial. Journal of Behavior Therapy and Experimental Psychiatry 40: 317–328. [DOI] [PubMed] [Google Scholar]
- Feigenbaum J, Fonagy P, Pilling S, et al. (2012) A real-world study of the effectiveness of DBT in the UK National Health Service. Dialectical behavioral therapy. British Journal of Clinical Psychology 51: 121–141. [DOI] [PubMed] [Google Scholar]
- Giesen-Bloo J, van Dyck R, Spinhoven P, et al. (2006) Outpatient psychotherapy for borderline personality disorder: Randomized trial of schema-focused therapy vs transference-focused psychotherapy. Arch Gen Psychiatry 63: 649–658. [DOI] [PubMed] [Google Scholar]
- Guyatt GH, Oxman AD, Schunemann HJ, et al. (2011) GRADE guidelines: A new series of articles in the Journal of Clinical Epidemiology. Journal of Clinical Epidemiology 64: 380–382. [DOI] [PubMed] [Google Scholar]
- Harned MS, Korslund KE, Linehan MM. (2014) A pilot randomized controlled trial of dialectical behavior therapy with and without the dialectical behavior therapy prolonged exposure protocol for suicidal and self-injuring women with borderline personality disorder and PTSD. Behaviour Research and Therapy 55: 7–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hermens ML, van Splunteren PT, van den Bosch A, et al. (2011) Barriers to implementing the clinical guideline on borderline personality disorder in the Netherlands. Psychiatric Services 62: 1381–1383. [DOI] [PubMed] [Google Scholar]
- Higgins JPT, Green S. (2008) Cochrane Handbook for Systematic Reviews of Interventions. Chichester; Hoboken, NJ: Wiley-Blackwell. [Google Scholar]
- Jorgensen CR, Freund C, Boye R, et al. (2013) Outcome of mentalization-based and supportive psychotherapy in patients with borderline personality disorder: A randomized trial. Acta Psychiatrica Scandinavica 127: 305–317. [DOI] [PubMed] [Google Scholar]
- Kliem S, Kroger C, Kosfelder J. (2010) Dialectical behavior therapy for borderline personality disorder: A meta-analysis using mixed-effects modeling. Journal of Consulting and Clinical Psychology 78: 936–951. [DOI] [PubMed] [Google Scholar]
- Koons CR, Robins CJ, Tweed JL, et al. (2001) Efficacy of dialectical behavior therapy in women veterans with borderline personality disorder. Behavior Therapy 32: 371–390. [Google Scholar]
- Lieb K, Völlm B, Rücker G, et al. (2010) Pharmacotherapy for borderline personality disorder: Cochrane systematic review of randomised trials. British Journal of Psychiatry 196: 4–12. [DOI] [PubMed] [Google Scholar]
- Lieb K, Zanarini MC, Schmahl C, et al. (2004) Borderline personality disorder. Lancet 364: 453–461. [DOI] [PubMed] [Google Scholar]
- Linehan MM. (1993) Cognitive-Behavioral Treatment of Borderline Personality Disorder. New York: Guilford Press. [Google Scholar]
- Linehan MM, Armstrong HE, Suarez A, et al. (1991) Cognitive-behavioral treatment of chronically parasuicidal borderline patients. Archives of General Psychiatry 48: 1060–1064. [DOI] [PubMed] [Google Scholar]
- Linehan MM, Comtois KA, Murray AM, et al. (2006) Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviors and borderline personality disorder. Archives of General Psychiatry 63: 757–766. [DOI] [PubMed] [Google Scholar]
- Linehan MM, Korslund KE, Harned MS, et al. (2015) Dialectical behavior therapy for high suicide risk in individuals with borderline personality disorder: A randomized clinical trial and component analysis. JAMA Psychiatry 72: 475–482. [DOI] [PubMed] [Google Scholar]
- Linehan MM, Tutek DA, Heard HL, et al. (1994) Interpersonal outcome of cognitive behavioral treatment for chronically suicidal borderline patients. American Journal of Psychiatry 151: 1771–1776. [DOI] [PubMed] [Google Scholar]
- McMain SF, Links PS, Gnam WH, et al. (2009) A randomized trial of dialectical behavior therapy versus general psychiatric management for borderline personality disorder. American Journal of Psychiatry 166: 1365–1374. [DOI] [PubMed] [Google Scholar]
- Mergl R, Henkel V, Allgaier AK, et al. (2011) Are treatment preferences relevant in response to serotonergic antidepressants and cognitive-behavioral therapy in depressed primary care patients? Results from a randomized controlled trial including a patients’ choice arm. Psychotherapy and Psychosomatics 80: 39–47. [DOI] [PubMed] [Google Scholar]
- Moher D, Liberati A, Tetzlaff J, et al. (2009) Reprint–preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Physical Therapy 89: 873–880. [PubMed] [Google Scholar]
- Nadort M, Arntz A, Smit JH, et al. (2009) Implementation of outpatient schema therapy for borderline personality disorder with versus without crisis support by the therapist outside office hours: A randomized trial. Behaviour Research and Therapy 47: 961–973. [DOI] [PubMed] [Google Scholar]
- NICE (2009) Borderline Personality Disorder: Recognition and Management (Clinical Guideline [CG78]). London: NICE. [PubMed] [Google Scholar]
- Nordic Cochrane Centre (2014) Review Manager (Revman) Version 5.3. Copenhagen: The Cochrane Collaboration. [Google Scholar]
- Omar H, Tejerina-Arreal M, Crawford MJ. (2014) Are recommendations for psychological treatment of borderline personality disorder in current U.K. guidelines justified? Systematic review and subgroup analysis. Personality and Mental Health 8: 228–237. [DOI] [PubMed] [Google Scholar]
- Priebe S, Bhatti N, Barnicot K, et al. (2012) Effectiveness and cost-effectiveness of dialectical behaviour therapy for self-harming patients with personality disorder: A pragmatic randomised controlled trial. Psychotherapy and Psychosomatics 81: 356–365. [DOI] [PubMed] [Google Scholar]
- Samuels J. (2011) Personality disorders: Epidemiology and public health issues. International Review of Psychiatry 23: 223–233. [DOI] [PubMed] [Google Scholar]
- Steil R, Dyer A, Priebe K, et al. (2011) Dialectical behavior therapy for posttraumatic stress disorder related to childhood sexual abuse: A pilot study of an intensive residential treatment program. Journal of Traumatic Stress 24: 102–106. [DOI] [PubMed] [Google Scholar]
- Stoffers JM, Vollm BA, Rucker G, et al. (2012) Psychological therapies for people with borderline personality disorder. Cochrane Database of Systematic Reviews 8: CD005652. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Swift JK, Callahan JL, Vollmer BM. (2011) Preferences. Journal of Clinical Psychology 67: 155–165. [DOI] [PubMed] [Google Scholar]
- Tomko RL, Trull TJ, Wood PK, et al. (2014) Characteristics of borderline personality disorder in a community sample: Comorbidity, treatment utilization, and general functioning. Journal of Personality Disorders 28: 734–750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Torgersen S. (2012) Epidemiology. In: Widiger TA. (ed.) The Oxford Handbook of Personality Disorders. Oxford: Oxford University Press, pp. 186–205. [Google Scholar]
- Turner RM. (2000) Naturalistic evaluation of dialectical behavior therapy-oriented treatment for borderline personality disorder. Cognitive and Behavioral Practice 7: 413–419. [Google Scholar]
- Van Den Bosch LMC, Koeter MWJ, Stijnen T, et al. (2005) Sustained efficacy of dialectical behaviour therapy for borderline personality disorder. Behaviour Research and Therapy 43: 1231–1241. [DOI] [PubMed] [Google Scholar]
- Zanarini MC, Gunderson JG, Frankenburg FR, et al. (1990) Discriminating borderline personality disorder from other axis II disorders. American Journal of Psychiatry 147: 161–167. [DOI] [PubMed] [Google Scholar]
- Zanarini MC, Stanley B, Black DW, et al. (2010) Methodological considerations treatment trials for persons personality disorder. Annals of Clinical Psychiatry 22: 75–83. [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental material, Supplementary_Material for Specialized psychotherapies for adults with borderline personality disorder: A systematic review and meta-analysis by Matthijs Oud, Arnoud Arntz, Marleen LM Hermens, Rogier Verhoef and Tim Kendall in Australian & New Zealand Journal of Psychiatry