

Abstract
AIM
To investigate the acute effects of sinusoidal and stochastic resonance partial-body vibration in sitting position, including muscle activity, heart rate variability, balance and flexibility.
METHODS
Fifty healthy participants were assigned randomly to two training conditions: A sinusoidal partial-body vibration (SIN, 8 Hz) or a stochastic resonance partial-body vibration (STOCH, 8 ± 2 Hz). For baseline assessment participants sat on the vibration platform without vibration. Both training conditions consisted of five series of a one-minute vibration training and a one-minute break between them. In this experimental study surface electromyography (EMG) of the erector spinae (ES), one of the back muscles, and heart rate variability (HRV) was measured at baseline and during training. Balance and flexibility were assessed at baseline and immediately after training. Balance was measured with the modified star excursion balance test (mSEBT) and flexibility was assessed through the modified fingertip-to-floor method (mFTF).
RESULTS
Paired sample t-test showed a significant increase in balance that was restricted to STOCH (t = -2.22, P = 0.018; SIN: t = -0.09, P = 0.466). An increase in flexibility was also restricted to STOCH (t = 2.65, P = 0.007; SIN: t = 1.41, P = 0.086). There was no significant change of muscle activity in the ES-EMG in STOCH or SIN conditions. In both training conditions, HRV decreased significantly, but remained in a low-load range (STOCH: t = 2.89, P = 0.004; SIN: t = 2.55, P = 0.009).
CONCLUSION
In sitting position, stochastic resonance partial-body vibration can improve balance and flexibility while cardiovascular load is low. STOCH can be a valuable training option to people who are unable to stand (e.g., people, who are temporarily wheelchair-bound).
Keywords: Partial-body vibration, Balance, Flexibility, Sinusoidal, Stochastic resonance
Core tip: This experimental study shows an immediate improvement of balance and flexibility after one training session of stochastic resonance partial-body vibration (STOCH) in sitting position. STOCH in sitting position is a promising complement to stochastic resonance whole-body vibration (SR-WBV) in standing position, especially for individuals who are unable to do SR-WBV (e.g., people who are temporarily wheelchair-bound).
INTRODUCTION
Musculoskeletal diseases (MSD) are among the most common global health problems[1]. Wieser, Tomonaga[2] calculated the direct costs of MSD for the Swiss health system to be between CHF 8.7 and 11.4 billion per year. Together with cardiovascular diseases (10.3 billion), these are the highest costs for non-communicable diseases. Long-lasting vibration exposure at work has shown to be a risk factor for musculoskeletal diseases (MSD)[3], whereas a brief vibration experience may lead to beneficial training effects[4].
Thereby, stochastic resonance whole-body vibration (SR-WBV) is especially promising[5,6]. Compared to sinusoidal vibration which common vibration platforms are working with, stochastic vibration is random and uses lower frequency vibration exposure up to 12 Hz[7,8].
Effects of SR-WBV at the worksite are auspicious, especially in those with chronic MSD[9]. As cardiovascular load during SR-WBV is low[10], no sweating occurs during the training, making it especially promising for workplace interventions. Musculoskeletal well-being increased after a 4-wk SR-WBV training in workers of a steel manufacturing company[11]. The same was reported for employees that engaged in sedentary work. With those who suffered from back pain prior to SR-WBV profiting the most[12]. These positive effects of SR-WBV also appeared in employees of a university hospital after a 8-wk randomized controlled trial, having the highest impact on those with baseline health restraints[13]. SR-WBV is practiced in standing position. However, some older individuals and individuals in a wheel-chair may not be able to stand. As suggested by Eichelberger[14] in a single-case study vibration training in sitting position might be “advantageous in deconditioned persons, who suffer from frailty, musculoskeletal complaints, Parkinson’s disease, multiple sclerosis or after a stroke”. Therefore, this experimental study investigates partial-body vibration in sitting position and its related acute effects.
Partial-body vibration in sitting position
Thereby, this study tests both, sinusoidal partial-body vibration (SIN) and stochastic resonance partial-body vibration (STOCH). We use the same vibration device as Eichelberger[14]. In standing, as well as in sitting position, especially stochastic vibration provoked muscle activity[14,15] while cardiovascular activation was low[10,16]. Low cardiovascular activation makes stochastic vibration an appropriate training tool for older individuals and people with health problems[5].
According to previous research with whole-body vibration in standing position, we expect an increased muscle activity of the erector spinae (ES), one of the back muscles, during partial-body vibration in sitting position (H1). In addition, we expect low or absent cardiovascular activation during partial-body vibration in sitting position. Hence, heart rate variability (HRV) during training is expected to be unchanged or only slightly lower than during baseline measurement (H2).
Better balance, better flexibility
In Switzerland, every fourth accident is due to a slip, trip and fall incident[17]. They are also the most frequent accidents among office workers[18]. Better balance prevents slip, trip and fall incidents[19]. Aside from promising effects on musculoskeletal wellbeing, positive effects of SR-WBV were also found on surefootedness and balance in white-collar employees[12] and in health-care professionals[13]. Hence, we expect balance to be better after partial-body vibration training compared to baseline (H3).
Previous studies showed an increase of flexibility due to whole-body vibration training in the elderly[20], in healthy, young adults[21] as well as in young gymnasts[21]. In consequence, we expect flexibility after partial-body vibration training to be better than at baseline (H4).
How stochastic vibration works
While vibration frequency at sinusoidal vibration is constant, stochastic vibration changes randomly within a frequency range. Ward and colleagues defined stochastic resonance as “a nonlinear cooperative effect wherein the addition of a random process, or “noise” to a weak signal, or stimulus results in improved detectability or enhanced information content in some response”[22]. During stochastic vibration, upcoming vibration movements can not be anticipated by the human body, so it is constantly challenged to adapt its neural and muscular reactions. Moreover, the human body shows no muscular fatigue during the application[8,23-25]. It seems that an interaction of different types of neurophysiologic sensors is provoked by stochastic vibration while afferent and efferent signals are adjusted. This probably acts as exercise for the sensorimotor system[8].
In the current experimental study, we randomly assigned participants to SIN and STOCH. We expect both, SIN and STOCH to have acute effects on activity of surface electromyography (EMG), HRV, balance, and flexibility. Differences in training effectiveness between SIN and STOCH are likely to emerge only after longer training periods. However, based on previous findings on sinusoidal versus stochastic vibration in whole-body vibration training, we expect changes in muscle activity, HRV, balance, and flexibility to be more distinct in stochastic training condition than in sinusoidal training condition.
MATERIALS AND METHODS
Ethics
The study was performed in consensus with all requirements defined by the Swiss Society of Psychology and was conducted with the understanding and the consent of the human subject. The Ethical Committee of the responsible University faculty (University of Bern) has approved the study (No. 2016-5-000004).
Participants
Expecting a moderate effect size (d = 0.5) for the t-test analysis between two dependent means and a requirement of 80% power to detect an existing difference, the required sample size was 26 participants for each training condition SIN and STOCH. The inclusion criterion for the participants was to be in good health. The exclusion criteria were being pregnant, having osteosynthesis material (such as implants, screws, etc.) in the body, musculoskeletal disorders, joint problems (especially regarding the knee, hip and back), herniated discs, rheumatism (such as spondylitis, gout, osteoporosis, osteoarthritis), cardiovascular complaints and disorders related to the sense of balance (such as a hearing loss). Twenty-six participants took part in each training condition, so overall 52 participants participated in the study. Due to a broken cable, EMG measurements of two participants were not recorded. Therefore, these data sets were removed for data analysis. Participants who were students at the associated university were rewarded with two of 15 mandatory hours as a participant in studies.
Vibration platform
The vibration platform used in this study is a functional prototype consisting of a plate with a hydraulic vibration, constructed specifically for vibration training in sitting position. The device provides a range of motion of ± 13° around each of the three rotation axes and frequencies up to 15 Hz. Stochastic vibration can be introduced through random variation of frequency, amplitude or rotation axis. The chosen amplitude and frequency of the vibration was recommended by one of the co-authors (PE[14]). During SIN, an amplitude of 0.5° was applied in medial-lateral direction during a vibration frequency of 8 Hz. During STOCH, amplitude as well as frequency varied over a spectrum of 25%.
Muscle activity
Measurements of the muscle activity of the ES during MVC, baseline and training session were recorded for each participant. Therefore, surface electrodes were used (Ambu® BlueSensor N, Synmedic AG, Zürich) and “placed at 2 finger width lateral from the proc. spin. of L1” according to the SENIAM recommendation (Surface Electromyography for the Non-Invasive Assessment of Muscles)[26]. EMG signals were forwarded from a transmitter (TeleMyoTM 2400T G2, Noraxon Inc. United States, Velamed GmbH, Medizintechnik und Biomechanische Konzepte, Köln, Germany) to a receiver (TeleMyoTM 2400R Receiver, Noraxon Inc. United States, Velamed GmbH, Medizintechnik und Biomechanische Konzepte, Köln, Germany), which transformed these digital signals into analogue outputs. For recording and processing the data, the software ADS (analog and digital signal processing©, uk-labs, Kempen, Germany) was used.
Heart rate variability
The measurement of the R-R intervals (the interval from the onset of one R wave to the onset of the next one[27]) was taken while the participant was sitting on the vibration platform during baseline and training session. HRV was measured with Polar V800 and heart rate sensor Polar H7 (©Polar Electro 2016). Giles, Draper[28] showed that R-R intervals and HRV do not differ between recordings from Polar V800 and electrocardiography (ECG).
Balance
Balance was measured using the modified star excursion balance test (mSEBT) from Hertel, Braham[29] once after baseline condition and once after training session. The mSEBT measures dynamic balance into the three directions anterior, posteromedial and posterolateral. According to Gribble, Kelly[30] and Hertel, Miller[31] intra-test reliability (r = 0.84 to 0.93) and test-retest reliability (r = 0.89 to 0.93) are high. To exclude effects related to gender, it was important to normalize excursion distances to individual leg length of each participant[32].
Flexibility
The modified fingertip-to-floor method (mFTF) was used to assess flexibility. It was measured once after baseline condition and once after training session. Compared to the fingertip-to-floor method (FTF), the mFTF has the advantage that the participant stands on a box, so that measurements can be taken of participants who are able to touch the floor or reach beyond the level of the floor[33]. Therefore, negative values indicate a better flexibility than positive values. This test measures unspecific flexibility because spine, pelvis, hip joint and arms are involved[34]. Gauvin, Riddle[33] report high test-retest reliability (r = 0.98), as well as high inter-tester reliability (r = 0.95) of the mFTF. Stiffness is reported to be higher in the morning and a maximum of flexibility occurs between midday and midnight[35]. In order to partly control for stiffness and provide similar test conditions, every participant was tested in the afternoon or early evening.
Procedure
The study was conducted at the movement laboratory of Bern University of Applied Sciences, Applied Research and Development Physiotherapy. To make sure the procedure was standardized, a case report form (CRF) was prepared. The measurements for one participant lasted approximately 90 min. During this time two of three examiners (YF, NB, NB) needed to be present. The first examiner took the lead with the measurements, while the second examiner acted as his assistant. To prevent error due to monotony and routine, the role of the first and second examiner was changed regularly between the three examiners. After reading the study-information, participants signed a consent form. While a surface EMG electrode was placed on the ES (Figure 1), participants answered a demographical and behavioral questionnaire using Qualtrics (©2016 Qualtrics LLC), installed on an iPad Air2 (©2015 Apple Inc.). With an impedance meter (Digitimer model D175, Digitimer Ltd. Welwyn Garden City, United Kingdom) the skin resistance was tested and rated as sufficient being equal or lower as 5 kΩ. Afterwards, a measurement of a maximum voluntary contraction (MVC) of the ES was made in order to be used as reference value for the EMG measurements, rated as 100%[36]. While lying prone on a bench, participants were asked to extend their back against one examiner’s resistance. With this standardized test[36], MVC values of the ES were captured. For the MVC measurements, the participants were asked to hold the MVC 3 times for 5 s.
Figure 1.
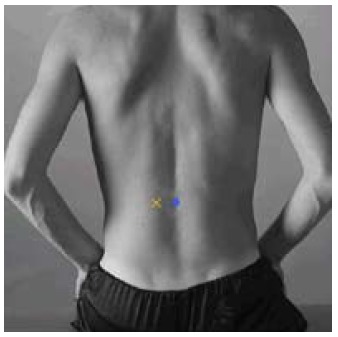
Placement of the electrodes according to SENIAM[27].
For the following baseline measurements, the participants had to sit on the vibration platform in an upright position (Figure 2). They were asked to keep calm and to focus on a black point on the wall at a distance of 2.5 m while no vibration occurred for one minute. During this time muscle activity and HRV were recorded. Then, participants were asked to complete the modified star excursion balance test (mSEBT) of Hertel, Braham[29] to assess balance. They were instructed to start with arms akimbo, then stand on one leg and stretch out the other leg as far as possible to touch the floor with the tip of their toes. The maximum distance reached without losing balance or lifting the supporting leg was measured and noted. The same procedure was repeated five times in three directions (anterior, posteromedial and posterolateral) with both legs.
Figure 2.
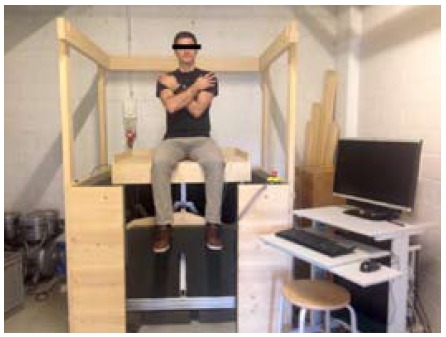
Sitting position on the vibration platform. HRV: Heart rate variability; EMG: Electromyography.
As reported by Blasimann[37], flexibility was assessed through the modified fingertip-to-floor method (mFTF). For this test participants stood on a box with both ankles touching each other. They were then instructed to keep their legs and arms straight and bend over as far as possible to push down a control bar in front of them. After one trial run, the same procedure was performed three times. While the first examiner gave verbal instructions, the second examiner wrote down the finger-floor distance in mm and put the control bar back to the starting position. After these tests, the baseline measurement was over and the training session began.
Participants were randomly assigned to SIN (8 Hz) or STOCH (8 ± 2 Hz). As the sequence of the two training conditions was alternated across trials in the movement laboratory, randomization was achieved through time of participation, which means that the first participant attended in SIN, the second in STOCH and so forth. Participants were blinded with respect to their training condition. However, a blinding of the examiners was not feasible.
The session consisted of five series, which lasted one minute each, with a one-minute break in between. This training regime with five series of a one-minute vibration training was based more on empirical experience from other studies about stochastic vibration training[11,12] than on scientific evidence, because the training parameters of stochastic vibration training show a wide range of applications that are not as well known as they are for strength or endurance training[38]. A vibration frequency of 8 ± 2 Hz was recommended for the STOCH condition, so acceleration exposure on the body was low[14]. For a better comparison, 8 Hz were selected for the SIN condition, too. During the training session, the participant was again sitting in an upright position on the vibration platform focusing on a point on the wall at a distance of 2.5 m while muscle activity and HRV were recorded. After the training session, the same measurements of balance and flexibility as described above were repeated. The whole procedure is shown in Figure 3.
Figure 3.
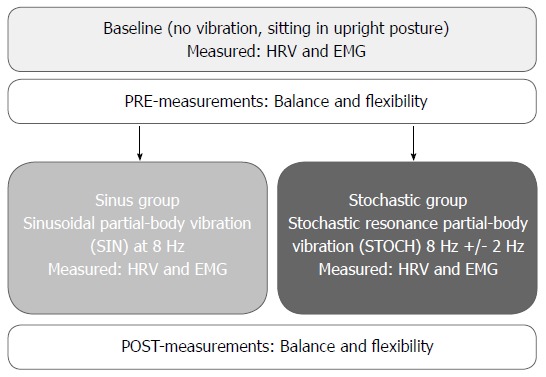
Flowchart of the procedure. EMG: Electromyography, muscular activation of the lower back muscle erector spinae (ES); HRV: Heart rate variability was measured with Polar V800. Balance was measured using the modified star excursion balance test (mSEBT) and expressed in centimeter; Flexibility was assessed with the fingertip-to-floor method (mFTF) and measured in centimeter.
Statistical analysis
Muscle activity, HRV as well as balance and flexibility were analyzed in a dependent sample t-test to examine differences between baseline and training conditions. Since all the hypotheses were directed, P-values were one-tailed with an α-level set at 5%. HRV, balance and flexibility were approximately normally distributed (P > 0.05), whereas EMG was not approximately normally distributed as assessed by the Kolmogorov-Smirnov-Test, P < 0.05. However, according to Field[39] the analyses of the hypotheses can be considered robust against violations of the normal distribution due to the same group size. Pearson’s descriptive statistics for the collected variables are shown in Table 1.
Table 1.
Descriptive and inferential statistics
| STOCH (n = 25) | SIN (n = 25) | |||||
| Variable | M | SD | M | SD | t | P |
| Sex (m, f) | 7m, 18f | 10m, 15f | -0.89 | 0.381 | ||
| Age (yr) | 25.12 | 2.89 | 25.40 | 4.38 | 0.27 | 0.791 |
| BMI (kg/m²) | 22.81 | 3.81 | 23.54 | 3.50 | 0.70 | 0.487 |
| Sport (1 “rarely” - 6 “prof.”) | 2.25 | 1.11 | 2.36 | 1.08 | 0.35 | 0.727 |
| Smoking (s, ns) | 7s, 18ns | 8s, 17ns | 0.30 | 0.763 | ||
| Last time nicotine (h) | 25.86 | 21.71 | 7.75 | 16.35 | -1.84 | 0.089 |
| Last time caffeine (h) | 7.65 | 8.25 | 9.40 | 9.08 | 0.64 | 0.527 |
| EMG ES (%MVC) | 29.67 | 22.43 | 25.17 | 18.50 | -0.77 | 0.443 |
| HRV (RMSSD, ms) | 35.21 | 16.77 | 35.69 | 19.52 | 0.09 | 0.926 |
| Balance-test (cm) | 73.34 | 8.23 | 77.77 | 6.75 | 2.08 | 0.043 |
| Flexibility-test (cm) | -2.02 | 9.2 | -2.01 | 9.54 | 0.001 | 0.999 |
EMG: Electromyography, muscular activation expressed as percentage of peak activation measured at maximal voluntary contraction (%MVC) of the lower back muscle erector spinae (ES); HRV: Heart rate variability was measured with the square root of the mean of the sum of the squares of the differences (RMSSD). Balance was measured using the modified star excursion balance test (mSEBT) and expressed in centimeter; Flexibility was assessed with the fingertip-to-floor method (mFTF) and expressed in centimeter.
RESULTS
Participant characteristics
Data of 50 healthy participants (33 females and 17 males, mean age = 25.3 years, SD = 3.7 years; BMI = 23.17 ± 3.64), assigned evenly to STOCH, SIN respectively, were analyzed in this study. Datas of twenty-five participants for each group STOCH and SIN were analyzed. The two groups showed no significant differences in any demographic characteristics or in baseline muscle activity, HRV or flexibility. However, balance in the SIN group was significantly better (longer distance reached) at baseline than in the STOCH group. T-test results and descriptive statistics for both training conditions are shown in Table 2.
Table 2.
Results of t-tests for each training condition
| STOCH (n = 25) | SIN (n = 25) | |||||||
| BL | T | BL | T | |||||
| mean ± SD | mean ± SD | t | P | mean ± SD | mean ± SD | t | P | |
| EMG ES (%MVC) | 29.67 ± 22.43 | 32.32 ± 24.03 | -0.96 | 0.174 | 25.17 ± 18.50 | 26.07 ± 14.73 | -0.51 | 0.307 |
| HRV (RMSSD, msec) | 35.21 ± 16.77 | 29.10 ± 12.64 | 2.89 | 0.004 | 35.69 ± 19.52 | 29.60 ± 12.90 | 2.55 | 0.009 |
| Balance-test (cm) | 73.34 ± 8.23 | 75.28 ± 9.35 | -2.22 | 0.018 | 77.77 ± 6.75 | 77.82 ± 6.12 | -0.09 | 0.466 |
| Flexibility-test (cm) | -2.02 ± 9.20 | -2.53 ± 9.08 | 2.65 | 0.007 | -2.01 ± 9.54 | -2.55 ± 9.75 | 1.41 | 0.086 |
Left: Stochastic resonance partial-body vibration (STOCH) at Baseline (BL) and Training condition (T); Right: Sinusoidal partial-body vibration (SIN) at BL and T; EMG: Electromyography, activation expressed as percentage of activation measured at maximal voluntary contraction (%MVC) of the lower back muscle erector spinae (ES); HRV: Heart rate variability was measured with the square root of the mean of the sum of the squares of the differences (RMSSD); Balance was measured using the modified star excursion balance test (mSEBT) and flexibility with fingertip-to-floor method (MFTF).
Higher muscle activity of the ES during STOCH and SIN (H1)
Overall, vibration training had no significant effect on muscle activity of the ES (t = -1.09, P = 0.140, n = 50). Although not significantly, muscle activity of the ES tended to be slightly higher during vibration training (29.20 ± 19.98 %MVC) than during baseline measurement (27.42 ± 20.47 %MVC).
Focusing on both training conditions, there was also no significant effect of STOCH (t = -0.96, P = 0.174, n = 25) and SIN (t = -0.51, P = 0.307, n = 25) on muscle activity of the ES found. Although not significantly, muscle activity of the ES tended to be slightly higher during STOCH (32.32 ± 24.03 %MVC) than during baseline measurement (29.67 ± 22.43 %MVC) and also higher during SIN (26.07 ± 14.73 %MVC) than during baseline measurement (25.17 ± 18.50 %MVC). According to Cohen[40], effect sizes are described as small (d = 0.2), medium (d = 0.5), and large (d ≥ 0.8). Effect sizes using Cohen’s d[40] for muscle activity of the ES for overall vibration was d = -0.087, for the STOCH group d = -1.136 and for the SIN group d = -0.490.
Lower HRV during STOCH and SIN (H2)
A significant effect on HRV was found during overall vibration training (t = 3.86, P = 0.0003, n = 50) compared to baseline measurement. HRV was significantly lower during vibration training (29.34 ± 12.65 ms) than during baseline measurement (35.45 ± 18.01 ms).
Focusing on both training conditions, STOCH (t = 2.89, P = 0.004, n = 25) and SIN (t = 2.55, P = 0.009, n = 25) have a significant effect on HRV. HRV during STOCH (29.10 ± 12.64 ms) as well as during SIN (29.60 ± 12.90 ms) were both significantly lower compared to baseline measurements (35.21 ± 16.77 ms) and (35.69 ± 19.52 ms) accordingly. Effect sizes using Cohen’s d[40] on HRV for overall vibration was d = 0.355, for STOCH d = 0.342 and d = 0.320 for SIN, respectively.
Increase in balance after STOCH and SIN (H3)
A significant effect on balance was found after overall vibration training (t = -1.83, P = 0.037, n = 50). Compared to baseline measurement (75.55 ± 7.77 cm), overall values for balance were significantly higher after vibration training (76.55 ± 7.92 cm).
Specifically, a significant effect was found after STOCH (t = -2.22, P = 0.018, n = 25) but not after SIN (t = -0.09, P = 0.466, n = 25). Balance was significantly increased after STOCH (75.28 ± 9.35 cm) compared to baseline measurement (73.34 ± 8.23), but not after SIN (77.82 ± 6.12 cm) compared to baseline measurement (77.77 ± 6.75 cm). Effect size using Cohen’s d[40] on balance for overall vibration was d = -0.127, for STOCH d = -0.216 and for SIN d = -0.008.
Increase in flexibility after STOCH (H4)
Overall, vibration training had a significant effect on flexibility (t = 2.49, P = 0.008, n = 25). Flexibility was significantly increased after overall vibration training (-2.54 ± 9.33 cm) compared to baseline measurement (-2.02 ± 9.27 cm). Specifically, a significant effect on flexibility could only be found after STOCH (t = 2.65, P = 0.007, n = 25), but not after SIN (t = 1.41, P = 0.086, n = 25). Flexibility was significantly increased after STOCH (-2.53 ± 9.08 cm) compared to baseline measurement (-2.02 ± 9.20 cm), but not after SIN (-2.55 ± 9.75 cm) compared to baseline measurement (-2.01 ± 9.54 cm). Effect size using Cohen’s d[40] on flexibility for overall vibration was d = 0.057, for STOCH d = 0.058 and d = 0.055 for SIN, respectively.
DISCUSSION
In the current experimental study, we expected both, SIN and STOCH to have acute effects on muscle activity, HRV, balance, and flexibility. Although differences in training effectiveness between the two groups are only likely to emerge after longer training periods, we expected changes in measured variables to be more distinct in stochastic training condition than in sinusoidal training condition.
Activity of the ES muscle did not increase with vibration training (H1). This finding goes against our expectation. A possible explanation could be, that the ES was already active during sitting position with upright posture at baseline measurement, so there was no significant increase of muscle activity during vibration training. Further studies on vibration training in the sitting position should focus on that. Our second hypothesis was confirmed, as there was a significant, but low cardiovascular activation in HRV, that was lower during training than at baseline (H2). Although HRV significantly decreased, it maintained in a low-load range[41]. In line with findings from SR-WBV[10,16], cardiovascular activation was low. The method seems suitable for older individuals and patients with mild cardiovascular problems. As expected, balance (H3) and flexibility (H4) significantly increased.
Looking at separate analyses for training effectiveness in sinusoidal and stochastic vibration conditions, the stochastic vibration condition seemed to contribute more to overall changes than the sinusoidal vibration condition. Balance and flexibility increased significantly after one training session of STOCH, but not after SIN. This indicates that positive effects from previous studies about stochastic vibration in standing position would also appear in sitting position[12,15,42]. Group differences can not be explained by differences in muscular activity of the ES.
To assess cardiac activity, we measured HRV during SIN and STOCH. HRV is also known as a stress index[43,44]. As this study was conducted on a prototype of a vibration platform, participants would possibly be somewhat anxious about the experiment. As expected, HRV was significantly lower during STOCH than SIN but the RMSSD-value was within the range of 27 ± 12 at all time as is recommended by Task Force of the European Society of Cardiology[41]. This implies that cardiac activation and/or stress level during SIN and STOCH was still low.
SR-WBV training seems to be a safe training intervention. Very few side effects of whole-body vibration were reported in a review of 112 studies. 104 studies that used sinusoidal whole-body vibration, reported 0.00120% side effects, whereas eight studies used SR-WBV and reported 0.00069% side effects. Additionally, side effects from sinusoidal whole-body vibration were more serious compared to those from SR-WBV[45]. As mentioned by Eichelberger, Fankhauser[14] STOCH might be advantageous in deconditioned persons, who suffer from frailty, musculoskeletal complaints, Parkinson’s disease, multiple sclerosis or after a stroke. Because the training was on a prototype of a vibration platform, which effects were only tested in a single case study before[14], it was important that our participants were healthy.
In longitudinal studies SR-WBV showed promising results to increase musculoskeletal well-being[11-13]. As SR-WBV is practiced in standing position, these results are limited to the standing position. Therefore, further longitudinal studies should focus on SIN and STOCH in sitting position to make these benefits available to people who are unable to do SR-WBV (e.g., people who are temporarily wheelchair-bound).
With this study we were able to make the first step in this direction. We found an immediate improvement of balance and flexibility after one training session of STOCH while cardiac-activation was low, but could not find a higher muscle activity of the ES in the lower back during the training session. This study had an experimental design, and many potential confounders were controlled by randomization. The participants were blinded with respect to their training condition. However, a blinding of the primary investigator was not feasible. As only one superficial back muscle was measured, there might have been an increase of muscle activity in other back muscles which were not measured.
ARTICLE HIGHLIGHTS
Research background
Stochastic resonance whole-body vibration (SR-WBV) is a promising health-intervention at the worksite. In previous works including 4 or even 8 weeks of training, SR-WBV was found to improve musculoskeletal pain and balance, measured as self-report and as recorded body sway on a balance platform. Improved balance is connected to a lower risk of slips and falls. Short trials of SR-WBV that amount to less than 10 min can be done at a worksite without a change of clothes or shoes. Cardiovascular demand with 5 Hz SR-WBV is low and permits SR-WBV in the untrained or elderly workforce.
Research motivation
SR-WBV is practiced in standing position. However, some older individuals and individuals in a wheel-chair may not be able to stand. Therefore, this experimental study investigates partial-body vibration in sitting position and its related acute effects.
Research objectives
The objective of this study was to investigate and quantify the acute effects of partial-body vibration in sitting position on muscle activity, heart-rate variability, balance and flexibility.
Research methods
The vibration platform used in this study is a functional prototype, constructed specifically for vibration training in sitting position. Every participant attended a baseline and a training condition. For baseline assessment participants sat on the vibration platform without vibration. The training condition was either a sinusoidal partial-body vibration (SIN, 8 Hz) or a stochastic resonance partial-body vibration (STOCH, 8 ± 2 Hz). Surface electromyography (EMG) of the erector spinae (ES), one of the back muscles, and heart rate variability (HRV) were measured at baseline and during training. Balance and flexibility were assessed at baseline and immediately after training. Balance was measured with the modified star excursion balance test (mSEBT) and flexibility was assessed through the modified fingertip-to-floor method (mFTF).
Research results
Paired sample t-test showed a significant increase in balance (STOCH: t = -2.22, P = 0.018; SIN: t = -0.09, P = 0.466) as well as in flexibility (STOCH: t = 2.65, P = 0.007; SIN: t = 1.41, P = 0.086) only after stochastic vibration in sitting position. There was no significant change of muscle activity in the ES-EMG in both training conditions. Also, HRV decreased significantly in both training conditions, but remained in a low-load range (STOCH: t = 2.89, P = 0.004; SIN: t = 2.55, P = 0.009).
Research conclusions
This experimental study showed benefits in balance and flexibility only for stochastic but not for sinusoidal vibration. Stochastic vibration in sitting position could be a promising complement to stochastic resonance whole-body vibration in standing position, especially for individuals who are unable for the standing position (e.g., people who are temporarily wheelchair-bound).
Research perspectives
As immediate effects of stochastic vibration in sitting position have not been tested before, especially on this prototype device, we needed to make sure that stochastic vibration in sitting position did have the expected effect and that no negative side-effects emerge from one single vibration training in this study. If side-effects would have appeared in healthy people, the device would not be used on an unhealthy sample in the future. As we observed the intended effects, and side effects did not appear in healthy people in this study, this device could possibly be used with patients in future research. Also, further studies should focus on long-term effects of partial-body vibration in sitting position.
Footnotes
Institutional review board statement: This study was reviewed and approved by the ethical committee of the responsible University faculty (University of Bern; Nr. 2016-5-000004).
Clinical trial registration statement: This study includes no patients and is not registered.
Informed consent statement: All study participants, or their legal guardian, provided informed written consent prior to study enrollment.
Conflict-of-interest statement: All author(s) state that for the current paper there is no financial or other relationship that might lead to a conflict of interest. There is no financial or other involvement of any stakeholders.
Data sharing statement: No additional data are available.
CONSORT 2010 statement: The guidelines of the CONSORT 2010 statement had adopted.
Manuscript source: Invited manuscript
Peer-review started: March 29, 2018
First decision: May 2, 2018
Article in press: May 23, 2018
Specialty type: Orthopedics
Country of origin: Switzerland
Peer-review report classification
Grade A (Excellent): 0
Grade B (Very good): B
Grade C (Good): 0
Grade D (Fair): D
Grade E (Poor): 0
P- Reviewer: Cheung WH, Dye DC S- Editor: Ji FF L- Editor: A E- Editor: Song H
Contributor Information
Yannik Faes, Department of Work and Organizational Psychology, University of Bern, Bern 3012, Switzerland.
Nora Banz, Department of Work and Organizational Psychology, University of Bern, Bern 3012, Switzerland.
Nathalie Buscher, Department of Work and Organizational Psychology, University of Bern, Bern 3012, Switzerland.
Angela Blasimann, Department of Health Professions, Bern University of Applied Sciences, Bern 3008, Switzerland.
Lorenz Radlinger, Department of Health Professions, Bern University of Applied Sciences, Bern 3008, Switzerland.
Patric Eichelberger, Department of Health Professions, Bern University of Applied Sciences, Bern 3008, Switzerland.
Achim Elfering, Department of Work and Organizational Psychology, University of Bern, Bern 3012, Switzerland. achim.elfering@psy.unibe.ch.
References
- 1.GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390:1211–1259. doi: 10.1016/S0140-6736(17)32154-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Wieser S, Tomonaga Y, Riguzzi M, Fischer B, Telser H, Pletscher M, Eichler K, Trost M, Schwenkglenks M. 2014. Die Kosten der nichtübertragbaren Krankheiten in der Schweiz (Costs of non-communicable diseases in Switzerland). Bundesamt für Gesundheit BAG, Bern. Available from: https://www.bag.admin.ch/dam/bag/de/dokumente/npp/forschungsberichte/forschungsberichte-ncd/kosten-ncd-in-der-schweiz.pdf.download.pdf/Schlussbericht%20COI%20NCDs%20in%20CH%202014%2007%2021.pdf. [Google Scholar]
- 3.Elfering A, Mannion AF. 2008. Epidemiology and risk factors of spinal disorders, in Spinal disorders. Springer; pp. 153–173. [Google Scholar]
- 4.Rogan S, Hilfiker R, Herren K, Radlinger L, de Bruin ED. Effects of whole-body vibration on postural control in elderly: a systematic review and meta-analysis. BMC Geriatr. 2011;11:72. doi: 10.1186/1471-2318-11-72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Herren K, Hotz Hangartner C, Oberli A, Radlinger L. Cardiovascular and metabolic strain during stochastic resonance therapy in stroke patients. Physioscience. 2009;5:13–17. [Google Scholar]
- 6.Rittweger J. Vibration as an exercise modality: how it may work, and what its potential might be. Eur J Appl Physiol. 2010;108:877–904. doi: 10.1007/s00421-009-1303-3. [DOI] [PubMed] [Google Scholar]
- 7.Cardinale M, Wakeling J. Whole body vibration exercise: are vibrations good for you? Br J Sports Med. 2005;39:585–589; discussion 589. doi: 10.1136/bjsm.2005.016857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Haas CT, Turbanski S, Kessler K, Schmidtbleicher D. The effects of random whole-body-vibration on motor symptoms in Parkinson‘s disease. NeuroRehabilitation. 2006;21:29–36. [PubMed] [Google Scholar]
- 9.Pang MY. Whole body vibration therapy in fracture prevention among adults with chronic disease. World J Orthop. 2010;1:20–25. doi: 10.5312/wjo.v1.i1.20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Elfering A, Thomann J, Schade V, Radlinger L. Stochastic resonance whole body vibration reduces musculoskeletal pain: A randomized controlled trial. World J Orthop. 2011;2:116–120. doi: 10.5312/wjo.v2.i12.116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Burger C, Schade V, Lindner C, Radlinger L, Elfering A. Stochastic resonance training reduces musculoskeletal symptoms in metal manufacturing workers: a controlled preventive intervention study. Work. 2012;42:269–278. doi: 10.3233/WOR-2012-1350. [DOI] [PubMed] [Google Scholar]
- 12.Elfering A, Arnold S, Schade V, Burger C, Radlinger L. Stochastic resonance whole-body vibration, musculoskeletal symptoms, and body balance: a worksite training study. Saf Health Work. 2013;4:149–155. doi: 10.1016/j.shaw.2013.07.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Elfering A, Schade V, Burger C, Stöcklin L, Bauer S, Radlinger L. Stochastic resonance training at work reduces musculoskeletal pain in nurses. In Duffy V, Lightner N. Advances in Human Aspects of Healthcare. AHFE Conference; USA. 2014. pp. 305–314. Available from: http://boris.unibe.ch/65745/ [Google Scholar]
- 14.Eichelberger P, Fankhauser R, Geering R, Rogan S. Trunk muscle activity and acceleration of the spine during partial-body vibration in a sitting position-a single case study. Physiotherapy. 2015;101:e347. [Google Scholar]
- 15.Lauper M, Kuhn A, Gerber R, Luginbühl H, Radlinger L. Pelvic floor stimulation: what are the good vibrations? Neurourol Urodyn. 2009;28:405–410. doi: 10.1002/nau.20669. [DOI] [PubMed] [Google Scholar]
- 16.Elfering A, Zahno J, Taeymans J, Blasimann A, Radlinger L. Acute effects of stochastic resonance whole body vibration. World J Orthop. 2013;4:291–298. doi: 10.5312/wjo.v4.i4.291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.SUVA. 2017. Unfallstatistik UVG 2017, Koordinationsgruppe für die Statistik der Unfallversicherung, K.f.d.S.d. Unfallversicherung, Editor. Available from: https://www.unfallstatistik.ch/d/publik/unfstat/pdf/Ts17.pdf. [Google Scholar]
- 18.EKAS. 2017. Arbeitssicherheit und Gesundheitsschutz in Bürobetrieben. Available from: http://www.ekas.admin.ch/redirect.php?cat=f%2BR3rLeQL4g%3Did=94. [Google Scholar]
- 19.Okubo Y, Schoene D, Lord SR. Step training improves reaction time, gait and balance and reduces falls in older people: a systematic review and meta-analysis. Br J Sports Med. 2017;51:586–593. doi: 10.1136/bjsports-2015-095452. [DOI] [PubMed] [Google Scholar]
- 20.Kawanabe K, Kawashima A, Sashimoto I, Takeda T, Sato Y, Iwamoto J. Effect of whole-body vibration exercise and muscle strengthening, balance, and walking exercises on walking ability in the elderly. Keio J Med. 2007;56:28–33. doi: 10.2302/kjm.56.28. [DOI] [PubMed] [Google Scholar]
- 21.Issurin VB, Liebermann DG, Tenenbaum G. Effect of vibratory stimulation training on maximal force and flexibility. J Sports Sci. 1994;12:561–566. doi: 10.1080/02640419408732206. [DOI] [PubMed] [Google Scholar]
- 22.Ward LM, Neiman A, Moss F. Stochastic resonance in psychophysics and in animal behavior. Biol Cybern. 2002;87:91–101. doi: 10.1007/s00422-002-0328-z. [DOI] [PubMed] [Google Scholar]
- 23.Luginbuehl H, Lehmann C, Gerber R, Kuhn A, Hilfiker R, Baeyens JP, Radlinger L. Continuous versus intermittent stochastic resonance whole body vibration and its effect on pelvic floor muscle activity. Neurourol Urodyn. 2012;31:683–687. doi: 10.1002/nau.21251. [DOI] [PubMed] [Google Scholar]
- 24.Ross SE, Arnold BL, Blackburn JT, Brown CN, Guskiewicz KM. Enhanced balance associated with coordination training with stochastic resonance stimulation in subjects with functional ankle instability: an experimental trial. J Neuroeng Rehabil. 2007;4:47. doi: 10.1186/1743-0003-4-47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Schollhorn WI, Beckmann H, Michelbrink M, Sechelmann M, Trockel M. Does noise provide a basis for the unification of motor learning theories? Int J Sport Psychol. 2006;37:1–22. [Google Scholar]
- 26.Seniam project. Cited 17 May 2018. Available from: http://www.seniam.org/
- 27.Farlex P. 2012. R-R interval, in Medical Dictionary. Available from: https://medical-dictionary.thefreedictionary.com/R-R+interval. [Google Scholar]
- 28.Giles D, Draper N, Neil W. Validity of the Polar V800 heart rate monitor to measure RR intervals at rest. Eur J Appl Physiol. 2016;116:563–571. doi: 10.1007/s00421-015-3303-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hertel J, Braham RA, Hale SA, Olmsted-Kramer LC. Simplifying the star excursion balance test: analyses of subjects with and without chronic ankle instability. J Orthop Sports Phys Ther. 2006;36:131–137. doi: 10.2519/jospt.2006.36.3.131. [DOI] [PubMed] [Google Scholar]
- 30.Gribble PA, Kelly SE, Refshauge KM, Hiller CE. Interrater reliability of the star excursion balance test. J Athl Train. 2013;48:621–626. doi: 10.4085/1062-6050-48.3.03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Hertel J, Miller SJ, Denegar CR. Intratester and Intertester Reliability during the Star Excursion Balance Tests. J Sport Rehabil. 2000;9:104–116. [Google Scholar]
- 32.Gribble PA, Hertel J. Considerations for normalizing measures of the Star Excursion Balance Test. MPEES. 2003;7:89–100. [Google Scholar]
- 33.Gauvin MG, Riddle DL, Rothstein JM. Reliability of clinical measurements of forward bending using the modified fingertip-to-floor method. Phys Ther. 1990;70:443–447. doi: 10.1093/ptj/70.7.443. [DOI] [PubMed] [Google Scholar]
- 34.Buckup K. 2009. Klinische Tests an Knochen, Muskeln und Gelenken. 5th ed. Thieme, Stuttgart. [Google Scholar]
- 35.Gifford LS. Circadian variation in human flexibility and grip strength. Aust J Physiother. 1987;33:3–9. doi: 10.1016/S0004-9514(14)60579-1. [DOI] [PubMed] [Google Scholar]
- 36.Wieben K, Falkenberg B. 2012. Muskelfunktion: Prüfung und klinische Bedeutung. 6th ed. Georg Thieme Verlag. [Google Scholar]
- 37.Blasimann A. Veränderungen des Finger-Boden-Abstands bei jungen Frauen im Tagesverlauf. Manuelletherapie. 2013;17:233–238. [Google Scholar]
- 38.Toigo M, Boutellier U. New fundamental resistance exercise determinants of molecular and cellular muscle adaptations. Eur J Appl Physiol. 2006;97:643–663. doi: 10.1007/s00421-006-0238-1. [DOI] [PubMed] [Google Scholar]
- 39.Field A. 2009. Discovering statistics using SPSS. 3rd ed. Sage publications. [Google Scholar]
- 40.Cohen J. A power primer. Psychol Bull. 1992;112:155–159. doi: 10.1037//0033-2909.112.1.155. [DOI] [PubMed] [Google Scholar]
- 41.Heart rate variability: standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation. 1996;93:1043–1065. [PubMed] [Google Scholar]
- 42.Elfering A, Schade V, Stoecklin L, Baur S, Burger C, Radlinger L. Stochastic resonance whole-body vibration improves postural control in health care professionals: a worksite randomized controlled trial. Workplace Health Saf. 2014;62:187–196. doi: 10.1177/216507991406200503. [DOI] [PubMed] [Google Scholar]
- 43.Thayer JF, Ahs F, Fredrikson M, Sollers JJ 3rd, Wager TD. A meta-analysis of heart rate variability and neuroimaging studies: implications for heart rate variability as a marker of stress and health. Neurosci Biobehav Rev. 2012;36:747–756. doi: 10.1016/j.neubiorev.2011.11.009. [DOI] [PubMed] [Google Scholar]
- 44.Vrijkotte TG, van Doornen LJ, de Geus EJ. Effects of work stress on ambulatory blood pressure, heart rate, and heart rate variability. Hypertension. 2000;35:880–886. doi: 10.1161/01.hyp.35.4.880. [DOI] [PubMed] [Google Scholar]
- 45.Herren K, Radlinger L. Risks and side-effects of whole body vibration training. WCPT Congress 2011 Amsterdam Holland. Physiotherapy. 2011;97:Supplement S1. Available from: https://www.researchgate.net/publication/ 296456229_RISKS_AND_SIDEEFFECTS_OF_WHOLE_BODY_VIBRATION_TRAINING. [Google Scholar]