

Abstract
Introduction:
In anorectal disorders, incidences of piles and fissures are increasing in Indian population due to western lifestyle. Many surgical methods are available to cure anorectal disorders, but now a days, demand for Ayurveda and herbal preparation is increasing in society.
Materials and Methods:
In this study, Apamarga Kshara application, infrared coagulation (IRC) procedure and Arshohara Vati (AV) tablet were administered for the management of internal hemorrhoid (Arsha). This study was an open labelled, prospective, interventional study, in which patients of piles [n = 30 (10 each group)] were selected from OPD of Institutional hospital. Apamarga Kshara application (AKA) was done on the internal piles for 1–3 sittings as per requirement, IRC was applied at the base of piles for one sitting and two tablets (500 mg each tablet) of AV were given orally thrice a day for 15 days. In all the three groups, the patients were assessed every week for 1 month and were followed up for another 1 month for relief in signs and symptoms.
Results:
Obtained results were analyzed and encouraging results were observed after completion of the treatment.
Conclusion:
The study concluded that Apamarga Kshara application is the most effective treatment for the management of internal hemorrhoid of 1st and 2nd degree in comparison to IRC procedure and administration of Arshohara Vati.
Keywords: Apamarga, Arsha, Arshohara Vati, Ayurveda, hemorrhoids, Kshara, piles
Introduction
Hemorrhoids is one of the common anorectal disorders that equally affect men and women.[1] The worldwide prevalence of hemorrhoids is around 4.4% and incidences increase with age. The pregnancy is also a predisposing risk factor for the development of symptomatic hemorrhoids in females.[2] The symptoms of piles are bleeding, pain, protrusion of piles, and perianal itching. Conservative medical treatment of hemorrhoids includes use of fiber supplements; lifestyle modifications may include relieving constipation, avoiding straining, proper fluid intake, better anal hygiene and sitz baths.[3] If the patients do not respond to conservative measures, rubber band ligation, sclerotherapy, infrared coagulation (IRC) and cryosurgery are some outpatient department (OPD) procedures.[4] Surgery, i.e. hemorrhoidectomy, for hemorrhoids is indicated in fourth grade when symptoms of bleeding, pain and prolapsed piles compromise the quality of life. In this context, Sushruta has mentioned four types of treatment modalities such as medical management (medicine), Ksharakarma (use of Kshara/Ksharasutra), Agnikarma (cauterization) and surgery according to the nature of Arsha (piles) with surgery as the last option.[5]
Treatment by the use of herbs is known to human beings since centuries. Recently, herbal treatments have gained popularity with documented effects on the influence of blood vessel wall tone, decrease of capillary permeability, improved circulation, decrease of edema and blockage of inflammatory mediators. It has been observed that anorectal disorders such as hemorrhoids can be managed by topical administration of Apamarga Kshara, IRC procedure and oral administration of Arshohara Vati that offer a significant and faster relief resulting in improved quality of life. Hence, the study has been planned to compare the efficacy of Apamarga Kshara, IRC and Arshohara Vati in the management of internal hemorrhoid of 1st and 2nd degree.
Materials and Methods
This study was an open, prospective, interventional study of 4 weeks. Patients having complaints of internal hemorrhoid of 1st and 2nd degree were selected from the OPD, department of Shalya Tantra, IPGT & RA, Jamnagar, Gujarat. Detailed clinical history and physical and local per rectal findings were recorded in clinical research proforma.
Inclusion criteria
Patients of either gender between 18 and 65 years; with 1st and 2nd degree internal piles; with Mridu, Prastruta, Avagadha, and Uchrita (soft, deep-seated and elevated piles) type of Arsha; with controlled blood pressure, diabetes mellitus (DM) and cardiac disorders were included in the study.
Exclusion criteria
Patients of either gender less than 18 years and >65 years; patients with 3rd and 4th degree piles; patients having rectal prolapse, fissure and fistula-in-ano having uncontrolled hypertension, diabetes mellitus and cardiac disorders; patients with malignancy of any organ; pregnant women and hepatitis B, tuberculosis, HIV and venereal disease research laboratory (VDRL) positive cases were excluded from the study.
Investigations
Routine hematological, biochemical, and microbial investigations such as Hb% (hemoglobin), total leukocyte count, differential leukocyte count, bleeding time, clotting time, erythrocyte sedimentation rate, fasting blood sugar, postprandial blood sugar, blood urea, serum creatinine, were done at baseline and at the end of the study and HIV, VDRL and HbSAg were done at baseline in the patients of the Arshohara Vati (AV) group.
Ethical clearance
The present clinical trial is approved by Institutional Ethics Committee vide letter no. PGT/7/_A/Ethics/2015_16/1490 (Dated 25/08/15) and is registered in CTRI. (CTRI/2016/12/007562 on 9/12/2016).
Ingredients of trial drugs
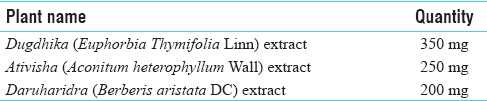
Apamarga Kshara [Table 1] was prepared in Shalya Tantra Department of the Institute and Arshohara Vati was provided by Dr. Vasishth's Ayu Remedies, Ahmedabad [Table 2].
Table 1.
Ingredients of Apamarga Kshara

Table 2.
Composition of Arshohara Vati
Grouping
Group Apamarga Kshara application (AKA): Apamarga Kshara paste application was done for one to three sittings as needed
Group IRC: IRC procedure was done for one sitting on all the piles masses
Group AV: Oral administration of Arshohara Vati tablet 500 mg, 2 tablets thrice a day after food for 15 days.
Do's and don’ts
Patients were advised to consume fiber-rich diet, green vegetables, plenty of water and buttermilk. Patients were advised to avoid spicy, non-vegetarian diet, oily and junk foods. A daily morning walk for half an hour was also advised.
Assessment criteria
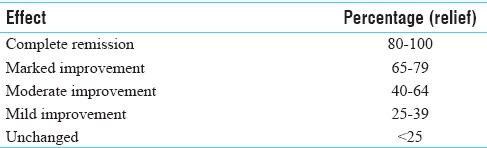
Efficacy was assessed for reduction in intensity of the following signs and symptoms during treatment weekly. Bleeding per rectum, painful defecation, prolapsed piles and discharge per rectum based on gradations were assessed. Overall assessment was done as shown in Table 3.
Table 3.
Overall assessment of effect
Statistical analysis
Statistical tests such as “Student's paired t-test,” “Wilcoxon signed-rank test” and “Kruskal–Wallis” were applied to assess the results.
Observations and Results
In this study of 30 patients with treatment period of 4 weeks observational study, 23 patients were male and 7 were female. Male predominance was found higher, which might be due to reporting of more male patients to the anorectal department. Twenty-six patients were from the age group of 18 and 40 years and the remaining were between 41 and 65 years, which showed that most of the patients were of the middle-age group. Six patients reported a family history of piles although considering this small sample study it is difficult to say that piles and fissures are hereditary diseases as it requires survey study on more samples. Of 30 patients, 19 patients had irregular bowel habits and 21 patients complained of constipation and hard stools. The constipation and irregular bowel movement are the main etiological factors of piles and fissure.
In this stduy, bleeding per rectum was present in 26 patients, among whome it was moderate in 25 patients. In maximum 11 patients PR bleeding was dropping in nature. In relation to defecation, a maximum of 16 patients had bleeding after defecation. A total of 22 patients had prolapse piles per rectum, where a maximum of 17 patients had spontaneous reduction of piles. A maximum of 21 patients had painful defecation, among them 18 patients had burning type of pain and 15 patients had mild pain. In 12 patients, serous type of discharge per rectum was reported.
Effect of therapy
In bleeding per rectum, it was observed that in Group AKA, the maximum improvement was noted on 21st day with 100% relief. This is due to the properties of Kshara such as Stambhana (haemostatic), Pachana (digestive) and Dahana (cauterized) mentioned in the texts to achieve hemostasis. In Group IRC, it was observed that maximum improvement was noted on the 21st day with 62.50% of relief. Heat created by IRC beam leads to scaring and tissue fixation, which leads to shrinking of hemorrhoids and recedes ultimately.[6] In Group AV, the maximum improvement was noted on 28th day with 100% relief. This is due to Stambhana properties of the drugs [Table 4].
Table 4.
Effect of therapy on bleeding per rectum
In painful defecation, it is observed that in Group AKA, the maximum improvement was noted on the 21st day with 100% relief. Painful defecation might be taken care off due to Ksharana (debriding), Pachana (digestive), Amahara (detoxifying) and Tri-Doshahara properties of Apamarga Kshara. In Group IRC, it is observed that the maximum improvement was noted on 14th day with 55.55% relief. This might be due to the fact that the heat that produced coagulates the engorged part of the vein, reducing painful defecation during strain. In Group AV, the maximum improvement was noted on the 21st day with 100% relief. This is due to Tridoshaghna (pacification of Tridosha) property [Table 5].
Table 5.
Effect of therapy on painful defecation
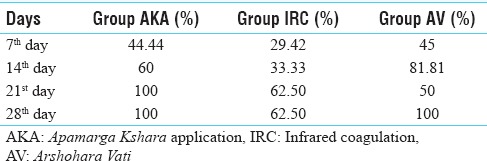
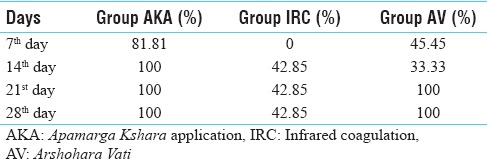
In prolapse per rectum, it is observed that in Group AKA, the maximum improvement was noted on the 14th day with 100% relief. Prolapse of pile mass might be reduced due to Vilayana (melting), Shodhana (purifying), Shoshana (drying), and Lekhana (scraping) properties of Kshara. In Group IRC, it is observed that the maximum improvement was noted on the 14th day with 42.85% relief. Heat created by infrared light causes a firm scar tissue at the base of pile masses which fixes nearby veins and mucosa in place, so they do not bulge out much into the anal canal. In Group AV, the maximum improvement was noted on the 21st day with 100% relief. This is due to its Vilayana (melting) and Shoshana (drying) properties of ingredients present in the trial drug [Table 6].
Table 6.
Effect of therapy on prolapse piles
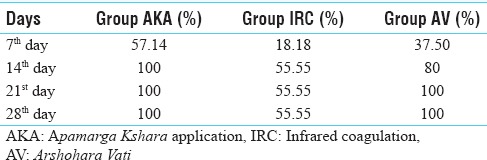
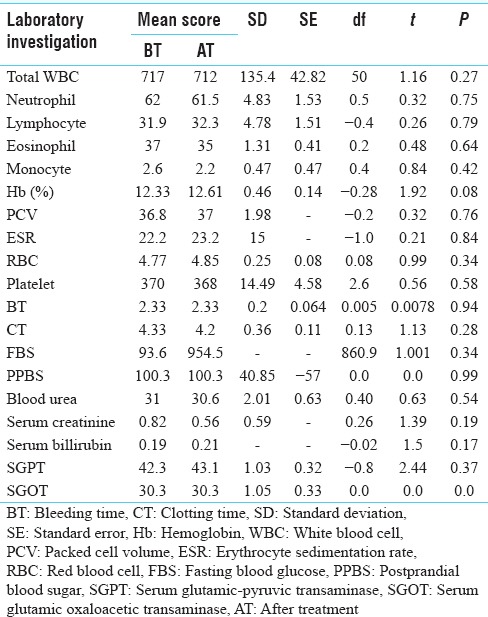
In discharge per rectum, it is observed that in Group AKA, the maximum improvement was noted on the 7th day onwards with 100% relief. Discharge per rectum may be tackled due to Shoshana (drying), Tikshana (penetrating), Stambhana (haemostatic) and Dahana (cauterization) properties. In Group IRC, it is observed that the maximum improvement was noted on the 14th day with 50% relief. Heat created by the infrared light causes mucosal burn and scar; hence, discharge subsides up to some extent. In Group AV, the maximum improvement was noted on the 14th day for 100% relief. This may be due to Pachana (digestive), Shoshana (drying) and Stambhana (haemostatic) properties of ingredients of the tablet [Table 7]. In patients of Group AV, two tablets (500 mg) of Arshohara Vati, thrice a day after food, were given orally in 10 patients, so the laboratory investigations were done in these patients before and after the treatment to assess the effect of drugs on these investigations. The findings showed that the change occurred with the treatment is not great enough to exclude the possibility that the difference in value is due to chance [Table 8]. Markers of inflammation like WBC neutrophils and eosinophils count were found reduced after treatment.
Table 7.
Effect of therapy on discharge per rectum
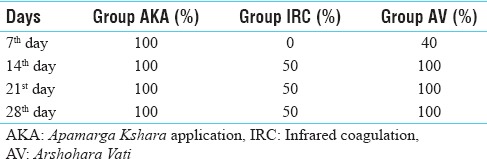
Table 8.
Effect on hematological investigations (paired t-test) in patients of AV group only
Overall assessment
Overall effect of therapy in Group AKA showed 80% (n = 8) of patients got complete remission. In Group IRC, it was noted that 20% of patients got complete remission and in Group AV, it was noted that 30% (n = 3) of patients got complete remission. Hence, it can be said that the patients with piles of 1st and 2nd degree were managed best by AKA group [Table 9].
Table 9.
Overall effect of therapy (n=10 each group)

Discussion
The present study of Apamarga Kshara, IRC and AV was designed to evaluate the efficacy of each treatment in the management of piles. Statistically highly significant results were obtained in patients of 1st and 2nd degree piles. In cases of internal piles, highly significant result was seen in features of bleeding per rectum and prolapse of piles irrespective of the decrease in size of piles in Group AKA. In Group AV, significant results were found in relieving painful defecation as well as discharge per rectum.
The percentage of relief after treatment has been calculated statistically; in Group AKA, 100% relief was noted in bleeding per rectum, 75% relief was noted in both painful defecation and discharge per rectum and 87.50% relief was found in prolapse of piles per rectum. In Group IRC, 87.50% relief was noted in bleeding per rectum, 62.50% relief was noted in painful defecation, 50% relief was noted in discharge per rectum, and 42.86% relief was noted in prolapse of piles. Whereas, in Group AV, 88.33% relief was noted in bleeding per rectum, 91.33% relief was noted in painful defecation, 100% relief was noted in discharge per rectum and 68.75% relief was noted in prolapse of piles.
Apamarga Kshara exerts many actions such as incision, excision debridement, scrapping and dissolution and Kshara cauterizes the tissue indirectly by virtue of its Ksharana property (corrosiveness), in the form of local application. It is due to its properties such as Pachana, Tikshana, Vilayaka, Shodhana, Shoshana, Amahara, Dahana, Stambhana and Lekhana that reduced all the symptoms in case of internal hemorrhoid.[7]
IRC creates a small burn, resulting in a minimal tissue injury (to a depth only approximately 3 mm); then, it results in less scaring and tissue fixation, which leads to shrinking of hemorrhoids and recedes ultimately.[5]
AV is a combination of three herbal drugs (Dugdhika, Ativisha, and Daru Haridra) that have several potencies which are capable to squeeze the pile cushion (formed by the blood vessels, connective tissue and smooth muscles), thus reducing the congestion of the blood in the pile mass, helping regulate the bowel movements and in turn lessen the need to strain at stools, improving digestion by improved production of the digestive enzymes and reducing venous engorgement.
Conclusion
The study concluded that group Apamarga Kshara application has been a better potential to treat internal piles of up to 2nd degree in comparison to infrared coagulation procedure and Arshohara Vati administration. The procedure is cost and time effective and without adverse effects.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Janicke DM, Pundt MR. Anorectal disorders. Emerg Med Clin North Am. 1996;14:757–88. doi: 10.1016/s0733-8627(05)70278-9. [DOI] [PubMed] [Google Scholar]
- 2.Avsar AF, Keskin HL. Haemorrhoids during pregnancy. J Obstet Gynaecol. 2010;30:231–7. doi: 10.3109/01443610903439242. [DOI] [PubMed] [Google Scholar]
- 3.Billingham RP, Isler JT, Kimmins MH, Nelson JM, Schweitzer J, Murphy MM, et al. The diagnosis and management of common anorectal disorders. Curr Probl Surg. 2004;41:586–645. doi: 10.1016/j.cpsurg.2004.04.002. [DOI] [PubMed] [Google Scholar]
- 4.Surgery of the Anus, Rectum and Colon. By, John Goligher with Collaboration of Herbort Duthie. Horold Nixon: A.I.T.B.S. Publishers and Distributors. 2002:131–4. [Google Scholar]
- 5.Acharya Y T, editor. 9th ed. Ch 6, Ver 3. Varanasi: Chaukhambha Orientalia; 2009. Sushruta Samhita of Sushruta, Chikitsa Sthana; p. 430. [Google Scholar]
- 6.Johanson JF, Rimm A. Optimal nonsurgical treatment of hemorrhoids: A comparative analysis of infrared coagulation, rubber band ligation, and injection sclerotherapy. Am J Gastroenterol. 1992;87:1600–6. [PubMed] [Google Scholar]
- 7.Matu MS, Kotangale YT, Rai AK. Topical application of Apamarg Kshara in hypergranulated wound management: A case study IAMJ. 2015;3(5):1569–71. [Google Scholar]