

Abstract
Background:
Due to sedentary lifestyle and stress, the incidence of metabolic disorders are increasing day by day. Among these polycystic ovarian syndrome (PCOS) is an intricate disorder affecting 4%–8% women in their reproductive age and related to ovarian dysfunction characterized by obesity, oligomenorrhea, anovulation and hyperandrogenism. In modern system of medicine, the available allopathic regimen has its own limitations, so it is need of time to find a safe and effective alternative therapy for such type of condition. The most common symptom in 85%–90% of PCOS patients is oligomenorrhea which can be correlated to Artava Kshaya (loss of menstrual fluid) in Ayurveda. Hence, in the present clinical study, Vamana Karma (therapeutic vomiting) with Ikshwaaku seed formulation followed by Shatapushpadi Ghanavati was planned.
Aims:
To evaluate the efficacy of Vamana Karma (therapeutic vomiting) followed by Shatapushpadi Ghanavati in the management of Aartava Kshaya (loss of menstrual fluid) w. s. r to PCOS.
Materials and Methods:
A total of 15 patients of PCOS were clinically diagnosed and treated by Vamana Karma (therapeutic vomiting) procedure with Ikshwaaku seed formulation. After completion of Vamana Karma (therapeutic vomiting) and Samsarjana Krama, (post therapy dietary regimen for revival) Shatapushpadi Ghanavati 2 Vati (each 500 mg) twice in a day with lukewarm water was given for 45 days. After completion of 2-month trial, assessment of therapy was estimated by subjective and objective parameters.
Results:
Statistically extremely significant (P < 0.0001) results were found in menstrual irregularities, obesity, and body mass index. The significant result in reduction of nondominant follicles (P = 0.01 and 0.03 for right and left ovary, respectively), lowering the fasting blood sugar level (P = 0.02) and hirsutism (P = 0.03) was found.
Conclusion:
Vamana Karma (therapeutic vomiting) followed by Shatapushpadi Ghanavati is very effective in the management of obese PCOS patients and increasing chances of conception.
Keywords: Artava Kshaya, polycystic ovarian syndrome, Shatapushpadi Ghanavati, Vamana Karma
Introduction
Polycystic ovarian syndrome (PCOS) is a most prevalent endocrinopathy which affects 4%–8% of women of reproductive age.[1] Forty percent of women have anovulatory infertility due to PCOS.[2] In this condition, hormonal imbalance affects follicular growth during the ovarian cycle causing the affected follicles to remain in immature form, leading to multiple ovarian cysts associated with obesity, oligomenorrhea, etc. Incidence of this disease is increasing nowadays because of sedentary lifestyle, pollution and excessive intake of junk food.[3]
In Ayurveda, such type of condition can be correlated under the broad heading of Artava Kshaya, as oligomenorrhea is the most common symptom affecting 85%–90% of PCOS patients.[4] The treatment advised for Artava Kshaya includes Samshodhana (bio purification) followed by Agneya drug and is the line of treatment according to Acharya Sushruta.[5] In further commentary on Sushruta Samhita, Dalhana describes Vamana Chikitsa (therapeutic emesis) for the same. For this purpose, Ikshwaaku seed formulation was specifically selected for Vamana Karma (therapeutic vomiting) as it is advised for Kapha and Granthi Vikara (cystic swellings).
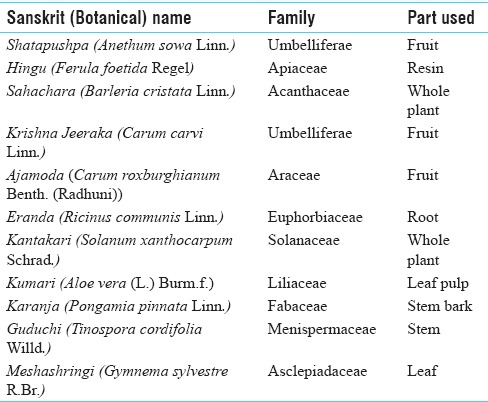
Shatapushpadi Ghanavati [Table 1] contains Agni Mahabhuta (fire element) predominant drugs, which corrects the residual pathology in the context of PCOS.
Table 1.
Contents of Shatapushpadi Ghanavati
Aims and objectives
To evaluate the efficacy of Vamana (therapeutic vometing) followed by Shatapushpadi Ghanavati on Artava Kshaya (loss of menstrual fluid) in relation to PCOS and to assess the findings based on ultrasonography (USG), obesity (body weight, body mass index [BMI], waist-hip ratio [WHR]) and blood sugar level in relation to PCOS.
Materials and Methods
A total of 15 female patients fulfilling the criteria for diagnosis of Artava Kshaya and PCOS were selected from the Outpatient and Inpatient Department of Panchakarma, National Institute of Ayurveda, Jaipur. Ethical clearance was obtained from Institutional Ethics Committee, dated November 7, 2014 (Approval number F10 (5)/EC/2014/7218), before commencement of the study. Informed consent was taken from each registered patient before starting the treatment. The trial is also registered in the Clinical Trial Registry of India (trial no: CTRI/2017/02/007825).
Study protocol
Study type: Interventional
Purpose: Treatment
Masking: Open label
Timing: Prospective
Endpoint: Efficacy and safety
Number of groups: One
Number of patients: 15 patients.
Drugs used in the trial
All the medicines were procured from NIA Pharmacy, Jaipur, except Ikshwaaku fruit [Figure 1], which was collected from post Aagadgaon, district Ahmednagar, Maharashtra (authenticated by the Department of Botany, Rajasthan University, Jaipur, with authentication number RUBL211524 dated April 11, 2015).
Figure 1.

Ikshwaaku fruit
Total duration of trial
The trial duration was 2 months.
Diagnostic criteria
Patients fulfilling the revised Rotterdam criteria (2003) were included.
The criteria state that two out of the following three criteria should be present in the diagnosis of PCOS:
Oligo-anovulation
Clinical and/or biochemical hyperandrogenism
Polycystic ovaries in USG (antral follicle count ≥12 and/or ovarian volume >10 ml).
Inclusion criteria
Age group 20–40 years (unmarried and married patients)
Diagnosed cases of PCOS
Irregular menses/scanty menses due to anovulatory cycle
Patient fit for Vamana Karma.
Exclusion criteria
Cervical tumor, polyp, carcinoma cervix
Uterine fibroid
Congenital anomalies of female genital tract
Tuberculous endometritis
Congenital adrenal hyperplasia
HIV/venereal disease research laboratory/HbsAg positive
Malignant disease and patients on cytotoxic drugs
Patient not fit for Vamana Karma.
Laboratory investigations
Following investigations were carried out before and after treatment.
Fasting blood sugar (FBS) level
Postprandial blood sugar (PPBS) level
USG (abdomen and pelvis)
Physical parameters such as body weight, BMI and WHR were also assessed.
Methodology
Procedure
Vamana Karma (therapeutic emesis)
Vamana Karma was administered in the following steps.
Panchakola powder[6] was used for Deepana and Pachana in the dosage of 3 g twice in a day before food for 3–7 days with lukewarm water followed by Snehapana (administration of oil orally) with Murchita Tila Taila[7] with initial 30 ml dose, increasing day by day according to Agni (digestive fire) and Koshtha (bowl motion habit) of the patient till Samyak Snigdha Lakshana (symptoms of complete oleation on body) were obtained. Dashamoola Taila was used for external therapeutic massage of oil to the entire body and Dashamoola Kwatha were used for external complete body massage with medicated oil for 2 days prior and on the day of Vamana.
Administration of Vamana Yoga-Ikshwaaku seed powder in the dosage of 5– 7 g with other conventional drugs such as Yashtimadhu (Glycyrrhiza glabra Linn.), Vacha (Acorus calamus Linn.), rock salt and honey.
Samsarjana Karma
The specific diet plan was advised to the patient according to Avara, Madhyama and Pravara Shuddhi (low, medium and complete purification level) after classical Vamana procedure.
Follow-up
Shatapushpadi Ghanavati (compounded formulation) was given for 45 days in the dose of 1 g (2 tablets each of 500 mg) for 2 times a day 1 or ½ h before food with lukewarm water.
Assessment criteria
Objective parameters
Blood sugar (fasting and postprandial)
Body weight, BMI, WHR
USG (includes endometrial thickness [ET], ovarian volume and number of nondominant follicles [NDF]).
Subjective parameters
Menstrual irregularities (includes duration, interval and pain associated with menses)
Acne
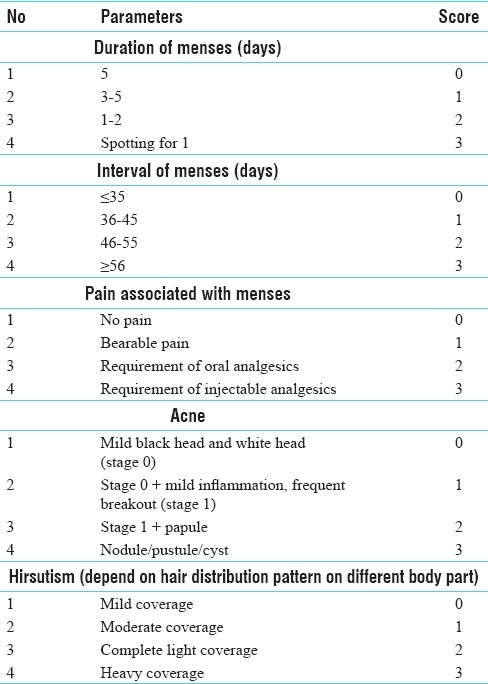
Hirsutism (based on Ferriman–Gallwey score). A special scoring pattern was adopted for assessment of subjective parameters [Table 2].
Table 2.
Scoring pattern of subjective parameters
Statistical analysis
Student's paired t-test was applied for objective parameters. Wilcoxon sign-rank test was applied out for analysis of all subjective parameters.
The obtained results were interpreted as follows:
>0.10 nonsignificant (NS)
<0.05 significant* (S)
<0.01 very significant** (VS)
<0.001 highly significant***
< 0.0001 extremely significant**** (ES).
Statistical software used
GraphPad InStat for Windows version 3.06, La Jolla, CA, USA, was used.
Observations
All patients had chief complaint of menstrual abnormalities, 33.33% patients had positive family history of diabetes, 73.33% patients had chronicity of PCOS >5 years. History of hair fall was noted in 76.66% of patients. Maximum patients 73.33% had hormonal therapy as treatment history, maximum patients (60%) reported consumption of Madhura Rasa dominant diet, 46.67% patients were taking Snigdha Ahara (fatty foods like milk products, etc.). 66.67% of the patients were addicted to tea, 60% were suffering from stress. All patients were having Artava Vaha Srotas Dushti (vitiated channels of female reproductive system) and 80% had history of not doing any physical exercise [Graph 1].
Graph 1.
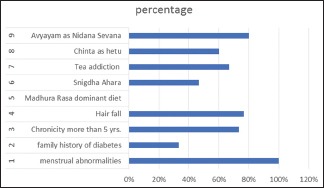
Observations related to PCOS
Results
Effect of therapy on subjective parameters
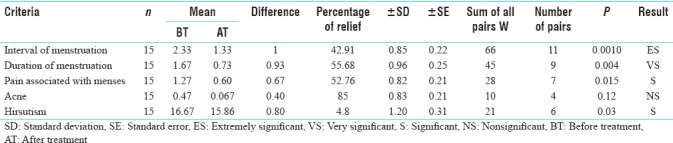
Out of 15 patients statistically extremely significant (ES) results were found in prolonged interval of menses (42.91%), very significant (VS) result in delayed menses (55.68%), significant result in painful menses (52.76%), nonsignificant (NS) changes in acne (85%) and significant changes were observed in hirsutism (4.8%) [Table 3].
Table 3.
Effect of therapy on subjective parameters
Effect of therapy on ultrasonography
Statistically results were found in mean effect of therapy (ET) (8.19%) and ovarian volume (right [32.66%] and left [15.77%] side of ovary). Statistically significant changes were observed in mean NDF of right (26.39%) and left (21.42%) side of the ovary after Vamana followed by Shatapushpadi Ghanavati [Table 4].
Table 4.
Effect of therapy on ultrasonographical parameter

Effect of therapy on other parameters
Effect of therapy on blood sugar
Out of 15 patients, significant change in FBS was noted in 8.33% patients and NS results were observed in PPBS in 5.56% patients [Table 5].
Table 5.
Effect of therapy on blood sugar

Effect of therapy on body weight, body mass index, and waist-hip ratio
In the present clinical study, statistically ES result was found in body weight (5.54%) and BMI (5.55%). Non-significant change was observed in WHR (0.83%) [Table 6].
Table 6.
Effect of therapy on body weight, body mass index, and waist-hip ratio

Overall effect of therapy on subjective parameter
On menstrual disorder
Of 15 patients, 3 (20%) patients got complete remission, 2 (13.33%) patients got moderate improvement, 5 (33.33%) patients got mild improvement and 4 (26.66%) patients had no improvement at all.
Acne
Of 15 patients, 3 (20%) patients got complete remission, 1 (6.66%) patient had mild improvement and 11 (73.33%) patients remain unchanged.
Hirsutism
Of 15 patients, all remained unchanged [Graph 2].
Graph 2.
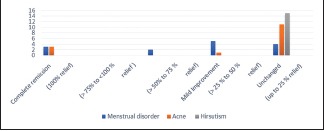
Total effect of therapy based on subjective assessment criteria
Discussion
Effect of therapy on primary outcome measures
The primary outcome of therapy is regularization of menstrual cycle in relation to interval, duration and pain associated with it. ES results (P = 0.0010) were found in interval of menses, VS (P = 0.004) in duration of menses, and significant result (P = 0.015) in pain associated with menses. Artava Kshaya results due to vitiation of Rasa Dhatu (plasma and lymphatic tissues) and involvement of Kapha and Vata. Vamana is Srotoshodhaka (clearing micro-channels in the body) in nature. Shatapushpadi Ghanavati has Deepana (Stomachic), Pachana (Digestant), Agni Deepana (increases digestive procedures) and Artava Janana (regularize menstruation) properties. Hence, Vamana followed by Shatapushpadi Ghanavati removes the obstruction of flow of Vata and increases the Artava Dhatu (female reproductive tissues) qualitatively as well as quantitatively which help in menstrual irregularities.
The Vamana drug Ikshwaku has testosterone-lowering effect which may decrease the androgen level of body. Hence, after Vamana, significant relief in hirsutism (P = 0.03) was observed.
Effect of therapy on secondary outcome measures
Significant result (P = 0.01 for right ovary and P = 0.03 for left ovary) was found in decreasing number of NDFs. Vamana with Ikshwaaku has testosterone-lowering effect.[8] The decrease level of luteinizing hormone stimulates follicle-stimulating hormone level, which is helpful in maturation of follicles. Further Aam Pachana (detoxification of metabolic toxins), Agni Deepana (increases digestion) properties of Shatapushpadi Ghanavati help in reducing the NDFs directly.
Effect of therapy on associated factors
The significant result (P = 0.02) was obtained in decrease in FBS level after completion of therapy. Vamana Karma along with Shatapushpadi Ghanavati has Agni Deepana (increases digestion), Sroto Shodhaka (clearing micro-channels in the body) properties, which indirectly increase the metabolism of liver which is the prime site of glucose metabolism. In support to this, advanced researches show that Ikshwaku has lipid-lowering, hypoglycemic effect.[9]
ES (P < 0.0001) results were found in obesity and BMI after completion of therapy. Sthaulya (obesity) is the Rasapradoshaja Vikara (disease caused due to vitiation of plasma and lymphatic tissues). As Vamana Karma cleanses microchannels of body, further Shatapushpadi Ghanavati has Sroto Shodhaka (clearing micro-channels in the body), Agni Deepana (increases digestion) and Lekhana (scraping) properties which scrap excess Meda (fat) from body and help in reducing body weight in general and BMI specifically.
Probable mode of Vamana Karma
Vamana Karma is the best therapy for the elimination of Kapha Dosha. According to Ayurveda, PCOS may be considered as Agni Vaishamyajanya Vikara (disease caused due to vitiation of metabolism) in general and Rasagni (metabolism at Rasa Dhatu level) and Medodhatvagni (metabolism at Meda Dhatu level) Mandya deficient in particular with Bahu Dosha Avastha (vitiated Dosha). As far as Dosha is concerned based on the pathology and symptom complex, it is Kapha-Vataja disorder. Due to increased Kapha and Agnimandya (deficient metabolism), more number of follicles are produced but not matured, resulting in cyst formation causing obstruction to the flow of Vata in proper direction, which in turn aggravates and results into anovulation and oligomenorrhea as Prakrita Vata (balanced Vata Dosha) is responsible for proper menstruation. Hence, the treatment should be planned to correct Agni, eliminate vitiated excessive Kapha Dosha and correct Vata Dosha by providing proper movement of Vata. To eliminate vitiated Dosha and to improve Agni, Samshodhana Chikitsa (bio purification) is a preferred treatment in Ayurveda.
Further Ikshwaaku seed formulation was preferred for Vamana Karma as it is specifically mentioned for Kapha and Granthi Vikara (cystic masses).[10] As PCOS is metabolic disorder, Vamana helps to increase metabolism of body, thereby reducing weight and specifically act on liver metabolism which is the main site of hormone formation. Furthermore, there is direct relation of estrogen and obesity. Weight loss can improve not thus increased only circulating androgen and glucose levels but also helps for ovulation and thus increases pregnancy rate in obese women with PCOS.[11]
After Samshodhana (bio purification) to correct the residual pathology, Shatapushpadi Ghanavati was selected which was prepared using known Kapha Vatahara (pacifying Kapha and Vata Dosha), Agni Deepana (increases digestion), Artava Pravartaka (regularize menstruation) and Garbhashaya Shodhaka (detoxify and improves the function of uterus)drugs.
With respect to the pathology of PCOS, Ushna (hot), Tikshna (sharp), Ruksha (dry) and Lekhana (scraping) properties of the ingredients of Shatapushpadi Ghanavati normalizes Kapha vitiation and Vatavaigunya (vitiated Vata Dosha), reduces excess Meda (fat), removes Srotorodha/Sanga (blockage in micro-channels of the body) and creates normal functioning of Apana Vata (subtype of Vata which responsible for expulsion of waste) thereby regularizing the function of Aartavavaha Srotas as Prakrita Vata is responsible for proper menstrual flow.
Conclusion
Vamana Karma followed by Shatapushpadi Ghanavati is effective in regularizing menstruation, achieving considerable reduction in body weight and BMI, and helpful in lowering FBS level. Thus, this treatment protocol can be useful in the management of obese PCOS patients. Further, a large sample size study may help to support the findings of the study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Azziz R, Woods KS, Reyna R, Key TJ, Knochenhauer ES, Yildiz BO, et al. The prevalence and features of the polycystic ovary syndrome in an unselected population. J Clin Endocrinol Metab. 2004;89:2745–9. doi: 10.1210/jc.2003-032046. [DOI] [PubMed] [Google Scholar]
- 2.Teede H, Deeks A, Moran L. Polycystic ovary syndrome: A complex condition with psychological, reproductive and metabolic manifestations that impacts on health across the lifespan. BMC Med. 2010;8:41. doi: 10.1186/1741-7015-8-41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Khot Bhagyashri, Lad Meenal, Patil Arun, Kakad Anil. Clinical efficacy of Ayurveda treatment on polycystic ovarian syndrome. IOSR J Pharm. 2013;3(4):21–5. [Google Scholar]
- 4.Hart R. Definitions, Prevalence and Symptoms of Polycystic Ovaries and the Polycystic Ovary Anshan, Ltd. 2007. [Last accessed on 2015 Aug 20]. pp. 15–26. Available from: https://www.ncbi.nlm.nih.gov/pubmed/15380140 .
- 5.Sharma A, editor. Ch. 15, Ver. 16. Varanasi: Chaukhamba Surbharti Prakashan; 2009. Sushruta Samhita of Sushruta with Sushrut, Sutra Sthana. 2010 Reprint edition; p. 120. [Google Scholar]
- 6.Shastri P, editor. 1st edition. Ch 4, Ver 8-11. Varanasi: Chaukhambha Sanskrit Samsthana; 2000. Shranghadhara Samhita of Sharanghadhra, Uttara Khanda; p. 313. [Google Scholar]
- 7.Mishra S, editor. 1st edition. Ch 5, Ver 1267-1268. Varanasi: Chaukhamba Surbharti Prakashan; 2015. Bhaishajya Ratnawali of Gananatha Sen; p. 206. [Google Scholar]
- 8.Malini T, Vanithakumari G. Antifertility effects of beta-sitosterol in male albino rats. J Ethnopharmacol. 1991;35:149–53. doi: 10.1016/0378-8741(91)90066-m. [DOI] [PubMed] [Google Scholar]
- 9.Katare C, Agrawal S, Jain M, Rani S, Saxena S, Prakash SB, et al. Lagenaria siceraria: A potential source of anti-hyperlipidemic and other pharmacological agents. [Last accessed on 2015 Oct 19];Curr Nutr Food Sci. 2011 7:1–7. Available from: http://www.austinpublishinggroup.com/ [Google Scholar]
- 10.Shukla V, Tripathi R, editors. Reprint Edition. Ch 3, Ver 9. Delhi: Chaukhamba Sanskrit; 2010. Charak Samhita of Agnivesh, Kalpasthan; p. 820. [Google Scholar]
- 11.Patel SM, Nestler JE. Fertility in polycystic ovary syndrome. [Last accessed on 2015 Aug 24];Endocrinol Metab Clin North Am. 2006 35:137–55. doi: 10.1016/j.ecl.2005.09.005. vii. Available from: https://www.ncbi.nlm.nih.gov/pubmed/16310646 . [DOI] [PubMed] [Google Scholar]