

Abstract
Sex steroid hormone signaling is critical in the development of breast cancers, although the role of the androgen receptor remains unclear. This study evaluated androgen receptor (AR) expression in normal breast tissue as a potential marker of breast cancer risk. We conducted a nested case–control study of women with benign breast disease (BBD) within the Nurses’ Health Studies. Epithelial AR expression was assessed by immunohistochemistry in normal tissue from the BBD biopsy and the percent of positive nuclei was estimated in ordinal categories of 10% for 78 breast cancer cases and 276 controls. Logistic regression models adjusting for the matching factors and BBD lesion type were used to calculate odds ratios (ORs) for the association between AR expression (tertiles: ≤10%, 11–30%, and >30%) and breast cancer risk. AR expression in normal breast tissue was not associated with subsequent breast cancer risk (ORT3vsT1 = 0.9, 95% CI = 0.4–1.8, p trend = 0.68). In comparison with low AR/low ER women, ORs of 0.4 (95% CI = 0.1–1.2) for high AR/high ER women, 1.8 (95% CI = 0.4–7.8) for low AR/high ER women, and 0.7 (95% CI = 0.3–1.6) for high AR/low ER women were observed (p interaction = 0.21). Ki67 did not modify the association between AR expression and breast cancer risk (p interaction = 0.75). There was little evidence for an overall association between AR expression in normal breast tissue and breast cancer risk. These findings did not show that the AR association varied by Ki67 expression in normal breast tissue, though there was suggestive heterogeneity by ER expression.
Molecular epidemiology: Male hormone receptor expression not linked to cancer risk
Levels of male hormone receptors in normal breast tissue do not seem to impact a woman’s risk of developing breast cancer. Kevin Kensler from the Dana-Farber Cancer Institute in Boston, Massachusetts, USA, and colleagues quantified expression of the androgen receptor (AR) in biopsy tissue taken from 354 women with benign breast disease, 78 of whom were later diagnosed with breast cancer. Although AR levels have been linked to outcomes in women who already have breast tumors, the study authors found no such association between AR expression and disease risk while women were still cancer-free. There was also little evidence for an interaction between AR levels and those of the estrogen receptor or the proliferation marker Ki67 on the incidence of breast cancer. However, the researchers caution, larger studies are needed to verify the results.
Introduction
Sex steroid hormones play a critical role in the development and progression of breast cancers.1,2 While estrogen signaling has long been hypothesized to be a promoter of breast carcinogenesis,3,4 the effects of androgen signaling are unclear. Circulating androgens are associated with breast cancer risk among postmenopausal women, conferring roughly twofold higher risk comparing highest-to-lowest quintiles.5 Some of this apparent association may be due to the conversion of androgens to estrogens, leading to activation of estrogen signaling pathways in the breast. When circulating androgens are adjusted for circulating estradiol, these associations attenuate, but not entirely to unity, suggesting a potential effect of androgens on the breast, independent of their conversion to estrogens.5–7 Circulating hormones show moderate correlations with hormone levels in the breast, indicating that these may be indirect markers of the hormonal milieu in the breast.8–12
The androgen receptor (AR) is expressed in 60–80% of breast cancers and is an emerging prognostic and predictive marker, as well as potential therapeutic target, in breast cancer.13,14 AR is more commonly co-expressed in estrogen receptor-positive (ER+) breast cancers (70–90%), though is still expressed in 40% of ER− cancers.15–17 Evidence from in vitro models suggests that the effects of AR signaling in breast cancers may depend on tumor ER expression.18,19 AR signaling promotes tumor growth and inhibits apoptosis in ER− breast cancers,20 while antagonizing ER signaling pathways in ER+ breast cancers.21 Epidemiologic studies have consistently found that AR expression is associated with improved breast cancer prognosis for women with ER+ breast cancer, in concordance with in vitro evidence.22 However, results from epidemiologic studies among women with ER− breast cancer are quite mixed.22 Although AR is expressed in normal breast epithelium, to date, AR expression and its potential interaction with ER expression have not been evaluated in normal breast tissue with respect to breast cancer risk. Few markers in normal tissue have been identified that predict future breast cancer risk.23–26 Of these, Ki67, a nuclear protein present in active phases of the cell cycle,27 has been most consistently linked to breast cancer risk.28–30 This association may be limited to women with low ER expression.29
In this analysis, we evaluated AR expression in normal breast tissue as a potential predictor of subsequent breast cancer risk in a nested case–control study within the Nurses’ Health Study and Nurses’ Health Study II cohorts and whether this association differed by ER co-expression. We further assessed potential effect modification by Ki67, given the heterogeneity previously observed for the Ki67-breast cancer association by ER expression. Finally, we explored the relationships between established breast cancer risk factors and AR expression in normal tissue.
Results
The median AR expression was 20% (IQR: 10%–43%) in this population of 354 women (78 cases and 276 controls). The Spearman correlations were 0.44 between AR and ER expression and −0.09 between AR and Ki67 expression. Age-standardized distributions of the study matching factors and BBD lesion type are shown in Table 1. The time elapsed between BBD biopsy and the index date was suggestively longer for controls. Cases were more likely to have proliferative BBD lesions with atypia than controls.
Table 1.
Age-standardized distributions of study matching factors and BBD lesion type among 78 breast cancer cases and 276 controls
| Variable | Breast cancer cases (n = 78) |
Controls (n = 276) |
|---|---|---|
| Age at cancer diagnosis, mean (SD) | 53.9 (8.7) | — |
| Year of BBD biopsy, % | ||
| Before 1980 | 41 | 40 |
| 1980–1989 | 48 | 46 |
| After 1989 | 11 | 15 |
| Time from BBD biopsy to index date, % | ||
| 0.5–4.9 years | 26 | 48 |
| 5.0–9.9 years | 39 | 24 |
| 10.0–14.9 years | 20 | 20 |
| 15.0+ years | 15 | 8 |
| BBD lesion type, % | ||
| Non-proliferative | 26 | 29 |
| Proliferative without atypia | 48 | 57 |
| Atypical hyperplasia | 26 | 15 |
In logistic regression models adjusting for the matching factors, AR expression in normal breast tissue was not associated with subsequent breast cancer risk (Table 2). After further adjustment for BBD lesion type, women with >30% AR expression had a non-significant 10% decrease in breast cancer risk compared to women with <10% expression (OR = 0.9, 95% CI = 0.4–1.8, p trend = 0.68). Similarly, a 10% increase in AR expression was not associated with breast cancer risk (OR = 1.0, 95% CI = 0.9–1.1) in the fully adjusted model.
Table 2.
Odds ratios (95% confidence interval) of developing breast cancer by tertile and per each 10% increase in AR expression in normal breast tissue
| Tertile 1 (≤10%) |
Tertile 2 (11–30%) |
Tertile 3 (>30%) |
P trend | 10% Increase | |
|---|---|---|---|---|---|
| Cases/controls | 19/63 | 31/108 | 28/105 | 78/276 | |
| Model 1 | Ref | 1.0 (0.5–1.9) | 1.0 (0.5–2.0) | 0.96 | 1.0 (0.9–1.1) |
| Model 2 | Ref | 1.0 (0.5–1.9) | 0.9 (0.4–1.8) | 0.68 | 1.0 (0.9–1.1) |
Model 1: Adjusting for age at breast cancer diagnosis/index date (<45, 45–54, and 55+), year of the BBD diagnosis (before 1980, 1980–1989, 1990 or later), and years elapsed between BBD diagnosis and breast cancer diagnosis/index date (0.5–4.9, 5–9.9, 10–14.9, and 15.0+)
Model 2: Adjusted for covariates in Model 1 + BBD lesion type (non-proliferative, proliferative without atypia, and atypical hyperplasia)
Among the 47 cases and 127 controls with measured AR and ER expression, there was no significant heterogeneity of the association between AR expression and the incidence of breast cancer by co-expression of ER in normal tissue (p heterogeneity = 0.21) (Fig. 1). Compared to women with low AR/low ER expression, women with high AR/high ER expression had a non-significant 60% lower risk of breast cancer (OR = 0.4, 95% CI = 0.1–1.2). Likewise, there was suggestive non-significant lower risk for women with high AR/low ER expression (OR = 0.7, 95% CI = 0.3–1.6), and higher risk for women with low AR/high ER expression (OR = 1.8, 95% CI = 0.4–7.8).
Fig. 1.
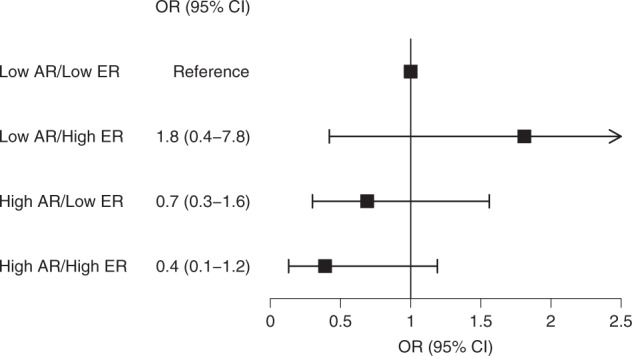
Odds ratios (95% confidence interval) of developing breast cancer by cross-classified AR and ER expression in normal breast TDLUs. ORs are estimated from unconditional logistic regression models among 47 cases and 127 controls and are adjusted for age at cancer diagnosis/index date, year of BBD biopsy, time between BBD diagnosis and breast cancer diagnosis/index date, and BBD lesion type. AR and ER are dichotomized at their median levels (20% for AR and 10% for ER). P value for test of heterogeneity is 0.21
Likewise, there was no significant effect modification by Ki67 expression (p heterogeneity = 0.75) (Fig. 2) among the 57 cases and 195 controls with measured AR and Ki67 expression. Women with Ki67 expression above the median had suggestively higher risk of breast cancer, irrespective of AR expression (low AR/high Ki67: OR = 1.5, 95% CI = 0.6–3.9; high AR/high Ki67: OR = 1.2, 95% CI = 0.5–3.1), relative to women with low AR and low Ki67 expression. High AR and low Ki67 expression was not associated with breast cancer risk, in comparison to low AR and low Ki67 expression (OR = 1.0, 95% CI = 0.4–2.5).
Fig. 2.
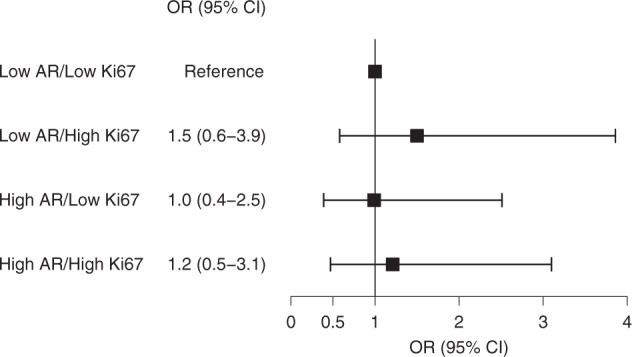
Odds ratios (95% confidence interval) of developing breast cancer by cross-classified AR and Ki67 expression in normal breast TDLUs. ORs are estimated from unconditional logistic regression models among 57 cases and 195 controls and are adjusted for age at cancer diagnosis/index date, year of BBD biopsy, time between BBD diagnosis and breast cancer diagnosis/index date, and BBD lesion type. AR and Ki67 are dichotomized at their median levels (20% for AR and 4% for Ki67). P value for test of heterogeneity is 0.75
Exploratory analyses regarding the relationship between breast cancer risk factors and AR expression in normal tissue yielded few apparent associations (Table 3). AR expression non-significantly increased with age. Mean AR expression in normal tissue was higher in women with atypical hyperplastic BBD lesions (mean 22.1 [95% CI = 14.3–34.3]) compared to women with proliferative lesions without atypia (mean 15.2 [95% CI = 12.2–18.8]) or women with non-proliferative lesions (mean 13.4 [95% CI = 9.9–18.1]), though these differences did not achieve statistical significance (p value = 0.18 from age-adjusted ANCOVA). No other notable associations were observed with breast cancer risk factors.
Table 3.
Breast cancer risk factors at time of BBD biopsy in relation to age-adjusted mean AR expression (95% confidence interval) in normal TDLUs among 276 controls
| n | Mean AR expression (95% CI) | P -valuea | |
|---|---|---|---|
| Age at BBD biopsy (yr.)b | 0.15 | ||
| <40 | 62 | 12.7 (9.0–17.8) | |
| 40–50 | 147 | 15.6 (12.5–19.4) | |
| >50 | 67 | 18.1 (13.0–25.1) | |
| BBD lesion type | 0.18 | ||
| Non-proliferative | 82 | 13.4 (9.9–18.1) | |
| Proliferative without atypia | 155 | 15.2 (12.2–18.8) | |
| Atypical hyperplasia | 39 | 22.1 (14.3–34.3) | |
| Age at first birth | 0.51 | ||
| Nulliparous | 12 | 15.8 (7.3–34.0) | |
| <25 years | 147 | 16.0 (12.9–20.0) | |
| 25–29 years | 91 | 14.8 (11.2–19.6) | |
| 30+ years | 13 | 8.8 (4.2–18.5) | |
| Age at menarche (yr.) | 0.33 | ||
| <12 | 56 | 13.9 (9.7–19.9) | |
| 12 | 79 | 15.9 (11.8–21.5) | |
| 13 | 80 | 13.9 (10.3–18.7) | |
| 14+ | 59 | 19.3 (13.6–27.3) | |
| Age at menopause (yr.) | 0.82 | ||
| Premenopausal | 122 | 17.7 (11.3–19.1) | |
| <50 | 81 | 16.8 (12.3–23.0) | |
| 50+ | 59 | 16.2 (11.3–23.2) | |
| Menopausal hormone therapy usec | 0.74 | ||
| Ever | 71 | 17.5 (12.6–24.3) | |
| Never | 70 | 16.2 (11.6–22.5) | |
| Oral contraceptive use | 0.18 | ||
| Ever | 131 | 14.0 (11.1–17.8) | |
| Never | 140 | 17.6 (14.0–22.1) | |
| BMI (kg/m2) at BBD biopsy | 0.53 | ||
| <25.0 | 179 | 16.0 (13.1–19.5) | |
| 25.0–29.9 | 57 | 15.3 (10.7–21.9) | |
| 30.0+ | 37 | 13.7 (8.8–21.3) | |
| BMI (kg/m2) at age 18 | 0.51 | ||
| <19.0 | 58 | 11.7 (8.3–16.5) | |
| 19.0–24.9 | 160 | 18.3 (14.9–22.5) | |
| 25.0+ | 26 | 13.9 (8.3–23.3) | |
| Weight change since age 18 | 0.77 | ||
| Gain <2 kg | 46 | 14.9 (10.1–21.9) | |
| Gain 2–20 kg | 100 | 17.8 (13.7–23.2) | |
| Gain 20+ kg | 108 | 15.1 (11.8–19.5) | |
| Alcohol consumption (g/week) | 0.39 | ||
| None | 81 | 17.4 (13.0–23.4) | |
| 0.1–4.9 | 75 | 13.0 (9.5–17.6) | |
| 5.0–14.9 | 38 | 19.8 (12.9–30.3) | |
| 15.0+ | 21 | 19.3 (10.9–34.3) | |
| Family history of breast cancer | 0.19 | ||
| Yes | 44 | 19.7 (13.2–29.4) | |
| No | 232 | 14.7 (12.4–17.5) |
Analyses are restricted to individuals with non-missing data. AR expression was log-transformed for analysis of covariance
aP -values are from global test of heterogeneity or test for trend (age at BBD biopsy, age at menarche, BMI at BBD biopsy, BMI at age 18, weight change, and alcohol consumption)
bNot adjusted for age
cRestricted to postmenopausal women
Discussion
The androgen receptor is an emerging biomarker of interest in breast cancer. Prior studies have shown that AR may have utility as a predictive or prognostic marker, or may even be a viable therapeutic target for certain breast cancer subtypes.13,14 In a nested case–control study within the NHS and NHSII cohorts, we found no association between AR expression in normal TDLUs and the subsequent incidence of breast cancer.
We likewise found little evidence for an interaction between AR and ER expression in normal breast TDLUs with respect to the incidence of breast cancer. However, in vitro and population evidence support the presence of a biologic interaction between AR and ER signaling in breast cancers.18,19 In ER− breast cancers, AR signaling can stimulate tumor growth. In contrast, in ER+ breast cancers, AR may have anti-proliferative effects—antagonizing ER signaling through the occupancy of shared or distinct-binding sites at ER target genes or through competition for transcriptional co-regulators, abrogating their interaction with ER.18,19 Comparatively little is known about the interactions between AR and ER signaling in normal breast epithelium, though evidence from animal models suggests that the AR may still inhibit estrogen-stimulated proliferation in normal breast tissue.31–33 We observed that women with high AR and high ER expression had suggestively lower risk of breast cancer, though this did not achieve statistical significance. While there were few individuals with low AR and high ER, they experience apparent higher risk of breast cancer, though again this was not statistically significant. The AR is more commonly expressed in breast epithelial cells than the ER, and while co-localization of AR and ER can occur, more often AR is expressed without ER.21 ER infrequently co-localizes with Ki67 in normal breast tissue, though this does often occur in malignant tissue.34,35 Prior analyses in this case–control study indicated that women with high Ki67 and low ER expression in normal TDLUs experienced higher breast cancer risk.29 Our findings indicated no heterogeneity for the association between Ki67 expression and breast cancer risk with respect to AR expression.
Circulating androgens are a consistent risk factor for breast cancer among postmenopausal women. Additionally, androgen levels in plasma were shown to be correlated with several breast cancer risk factors including age, menopausal status, obesity, smoking, and alcohol consumption in a pooled analysis of 13 prospective studies.36 This analysis showed no link between other reproductive factors (such as age at menarche, age at first birth, and parity) and concentrations of circulating androgens. A prior analysis in the NHS found that positive associations between obesity and weight change and breast cancer risk, and the inverse association between physical activity and breast cancer risk, were generally stronger for the risk of AR− tumors.37 Age at first birth and oral contraceptive use were also found to be associated with the incidence of AR− breast cancer.38 In contrast, alcohol consumption was found to be associated with the incidence of AR+ tumors.39 Apart from a non-significant suggestive positive association with age, we found no relationships between these risk factors and AR expression levels in normal breast tissue. Prior studies have evaluated the associations between breast cancer risk factors and ER and progesterone receptor (PR) expression in normal tissue.26,40–42 These studies found age, adult BMI, and alcohol consumption to be positively associated with ER expression and an inverse association with breastfeeding among parous women. Age, height, adult BMI, and BMI at age 18 were correlated with higher PR expression. While these risk factors may affect hormone receptor signaling in normal tissue, we found no relationship between these variables and AR expression, suggesting that their effects may not be through AR signaling pathways.
This study benefits from a unique design that allowed for the evaluation of a hypothesis that AR signaling in normal tissue may contribute to carcinogenesis in the breast. Given the uniqueness and resources required of the design, however, the sample size is quite limited. This reduced the statistical power available, in particular to evaluate interactions between AR and ER and Ki67 expression. Notably, this sample size has been sufficient to observe significant associations between IGF1R, EZH2, and Ki67 and breast cancer risk within the same nested case–control study.23–25,29 The limited sample size also precludes adjustment for many variables, leaving the findings susceptible to possible residual confounding. Additionally, the success rate for acquiring tissue from the BBD biopsy was low; though the women for whom we successfully obtain or do not obtain tissue have similar risk factor profiles (Supplementary Table 1). Thus, there is lesser potential for a selection bias through this mechanism. Measurement error in the assessment of tissue markers could arise through the use of TMAs rather than whole tissue sections. However, the ICCs across cores indicated good reliability for AR and ER expression, and modest for Ki67, suggesting that the cores may sufficiently represent all normal breast TDLUs. Finally, there was an apparent association between type of BBD lesion and AR expression, suggesting potential field effects from the BBD lesion in the normal TDLUs included in the TMAs. Hence, our findings may only be applicable to women with BBD.
In conclusion, we found no association between AR expression in normal breast TDLUs and subsequent breast cancer risk, nor any evidence of effect heterogeneity by co-expression of ER or Ki67. Due to the limited sample size in our analysis, these associations should be further evaluated in other populations.
Methods
Study population
The Nurses’ Health Study (NHS) was established in 1976 with the enrollment of 121,700 US female registered nurses aged 30–55 years, while the Nurses’ Health Study II (NHSII) consists of 116,429 US female registered nurses aged 25–42 years at cohort baseline in 1989. Detailed descriptions of cohort procedures have been reported elsewhere.43 Briefly, cohort members completed baseline questionnaires that provided medical histories and extensive information about demographic, lifestyle, reproductive, and dietary risk factors for breast cancer. Cohort members have updated this information biennially through follow-up questionnaires. NHS and NHSII participants also report new diagnoses of breast cancer and fibrocystic or benign breast disease (BBD) in the biennial questionnaires. These diagnoses are confirmed via medical record review or verbal confirmation from the nurse herself. All study protocols were approved by the institutional review board at Brigham and Women’s Hospital (Boston, MA) and informed consent was obtained from all study participants.
A nested case–control study was constructed within the two cohorts, wherein cases were women who reported a diagnosis of breast cancer after cohort baseline (through 1998 for NHS and 1999 for NHSII) and had previously reported a BBD diagnosis (either prior to study entry or after study baseline). Controls were women with a diagnosis of BBD who did not subsequently develop breast cancer. Details of this case–control study have been described elsewhere.23,44 A median of 8 years (interquartile range [IQR] 5–12) elapsed between the BBD and breast cancer diagnoses for cases, and cases for which this time period was <6 months were excluded. Cases and controls were matched 1:4 on the age at breast cancer diagnosis (index date for controls), year of the BBD diagnosis, and years elapsed between BBD diagnosis and breast cancer diagnosis (index date).
BBD tissue acquisition and immunohistochemical assays
For the identified cases and controls, study investigators requested H&E slides and later formalin-fixed paraffin-embedded tissue from the BBD biopsy from the diagnosing hospital. Slides were obtained for 463 cases and 1853 controls, and then within this group BBD tissue blocks were obtained for 177 cases and 719 controls. Three hundred eighty-eight participants with the following BBD lesion types were eligible for inclusion in tissue microarrays (TMAs): apocrine metaplasia, non-apocrine cysts, usual ductal hyperplasia, atypical ductal hyperplasia, and atypical lobular hyperplasia. For each of these participants, breast pathologists selected three representative areas of tissue containing normal terminal ductal lobular units (TDLUs).45 These areas were cored (0.6 mm) and assembled into six TMAs. The TMAs were then sectioned and stained for AR protein expression (Dako M3562 antibody, 1:200) and four of six TMAs for ER protein expression (Neomarkers RM-9101-S antibody, 1:40). The stained TMAs were then reviewed by pathologists who estimated AR and ER expression as 0%, 1%, or in ordinal categories of 10% in the epithelial tissue in each core. The mean expression for AR and ER was then calculated across the three cores for each individual. The maximum expression and geometric mean across cores were also evaluated and yielded similar results (data not shown). Ki67 expression (Vector VP-RM04 antibody, 1:250) was scored using Definiens Tissue Studio (Munich, Germany), an automated imaging analysis software program, which produced a 0–100% continuous estimate of expression. Women with low cellularity (<100 detected nuclei) for Ki67 expression were excluded from the analysis. Intraclass correlations were 0.66 for AR, 0.69 for ER, and 0.36 for Ki67, indicating some heterogeneity in expression across cores within individuals. Thirty-four individuals did not have evaluable AR expression in any of the three cores, leaving to a final sample size of 354 individuals (78 cases and 276 controls). Characteristics of participants selected into the nested case–control study with and without evaluable AR expression in normal tissue are shown in the supplement.
Statistical analysis
AR expression was categorized into tertiles as defined by the distribution among the controls (0–10%, 11–30%, and >30%). As tissue from the BBD biopsy was not obtained from all members of case–control sets, unconditional logistic regression models adjusting for the study matching factors and type of BBD lesion were used to estimate odds ratios (OR) and 95% confidence intervals (95% CI) for the association between AR expression in normal breast tissue and subsequent breast cancer risk. Other established breast cancer risk factors were considered as potential confounders, but were not included in final models, given their weak associations with AR expression and the limited sample size. Tests for linear trends were performed by fitting the regression models with a linear covariate taking the median AR expression level of each tertile. To evaluate the potential interaction between AR and ER or Ki67 expression, four categories were created by dichotomizing each distribution at the median level among the controls (20% for AR, 10% for ER, and 4% for Ki67). The p value for the test of heterogeneity was then calculated using a likelihood ratio test for the AR-by-ER or AR-by-Ki67 product term. The associations between established breast cancer risk factors and AR expression (natural log-transformed) among controls were assessed using analysis of covariance (ANCOVA) adjusting for age at BBD biopsy. Nineteen controls (of 276) with 0% AR expression were reassigned to 1% (minimum detectable positive AR expression) for the ANCOVA analysis. A 0.05 level of significance was used for all statistical tests. All analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC). As applicable, the analyses performed and reported are adherent to the REMARK recommendations for tumor marker prognostic studies.46
Electronic supplementary material
Acknowledgements
We would like to thank the participants and staff of the Nurses’ Health Study and the Nurses’ Health Study II for their valuable contributions as well as the following state cancer registries for their help: AL, AZ, AR, CA, CO, CT, DE, FL, GA, ID, IL, IN, IA, KY, LA, ME, MD, MA, MI, NE, NH, NJ, NY, NC, ND, OH, OK, OR, PA, RI, SC, TN, TX, VA, WA, and WY. This work was supported by the National Cancer Institute at the National Institute of Health (P50CA168504, UM1CA186107, UM1CA176726, and P01CA87969). K.H.K. was supported through National Research Service Awards F31CA192462 and T32CA009001 by the National Cancer Institute. M.B. is supported by the Breast Cancer Research Foundation. The study sponsors had no role in the design of the study; the collection, analysis, and interpretation of the data; the writing of the manuscript; or the decision to submit the manuscript for publication. The authors assume full responsibility for the analyses and interpretation of these data.
Author contributions
K.H.K. designed and conducted the research, performed the statistical analyses, interpreted the results, and drafted the manuscript. R.M.T. and M.B. designed and supervised the research, and made substantial contributions to the statistical analysis, interpretation of results, and revisions to the manuscript. F.B., G.M.B., Y.J.H., A.H.B., and S.J.S. contributed to acquisition of tissue data, performed the immunohistochemical assays, and revised the manuscript. A.H., B.A.R., A.H.E., and S.E.H. made significant contributions to the statistical analysis and revision of the manuscript. All authors approved the final manuscript and agreed to be accountable for all aspects of the work.
Data availability
The data that support the findings of this study are available from the Nurses’ Health Studies, however they are not publicly available. Investigators interested in using the data can request access, and feasibility will be discussed at an investigators meeting. Limits are not placed on scientific questions or methods, and there is no requirement for co-authorship. Additional data sharing information and policy details can be accessed at http://www.nurseshealthstudy.org/researchers.
Competing interests
A.H.B. is the co-founder and CEO of PathAI, Inc. The remaining authors declare no competing interests.
Footnotes
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Supplementary information accompanies the paper on the npj Breast Cancer website (10.1038/s41523-018-0085-3).
References
- 1.Cuzick J, et al. Overview of the main outcomes in breast-cancer prevention trials. Lancet. 2003;361:296–300. doi: 10.1016/S0140-6736(03)12342-2. [DOI] [PubMed] [Google Scholar]
- 2.Early Breast Cancer Trialists’ Collaborative Group. Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet 365, 1687–1717 (2005). [DOI] [PubMed]
- 3.Pike MC, Krailo MD, Henderson BE, Casagrande JT, Hoel DG. ‘Hormonal’ risk factors, ‘breast tissue age’ and the age-incidence of breast cancer. Nature. 1983;303:767–770. doi: 10.1038/303767a0. [DOI] [PubMed] [Google Scholar]
- 4.Colditz GA, Rosner BA, Chen WY, Holmes MD, Hankinson SE. Risk factors for breast cancer according to estrogen and progesterone receptor status. J. Natl Cancer Inst. 2004;96:218–228. doi: 10.1093/jnci/djh025. [DOI] [PubMed] [Google Scholar]
- 5.Key T, Appleby P, Barnes I, Reeves G. Endogenous sex hormones and breast cancer in postmenopausal women: reanalysis of nine prospective studies. J. Natl Cancer Inst. 2002;94:606–616. doi: 10.1093/jnci/94.8.606. [DOI] [PubMed] [Google Scholar]
- 6.Missmer SA, Eliassen AH, Barbieri RL, Hankinson SE. Endogenous estrogen, androgen, and progesterone concentrations and breast cancer risk among postmenopausal women. J. Natl Cancer Inst. 2004;96:1856–1865. doi: 10.1093/jnci/djh336. [DOI] [PubMed] [Google Scholar]
- 7.Kaaks R, et al. Postmenopausal serum androgens, oestrogens and breast cancer risk: the European prospective investigation into cancer and nutrition. Endocr. Relat. Cancer. 2005;12:1071–1082. doi: 10.1677/erc.1.01038. [DOI] [PubMed] [Google Scholar]
- 8.Recchione C, et al. Testosterone, dihydrotestosterone and oestradiol levels in postmenopausal breast cancer tissues. J. Steroid Biochem. Mol. Biol. 1995;52:541–546. doi: 10.1016/0960-0760(95)00017-T. [DOI] [PubMed] [Google Scholar]
- 9.Mady EA, Ramadan EE, Ossman AA. Sex steroid hormones in serum and tissue of benign and malignant breast tumor patients. Dis. Markers. 2000;16:151–157. doi: 10.1155/2000/305940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Brignardello E, et al. Dehydroepiandrosterone concentration in breast cancer tissue is related to its plasma gradient across the mammary gland. Breast Cancer Res. Treat. 1995;33:171–177. doi: 10.1007/BF00682724. [DOI] [PubMed] [Google Scholar]
- 11.Falk RT, et al. Sex steroid hormone levels in breast adipose tissue and serum in postmenopausal women. Breast Cancer Res. Treat. 2012;131:287–294. doi: 10.1007/s10549-011-1734-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lonning PE, et al. Tissue estradiol is selectively elevated in receptor positive breast cancers while tumour estrone is reduced independent of receptor status. J. Steroid Biochem. Mol. Biol. 2009;117:31–41. doi: 10.1016/j.jsbmb.2009.06.005. [DOI] [PubMed] [Google Scholar]
- 13.Kono M, et al. Androgen receptor function and androgen receptor-targeted therapies in breast cancer: a review. JAMA Oncol. 2017;3:1266–1273. doi: 10.1001/jamaoncol.2016.4975. [DOI] [PubMed] [Google Scholar]
- 14.Majumder A, Singh M, Tyagi SC. Post-menopausal breast cancer: from estrogen to androgen receptor. Oncotarget. 2017;8:102739–102758. doi: 10.18632/oncotarget.22156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Gonzalez LO, et al. Androgen receptor expresion in breast cancer: relationship with clinicopathological characteristics of the tumors, prognosis, and expression of metalloproteases and their inhibitors. BMC Cancer. 2008;8:149. doi: 10.1186/1471-2407-8-149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Niemeier LA, Dabbs DJ, Beriwal S, Striebel JM, Bhargava R. Androgen receptor in breast cancer: expression in estrogen receptor-positive tumors and in estrogen receptor-negative tumors with apocrine differentiation. Mod. Pathol. 2010;23:205–212. doi: 10.1038/modpathol.2009.159. [DOI] [PubMed] [Google Scholar]
- 17.Collins LC, et al. Androgen receptor expression in breast cancer in relation to molecular phenotype: results from the Nurses’ Health Study. Mod. Pathol. 2011;24:924–931. doi: 10.1038/modpathol.2011.54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hickey TE, Robinson JL, Carroll JS, Tilley WD. Minireview: the androgen receptor in breast tissues: growth inhibitor, tumor suppressor, oncogene? Mol. Endocrinol. 2012;26:1252–1267. doi: 10.1210/me.2012-1107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lim E, Ni M, Hazra A, Tamimi R, Brown M. Elucidating the role of androgen receptor in breast cancer. Clin. Investig. 2012;2:1003–1011. doi: 10.4155/cli.12.88. [DOI] [Google Scholar]
- 20.Doane AS, et al. An estrogen receptor-negative breast cancer subset characterized by a hormonally regulated transcriptional program and response to androgen. Oncogene. 2006;25:3994–4008. doi: 10.1038/sj.onc.1209415. [DOI] [PubMed] [Google Scholar]
- 21.Peters AA, et al. Androgen receptor inhibits estrogen receptor-alpha activity and is prognostic in breast cancer. Cancer Res. 2009;69:6131–6140. doi: 10.1158/0008-5472.CAN-09-0452. [DOI] [PubMed] [Google Scholar]
- 22.Bozovic-Spasojevic I, et al. The prognostic role of androgen receptor in patients with early-stage breast cancer: a meta-analysis of clinical and gene expression data. Clin. Cancer Res. 2017;23:2702–2712. doi: 10.1158/1078-0432.CCR-16-0979. [DOI] [PubMed] [Google Scholar]
- 23.Tamimi RM, et al. Expression of IGF1R in normal breast tissue and subsequent risk of breast cancer. Breast Cancer Res. Treat. 2011;128:243–250. doi: 10.1007/s10549-010-1313-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Beca F, et al. EZH2 protein expression in normal breast epithelium and risk of breast cancer: results from the Nurses’ Health Studies. Breast Cancer Res. 2017;19:21. doi: 10.1186/s13058-017-0817-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Oh, H. et al. Expression of estrogen receptor, progesterone receptor, and Ki67 in normal breast tissue in relation to subsequent risk of breast cancer. NPJ Breast Cancer2, 10.1038/npjbcancer.2016.32 (2016). [DOI] [PMC free article] [PubMed]
- 26.Khan SA, Rogers MA, Khurana KK, Meguid MM, Numann PJ. Estrogen receptor expression in benign breast epithelium and breast cancer risk. J. Natl Cancer Inst. 1998;90:37–42. doi: 10.1093/jnci/90.1.37. [DOI] [PubMed] [Google Scholar]
- 27.van Dierendonck JH, Keijzer R, van de Velde CJ, Cornelisse CJ. Nuclear distribution of the Ki-67 antigen during the cell cycle: comparison with growth fraction in human breast cancer cells. Cancer Res. 1989;49:2999–3006. [PubMed] [Google Scholar]
- 28.Nassar A, et al. Ki-67 expression in sclerosing adenosis and adjacent normal breast terminal ductal lobular units: a nested case-control study from the Mayo Benign Breast Disease Cohort. Breast Cancer Res. Treat. 2015;151:89–97. doi: 10.1007/s10549-015-3370-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Huh SJ, et al. The proliferative activity of mammary epithelial cells in normal tissue predicts breast cancer risk in premenopausal women. Cancer Res. 2016;76:1926–1934. doi: 10.1158/0008-5472.CAN-15-1927. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Santisteban M, et al. Ki67: a time-varying biomarker of risk of breast cancer in atypical hyperplasia. Breast Cancer Res. Treat. 2010;121:431–437. doi: 10.1007/s10549-009-0534-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Walters KA, Simanainen U, Handelsman DJ. Molecular insights into androgen actions in male and female reproductive function from androgen receptor knockout models. Hum. Reprod. Update. 2010;16:543–558. doi: 10.1093/humupd/dmq003. [DOI] [PubMed] [Google Scholar]
- 32.Dimitrakakis C, et al. A physiologic role for testosterone in limiting estrogenic stimulation of the breast. Menopause. 2003;10:292–298. doi: 10.1097/01.GME.0000055522.67459.89. [DOI] [PubMed] [Google Scholar]
- 33.Peters AA, Ingman WV, Tilley WD, Butler LM. Differential effects of exogenous androgen and an androgen receptor antagonist in the peri- and postpubertal murine mammary gland. Endocrinology. 2011;152:3728–3737. doi: 10.1210/en.2011-1133. [DOI] [PubMed] [Google Scholar]
- 34.Clarke RB, Howell A, Potten CS, Anderson E. Dissociation between steroid receptor expression and cell proliferation in the human breast. Cancer Res. 1997;57:4987–4991. [PubMed] [Google Scholar]
- 35.Russo J, Ao X, Grill C, Russo IH. Pattern of distribution of cells positive for estrogen receptor alpha and progesterone receptor in relation to proliferating cells in the mammary gland. Breast Cancer Res. Treat. 1999;53:217–227. doi: 10.1023/A:1006186719322. [DOI] [PubMed] [Google Scholar]
- 36.Key TJ, et al. Circulating sex hormones and breast cancer risk factors in postmenopausal women: reanalysis of 13 studies. Br. J. Cancer. 2011;105:709–722. doi: 10.1038/bjc.2011.254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Zhang X, et al. Adult body size and physical activity in relation to risk of breast cancer according to tumor androgen receptor status. Cancer Epidemiol. Biomark. Prev. 2015;24:962–968. doi: 10.1158/1055-9965.EPI-14-1429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Elebro K, Butt S, Dorkhan M, Jernstrom H, Borgquist S. Age at first childbirth and oral contraceptive use are associated with risk of androgen receptor-negative breast cancer: the Malmo Diet and Cancer Cohort. Cancer Causes Control. 2014;25:945–957. doi: 10.1007/s10552-014-0394-2. [DOI] [PubMed] [Google Scholar]
- 39.Wang J, et al. Alcohol consumption and risk of breast cancer by tumor receptor expression. Horm. Cancer. 2015;6:237–246. doi: 10.1007/s12672-015-0235-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Oh H, et al. Breast cancer risk factors in relation to estrogen receptor, progesterone receptor, insulin-like growth factor-1 receptor, and Ki67 expression in normal breast tissue. NPJ Breast Cancer. 2017;3:39. doi: 10.1038/s41523-017-0041-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Ricketts D, et al. Estrogen and progesterone receptors in the normal female breast. Cancer Res. 1991;51:1817–1822. [PubMed] [Google Scholar]
- 42.Lawson JS, Field AS, Tran DD, Houssami N. Hormone replacement therapy use dramatically increases breast oestrogen receptor expression in obese postmenopausal women. Breast Cancer Res. 2001;3:342–345. doi: 10.1186/bcr318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Colditz GA, Manson JE, Hankinson SE. The Nurses’ Health Study: 20-year contribution to the understanding of health among women. J. Women’s Health. 1997;6:49–62. doi: 10.1089/jwh.1997.6.49. [DOI] [PubMed] [Google Scholar]
- 44.Collins LC, et al. The influence of family history on breast cancer risk in women with biopsy-confirmed benign breast disease: results from the Nurses’ Health Study. Cancer. 2006;107:1240–1247. doi: 10.1002/cncr.22136. [DOI] [PubMed] [Google Scholar]
- 45.Collins LC, et al. Potential role of tissue microarrays for the study of biomarker expression in benign breast disease and normal breast tissue. Appl. Immunohistochem. Mol. Morphol. 2009;17:438–441. doi: 10.1097/PAI.0b013e3181993d86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.McShane LM, et al. REporting recommendations for tumour MARKer prognostic studies (REMARK) Br. J. Cancer. 2005;93:387–391. doi: 10.1038/sj.bjc.6602678. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The data that support the findings of this study are available from the Nurses’ Health Studies, however they are not publicly available. Investigators interested in using the data can request access, and feasibility will be discussed at an investigators meeting. Limits are not placed on scientific questions or methods, and there is no requirement for co-authorship. Additional data sharing information and policy details can be accessed at http://www.nurseshealthstudy.org/researchers.