

Abstract
Background:
Research indicates social communicative behaviours develop atypically during the second year in Autism Spectrum Disorder (ASD; e.g., Jones, Gliga, Bedford, Charman & Johnson, 2014). The present study evaluated whether these behaviours also differed in the extent to which they were coordinated across modalities.
Aim:
To measure joint attention behaviours (e.g., gaze shifts, gestures), vocalisations, and their coordination among a cohort of infants with an older sibling with ASD (Heightened Risk; HR).
Methods & Procedures:
This prospective longitudinal study examined 50 HR infants at 14, 18 and 24 months. The Early Social Communication Scales (ESCS; Mundy et al., 2003)—a structured toy play task which assesses infant joint attention behaviour—was administered to infants at each age point in the home. Infants’ joint attention behaviours, vocalisations, and instances where they overlapped were coded from videos. At 36 months, 9 infants received an ASD diagnosis (HR-ASD), 15 had a significant language delay (HR-LD), and 26 were classified no diagnosis (HR-ND).
Outcomes & Results:
Findings revealed that HR-ASD infants produced fewer advanced joint attention behaviours, and their vocalisations were less frequent and less advanced than HR-LD and HR-ND infants. Notably, HR-ASD infants also coordinated these behaviours together less frequently than their HR peers.
Conclusions & Implications:
Differences in the coordination of early communicative behaviours may have negative cascading effects on social and language development for infants who develop ASD. Current intervention practices may be complemented by efforts to increase the coordinated quality of communicative behaviours.
Keywords: Autism Spectrum Disorder (ASD), gesture, language delay, outcome, preverbal
Autism Spectrum Disorder (ASD) is a neurodevelopmental disorder characterized by deficits in social communication and social interaction, as well as the presence of repetitive behaviours and restricted interests or activities (DSM-5; American Psychiatric Association, 2013). Although caregivers and researchers report features of ASD in the first years of life, reliable diagnosis is difficult before age 2 (e.g., Chawarska, Macari, Volkmar, Kim & Shic, 2014). As a result, researchers have studied a group of infants at heightened risk (HR) for an ASD diagnosis (viz., the younger siblings of older children with ASD); for HR infants, the recurrence rate is estimated at 18.7% (Ozonoff et al., 2011). Observing this population prospectively from infancy allows researchers to assess early development in infants who later develop ASD and identify potential early markers of the disorder (Goldberg et al., 2005; Yirmiya et al., 2006).
Delays in early communication are well documented in HR infants who are eventually diagnosed with ASD (see Jones, Gliga, Bedford, Charman & Johnson, 2014, for review). Additionally, in comparison to infants with no family history of ASD (Low Risk; LR), even HR infants who do not go on to receive an ASD diagnosis have an elevated likelihood of language delays (Cassel et al., 2007; Goldberg et al., 2005; Patten et al., 2014; Yirmiya et al., 2006). The present study was therefore designed to investigate two areas of communicative development—joint attention and vocalisation—in a sample of HR infants. These behaviours were measured longitudinally at 14, 18, and 24 months in three groups of HR infants: infants later diagnosed with ASD (HR-ASD), infants with eventual language delays (HR-LD), and infants without a diagnosis or language delay (No Diagnosis; HR-ND). Joint attention and vocalisation are especially important as they constitute raw materials for social communication during infancy (e.g., Bakeman & Adamson, 1984; Bruner, 1977; Gros-Louis, West, Goldstein & King, 2006). Indeed, joint attention and vocal development both predict later language ability (Charman et al., 2000; Morales et al., 2000; Murray et al., 2008) and serve as foundational targets for early intervention (e.g., Mundy & Crowson, 1997).
To date, the literature on HR infants has typically examined these early communicative behaviours in isolation. Yet these skills not only develop simultaneously during infancy, they are also frequently used in combination when infants interact with caregivers and peers (Harding & Golinkoff, 1979; Bakeman & Adamson, 1984). For example, an infant may look at a desired but out of reach object, shift gaze to a caregiver, and vocalise to attract the attention of the caregiver while simultaneously reaching to request the object. It has been suggested that this type of coordination makes these behaviours more salient to the caregiver, and therefore potentially more successful in eliciting social responses (e.g., Parladé & Iverson, 2015; Iverson & Wozniak, 2016). Given the dearth of research examining joint attention and vocalisation production simultaneously, the present study focused on the development and coordination of these behaviours in HR infants across the second year.
Joint attention and vocalisation in typical development
Joint attention—the shared, triadic attention of two social partners with an object—is a critical component of early communicative growth in neurotypical infants and plays a role in early language development (Bakeman & Adamson, 1984; Morales et al., 2000) and cognition (Morales et al., 2000; Mundy et al., 2007). By 6 months, infants follow the gaze of a caregiver to a new location (Murray et al., 2008). By 12 months they behave in a variety of ways to establish joint attention—for instance, they alternate gaze between a caregiver and objects, they reach to request objects, and they hold up attractive objects to show others (e.g., Carpenter, Nagell & Tomasello, 1998). These behaviours typically serve two functions: 1) they establish shared attention to an object or event with a social partner to indicate interest (e.g., making eye contact with an adult while holding a toy); and/or 2) they request the help of a social partner to achieve a desired goal (e.g., handing a closed container to an adult to open it).
While the literature on joint attention has focused on nonverbal behaviours such as eye gaze and gesture, infants also vocalise during social interactions. At the same time that joint attention behaviours emerge and develop there are simultaneous changes in vocal development. Early vocalisations consist of vowel-only sounds (e.g., [ah]), but by 6 months infants begin to produce syllabic vocalisations, which contain consonant-vowel units (e.g., [bababa]; Oller, Eilers, Neal, & Schwartz, 1999; Paul, Fuerst, Ramsay, Chawarska, & Klin, 2011). Throughout the first year these increase in frequency and complexity (e.g., Oller et al., 1999). These vocalisations are an important milestone as they serve as a prerequisite for later word production (e.g., Oller et al., 1999).
As infants develop, they begin to combine multiple communicative behaviours, such as pairing vocalisations with gestures (Bates, Benigni, Bretherton, Camaioni & Volterra, 1979; Bruner, 1977). Pairing vocalisations with other nonverbal communicative behaviours may be particularly important for communication development because vocalisations are influential in directing caregivers’ attention and responses. For example, a caregiver who is across the room is more likely to respond to an infant’s reach/request gesture paired with a vocalisation than to the same gesture alone (Goldstein, King, & West, 2003; Gros-Louis et al., 2006; Harding & Golinkoff, 1979; Hsu & Fogel, 2001). Studies suggest that caregivers frequently respond contingently to their infants’ vocalisations (e.g., Gros-Louis et al., 2006; but see Fagan & Doveikis, 2017) and provide richer responses to syllabic vocalisations (e.g., by imitating or expanding on the infants’ vocalisation) relative to less advanced vowel-only vocalisations (Gros-Louis et al., 2006). Considering that extensive research has documented a robust relation between joint attention behaviours and later language ability (e.g., Charman et al., 2000; Morales et al., 2000; Murray et al., 2008), it is surprising that there has been relatively little work describing the role of vocalisations in enhancing infants’ joint attention behaviour (Winder, Wozniak, Parladé, & Iverson, 2013). Understanding the coordination of these behaviours during social interactions may be useful in understanding communicative development in both typical and atypical development.
Joint attention and vocalisation in HR infants and toddlers with ASD
Infants with ASD demonstrate differences in the frequency and content of their joint attention behaviours compared to neurotypical infants (Charman, 1998; Goldberg et al. 2005; Shumway & Wetherby, 2009; Toth, Munson, Meltzoff, & Dawson, 2006). In addition, there is evidence that HR infants as a group—including those who do not receive an ASD diagnosis— show differences in joint attention behaviours relative to LR samples. On average, HR infants without ASD produce joint attention behaviours at rates more similar to those of children with ASD than to those of LR peers (Cassel et al., 2007; Goldberg et al., 2005; Yirmiya et al., 2006). For example, Goldberg et al. (2005) used the Early Social Communication Scales (ESCS; Mundy et al., 2003)—a standardized assessment aimed at eliciting joint attention behaviours—to compare three groups of children: LR toddlers (mean age = 15.3 months), HR toddlers without ASD (mean age = 17.1 months), and young children with ASD (mean age = 29.9 months). There were no significant differences in joint attention behaviours between children with ASD and the HR toddlers without ASD. However, both groups produced significantly fewer joint attention behaviours than the LR toddlers.
Differences in pre-speech vocalisations and vocal development have also been described in studies of HR infants, and especially HR-ASD infants. For example, Paul et al. (2011) examined vocalisations from 6 to 12 months in HR and LR infants. Although HR infants did not differ from LR infants in overall frequency of vocalisations, there were notable differences in the quality and types of vocalisations observed. Specifically, HR infants produced more non-speech (e.g., growl, yell, squeal) and fewer syllabic vocalisations than their LR peers (see also Plumb & Wetherby, 2013; Schoen, Paul, & Chawarska, 2011). While the Paul et. al (2011) study did not have diagnostic outcomes for their sample, other research has demonstrated that infants with a later ASD diagnosis exhibit delays in the onset of babbling (i.e. syllabic vocalisations with repeated consonant-vowel units; e.g., [bababa], [mamama]) and lower rates of overall and syllabic vocalisation compared to neurotypical peers (Patten et al., 2014). In addition, the social function of vocalisations appears to differ in ASD: HR-ASD infants produce fewer vocalisations directed at social partners compared to their LR peers (Ozonoff et al., 2010). Although the current research has established differences between LR and HR infants as a group, and between ASD infants and neurotypical infants, none of these studies were able to compare vocal development among HR infants with and without language delays or ASD. Thus, the specificity of delays observed in vocal development among HR infants remains unclear.
Given the apparent differences in joint attention and vocalisations reported in studies that have considered these behaviours separately, it is unsurprising that HR infants with a later ASD diagnosis also coordinate them less frequently (Parladé & Iverson, 2015; Winder et al., 2013). In a longitudinal study comparing LR, HR-ASD, HR-LD, and HR-ND infants, Parladé & Iverson (2015) examined the development of gesture+vocalisation coordinations (i.e., infant produces gesture while simultaneously vocalising) and found that while both HR-LD and HR-ASD infants exhibited initial delays in production of these coordinations, only HR-ASD infants showed significantly slowed growth over time compared to all other groups. Indeed, the slope of growth for the HR-ASD group was close to zero, indicating that although their HR peers were increasingly coordinating gestures with vocalisations, HR-ASD infants were not.
This pattern is striking, and further research is needed to determine whether it is robust. Differences in isolated joint attention behaviours and isolated vocalisations appear to be characteristic of HR infants as a group. Differences in their coordination, however, appear to be specific to infants with ASD. Identifying qualities of communicative development that are unique to ASD has valuable theoretical and clinical implications—particularly in light of the substantial variability in communication that characterizes HR infants as a group. The present study set out to extend this work by assessing the coordination of joint attention and vocalisations longitudinally in three groups of HR infants who varied in developmental outcome at age 3 years.
The Present Study
The aim of the present study was to examine the development of: a) frequency and quality of joint attention behaviours; b) frequency and quality of vocalisations; and c) coordination of joint attention behaviours with vocalisations in HR-ASD, HR-LD and HR-ND infants. These behaviours were assessed longitudinally at 14, 18, and 24 months of age during administration of the ESCS. By focusing on HR infants, we can examine individual variability in the behaviours under consideration in a population with a variety of developmental outcomes during a time period before many children receive a diagnosis.
Method
Participants
Fifty (30 males) full biological, later born infant siblings of children with a confirmed diagnosis of ASD participated in the present study. Participants were recruited through a university Autism Research Program and through flyers, professional referrals, and word of mouth. Prior to enrollment, older siblings were administered the Autism Diagnostic Observation Schedule-Generic (ADOS-G; Lord et al., 2000) by a trained clinician. Infants were eligible to participate in the study only if their older sibling scored above the Autism cutoff on the ADOS-G and met DSM-IV criteria for Autistic Disorder. Parents signed informed consents prior to participation; the research protocol was approved by the University Institutional Review Board. All infants were from full-term, uncomplicated pregnancies and from monolingual English-speaking families. Forty-three infants were Caucasian, four were Hispanic, two were Asian American and one infant was African American.
Outcome Classification
At 36 months, all infants were administered the ADOS-G by an experienced clinician. The ADOS-G reliably differentiates children with ASD from children who might have other developmental delays or no ASD diagnosis (Lord et al., 2000). Diagnoses were made based on administration of the ADOS, DSM-IV-TR criteria, and clinical best estimate. Clinicians were formally trained on the administration of the ADOS and met official research reliability criteria. They were naïve to all prior study data. Based on these criteria, 9 infants (6 males) were classified as HR-ASD.
HR infants were classified as language delayed (HR-LD) if they did not receive a diagnosis of ASD and either of the following criteria were met (Iverson et al., 2018; Parladé & Iverson, 2015; West, Leezenbaum, Northrup, & Iverson, in press): a) standardized scores on the MacArthur-Bates Communicative Development Inventory, Words and Sentences (CDI-II; Fenson et al., 1993) or CDI-III at or below the 10th percentile at more than one time point between 18 and 36 months (e.g.,, Ellis Weismer & Evans, 2002; Heilmann, Ellis Weismer, Evans, & Hollar, 2005); or b) standardized score on the CDI-III at or below the 10th percentile and a standardized score on the Receptive and/or Expressive Language subscales of Mullen Scale of Early Learning (MSEL; Mullen, 1995) equal to or greater than 1.5 standard deviations below the mean at 36 months (e.g.,, Landa & Garrett-Mayer, 2006; Ozonoff et al., 2010). Based on these criteria, 15 infants (9 males) were classified as HR-LD. The remaining 26 infants (15 males) did not meet the criteria for ASD or LD and were classified as having no diagnosis (HR-ND).
Demographic information for infants in each outcome group are presented in Table 2. All demographic information was collected at the first visit. As can be seen in the table, the majority of families were Caucasian and held college or graduate degrees. Mann-Whitney U tests revealed that mothers’ years of education did not differ statistically between the outcome groups, nor did mean ages of mothers or fathers (see Table 2). Although information on family income was unavailable, parental occupations were identified in order to provide a general index of socio-economic status. Over half of the mothers in the study (56%) did not work outside the home, so paternal occupations were used to calculate Nakao-Treas occupational prestige scores, a measure of occupational social standing that correlates highly with socio-economic factors (Nakao & Treas, 1994). For one LD family it was impossible to identify the father’s occupation with enough precision to assign a prestige score. Mann-Whitney U tests with occupational prestige data from the remaining families indicated no statistically significant difference between groups.
Table 2.
Demographic information for the three outcome groups.
| HR-ND | HR-LD | HR-ASD | |
|---|---|---|---|
| Gender | |||
| Male | 11 (42.3%) | 6 (40%) | 6 (66%) |
| Female | 15 (57.7%) | 9 (60%) | 3 (33%) |
| Racial/ethnic minority | 0 (0%) | 4 (26.7%) | 3 (33%) |
| Speech Interventiona | 1 (3.8%) | 8 (53.3%) | 6 (66%) |
| Mean age | |||
| Mother | 33.65 (3.14) | 34.73 (3.36) | 31 (4.5) |
| Father | 36.57 (5.4) | 37.87 (3.91) | 34.78 (4.82) |
| Maternal Education | |||
| Postgraduate | 12 (46.2%) | 6(40%) | 2 (22.2%) |
| College | 13 (50%) | 8 (53.3%) | 3 (33 %) |
| High School | 1 (3.8%) | 1 (6.7%) | 4 (44.4%) |
| Paternal Education | |||
| Postgraduate | 6 (23.1%) | 6 (40%) | 4 (44.4%) |
| College | 19 (73.1%) | 8 (53.3%) | 3 (33%) |
| High School | 1 (22.2%) | 1 (22.2%) | 2 (22.2%) |
| Mean Paternal Occupational Prestige | 53.8 (14.95) | 52.02 (14.52) | 53.38 (17.32) |
Data reflect the numbers of infants who were receiving speech-language services in each outcome group.
Procedure
Infants were visited at home on a monthly basis between 5 and 14 months, with follow-up visits at 18, 24, and 36 months. At the 14-, 18-, and 24-month visits, infants were administered the Early Social Communication Scales (ESCS; Mundy et al., 2003). The ESCS is a 15- to 20-minute experimenter-administered semi-structured toy play interaction that is widely used to assess nonverbal joint attention behaviours at these ages. Administration occurred at a table with the child sitting across from the experimenter. The same toys were presented at each visit and included wind-up toys, a puppet, a book, posters, and social toys (e.g., sunglasses, a bowl and spoon, a comb and a hat). Trained examiners administered the ESCS in accordance with standard procedures outlined in the abridged ESCS manual (Mundy et al., 2003). In addition, because the goal of this research was to investigate the coordination of non-verbal joint attention behaviours as elicited in the ESCS and infant vocalisation, infants wore a wireless microphone housed in a vest worn over their clothing, allowing for high quality recording of vocalisations.
Coding
Coding for this study was completed by members of the research team naive to group membership. Two different teams completed the ESCS coding and the vocalisation coding.
ESCS.
ESCS coding followed standard procedures described in the ESCS manual (Mundy et al., 2003). The ESCS is a reliable and valid measure of early social communication development (e.g., Mundy et al., 1988, 1994, 1995) that focuses on two types of spontaneous joint attention behaviours: Initiating Behavioural Requests (IBR) and Initiating Joint Attention (IJA). IBR behaviours (e.g., extending an arm toward a toy) are those that request a social partner to do something (e.g., hand the toy to the child). IJA behaviours are those that function to establish shared visual attention with the experimenter to communicate interest in an object or activity; either in mutual gaze or shared gaze toward an object (e.g., holding up a toy to show the experimenter).
IJA and IBR behaviours were further classified as low or high following the guidelines of the manual (Mundy et al., 2003). Low behaviours (e.g., alternating gaze between an object and the experimenter) are those that typically emerge earlier in development (Bakeman & Adamson, 1984; Seibert, Hogan & Mundy, 1984; Mundy, Sigman & Kasari, 1994). High behaviours reflect more developmentally advanced actions (e.g., pointing to a distal object while making eye contact with the experimenter). All observable behaviours were coded from videotaped ESCS administrations with no minimum duration necessary. High and low behaviours were coded as distinct behaviours, and infants did not need to perform a low behaviour in order to get credit for a high behaviour. Further description of these categories can be found in Table 1.
Table 1.
Description of Early Social Communication Scales codes.
| Joint attention category | Base behaviour | Description |
|---|---|---|
| IJA (low) | eye contact | child makes spontaneous eye contact with tester while the child is holding or touching a toy |
| alternate gaze | child alternates gaze between an activated mechanical toy and the tester’s eyes | |
| IJA (high) | point | child spontaneously points with index finger toward an activated mechanical toy, a picture in book, or distal object |
| show | child raises a toy upward to show tester; does not give toy to tester | |
| IBR (low) | eye contact | child makes spontaneous eye contact with tester when the object is out of reach |
| reach | child extends arm toward an out of reach toy | |
| appeal | child combines a reach and eye contact with the tester | |
| IBR (high) | give | child extends an object toward the tester and gives up the toy |
| point | child spontaneously points to an inactive toy |
Note. IJA = Initiating Joint Attention; IBR = Initiating Behavioural Request. High and low behaviours can be done with or without eye contact. Children did not need to produce a low behaviour skill to receive credit for high behaviour.
In this study inter-rater reliability was assessed via intra-class correlation coefficients (ICCs) computed using the raw total counts between raters on 15% (n=22) of the videos. Agreement was .99 for low IJA, .98 for high IJA behaviours, .96 for low IBR, and 1.00 for high IBR.
Vocalisations.
All vocalisations (excluding sneezing, coughing, breathing, laughing, and other vegetative noises) produced by infants during the ESCS administration were identified and coded. Separate vocalisations were coded if there was at least a 1 second pause or an audible breath between vocalisations. All non-word vocalisations were categorised according to whether or not they contained a consonant sound. Vocalisations that did not contain a consonant sound (e.g., [aaaaa], [oooooo]) were coded as vowel only. Those that contained a consonant sound (e.g., [maba], [dadada]) were categorised as syllabic. Infants were credited with producing a word if they produced either an English word (e.g., “ball”), or a vocalisation that was consistently used to refer to a specific object (e.g., [baba] for “ball”). Inter-rater reliability was assessed via intra-class correlation coefficients (ICCs) computed using raw total counts of each type of vocalisation on 20% (n=30) of the videos. Reliability was .93 for vowel-only vocalisations, .91 for syllabic vocalisations, and .98 for words.
Coordinations.
Coordination of joint attention behaviour and vocalisation was identified any time there was an overlap in time between a joint attention behaviour and a vocalisation. If an infant vocalised at any point during a joint attention behaviour, it was considered to be a coordination. Coordinations were identified separately for IJA and IBR behaviours.
Results
This study was designed to examine the development of joint attention behaviours, vocalisations, and their coordination in three groups of HR infants with varying developmental outcomes. Although there were no significant differences in ESCS observation lengths as a function of outcome group, F(2, 46) = 1.820, p = .173; MND = 16.95, SDND = 2.98, MLD = 16.94, SDLD = 2.53, MASD = 15.39, SDASD = 3.17, frequencies for each variable were converted to rates per 10 minutes in order to control for slight differences in duration. Furthermore, initial examination of distributions indicated that all variables, which possessed an artificial lower bound at 0, had a positive skew and were therefore logarithmically or square root transformed prior to conducting statistical analyses. Mann-Whitney U tests did not reveal any significant gender differences in any of the variables considered. Therefore, all analyses were conducted with data collapsed across males and females.
Joint attention behaviours
Rates per 10 minutes of the four joint attention behaviours (low IBR, high IBR, low IJA, high IJA) were calculated for each infant; descriptive statistics are presented in Table 3. In order to test for group differences in these behaviours over time, 3 × 3 repeated measures ANOVAs with Age (14, 18, 24 months) as a within-subjects factor and Outcome (HR-ND, HR-LD, HR-ASD) as a between-subjects factor were computed separately for each behaviour. As can be seen in Table 3, HR-ASD infants tended to produce low IBR, high IBR, and low IJA behaviours less frequently than their HR-ND and HR-LD peers. However, this trend did not achieve significance: there were no main effects of Age or Outcome for these three variables. The interaction terms were also non-significant.
Table 3.
Production of joint attention behaviours by outcome group at 14, 18, and 24 months.
| HR-ND (n=26) |
HR-LD (n=15) |
HR-ASD (n=9) |
|||||
|---|---|---|---|---|---|---|---|
| Variable | Age | M (SD) | % of Infants |
M (SD) | % of Infants |
M (SD) | % of Infants |
| Low IBR | 14 | 6.79 (5.16) | 100% | 6.87 (7.41) | 100% | 5.79 (3.04) | 100% |
| 18 | 7.83 (4.89) | 100% | 7.67 (4.46) | 100% | 5.09 (2.72) | 100% | |
| 24 | 6.25 (3.07) | 100% | 6.75 (5.15) | 100% | 4.64 (4.44) | 100% | |
| High IBR | 14 | 7.30 (6.20) | 100% | 5.95 (3.94) | 100% | 8.54 (5.19) | 100% |
| 18 | 8.95 (6.10) | 96.2% | 7.14 (6.99) | 100% | 6.31 (3.99) | 100% | |
| 24 | 9.26 (5.76) | 96.2% | 8.39 (6.60) | 100% | 6.73 (3.53) | 100% | |
| Low IJA | 14 | 8.25 (4.23) | 100% | 9.54 (5.81) | 100% | 9.83 (8.26) | 100% |
| 18 | 8.35 (6.00) | 92.3% | 8.65 (6.65) | 93.3% | 8.87 (5.38) | 100% | |
| 24 | 9.74 (4.88) | 100% | 9.94 (4.20) | 100% | 6.34 (5.28) | 100% | |
| High IJA | 14 | 2.76 (2.60) | 96.2% | 1.66 (2.73) | 73.3% | 0.46(0.64) | 44.4% |
| 18 | 1.49 (1.50) | 73.1% | 1.35 (1.38) | 80% | 0.29 (0.15) | 33% | |
| 24 | 1.85 (1.37) | 96.2% | 1.61 (1.52) | 66.6% | 0.06 (0.23) | 11.1% | |
Note. ND = No Delay; LD = Language Delay; ASD = Autism Spectrum Disorder; M = Mean; SD = Standard Deviation; # of infants = Percentage of infants who produced the behaviour
With regard to high IJA behaviours, however, a different pattern emerged. Results of the ANOVA revealed a significant overall effect of Outcome, F(2,47) = 14.430, p < .001, = 0.38. Follow up simple effects analyses using a Sidak adjustment indicated that the differences between the HR-ASD and HR-ND and the HR-ASD and HR-LD groups were both significant, p < .001, p = .001, indicating that the HR-ASD group produced fewer high IJA behaviours overall compared to their peers. Although there was also a tendency for the HR-LD group to produce high IJA behaviours less frequently than their HR-ND peers, this difference did not achieve statistical significance, p = .081.
As can also be seen in Table 3, the percentage of HR-ASD infants producing even a single high IJA behaviour was low at all three age points and decreased over time. This pattern was only apparent in the HR-ASD group. Two-tailed Fishers exact tests carried out at each age indicated that at 14 months the percentage of children producing any high IJA behaviours in the HR-ASD group did not differ significantly from that for the HR-LD group, p = .212, but did differ from the HR-ND group, p = .002. However, at 18 and 24 months the percentages of HR-ASD infants producing high IJA behaviours were significantly lower than those for both the HR-ND, p = 0.050, p < 0.001, and HR-LD groups, p = 0.036, p = 0.013.
Vocalisations
Next, we examined infant production of the three types of vocalisations (vowel-only, syllabic, words) over time by calculating rates per 10 minutes for each vocalisation type for individual infants. Descriptive statistics are presented in Table 4 for each vocalisation type, age, and outcome group; data are also plotted in Figure 1. To examine differences in the types of vocalisations produced across the three age points in the three outcome groups, a 3 (Vocalisation Type) × 3 (Age) × 3 (Outcome) repeated measures ANOVA was carried out on the data. Results revealed significant main effects of Outcome, F(2,47) = 6.23, p < 0.001, = 0.21, Vocalisation Type, F(2,94) = 101.175, p < .001, = 0.68, and Age, F(2,94) = 9.522, p < .001, = 0.17, as well as a significant interaction between Vocalisation Type and Age, F(4,188) = 30.781, p < .001, = 0.40. However, these were qualified by a three-way interaction between Vocalisation Type, Age, and Outcome, F(8,188) = 8.613, p < .001, = 0.27, indicating that the relationship between infant age and vocal production varied between outcome groups.
Table 4.
Rates per 10 minutes of vocalisation production by outcome group at 14, 18, and 24 months.
| HR-ND (n=26) | HR-LD (n=15) | HR-ASD (n=9) | ||
|---|---|---|---|---|
| Vocalisation Type |
Age | Mean (SD) | Mean (SD) | Mean (SD) |
| Vowel Only | 14 | 19.08 (13.98) | 14.45 (12.00) | 4.47 (2.23) |
| 18 | 16.13 (11.71) | 11.09 (12.32) | 7.83 (7.28) | |
| 24 | 5.34 (6.98) | 8.56 (9.12) | 9.27 (8.75) | |
| Syllabic | 14 | 17.18 (14.31) | 16.19 (14.54) | 6.34 (6.19) |
| 18 | 21.67 (26.54) | 14.25 (14.88) | 5.77 (7.50) | |
| 24 | 15.62 (10.77) | 25.62 (19.57) | 11.62 (10.40) | |
| Word | 14 | 0.07 (0.25) | 0.00 (0.00) | 0.00 (0.00) |
| 18 | 4.13 (10.45) | 0.21 (0.38) | 0.71 (1.91) | |
| 24 | 23.44 (20.17) | 2.21 (9.09) | 2.12 (4.94) |
Note. ND = No Diagnosis; LD = Language Delay; ASD = Autism Spectrum Disorder; SD = Standard Deviation
Figure 1.
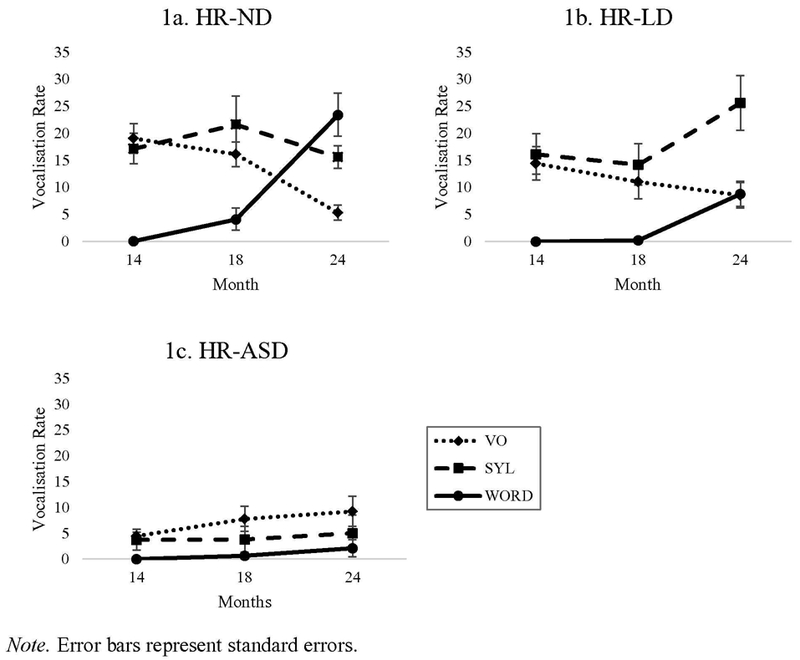
Rates per 10 minutes of vowel-only vocalisations, syllabic vocalisations, and words produced at 14, 18, and 24 months by (a) HR-ND, (b) HR-LD, and (c) HR-ASD infants.
To clarify the source of this three-way interaction, follow-up 3 (Age) × 3 (Vocalisation Type) repeated measures ANOVAs were calculated separately for each Outcome group. These revealed a significant Age by Vocalisation Type interaction both for HR-ND, F(4,100) = 71.71, p < .001, = 0.74, and HR-LD infants, F(4,56) = 10.61, p < .001, = 0.43, but, notably, not for the HR-ASD group, F(4,32) = 0.657, p = 0.63, = 0.08. Thus, while ND and LD infants showed significant change with age in the frequency with which they produced different types of vocalisations, the ASD group did not. As can be seen in Figure 1, among HR-ND infants, less complex vocalisations (i.e. vowel-only vocalisations) decreased with age, while words showed a sharp increase, particularly from 18 to 24 months. The HR-LD group showed a somewhat different pattern, with a smaller decrease in vowel-only vocalisations, but substantial increases in both syllabic vocalisations and word production between 18 and 24 months. In contrast, the HR-ASD group consistently produced vocalisations of all three types at low rates and with no age-related changes.
Coordination of joint attention behaviours and vocalisations
Finally, we examined how infants coordinated vocalisations with joint attention behaviours. For these analyses, we calculated the proportions of joint attention behaviours that were paired with a vocalisation by dividing the total number of coordinations by the total number of joint attention behaviours produced). These were calculated separately for IJA and IBR behaviours. Using proportions allowed us to control for differences in baseline frequencies of joint attention behaviours. Finally, low and high IJA behaviours were collapsed into a single category because many of the HR-ASD infants did not produce any high IJA behaviours and therefore did not have opportunities to combine them with vocalisations. Descriptive statistics for IJA + Vocalisation, low IBR + Vocalisation, and high IBR + Vocalisation are presented in Table 5. These data are also depicted in Figure 2.
Table 5.
Proportions of joint attention and vocalisation coordination by outcome group at 14, 18, and 24 months
| HR-ND (n=26) |
HR-LD (n=15) |
HR-ASD (n=9) |
||
|---|---|---|---|---|
| Age | M (SD) | M (SD) | M (SD) | |
| IJA+VOC | 14 | .33 (.26) | .32 (.34) | .06 (.08) |
| 18 | .58 (.92) | .26 (.39) | .15 (.27) | |
| 24 | .32 (.33) | .68 (.84) | .18 (.13) | |
| Low IBR+VOC |
14 | .38 (.26) | .30 (.27) | .19 (.14) |
| 18 | .45 (.24) | .35 (.26) | .24 (.25) | |
| 24 | .46 (.23) | .46 (.17) | .18 (.17) | |
| High IBR+VOC |
14 | .41 (.2) | .29 (.21) | .17 (.22) |
| 18 | .37 (.29) | .28 (.23) | .21 (.24) | |
| 24 | .49 (.24) | .47 (.24) | .22 (.26) |
Note. ND = No Diagnosis; LD = Language Delay; ASD = Autism Spectrum Disorder; M = Mean; SD = Standard Deviation
Figure 2.
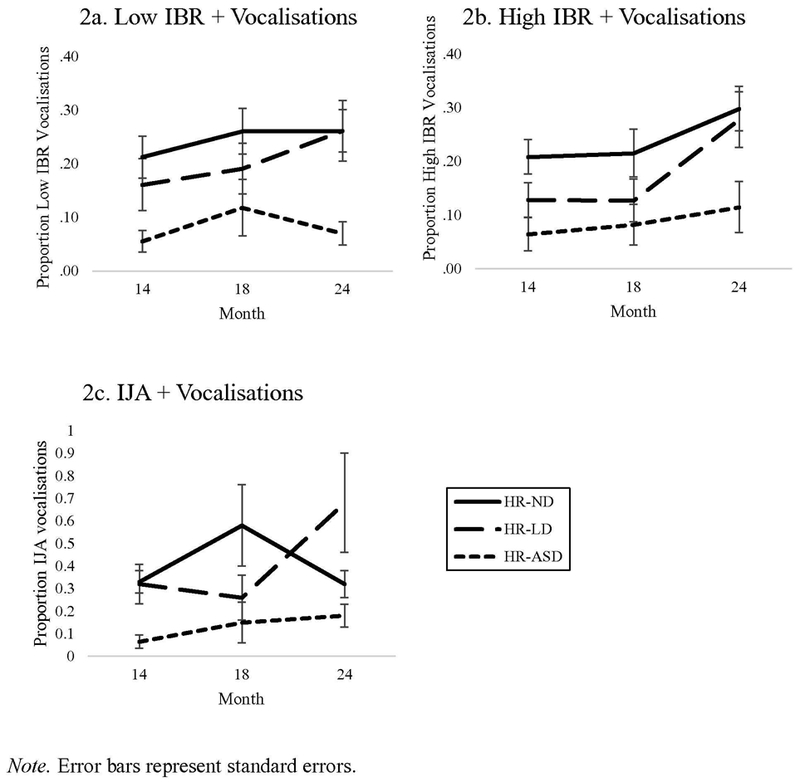
Proportions of (a) IJA+vocalisation, (b) Low IBR+Vocalisation, and (c) High IBR+Vocalisation coordinations produced at 14, 18, and 24 months by HR-ND, HR-LD, and HR-ASD infants.
For IJA + vocalisations, a 3 (Age) by 3 (Outcome) repeated measures ANOVA yielded a significant main effect only for Outcome, F(2,45) = 4.45, p = .017, = 0.17. Simple effects analyses further revealed that the HR-ASD group produced a significantly lower proportion of IJA+ vocalisation coordinations than the HR-ND, p = .008, and HR-LD groups, p = .015. The HR-ND group did not differ from the HR-LD group, p = .949.
A similar pattern was observed for low IBR + vocalisation coordinations. A 3 (Age) by 3 (Outcome) repeated measures ANOVA indicated a significant main effect of Outcome only, F(2,47) = 5.381, p = .008, = 0.19. Again, simple effects analyses indicated that a significantly lower proportion of low IBR + vocalisation coordinations were produced by the HR-ASD group than both the HR-ND, p=.002, and HR-LD groups, p=.033. The ND and LD groups did not differ from one another, p=.295.
Finally, a 3 (Age) by 3 (Outcome) repeated measures ANOVA was calculated for high IBR + vocalisation coordinations. This revealed a significant main effect of Age, F(2,88) = 3.428, p = .037, = 0.07, and Outcome, F(2,44) = 5.575, p = .007, = 0.20. Simple effects comparisons indicated that although there was no significant change in coordinations from 14 to 18 months, p = .878; there was a significant increase in coordinations between 18 and 24 months, p=.022. With regard to the effect of outcome, differences between the HR-ND and HR-LD groups were not significant, p = .150, but the ASD group differed significantly from the HR-ND group, p=.022, and marginally from the HR-LD group, p=.054. Note that there were no statistical differences in the numbers of IBR behaviours produced between the three outcome groups (see Table 3); thus this difference emerges only in the coordination of IBR behaviours with vocalisations.
Discussion
The present study examined the production of joint attention behaviours, vocalisations, and their coordination in infants at heightened risk for ASD. Consistent with previous findings, HR infants who later received an ASD diagnosis differed in production of joint attention behaviours and vocalisations compared to their HR peers (Charman, 1998; Goldberg et al. 2005; Shumway & Wetherby, 2009; Toth et al., 2006). Importantly, they were also less likely to coordinate these behaviours. Below we discuss these findings in turn, focusing on how these differences may impact infants’ social interactions and subsequent communicative development, and we suggest some potential clinical implications.
Differences in joint attention behaviours and vocalisation in ASD
Examination of infants’ joint attention behaviour indicated that for less advanced joint attention behaviours (e.g., reaching to request a desired object), there were no significant differences between HR-ASD infants and their peers. However, HR-ASD infants displayed far fewer advanced initiating joint attention behaviours (e.g., showing objects to others) than other HR infants. This is consistent with prior work, both using the ESCS—which actively elicits these behaviours—as well as naturalistic observation (Rozga et al., 2011; Watson, Crais, Baranek, Dykstra & Wilson, 2013).
Regarding vocalisations, both the HR-ND and HR-LD groups increased the frequency and complexity of their vocalisations over time (although not surprisingly, word production was attenuated for HR-LD infants relative to HR-ND infants). In contrast, the HR-ASD group consistently produced fewer vocalisations than their peers, and production did not increase over time. In addition, the vocalisations they produced were less complex, primarily vowel-only vocalisations. This aligns with previous studies that report disruptions in vocal development in ASD (Paul et al., 2011; Plumb & Wetherby, 2013; Schoen et al., 2011).
Considered together, these differences in joint attention and vocal behaviours are likely to impact infants’ social environments. Caregivers are sensitive to their infants’ communicative actions and are more responsive to advanced behaviours (e.g., syllabic vocalisations are more likely to receive a response than vowel-only vocalisations; Gros-Louis et al., 2006). A study by Leezenbaum et al. (2014) examined maternal responses to HR and LR infants’ gestures at 13 and 18 months. There were no differences in maternal responsiveness to infant gestures, but the types of gestures infants used differed between groups. Specifically, LR infants produced more point/show gestures, whereas HR infants tended to use reaches/gives. Analysis of mothers’ responses to these two gesture categories indicated that both groups of mothers were significantly more likely to translate the referent (i.e., provide its label) of point/show compared to give/request gestures. Thus, because HR infants produced significantly fewer show and point gestures that were most likely to elicit a translation response, they received fewer translations, which are precisely the type of response that is effective for promoting word learning.
Although these results were obtained using an experimenter-administered assessment, they highlight an important principle: differences in infant communication likely engender differences in caregiver communication—they interact through a social feedback loop. To illustrate, consider an infant who produces syllabic vocalisations. Adults respond to these conversationally, providing valuable verbal input. In a continuous cycle of contingency, these responses reinforce infants’ more developmentally advanced vocalisations (e.g., Martinsen & Smith, 1989) and assist them in acquiring new speech-like patterns (e.g., Goldstein & Schwade, 2008). The present findings suggest that this feedback loop unfolds differently in ASD. Because HR-ASD infants produce less advanced and less frequent joint attention behaviours and vocalisations, and because these differences may lead to a reduction in opportunities for high quality caregiver responses, the nature of the social-communicative input they receive likely differs from that directed to HR infants without ASD (see Iverson & Wozniak, 2016, for more extended discussion). For HR-ASD infants who exhibit significant, early-appearing vulnerabilities in social-communicative development, these differences in output may influence input in ways that further constrain opportunities for learning.
Differences in coordinated communication in ASD
Although base rates of less advanced joint attention behaviours were similar across groups, differences emerged when we analysed their coordination with vocalisations, such that HR-ASD infants vocalised significantly less often during these moments than HR-LD and HR-ND peers. This result is consistent with prior work reporting that toddlers with ASD combine communicative behaviours less often than peers (Parladé & Iverson, 2015; Shumway & Wetherby, 2009; Wetherby et al., 2004) and with evidence indicating that difficulties with coordination of communicative behaviours is characteristic of communication in ASD (Shumway & Wetherby, 2009; Stone, Ousley, Yoder, Hogan, & Hepburn, 1997).
Coordinating behaviour across modalities is a fundamental part of mature social communication, which involves a complex interplay between vocalisation, gesture, eye gaze, and facial affect. From relatively early in life, neurotypical infants coordinate these behaviours at above-chance levels (Bates, 1976; Crais et al., 2009; Stone et al., 1997). In infancy, these coordinations may serve an especially important function by increasing the salience and success of bids for joint attention (Goldin-Meadow, Goodrich, Sauer, & Iverson, 2007; Martinsen & Smith, 1989). Vocalisations are particularly effective in directing the attention of others (e.g., Gros-Louis et al., 2006). Communicative behaviours such as gaze shifts, smiles, and gestures require that the social partner visually monitor the infant to respond contingently, and thus they may go unnoticed. Vocalisations add an auditory cue that may enhance the likelihood of infants’ success in gaining or redirecting adult attention (e.g., Martinsen & Smith, 1989). Maybe even more importantly, adding a vocalisation to another behaviour represents a high degree of persistence and directedness on the part of the child. This directed, persistent quality may signal a readiness to learn to social partners. Future work should investigate the extent to which these coordinations contribute to infants’ social input from caregivers, above and beyond base rates of individual communicative behaviours.
Limitations and Future Directions
While this study has numerous methodological strengths, including a longitudinal and prospective design, it is important to note some limitations and directions for future work. First, we were unable to include a LR comparison group in this study. As described above, previous research has found differences between LR infants and HR infants, including those who do not go on to develop ASD, in both JA and vocalisation production (Cassel et al., 2007; Goldberg et al., 2005; Yirmiya et al., 2006). By virtue of having an older sibling with ASD, HR infants differ from LR infants both genetically and with regard to their home environments. However, the specific impact of having another child with ASD in the home on HR infants’ developmental experience is not yet well understood. While understanding the specificity of development among HR infants with and without language delays and ASD is a significant contribution to the literature, evaluating how HR infants, particularly those without an ASD diagnosis, compare to infants at low risk for ASD will be important to examine in future studies. Second, the sample of infants in this study was predominantly Caucasian and with highly educated parents, and thus external validity may be limited. A replication of this study with a more diverse population would help generalize the results. Finally, given the low production of some behaviours, even at 24 months in the ASD and LD groups, an extension of this study to later time points would clarify whether developmental trajectories in these groups plateau or ultimately follow a similar but delayed course compared to neurotypical peers.
Conclusions and Clinical Implications
Due to core social communication deficits in Autism Spectrum Disorder (APA, 2013), a central aim of research on infant development in ASD has been to uncover how communicative development differs from neurotypical samples. This effort has revealed differences in the onset and frequency of early communicative behaviours (e.g., Jones et al., 2014). The present study extends this work, finding that these behaviours also differ along another dimension: their coordination across modalities. Our findings have two general clinical implications. First, features of communicative behaviours—in particular, the extent to which they were coordinated with one another—distinguished HR infants with ASD from those with non-ASD language delay. This information could bolster efforts to enhance the differential diagnosis of ASD vs. language delay. Parents of infants eventually diagnosed with ASD often report that delayed language was the earliest indicator that their infant was developing atypically (e.g., Sacrey et al., 2015). Clinically, however, it is difficult to distinguish between ASD vs. language delay in very young children (Camarata, 2014), yet the ability to make this distinction has important consequences for decisions about the provision and direction of early intervention services. The findings reported above suggest that inclusion of opportunities to observe production of communicative behaviours in coordination in early screening and evaluation efforts is warranted.
Second, many early intervention approaches for very young children with or at risk for ASD focus on increasing infants’ communicative behaviours, with a particular emphasis on increasing bouts of joint attention via social gaze (see Bradshaw, Steiner, Gengoux, & Koegel, 2015, for a review). While these interventions have demonstrated some success in achieving this goal, it may also be useful to promote the coordination of multiple communicative behaviours. For example, encouraging production of vocalisations together with other communicative behaviours (e.g., eye gaze, gestures) may provide infants with more effective means of conveying communicative messages. Vocalisations combined with other social cues may be more salient to caregivers, enhancing the likelihood of an adult response, and they may also provide additional clues about the focus of the child’s attention (e.g., Goldstein, Schwade, Briesch, & Syal, 2010). In addition, coaching parents to recognize and respond to less salient or less developmentally advanced forms of communication (e.g., give/request gestures) with rich verbal input linked to infants’ current focus of attention may provide infants with increased opportunities for communicative exchange. Such an approach could enrich the everyday communicative environment in ways that encourage positive growth in very young children with communication delays with or without ASD. In particular, incorporating these techniques in Naturalistic Developmental Behavioural Interventions (NBDIs), which leverage parent coaching within naturalistic settings (e.g., during a bath time routine) to enhance early learning for children with ASD (Schreibman et al., 2015) may be beneficial. These models often incorporate imitation of joint attention behaviours; however, additional emphasis should focus on encouraging parents to imitate and expand on their child’s less salient gestures and vocalisations (e.g., VO vocalisations). Exposing young children to more advanced variations of their own gestures and vocalisations could challenge them to try new and diverse communicative behaviours while enhancing caregiver-child interaction.
What This Paper Adds.
Neurotypical infants frequently vocalise during bouts of joint attention—this reflects a directedness on the part of the infant. Considerable evidence indicates both early social behaviour and vocal development are atypical in Autism Spectrum Disorder (ASD); yet less is known about whether their coordination also differs.
· Results replicate prior accounts that joint attention behaviour and vocalisations are less frequent among infants who develop ASD. Importantly, they are also significantly less coordinated than both neurotypical and language delayed peers.
· Cross-modal coordination distinguished infants with eventual ASD from peers with language delay, which may have relevance for earlier detection efforts. Additionally, findings suggest that early intervention efforts aimed at increasing social-communication may benefit from a focus on increasing the coordinated quality of target behaviours.
Acknowledgments
Funding: This study was funded by Autism Speaks and the National Institutes of Health (R01 HD54979), with additional support from HD35469 and HD055748.
Footnotes
Conflict of Interest: The authors declare that they have no conflict of interest.
References
- AMERICAN PSYCHIATRIC ASSOCIATION, 2013, Diagnostic and statistical manual of mental disorders: DSM-5. (American Psychiatric Association: Washington, DC: ) [Google Scholar]
- BAKEMAN R and ADAMSON L, 1984, Coordinating attention to people and objects in mother-infant and peer-infant interactions. Child Development, 55, 1278–1289. [PubMed] [Google Scholar]
- BATES E, 1976, Language and context: The acquisition of pragmatics (New York: Academic Press; ). [Google Scholar]
- BATES E, BENIGNI L, BRETHERTON I, CAMAIONI L, and VOLTERRA V, 1979, The emergence of symbols: Cognition and communication in infancy (New York: Academic Press; ). [Google Scholar]
- BRADSHAW J, STEINER AM, GENGOUX G, and KOEGEL LK, 2015, Feasibility and effectiveness of very early intervention for infants at-risk for autism spectrum disorder: A systematic review. Journal of Autism and Developmental Disorders, 45, 778–794. [DOI] [PubMed] [Google Scholar]
- BRUNER JS, 1977, Early social interaction and language acquisition In Schaffer HR (ed), Studies in Mother-Infant Interaction (London: Academic Press; ), pp. 271–289. [Google Scholar]
- CAMARATA S, 2014, Early identification and early intervention in autism spectrum disorders: Accurate and effective? International Journal of Speech-Language Pathology, 16, 1–10. [DOI] [PubMed] [Google Scholar]
- CARPENTER M, NAGELL K, and TOMASELLO M, 1998, Social cognition, joint attention, and communicative competence from 9 to 15 months of age. Monographs of the Society for Research in Child Development, 63 (4, Serial No. 255), 1–143. [PubMed] [Google Scholar]
- CASSEL T, MESSINGER D, IBANEZ L, HALTIGAN J, ACOSTA S, and BUCHMAN A, 2007, Early social and emotional communication in the infant siblings of children with autism spectrum disorders: An examination of the broad phenotype. Journal of Autism and Developmental Disorders, 37, 122–132. [DOI] [PubMed] [Google Scholar]
- CHARMAN T, 1998, Specifying the nature and course of the joint attention impairment in autism in the preschool years: Implications for diagnosis and intervention. Autism, 2, 61–79. [Google Scholar]
- CHARMAN T, BARON-COHEN S, SWETTENHAM J, BAIRD G, COX A, and DREW A, 2000, Testing joint attention, imitation, and play as infancy precursors to language and theory of mind. Cognitive Development, 15, 481–498 [Google Scholar]
- CHAWARSKA K, MACARI SL, VOLKMAR FR, KIM SH, and SHIC F, 2014, ASD in infants and toddlers Handbook of Autism and Pervasive Developmental Disorders, Fourth Edition. [Google Scholar]
- CRAIS E, WATSON LR, and BARANEK GT, 2009, Use of gesture development in profiling children’s prelinguistic communication skills. American Journal of Speech-Language Pathology. 18:95–108. [DOI] [PubMed] [Google Scholar]
- ELLIS WEISMER S, and EVANS J, 2002, The role of processing limitations in early identification of specific language impairment. Topics in Language Disorders, 22, 15–29. [Google Scholar]
- FAGAN MK and DOVEIKIS KN, 2017, Ordinary interactions challenge proposals that maternal verbal responses shape infant vocal development. Journal of Speech, Language, and Hearing Research, 60, 2819–2827. [DOI] [PubMed] [Google Scholar]
- FENSON L, DALE PS, REZNICK JS, THAL D, BATES E, HARTUNG JP, . . . and REILLY JS, 1993, MacArthur Communicative Development Inventories: User’s guide and technical manual (San Diego, CA: Singular; ). [Google Scholar]
- GOLDBERG WA, JARVIS KL, OSANN K, LAULHERE TM, STRAUB C, THOMAS R, FILIPEK P, and SPENCE MA, 2005, Brief report: Early social communication behaviours in the younger siblings of children with autism. Journal of Autism and Developmental Disorders, 35, 657–664. [DOI] [PubMed] [Google Scholar]
- GOLDIN-MEADOW S, GOODRICH W, SAUER E, and IVERSON JM, 2007, Young children use their hands to tell their mothers what to say. Developmental Science, 10, 778–785. [DOI] [PubMed] [Google Scholar]
- GOLDSTEIN MH, KING AP, and WEST MJ, 2003, Social interaction shapes babbling: Testing parallels between birdsong and speech. Proceedings of the National Academy of Sciences, 100, 8030–8035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- GOLDSTEIN MH, and SCHWADE JA, 2008, Social feedback to infants’ babbling facilitates rapid phonological learning. Psychological Science, 19, 515–523. [DOI] [PubMed] [Google Scholar]
- GOLDSTEIN MH, SCHWADE J, BRIESCH J, and SYAL S, 2010, Learning while babbling: Prelinguistic object-directed vocalisations indicate a readiness to learn. Infancy, 15, 362–391. [DOI] [PubMed] [Google Scholar]
- GROS-LOUIS J, WEST M, GOLDSTEIN M, and KING A, 2006, Mothers provide differential feedback to infants’ prelinguistic sounds. International Journal of Behavioural Development, 30, 509–516. [Google Scholar]
- HARDING CG, and GOLINKOFF RM, 1979, The origins of intentional vocalisation in prelinguistic infants. Child Development, 50, 33–40. [PubMed] [Google Scholar]
- HEILMANN J, WEISMER SE, EVANS J, and HOLLAR C, 2005, Utility of MacArthur-Bates Communicative Development Inventory in identifying language abilities of late-talking and typically developing toddlers. American Journal of Speech-Language Pathology, 14, 40–51. [DOI] [PubMed] [Google Scholar]
- HSU HC, FOGEL A, and MESSINGER D, 2001, Infant non-distress vocalisation during mother-infant face-to-face interaction: Factors associated with quantitative and qualitative differences. Infant Behaviour and Development, 24, 107–128. [Google Scholar]
- IVERSON JM, and WOZNIAK RH, 2016, Transitions to intentional and symbolic communication in typical development and in Autism Spectrum Disorder In Keen D, Meadan H, Brady N, and Halled J (eds), Prelinguistic and Minimally Verbal Communicators on the Autism Spectrum (Singapore: Springer; ), pp. 51–72. [Google Scholar]
- IVERSON JM, NORTHRUP JB, LEEZENBAUM NB, PARLADÉ MV, KOTERBA EA, and WEST KL, 2018, Early gesture and vocabulary development in infant siblings of children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 48, 55–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- JONES EJ, GLIGA T, BEDFORD R, CHARMAN T, and JOHNSON MH, 2014, Developmental pathways to autism: A review of prospective studies of infants at risk. Neuroscience and Biobehavioural Reviews, 39, 1–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- LANDA R, and GARRETT-MAYER E, 2006, Development in infants with autism spectrum disorders: A prospective study. Journal of Child Psychology and Psychiatry, 47, 629–638. [DOI] [PubMed] [Google Scholar]
- LEEZENBAUM NB, CAMPBELL SB, BUTLER D, and IVERSON JM, 2014, Maternal verbal responses to communication of infants at low and heightened risk of autism. Autism, 18, 694–703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- LORD C, RISI S, LAMBRECHT L, COOK EH, LEVENTHAL BL, DILAVORE P, et al. , 2000, The Autism Diagnostic Observation Schedule–Generic: A standard measure of social and communication deficits associated with the spectrum of autism. Journal of Autism and Developmental Disorders, 30, 205–223. [PubMed] [Google Scholar]
- MARTINSEN H, and SMITH L, 1989, Studies of vocalisation and gesture in the transition to speech In von Tetzchner S, Siegel LS and Smith L (eds), The social and cognitive aspects of normal and atypical language development (New York: Springer; ), pp. 95–112. [Google Scholar]
- MORALES M, MUNDY P, DELGADO CEF, YALE M, MESSINGER D, NEAL R, and SCHWARTZ HK, 2000, Responding to joint attention across the 6- through 24-month age period and early language acquisition. Journal of Applied Developmental Psychology, 21, 283–298. [Google Scholar]
- MULLEN EM, 1995, Mullen Scales of Early Learning (Circle Pines, MN: American Guidance Service; ). [Google Scholar]
- MUNDY P, SIGMAN M, KASARI C, and YIRMIYA N, 1988, Nonverbal communication skills in down syndrome children. Child Development, 59, 235–249. [PubMed] [Google Scholar]
- MUNDY P, SIGMAN M, and KASARI C, 1994, Joint attention, developmental level, and symptom presentation in young children with autism. Development and Psychopathology, 6, 389–401. [Google Scholar]
- MUNDY P, KASARI C, SIGMAN M, and RUSKIN E, 1995, Nonverbal communication and language development in children with down syndrome and children with normal development. Journal of Speech and Hearing Research, 38, 157–167. [DOI] [PubMed] [Google Scholar]
- MUNDY P, and CROWSON M, 1997, Joint attention and early social communication: Implications for research on intervention with autism. Journal of Autism and Developmental Disorders, 27, 653–676. [DOI] [PubMed] [Google Scholar]
- MUNDY P, DELGADO C, BLOCK J, VENEZIA A, and SIEBERT J, 2003, Early Social Communication Scales (University of Miami, Coral Gables, FL: ). [Google Scholar]
- MUNDY P, BLOCK J, VAUGHN VAN HECKE A, DELGADO C, PARLADÉ M, and POMERAS Y, 2007, Individual differences in the development of joint attention in infancy. Journal of Child Psychology and Psychiatry, 44, 793–809. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MURRAY DS, CREAGHEAD NA, MANNING-COURTNEY P, SHEAR PK, BEAN J, and PRENDEVILLE J, 2008, The relationship between joint attention and language in children with autism spectrum disorder. Focus on Autism and Other Developmental Disabilities, 23, 5–14. [Google Scholar]
- NAKAO K, and TREAS J, 1994, Updating occupational prestige and socioeconomic scores: How the new measures measure up. Sociological Methodology, 24, 1–72. [Google Scholar]
- OLLER D, EILERS R, NEAL A, and SCHWARTZ H, 1999, Precursors to speech in infancy: The prediction of speech and language disorders. Journal of Autism and Developmental Disorders, 32, 223–245. [DOI] [PubMed] [Google Scholar]
- OZONOFF S, IOSIF AM, BAGUIO F, COOK IC, HILL MM, HUTMAN T, ... and STEINFELD MB, 2010, A prospective study of the emergence of early behavioural signs of autism. Journal of the American Academy of Child and Adolescent Psychiatry, 49, 256–266. [PMC free article] [PubMed] [Google Scholar]
- OZONOFF S, YOUNG GS, CARTER A, MESSINGER D, YIRMIYA N, ZWAIGENBAUM L, ... and HUTMAN T, 2011, Recurrence risk for autism spectrum disorders: A Baby Siblings Research Consortium study. Pediatrics, 128, e488–e495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- PARLADÉ MV, and IVERSON JM, 2015, The development of coordinated communication in infants at heightened risk for autism spectrum disorder. Journal of Autism and Developmental Disorders, 45, 2218–2234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- PATTEN E, BELARDI K, BARANEK GT, WATSON LR, LABBAN JD, and OLLER DK, 2014, Vocal patterns in infants with autism spectrum disorder: Canonical babbling status and vocalisation frequency. Journal of Autism and Developmental Disorders, 44, 2413–2428. [DOI] [PMC free article] [PubMed] [Google Scholar]
- PAUL R, FUERST Y, RAMSAY G, CHAWARSKA K, and KLIN A, 2011, Out of the mouths of babes: Vocal production in infant siblings of children with ASD. Journal of Child Psychology and Psychiatry, 52, 588–598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- PLUMB AM, and WETHERBY AM, 2013, Vocalisation development in toddlers with autism spectrum disorder. Journal of Speech, Language, and Hearing Research, 56, 721–734. [DOI] [PubMed] [Google Scholar]
- ROZGA A, HUTMAN T, YOUNG GS, ROGERS SJ, OZONOFF S, DAPRETTO M, and SIGMAN M, 2011, Behavioural profiles of affected and unaffected siblings of children with autism: Contribution of measures of mother–infant interaction and nonverbal communication. Journal of Autism and Developmental Disorders, 41, 287–301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- SACREY LAR, ZWAIGENBAUM L, BRYSON S, BRIAN J, SMITH IM, ROBERTS W, ... and VAILLANCOURT T, 2015, Can parents’ concerns predict autism spectrum disorder? A prospective study of high-risk siblings from 6 to 36 months of age. Journal of the American Academy of Child and Adolescent Psychiatry, 54, 470–478. [DOI] [PubMed] [Google Scholar]
- SCHOEN E, PAUL R, and CHAWARSKA K, 2011, Phonology and vocal behaviour in toddlers with autism spectrum disorders. Autism Research, 4, 177–188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- SCHREIBMAN L, DAWSON G, STAHMER AC, LANDA R, ROGERS SJ, MCGEE GG, … and HALLADAY A, 2015, Naturalistic Developmental Behavioural Intervention: Empirically validated treatments for autism spectrum disorder. Journal of Autism and Developmental Disorders, 45, 2411–2428. [DOI] [PMC free article] [PubMed] [Google Scholar]
- SEIBERT JM, HOGAN AE, and MUNDY PC, 1984, Mental age and cognitive stage in young handicapped and at-risk children. Intelligence, 8, 11–9. [Google Scholar]
- SHUMWAY S, and WETHERBY AM, 2009, Communicative acts of children with autism spectrum disorders in the second year of life. Journal of Speech, Language, and Hearing Research, 52, 1139–1156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- STONE WL, OUSLEY OY, YODER PJ, HOGAN KL, and HEPBURN SL, 1997, Nonverbal communication in two-and three-year-old children with autism. Journal of Autism and Developmental Disorders, 27, 677–696. [DOI] [PubMed] [Google Scholar]
- TOTH K, MUNSON J, MELTZOFF AN, and DAWSON G, 2006, Early predictors of communication development in young children with autism spectrum disorder: Joint attention, imitation, and toy play. Journal of Autism and Developmental Disorders, 36, 993–1005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- WATSON LR, CRAIS ER, BARANEK GT, DYKSTRA JR, and WILSON KP, 2013, Communicative gesture use in infants with and without autism: A retrospective home video study. American Journal of Speech-Language Pathology, 22, 25–39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- WETHERBY AM, WOODS J, ALLEN L, CLEARY J, DICKINSON H, and LORD C, 2004, Early indicators of autism spectrum disorders in the second year of life. Journal of Autism and Developmental Disorders, 34, 473–493. [DOI] [PubMed] [Google Scholar]
- WEST KL, LEEZENBAUM NB, NORTHRUP JB, and IVERSON JM, in press, The relation between walking and language in infant siblings of children with Autism Spectrum Disorder. Child Development. [DOI] [PMC free article] [PubMed] [Google Scholar]
- WINDER BM, WOZNIAK RH, PARLADÉ MV, and IVERSON JM, 2013, Spontaneous initiation of communication in infants at low and heightened risk for Autism Spectrum Disorder. Developmental Psychology, 49, 1931–1942. [DOI] [PMC free article] [PubMed] [Google Scholar]
- YIRMIYA N, GAMLIEL I, PILOWSKY T, FELDMAN R, BARON-COHEN S, and SIGMAN M, 2006, The development of siblings of children with autism at 4 and 14 months: Social engagement, communication, and cognition. Journal of Child Psychology and Psychiatry, 47, 511–523. [DOI] [PubMed] [Google Scholar]