

Abstract
Background:
Vitamin D is associated with musculoskeletal function in our body, and its deficiency is a common health problem all over the world. Low back pain (LBP) is an important health problem in terms of low quality of life, loss of work power, and cost of diagnosis and treatment approaches.
Aims:
The purpose of this study is to investigate the relationship between pain severity and Vitamin D deficiency in patients who applied to pain polyclinic with LBP.
Settings and Design:
This was a retrospective, observational study.
Subjects and Methods:
The files of patients aged between 18 and 70 years who applied to our hospital between January and February 2018 were examined retrospectively by a specialist. Serum 25-hydroxyvitamin D (25(OH)D) level, Visual Analogue Scale (VAS), age, education level, marital status, working status, and body mass index (BMI) values recorded in patient files were included in the study. The limit value of Vitamin D was accepted as 20 ng/mL. Patients were divided into two groups according to their levels of Vitamin D. Patients with serum 25(OH)D levels below 20 ng/mL were considered as the deficiency of Vitamin D (Group 1) and patients with 20 ng/mL and over 20 ng/mL values were considered as normal in terms of Vitamin D (Group 2).
Statistical Analysis Used:
Descriptive statistical data were presented as mean, standard deviation, numbers, and percentage. There was no difference between the normally distributed group and the non-normally distributed group in terms of vitamin D levels. To compare the frequencies, the Chi-square test was used. To define the linear association between independent variables and Vitamin D level, Spearman's rho correlation coefficients were calculated.
Results:
The level of Vitamin D was measured in 98 patients aged 18–70 years who applied to our hospital's polyclinic due to LBP during the study period. The deficiency of vitamin was detected in 84 (85.7%) of the patients, while Vitamin D was found in 14 (14.3%) as normal. Groups were similar in terms of age, gender, BMI, educational level, marital status and working status (p> 0.05); however, there was a statistically significant difference between the two groups in terms of VAS score and levels of Vitamin D (P < 0.001 and P < 0.001, respectively). While there was a negative correlation between D vitamin level and VAS score (r = −0.594, P < 0.001), there was no correlation between age, gender, BMI, education level, marital status, and working status (P > 0.05).
Conclusions:
The deficiency of Vitamin D is often asymptomatic, and also, it can cause bone and muscle pain. In our study, we determined that the severity of pain increased in patients with LBP as the deficiency of Vitamin D increased. For this reason, we recommend to be evaluated the level of Vitamin D in patients with LBP.
Keywords: Low back pain, pain intensity, serum 25-hydroxyvitamin D, Vitamin D deficiency
INTRODUCTION
Vitamin D, one of the vitamins of fat-soluble vitamins, is a group of sterols which are hormones and hormone precursors because it can also be synthesized endogenously. The most important effects are on calcium metabolism, phosphorus metabolism, and bone mineralization.[1,2] In recent years, the deficiency and insufficiency of Vitamin D have been determined to be associated with many chronic diseases.[3,4] In our country also, the deficiency or insufficiency of Vitamin D has appeared more and more in the recent period, with increasing opportunities and availability of healthcare. In some sources, the deficiency of Vitamin D is now considered as a global epidemic.[5] The level of serum 25-hydroxyvitamin D (25(OH)D) should be measured to assess the Vitamin D status. It is accepted that if the level of serum 25(OH)D is >30 ng/mL, the level of Vitamin D is adequate; if it is 20–30 ng/mL, there is Vitamin D deficiency; if it is <20 ng/mL, there is lack of Vitamin D; and if it is <10 ng/mL, there is a serious lack of Vitamin D. Due to the low number of foods containing Vitamin D, a small proportion (10%–20%) of this vitamin is consumed with food. A significant portion (80%–90%) is synthesized in the skin by ultraviolet B rays. For synthesis, direct sunlight contact is required on the skin. The angle of sunlight reaching the earth's surface is effective in the synthesis of Vitamin D. At the geographic latitudinal of our country, the synthesis of Vitamin D takes place between May and November. Since the appropriate beam angle is between 10.00 A.M and 03.00 P.M, it is advisable to go out in the sun at these times for the synthesis of Vitamin D. If the whole body is exposed to sunlight and appears light pink color at appropriate times during summer, about 20,000 IU Vitamin D synthesis occurs at an equivalent level to the dose of Vitamin D.[5,6]
It is estimated that about one billion people in the world are experiencing lack of Vitamin D. In the literature, the Vitamin D status differs in different countries, even in different regions of the same country. In the United States and Europe, 40%–100% of elderly men and women living in society (not at nursing home) have been reported to have Vitamin D deficiency.[7]] In a study Uçar et al have done in recent years in Ankara of Turkey.; they've reported vitamine D deficiency (51.8%), vitamine D insufficiency (20.7%).[8] Clinical findings of Vitamin D deficiency depend on the grade and duration of deficiency. Most patients are asymptomatic.[9] Deficiency causes rickets in children and osteomalacia in adults. In some patients, bone loss due to secondary hyperparathyroidism is accelerated and osteoporosis develops. Patients may develop a decrease in bone mineral density, widespread bone muscle pain, bone sensitivity, muscle weakness, walking difficulty, and fractures, depending on the degree of deficiency and failure.[10,11,12,13]
In people having lack of Vitamin D, the muscle strength of waist, back, neck decreases. Decreased muscle strength can cause herniated disc and cervical discal hernia. All of this is reflected in the patient's pain. We wanted to pay attention to the necessity of considering the lack of Vitamin D in low back pain (LBP) which is one of the common complaints of our patients.
SUBJECTS AND METHODS
This is a retrospective, observational study.
Source of data
The study was conducted in accordance with the Declaration of Helsinki. We included 98 patients who had appealed to our polyclinic with a complaint of LBP between January and February 2018, who had been diagnosed with disc herniation in the lumbar magnetic resonance, and whose level of Vitamin D had been measured.
Sampling procedure
The data of patients between 18 and 70 years of age with a diagnosis of LBP were included in the study by means of the automation system and its files by specialist doctors. Patients who admitted to our outpatient clinic with LBP were divided into two groups as Vitamin D deficient (Group 1) with a Vitamin D level below 20 ng/mL and normal (Group 2) with a value above 20 ng/mL. The relationship between severity of pain and Vitamin D levels was evaluated.
Method of collection of data
Inclusion criteria
Patients whose
Pain has been defined
Pain level has been determined by visual analog scale (VAS)
Vitamin D levels have been determined in ng/mL.
Exclusion criteria before work
Patients who have missing demographic or study data
Trauma, infection, and endocrinologic, neurological, and rheumatologic patients diagnosed with diseases, tumors, and depression
Patients who are followed up with osteomalacia diagnosis
Patients with advanced osteoporosis and compression fracture in X-ray were excluded from the screening.
As a result of the screening, 98 patients were eligible to be included in the study [Figure 1]. Patients' demographic data including age, gender, body mass index (BMI), education level, marital status, and occupation were recorded.
Figure 1.
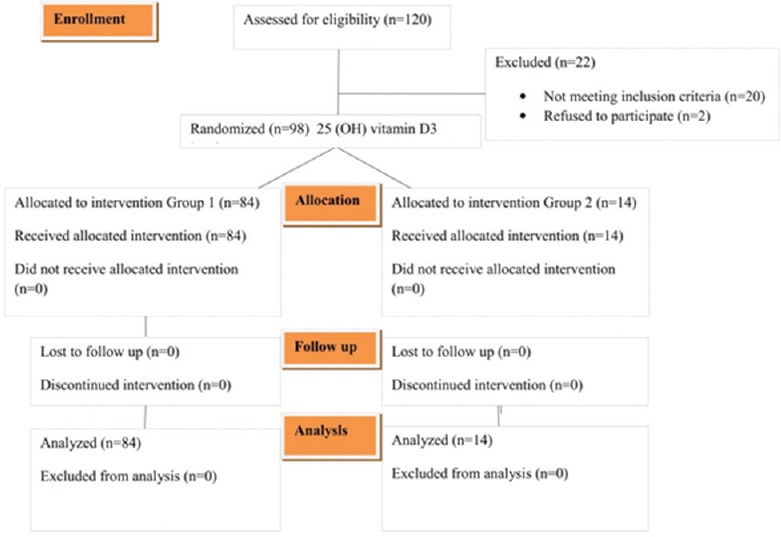
Consort diagram (Group 1 = Serum 25-hydroxyvitamin D 3 deficient; Group 2 = Serum 25-hydroxyvitamin D 3 normal)
Pain level was evaluated as nominal data determined by 10-cm Visual Analog Scale (VAS). VAS is resulted from marking on a horizontal line where patients have no pain shown as “0” and where the pain is the most severe shown as “10.”
Statistical analysis
All the analyses were carried out by means of Windows SPSS software (IBM Corp., Released 2013. IBM SPSS Statistics for Windows, version 22.0. (IBM Corp., Armonk, NY, USA). Appropriateness of variables was investigated with visual and analytical methods. Descriptive statistical data were presented as mean, standard deviation, numbers, and percentage. There was no difference between the normally distributed group and the non-normally distributed group in terms of vitamin D levels. To compare frequencies, the Chi-square test was used. To define the linear association between independent variables and Vitamin D level, Spearman's rho correlation coefficients were calculated. The statistical significance level was accepted as P < 0.05. As correlation coefficients, the correlations between 0 and 0.25 were assessed as “none,” between 0.25 and 0.50 as “weak-moderate,” between 0.50 and 0.75 as “severe,” and between 0.75 and 1.00 as “much severe.”
Ethics, consent and permissions
This study was reviewed and approved by the Institutional Review Board at the Diyarbakir Gazi Yasargil Training and Education Hospital, ID: 51, 2017, Diyarbakir/Turkey. Written informed consent was obtained from all patients.
RESULTS
Forty-six patients (46.9%) were men and 52 (53.1%) of 98 patients who applied to our polyclinic due to LBP were women. The mean Vitamin D level was lower in women (12.21 ± 9.25 ng/mL) than in men (14.28 ± 6.35 ng/mL) but not statistically meaningful (P > 0.206).
Group 1 consisted of patients with Vitamin D deficiency and Group 2 consisted of patients with Vitamin D normal. D vitamin deficiency (Group 1) was detected in 84 (85.7%) of the patients, while Vitamin D level was found to be normal in 14 (14.3%) of the patients (Group 2).
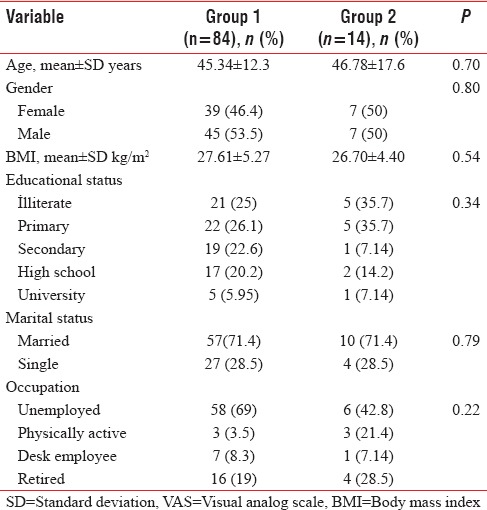
Sociodemographic data of the groups are presented in Table 1. The mean age of the groups (45, 34 ± 12.3 years vs. 46.78 ± 17.6 years), sex, BMI (27.61 ± 5.27 kg/m2 vs. 26.70 ± 4.40 kg/m2), education level, and marital status were compared, but there was no statistically significant difference between the results (P > 0.05), [Table 1].
Table 1.
Distribution of the general characteristics of the low back pain patients
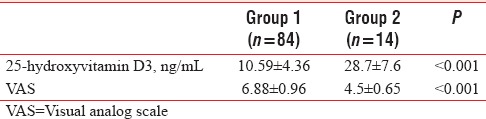
In comparison of D vitamin levels of the groups, Group 1 (10.59 ± 4.36 ng/mL) was statistically significantly lower than Group 2 (28.7 ± 7.6 ng/mL) (P < 0.001). In the comparison of VAS scores of the groups, Group 1 (6.88 ± 0.96) was statistically significantly higher (P < 0.001) than Group 2 (4.5 ± 0.65) [Table 2].
Table 2.
Group 25-hydroxyvitamin D3 levels and pain severity scores
While a negative correlation was found between D vitamin level and VAS score with Spearman's rho (r = −0.594, P < 0.001) [Figure 2], no correlation was found between BMI, age, education level, marital status, and working status (P > 0.05).
Figure 2.
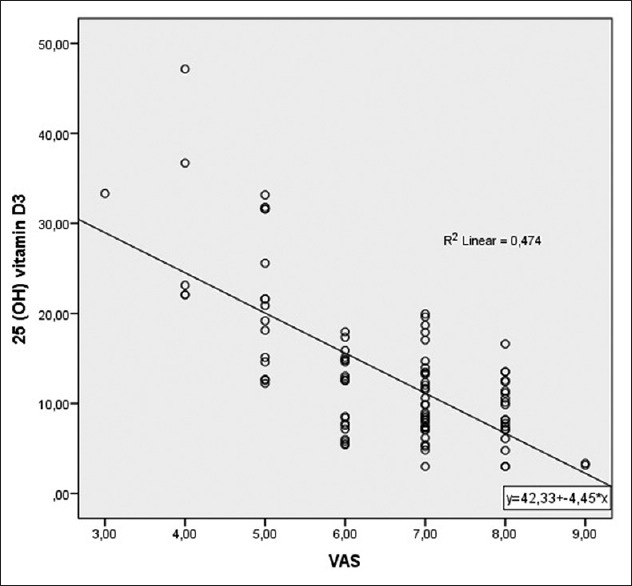
Association between scores obtained in 25-hydroxyvitamin D3 and in the VAS
DISCUSSION
In our study, we investigated the relationship between the severity of pain and the level of Vitamin D in patients with LBP and those who applied to the pain clinic. The data we obtained showed that patients with LBP had a deficiency of Vitamin D and that there was a negative correlation between the level of Vitamin D and pain severity. We also found that Vitamin D levels in young female patients with LBP were lower than males but not statistically significant. In a review study that supports our study, the relationship between Vitamin D and LBP has been investigated and it has been found that patients with LBP have lower serum 25(OH)D levels and more common in younger women.[14] The mean age of the groups (45.34 ± 12.3 years vs. 46.78 ± 17.6 years), sex, BMI (27.61 ± 5.27 kg/m2 vs. 26.70 ± 4.40 kg/m2), education level, marital status, and working conditions were compared and any statistically significant differences were not found.
When we performed literature review, there were few studies investigating the relationship between D vitamin and pain severity. In some studies, there was a significant correlation between serum 25(OH)D and pain severity.[15] However, in some studies, serum 25(OH)D and pain severity were not significantly correlated.[16,17] Considering these conflicting findings, careful evaluation of Vitamin D supplementation is required.
LBP and lack of vitamins are the most common health problems in our country and all over the world. The synthesis of >90% of Vitamin D in the body occurs under the influence of sunlight. Vitamin D, taken with foods, does not have a significant contribution, especially after a supplement is not taken. Seasonal and geographical changes are inevitable in the synthesis of Vitamin D in the derailment as the primary source is sunlight.[18,19,20] The average prevalence in Vitamin D deficiency prevalence studies in the USA is reported as 41.6%, which is 82.1% in Black people and 69.2% in Hispanics.[21] Hovsepian et al.[22] reported a 50.8% prevalence of Vitamin D deficiency in the young adult population. In a large retrospective study conducted in our country, Çidem et al.[23] reported a Vitamin D deficiency ratio of 71.7% in the population, which is a common body pain. The population in our study was selected from a group of pain complaints, and 85.7% of the cases were found to have Vitamin D deficiency and 14.3% to have a normal range of Vitamin D. This result shows serious similarity with a retrospective study by Karahan et al.,[24] who determined that 2202 (70.9%) of 3104 registered patients having nonspecific musculoskeletal pain had Vitamin D deficiency, while 516 patients (16.6%) had Vitamin D inadequacy (total 87.5%) and 386 (12.4%) have normal range of Vitamin D.
In a study conducted by Al Faraj and Al Mutairi, in patients with chronic LBP between 15 and 52 years of age, 299 (83%) out of 360 patients were found to have low Vitamin D level and Vitamin D deficiency was considered to be one of the major factors of chronic LBP.[25] In a study conducted in our country in 2013, 8457 patients who have common pain with a mean age of 46.7 years were evaluated, and the prevalence of Vitamin D deficiency was found to be 71.7% in this group.[23] In a study conducted by Badsha et al., 139 patients who were diagnosed with pain complaints and D vitamin deficiency were treated with Vitamin D and 90% of them achieved clinical improvement.[26] However, in a review of four studies comparing placebo and D vitamin therapy in patients with pain complaints, only one study showed that Vitamin D supplements were superior to placebo.[27]
Limitations of the study
The most important limitation of our study is a retrospective study. It is also not possible to generalize the outcome because the study group population was selected from patients with LBP who had applied to the pain clinic. In our study, the values associated with Vitamin D metabolism such as calcium, phosphorus, and alkaline phosphatase have not been examined and laboratory methods do not show an accurate homogeneity as in many multicenter studies.
CONCLUSIONS
Our study indicates a connection between Vitamin D deficiency and the severity of the pain in patients with LBP. The widespread screening of Vitamin D levels in individuals with LBP should be taken into consideration because of the cheap, safe, treatable form of the symptoms for clinicians. Prospective studies are essential to demonstrate the association between LBP and Vitamin D deficiency and to investigate whether Vitamin D deficiency increases the risk of developing LBP to determine the potential role of Vitamin D deficiency in the prevention of LBP.
Financial support and sponsorship
The study was funded by departmental resources.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The manuscript has been read and approved by all the authors, that the requirements for authorship as stated earlier in this document have been met, and that each author believes that the manuscript represents honest work.
REFERENCES
- 1.Champe PC, Harvey A FD. In: Lippincott's Illustrated eviews Series. 3rd ed. Ulukaya E, editor. Nobel Medicine Bookstores; 2007. [Google Scholar]
- 2.Richard BF, Demay Marie B, Krane Stephen M, Kronenberget Henry M. Bone and Mineral Metabolism in Health and Disease. Harrison's Princ Intern Med. 2005;16:2238–86. [Google Scholar]
- 3.Holick MF. Vitamin D: A D-lightful health perspective. Nutr Rev. 2008;66:S182–94. doi: 10.1111/j.1753-4887.2008.00104.x. [DOI] [PubMed] [Google Scholar]
- 4.Hyppönen E, Boucher BJ, Berry DJ, Power C. 25-hydroxyvitamin D, IGF-1, and metabolic syndrome at 45 years of age: A cross-sectional study in the 1958 British birth cohort. Diabetes. 2008;57:298–305. doi: 10.2337/db07-1122. [DOI] [PubMed] [Google Scholar]
- 5.Wacker M, Holick MF. Vitamin D-effects on skeletal and extraskeletal health and the need for supplementation. Nutrients. 2013;5:111–48. doi: 10.3390/nu5010111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357:266–81. doi: 10.1056/NEJMra070553. [DOI] [PubMed] [Google Scholar]
- 7.Lips P. Vitamin D status and nutrition in Europe and Asia. J Steroid Biochem Mol Biol. 2007;103:620–5. doi: 10.1016/j.jsbmb.2006.12.076. [DOI] [PubMed] [Google Scholar]
- 8.Uçar F, Taşlıpınar MY, Soydaş AÖ, Özcan N. 25-OH Vitamin D Levels in Patients Admitted to Ankara Etlik Specialty Training and Research Hospital. Eur J Basic Med Sci. 2012;2:12–5. [Google Scholar]
- 9.Valcour A, Blocki F, Hawkins DM, Rao SD. Effects of age and serum 25-OH-vitamin D on serum parathyroid hormone levels. J Clin Endocrinol Metab. 2012;97:3989–95. doi: 10.1210/jc.2012-2276. [DOI] [PubMed] [Google Scholar]
- 10.Garg MK, Tandon N, Marwaha RK, Menon AS, Mahalle N. The relationship between serum 25-hydroxy Vitamin D, parathormone and bone mineral density in İndian population. Clin Endocrinol (Oxf) 2014;80:41–6. doi: 10.1111/cen.12248. [DOI] [PubMed] [Google Scholar]
- 11.Cauley JA, Parimi N, Ensrud KE, Bauer DC, Cawthon PM, Cummings SR, et al. Serum 25-hydroxyvitamin D and the risk of hip and nonspine fractures in older men. J Bone Miner Res. 2010;25:545–53. doi: 10.1359/jbmr.090826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hoy D, Brooks P, Blyth F, Buchbinder R. The epidemiology of low back pain. Best Pract Res Clin Rheumatol. 2010;24:769–81. doi: 10.1016/j.berh.2010.10.002. [DOI] [PubMed] [Google Scholar]
- 13.Atadağ Y, Aydın A, Kaya D, Köşker HD, Başak F US. Amendments in Application Reasons to the Third Step Health Care Establishment by İmplementation of Family Practise. Turkey Family Practise Journal. 2016;20:141–51. [Google Scholar]
- 14.Zadro J, Shirley D, Ferreira M, Carvalho-Silva AP, Lamb SE, Cooper C, et al. Mapping the association between Vitamin D and low back pain: A systematic review and meta-analysis of observational studies. Pain Physician. 2017;20:611–40. [PubMed] [Google Scholar]
- 15.Lotfi A, Abdel-Nasser AM, Hamdy A, Omran AA, El-Rehany MA. Hypovitaminosis D in female patients with chronic low back pain. Clin Rheumatol. 2007;26:1895–901. doi: 10.1007/s10067-007-0603-4. [DOI] [PubMed] [Google Scholar]
- 16.Johansen JV, Manniche C, Kjaer P. Vitamin D levels appear to be normal in Danish patients attending secondary care for low back pain and a weak positive correlation between serum level Vitamin D and modic changes was demonstrated: A cross-sectional cohort study of consecutive patients with non-specific low back pain. BMC Musculoskelet Disord. 2013;14:78. doi: 10.1186/1471-2474-14-78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ghai B, Bansal D, Kapil G, Kanukula R, Lavudiya S, Sachdeva N. High prevalence of hypovitaminosis D in İndian chronic low back patients. Pain Physician. 2015;18:E853–62. [PubMed] [Google Scholar]
- 18.Fidan F, Alkan BM, Tosun A. Pandemic of the Era: Vitamin D Deficiency and Insufficiency. Türk Osteoporoz Derg. 2014;20:71–4. [Google Scholar]
- 19.Yilmaz H, Bodur S, Karaca G. The association between Vitamin D level and chronic Pain and depression in premenopausal women. Turk J Phys Med Rehabil. 2014;60:121–5. [Google Scholar]
- 20.Wacker M, Holick MF. Sunlight and Vitamin D: A global perspective for health. Dermatoendocrinol. 2013;5:51–108. doi: 10.4161/derm.24494. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Forrest KY, Stuhldreher WL. Prevalence and correlates of Vitamin D deficiency in US adults. Nutr Res. 2011;31:48–54. doi: 10.1016/j.nutres.2010.12.001. [DOI] [PubMed] [Google Scholar]
- 22.Hovsepian S, Amini M, Aminorroaya A, Amini P, Iraj B. Prevalence of Vitamin D deficiency among adult population of İsfahan city, İran. J Health Popul Nutr. 2011;29:149–55. doi: 10.3329/jhpn.v29i2.7857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Çidem M, Kara S, Sarı H, Özkaya M, Karacan İ. Prevalence and risk factors of Vitamin D deficiency in patients with widespread musculoskeletal pain. J Clin Exp Investig. 2013;4:488–91. [Google Scholar]
- 24.Fidan F, Alkan BM, Tosun A. Pandemic of the Era: Vitamin D Deficiency and Insufficiency. Türk Osteoporoz Derg. 2014;20:71–4. [Google Scholar]
- 25.Al Faraj S, Al Mutairi K. Vitamin D deficiency and chronic low back pain in Saudi Arabia. Spine (Phila Pa 1976) 2003;28:177–9. doi: 10.1097/00007632-200301150-00015. [DOI] [PubMed] [Google Scholar]
- 26.Badsha H, Daher M, Ooi Kong K. Myalgias or non-specific muscle pain in Arab or Indo-Pakistani patients may indicate Vitamin D deficiency. Clin Rheumatol. 2009;28:971–3. doi: 10.1007/s10067-009-1146-7. [DOI] [PubMed] [Google Scholar]
- 27.Straube S, Derry S, Moore AR, McQuay HJ. Vitamin D for the treatment of chronic painful conditions in adults [Systematic review] Cochrane Database Syst Rev. 2015;5:1–52. doi: 10.1002/14651858.CD007771.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]