

Abstract
Diabetes mellitus and heart failure are two multifaceted entities characterised by high morbidity and mortality. Early epidemiological and prospective studies have observed the frequent co-existence of both conditions. Importantly, diabetes mellitus can precipitate or worsen heart failure due to the accumulation of advanced glycation end products, oxidative stress, inflammatory status impairment, decay of intracellular calcium, changes in microRNAs expression, not to mention atherosclerosis progression and coronary artery disease. Heart failure also impairs glucose metabolism through less well-known mechanisms. Attention must especially be given in the treatment as there are frequently adverse interactions between the two diseases and novel agents against diabetic cardiomyopathy are under investigation. As several missing links still exist in the connection between heart failure and diabetes mellitus we will review, in this article, the most recent data underlying the interaction of them and provide an overview of the most important clinical perspectives.
Keywords: Diabetes mellitus, heart failure, treatment, oxidative stress, inflammation, pathophysiology
Diabetes mellitus (DM) is a group of diseases characterised by metabolic disturbances with increasing prevalence worldwide.[1] Individuals with DM present several detrimental micro- and macrovascular complications such as retinopathy, nephropathy, neuropathy, atherosclerosis and coronary heart disease.[2,3] Accordingly, efforts for early diagnosis and appropriate management are of ultimate importance.
Despite the emphasis by clinicians in the prompt control of DM several cardiovascular diseases such as hypertension, coronary heart disease, stroke, peripheral vascular disease, etc., have been linked to impaired glucose management.[4] Recently, the awareness in the scientific community of the two-way association between DM and heart failure (HF) has steadily increased and has gained research interest.
HF is a syndrome with a complex pathophysiology, several aetiologies and different clinical presentations characterised by high morbidity and mortality.[5–7] According to some reports the co-existence of HF and DM is as high as almost 40 %,[8] growing the necessity for more in-depth understanding of the common pathophysiological pathways and for effective management of both entities.
As several missing links still exist in the connection between HF and DM we review in this article the most recent data underlying the interaction between them and provide an overview of the most important clinical perspectives.
Diabetes Mellitus and Heart Failure – A Bidirectional Relationship
From Diabetes Mellitus to Heart Failure
The concept that DM can cause or precipitate HF has been generated even from the Framingham study who estimated that men and women with DM have a two and four times, respectively, increased risk to develop HF compared with non-DM subjects.[9] Epidemiological studies have confirmed this relationship and revealed that impaired glucose tolerance, increased serum glucose levels and glycated haemoglobin levels are associated not only with incidence of systolic HF but also with the prevalence of diastolic dysfunction (see Table 1). Accordingly, guidelines have accepted DM and metabolic syndrome as risk factors for HF,[17] and the term diabetic cardiomyopathy was used to define either systolic or diastolic left ventricular dysfunction in otherwise healthy diabetic persons in the absence of clinically significant coronary, valvular or hypertensive disease.[18] Thus, patients with DM can be categorised in the stage A of the American College of Cardiology Foundation (ACCF)/American Heart Association (AHA) classification of HF, meaning that diabetic subjects are at high-risk for HF but without structural heart disease or symptoms of HF. Therapeutic interventions aim to modify risk factors and guidelines draw attention to monitor and treat DM as early as possible.[17]
Table 1: Studies Examined the Association between Diabetes Mellitus and Heart Failure.
| Study/Author | Design | Subjects | Results |
|---|---|---|---|
| Nichols et al. 2004[10] | Retrospective cohort | 8,231 patients with DM and 8,845 non-DM patients | The incidence rate of HF in DM subjects was 3 times that of non-DM |
| Iribarren et al. 2001[11] | Prospective cohort (2.2 years follow-up) | 49.000 DM patients | Increased levels were associated with greater risk of HF |
| Stratton et al. 2000 (UKPDS 35)[12] | Prospective observational study | 4,585 DM patients | In type 2 DM patients the risk of diabetic complications and HF was strongly associated with previous hyperglycaemia |
| Matsushita et al. 2010 (ARIC study)[13] | Prospective cohort (14.1 years follow-up) | 11.000 subjects free of DM or HF at baseline | Elevated HbA1c (≥5.5–6.0 %) was associated with incident HF |
| He et al. 2001 (NHANES I)[14] | Prospective cohort (19 years follow-up) | 13.643 subjects without HF | DM is an independent risk factor for HF (relative risk 1.85) |
| Boonman-de Winter et al. 2012[15] | Cross-sectional study | 605 patients with type 2 DM | HF (28 %) and left ventricular dysfunction (23 %) are highly prevalent in DM patients |
| Vasilliadis et al. 2014[8] | Cross-sectional | 200 HF patients | From HF subjects 27 % had type 2 DM and 10 % type 1 DM |
| Bertoni et al. 2004[16] | Prospective cohort study (5 years follow-up) | 151.000 DM subjects over 65 years old | The incidence rate of HF was estimated at 12.6 per 100 person-years |
ARIC = Atherosclerosis Risk in Community; DM = diabetes mellitus; HbA1c = glycated haemoglobin; HF = heart failure; NHANES I = First National Health and Nutrition Examination Survey Epidemiologic Follow-up Study; UKPDS = UK Prospective Diabetes Study.
Pathophysiological Connections
Despite the close relationship of these two conditions the difficulties in making a causal pathophysiological connection between DM and HF are formidable as we have to distinguish between insulin deficient and insulin resistant DM and between systolic HF, diastolic HF or HF caused by other aetiologies such as conduction disturbances, tachycardiomyopathy, HF of valvular aetiology, etc. (see Figure 1).
Figure 1: Schematic Depiction of the Bidirectional Relationship between Diabetes Mellitus and Heart Failure.
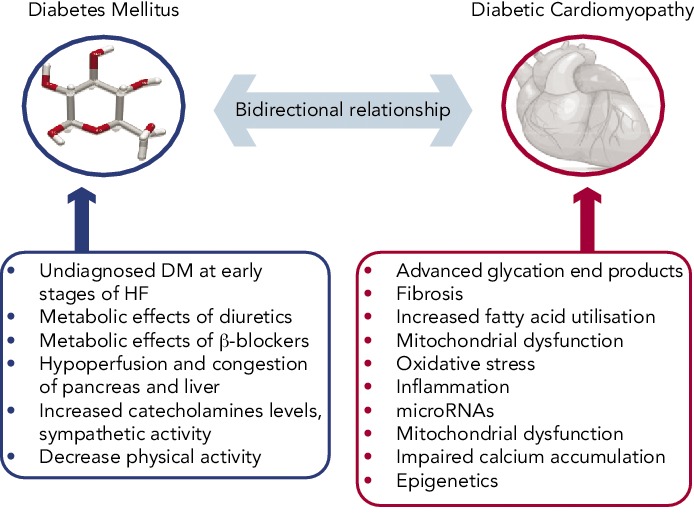
DM = diabetes mellitus; HF = heart failure.
Advanced glycation end products, which are formed in DM subjects after non-enzymatic reaction between protein and sugar residues, can possibly explain the link between DM and HF.[19] Advanced glycation end products are increased in patients with chronic HF, they correlate inversely with left ventricular ejection fraction and are related to the severity and prognosis of the disease.[20,21] Advanced glycation end products upregulate the hypertrophy-associated genes in cardiomyocytes via the activation of dendritic cells and may be responsible for the hypertrophic and fibrotic phenotype in DM subjects.[22]
A plethora of other mechanisms have also been proposed. Diabetes-related alterations in the expressions of some calcium-associated proteins may lead to progressive intracellular decay of calcium and in the development of diabetic cardiomyopathy.[23] In rats with diabetic cardiomyopathy there are also decreased serum and myocardial levels of adiponectin implying a possible connection between this anti-inflammatory protein and HF.[24] Hearts in humans with DM are characterised by increased fatty acid metabolism and oxidation, which is considered a pathophysiological mechanism in the development of HF.[25] Moreover, animal studies have revealed increased myocardial levels of cardiotoxic inflammatory cytokines (tumour necrosis factor-alpha, intereukin-6, etc.) in diabetic models.[26]
Hyperinsulinaemia also impairs phosphatidylinositol 3-kinases pathway and can precipitate myocardial dysfunction.[27] Furthermore, accumulation of reactive oxygen species affects the coronary circulation and causes myocardial hypertrophy and fibrosis.[28] Carbonic anhydrases have been shown to play a major role in diabetic microangiopathy. Recently, carbonic anhydrases I and II were found elevated in myocardial tissues from post-infarction HF patients with DM. They can induce cardiomyocyte hypertrophy and death in vitro, which are prevented by sodium-hydrogen exchanger-1 inhibition.[29] MicroRNAs are also differentially expressed in myocardial tissues from subjects with diabetic cardiomyopathy compared with non-diabetic HF, and specific patterns have been recognised.[30–32] These data may provide new targeted treatment of diabetic HF.
We also notice that diabetes frequently precedes coronary heart disease,[33] chronic kidney disease[34] and hypertension,[35] which are major risk factors and account for the majority of HF cases,[5] further explaining the close relationship between DM and HF observed in epidemiological studies.
Clinical and Epidemiological Connections
Further to pathophysiological connections, several clinical data have confirmed the detrimental impact of DM in HF course and prognosis. DM predicts readmissions of HF patients[36] and increases mortality in subjects with left ventricular dysfunction.[37] Elevated troponin levels in patients with DM are also associated with increased HF and cardiovascular mortality.[38] Recently, it was also confirmed that DM can be used in a model to predict chronic HF patients at risk of hospitalisation.[39] Moreover, in patients with type 2 DM, glycated haemoglobin significantly predicts future HF hospitalisation independently of baseline b-type natriuretic peptide (BNP) level or echocardiographic parameters.[40]
From Heart Failure to Diabetes Mellitus
The dual nature of the relationship of HF and DM is supported by prospective cohort studies. DM was developed in 29 % of HF subjects compared with 18 % of matched control subjects during a three-year follow-up study.[41] Moreover, in a cohort of 50.874 patients, HF severity (as determined by loop diuretic dosages) predicts the risk of developing diabetes after myocardial infarction.[42]
Nevertheless, the mechanisms precipitating DM and HF are not well-studied. Firstly, we have to notice the possibility that the increased incidence of DM during the course of HF may be an epiphenomenon of the lenient monitoring for impaired glucose metabolism, with glycated haemoglobin and with oral glucose tolerance tests in the early stages of HF. Accordingly, guidelines emphasise the importance of proper diagnosis of DM in HF subjects.[5]
We can also hypothesise that the decreased physical activity in HF patients may lead to decreased insulin sensitivity and to compensatory insulin requirements and hyperglycaemia. In addition, increased catecholamines levels and sympathetic activity stimulate gluconeogenesis and glycogenolysis.[43] Indeed, there is a decrease in insulin sensitivity according to New York Heart Association (NYHA) functional status of HF patients.[44]
Furthermore we can hypothesise that the haemodynamic consequences accompanying HF (decreased forward blood flow and increased central venous pressure) lead to hypoperfusion and congestion of the pancreas and liver, which may impair their ability to regulate metabolic homeostasis. Confirmatory data are provided by a recent study, which concludes that left ventricular assist devices improve blood glucose control in DM patients.[45]
Finally, we have to notice the possible adverse effects of established HF treatments, such as beta (β)-blockers and diuretics in blood glucose control.[46]
Diabetes Mellitus and Heart Failure Diagnosis
As HF diagnosis is based on the combination of clinical data and diagnostic tests, BNP levels can help to distinguish between cardiac and non-cardiac causes of acute dyspnoea in the emergency department.[47] BNP levels and reference limits can be affected by several factors such as age, obesity, renal impairment, etc.[48] Nevertheless, data from the Breathing Not Properly Multinational Trial suggest that diabetes status is not a confounding variable to be considered when interpreting BNP concentrations in patients who present acutely with dyspnoea.[47] However, in asymptomatic diabetic patients there was no significant difference among non-HF patients, HF patients and those with a HF history,[49] and no conclusions could be rendered as to the role of BNP testing for screening asymptomatic diabetic patients for left ventricular dysfunction because the degree of disease severity among the diabetic patients could not be assessed. Therefore, in the diagnostic work-up of diabetic patients presented not emergently in primary care centres, we must follow the diagnostic algorithm proposed by the guidelines, which emphasises that patients with high pre-test likelihood of HF may be referred directly for echocardiography.[5]
Moreover, clinicians should not overlook that DM patients with stable coronary heart disease may present with atypical symptoms, such as shortness of breath. Accordingly, we must be cautious in the interpretation of dyspnoea in these patients.[50]
Management of Heart Failure and Diabetes Mellitus
As both entities (HF and DM) are characterised by high morbidity and mortality, efforts for the best possible management must be taken. Nevertheless, treatment of HF may adversely interact with DM and vice versa (see Tables 2 and 3).
Table 2: Key Points in the Management of Heart Failure in Patients with Diabetes Mellitus.
| Diuretics | |
| β-blockers | |
| Mineralocorticoid receptor antagonists |
|
DM = diabetes mellitus; EPHESUS = Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study; MERIT HF = Metoprolol Randomized Intervention Trial in Congestive Heart Failure.
Table 3: Key Points in the Management of Diabetes Mellitus in Patients with Heart Failure.
|
|
| Thiazolidinediones |
|
|
|
| Incretins | |
|
|
| Metformin | |
| Sulphonylureas |
|
| Insulin |
|
DM = diabetes mellitus; HbA1c = glycated haemoglobin; HF = heart failure; PRAPγ = peroxisome proliferator-activated receptor gamma.
Heart Failure Treatment – Interaction with Diabetes Mellitus
Diuretics
Diuretics, especially furosemide, are one of the most useful treatments in HF patients for symptom relief and are used to achieve euvolaemia.[5] Data from studies and meta-analyses (mostly in hypertensive subjects) suggest an association between incident diabetes and diuretics.[46] Hypokalaemia, changes in autonomic nervous system function, in beta (β)-cell insulin release and in insulin’s peripheral effects are the proposed mechanisms.[51,68] Accordingly, in HF patients under diuretic treatment attention to keep potassium levels and glycaemic status under control must be attained. Thiazides have been shown to promote hyperglycaemia and loop diuretics may be better tolerated in DM patients.[52]
Beta-blockers
Beta (β)-blockers especially when they are combined with diuretics can precipitate DM.[46] Newer β-blockers with vasodilating actions, such as carvedilol and nebivolol, are less metabolic effective compared with metoprolol, do not affect glycaemic control and improve some components of the metabolic syndrome through improvement of the oxidative stress, insulin sensitivity and adiponectin levels.[53,54]. Vasodilating b-blockers increase survival in HF patients[5] and should be preferred in patients with DM. Another β-blocker that can improve survival and symptoms in HF is metoprolol. Although it adversely affects insulin sensitivity, the Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure (MERIT-HF) trial has shown that it can reduce mortality and HF symptoms similar to DM and non-DM patients.[55] A recent prospective study in HF patients with DM also concluded that metoprolol is highly safe and tolerable, and can remarkably improve the clinical status of the patients.[69]
Mineralocorticoid Receptor Antagonists
Eplerenone is a novel minelarocorticoid receptor antagonist, which is useful in HF patients. Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study (EPHESUS) in patients after acute myocardial infarction, ejection fraction <40 % and DM revealed that eplerenone on top of angiotensin-converting enzyme inhibitors or angiotensin receptor blockers can decrease mortality.[56] As renal dysfunction frequently co-exists with DM and HF,[70] attention to renal function and hyperkalaemia must be applied when the combination of eplerenone and angiotensin-converting enzyme inhibitors or angiotensin receptor blockers are used.
Diabetes Mellitus Treatment – Interaction with Heart Failure
Glycaemic control is of importance in DM subjects with HF as it is supposed to decrease free fatty acid oxidation by myocardial cells and increase the use of glucose as a substrate for metabolic requirements.[57] Nevertheless, attention must be given to the results of the Action in Diabetes and Vascular Disease: Preterax and Diamicron MR Controlled Evaluation (ADVANCE) and Action to Control Cardiovascular Risk in Diabetes (ACCORD) trials, which have shown that intensive treatment with a glycated haemoglobin target ≤6.5 % failed to influence macrovascular complications.[58,59] The glycaemic control can be achieved with glucose lowering drugs of different categories and it seems that there are differences in the way that they affect HF. Nevertheless, most data are based on observational studies. Randomised control trials exist only for thiazolidinediones.
Thiazolidinediones
Thiazolidinediones are peroxisome proliferator-activated receptor gamma (PRARγ) agonists, which can induce sodium retention and HF. This effect results from the increase in tubular sodium and water reabsorption in specific nephron segments or from stimulation of sodium reabsorption in the collecting duct.[60] Although PRARγ remains an attractive target for glycaemic control, thiazolidinediones’ clinical use is now limited and are avoided in patients with HF.[71] Nevertheless, several non-thiazolidinedione selective PPARγ modulators free of sodium retention are now tested in preclinical trials.[61]
Incretins
Glucagon-like peptide-1 (GLP-1) agonists and dipeptidyl peptidase-4 (DPP-4) inhibitors are a new class of anti-diabetic drugs. Except from their favourable effects in glycaemic control, preclinical data and early clinical reports support their clinical benefit in HF patients. GLP-1 increases cyclic adenosine monophosphate in cardiac myocytes but independently from a toxic increase in calcium levels and in myocytes xsxs.[72] Preclinical data in dogs and pigs with dilated cardiomyopathy have demonstrated that infusion of GLP-1 improves left ventricle function and stroke volume.[62,63] After myocardial infarction infusion of GLP-1, patients with left ventricle dysfunction showed improved ejection fraction and wall motion.[73] A non-randomised study in 12 HF patients concluded that chronic infusion of GLP-1 significantly improves left ventricular function, functional status and quality of life in patients with severe HF.[64] In contrast, Halbirk et al. concluded that 48 hours infusion of GLP-1 had no major cardiovascular effects in patients without diabetes but with compensated HF.[74] Taken together we can conclude that although there are no definite data on the impact of incretins in HF, early observations favour their use in HF subjects.
Other Glucose Lowering Treatment
The main concern regarding the use of metformin in HF patients despite their clinical benefits and the lower rates of mortality was the risk of lactic acidosis.[65] Novel data do not support this risk.[66,75] UK Prospective Diabetes Study (UKPDS) concluded that there was no difference between sulphonylureas and insulin treatment in cardiovascular complication,[66] while it seems that metformin compared with sulphonylureas decrease hospitalisations at least in some studies.[66,76] Regarding insulin treatment there are no reports that can affect HF status.[67]
Non-conventional Treatment of Diabetic Cardiomyopathy
Beyond the standard HF treatment, several novel approaches have been developed (see Table 4).
Table 4: Non-conventional and Experimental Treatment of Diabetic Cardiomyopathy.
| Superoxide dismutase | Transgenic mice with DM expressing cardiac specific superoxide dismutase have shown improvement in cardiac remodeling and left ventricle function[77] |
| Coenzyme Q10 | Effectively targets reactive oxygen species in diabetic mice and prevented effectively diabetic cardiomyopathy[78] |
| Phosphoinositide 3-kinase | In transgenic mice prevented diabetes-induced cardiomyopathy[79] |
| Omega-3 (n-3) polyunsaturated fatty acids | Improved ejection fraction in a rat model of DM[80] |
| B-type natriuretic peptide | Chronic treatment at low doses improved the metabolic profile and prevented the development of myocardial dysfunction in obese diabetic mice[81] |
| p38 MAPK | Inhibition of p38 MAPK by SB203580 (a pharmacological inhibitor) prevented cardiac inflammation and attenuated left ventricular dysfunction in a mouse model of diabetic cardiomyopathy[82] |
DM = diabetes mellitus; MAPK = mitogen-activated protein kinase.
Ex vivo studies support the notion that superoxide dismutase can offer protection from HF.[83] In vivo studies in transgenic DM mice expressing cardiac specific superoxide dismutase show improvement in cardiac remodeling and left ventricle function.[77]
Coenzyme Q10 is a potent antioxidant free of adverse effects, which can maintain cardiomyocyte and mitochondrial function. Recent preclinical data suggest that chronic supplementation with coenzyme Q10 can represent an effective approach for managing diabetic cardiomyopathy.[78,84] Phosphoinositide 3-kinase is a cardioprotective kinase, which when enhanced in transgenic mice can prevent diabetes-induced cardiomyopathy adverse cardiac remodeling and dysfunction.[79]
Interestingly, numerous, mostly preclinical, studies have shown that interventions such as omega-3 (n-3) polyunsaturated fatty acids can improve cardiac output and ejection fraction as well as stroke volume and stroke work in a rat model of DM.[80] This improvement may be mediated through attenuation of myocardial connexin-43 abnormalities. In contrast n-6 polyunsaturated fatty acids could accelerate myocardial abnormalities in diabetic rats.[85]
Conclusion
HF and DM frequently co-exist in a bidirectional relationship as it is proposed by pathophysiological and epidemiological data. At the moment several pathophysiological connections have been proposed but we cannot definitively conclude on the pathophysiological mechanisms precipitating this complex interaction. Both entities are characterised by high morbidity and mortality, and treatment must target the overall improvement as DM treatment can decompensate HF and vice versa. Novel therapeutic agents against diabetic cardiomyopathy are under investigation raising hopes for better management in the future.
References
- 1.Guariguata L, Whiting DR, Hambleton I et al. Global estimates of diabetes prevalence for 2013 and projections for 2035, Diabetes Res Clin Pract. 2014;103:137–49. doi: 10.1016/j.diabres.2013.11.002. [DOI] [PubMed] [Google Scholar]
- 2.Tousoulis D, Papageorgiou N, Androulakis E et al. Diabetes mellitus-associated vascular impairment: novel circulating biomarkers and therapeutic approaches, J Am Coll Cardiol. 2013;62:667–76. doi: 10.1016/j.jacc.2013.03.089. [DOI] [PubMed] [Google Scholar]
- 3.Barber SR, Davies MJ, Khunti K, Gray LJ. Risk assessment tools for detecting those with pre-diabetes: A systematic review, Diabetes Res Clin Pract. 2014;105(1):1–13. doi: 10.1016/j.diabres.2014.03.007. [DOI] [PubMed] [Google Scholar]
- 4.Strom Williams JL, Lynch CP, Winchester R et al. Gender Differences in Composite Control of Cardiovascular Risk Factors Among Patients with Type 2 Diabetes, Diabetes Technol Ther. 2014;16(7):421–7. doi: 10.1089/dia.2013.0329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.McMurray JJ, Adamopoulos S, Anker SD et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC, Eur Heart J. 2012;33:1787–847. doi: 10.1093/eurheartj/ehs104. [DOI] [PubMed] [Google Scholar]
- 6.Tousoulis D, Oikonomou E, Siasos G, Stefanadis C. Statins in heart failure-With preserved and reduced ejection fraction. An update, Pharmacol Ther. 2014;141:79–91. doi: 10.1016/j.pharmthera.2013.09.001. [DOI] [PubMed] [Google Scholar]
- 7.Tousoulis D, Oikonomou E, Siasos G et al. Predictive value of biomarkers in patients with heart failure, Curr Med Chem. 2012;19:2534–47. doi: 10.2174/092986712800492968. [DOI] [PubMed] [Google Scholar]
- 8.Vasiliadis I, Kolovou G, Kolovou V et al. Gene polymorphisms and thyroid function in patients with heart failure, Endocrine. 2014;45:46–54. doi: 10.1007/s12020-013-9926-x. [DOI] [PubMed] [Google Scholar]
- 9.Kannel WB, Hjortland M, Castelli WP. Role of diabetes in congestive heart failure: the Framingham study, Am J Cardiol. 1974;34:29–34. doi: 10.1016/0002-9149(74)90089-7. [DOI] [PubMed] [Google Scholar]
- 10.Nichols GA, Gullion CM, Koro CE et al. The incidence of congestive heart failure in type 2 diabetes: an update, Diabetes care. 2004;27:1879–84. doi: 10.2337/diacare.27.8.1879. [DOI] [PubMed] [Google Scholar]
- 11.Iribarren C, Karter AJ, Go AS et al. Glycemic control and heart failure among adult patients with diabetes, Circulation. 2001;103:2668–73. doi: 10.1161/01.cir.103.22.2668. [DOI] [PubMed] [Google Scholar]
- 12.Stratton IM, Adler AI, Neil HA et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study, BMJ. 2000;321:405–12. doi: 10.1136/bmj.321.7258.405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Matsushita K, Blecker S, Pazin-Filho A et al. The association of hemoglobin a1c with incident heart failure among people without diabetes: the atherosclerosis risk in communities study, Diabetes. 2010;59:2020–6. doi: 10.2337/db10-0165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.He J, Ogden LG, Bazzano LA et al. Risk factors for congestive heart failure in US men and women: NHANES I epidemiologic follow-up study, Arch Intern Med. 2001;161:996–1002. doi: 10.1001/archinte.161.7.996. [DOI] [PubMed] [Google Scholar]
- 15.Boonman-de Winter LJ, Rutten FH, Cramer MJ et al. High prevalence of previously unknown heart failure and left ventricular dysfunction in patients with type 2 diabetes, Diabetologia. 2012;55:2154–62. doi: 10.1007/s00125-012-2579-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bertoni AG, Hundley WG, Massing MW et al. Heart failure prevalence, incidence, and mortality in the elderly with diabetes, Diabetes care. 2004;27:699–703. doi: 10.2337/diacare.27.3.699. [DOI] [PubMed] [Google Scholar]
- 17.Yancy CW, Jessup M, Bozkurt B et al. 2013 ACCF/AHA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines, Circulation. 2013;128:1810–52. doi: 10.1161/CIR.0b013e31829e8807. [DOI] [PubMed] [Google Scholar]
- 18.Rutter MK, Parise H, Benjamin EJ et al. Impact of glucose intolerance and insulin resistance on cardiac structure and function: sex-related differences in the Framingham Heart Study, Circulation. 2003;107:448–54. doi: 10.1161/01.cir.0000045671.62860.98. [DOI] [PubMed] [Google Scholar]
- 19.Hartog JW, Voors AA, Bakker SJ et al. Advanced glycation end-products (AGEs) and heart failure: pathophysiology and clinical implications, Eur J Heart Fail. 2007;9:1146–55. doi: 10.1016/j.ejheart.2007.09.009. [DOI] [PubMed] [Google Scholar]
- 20.Hartog JW, Voors AA, Schalkwijk CG et al. Clinical and prognostic value of advanced glycation end-products in chronic heart failure, Eur Heart J. 2007;28:2879–85. doi: 10.1093/eurheartj/ehm486. [DOI] [PubMed] [Google Scholar]
- 21.Simm A, Wagner J, Gursinsky T et al. Advanced glycation endproducts: a biomarker for age as an outcome predictor after cardiac surgery?, Exp Gerontol. 2007;42:668–75. doi: 10.1016/j.exger.2007.03.006. [DOI] [PubMed] [Google Scholar]
- 22.Cao W, Chen J, Chen Y et al. Advanced glycation end products promote heart failure through inducing the immune maturation of dendritic cells, Appl Biochem Biotechnol. 2014;172:4062–77. doi: 10.1007/s12010-014-0804-7. [DOI] [PubMed] [Google Scholar]
- 23.Zhao SM, Wang YL, Guo CY et al. Progressive decay of Ca2+ homeostasis in the development of diabetic cardiomyopathy, Cardiovasc Diabetol. 2014;13:75. doi: 10.1186/1475-2840-13-75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Li J, Su S, Zong X. Analysis of the association between adiponectin, adiponectin receptor 1 and diabetic cardiomyopathy, Exp Ther Med. 2014;7:1023–7. doi: 10.3892/etm.2014.1539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Bugger H, Boudina S, Hu XX et al. Type 1 diabetic akita mouse hearts are insulin sensitive but manifest structurally abnormal mitochondria that remain coupled despite increased uncoupling protein 3, Diabetes. 2008;57:2924–32. doi: 10.2337/db08-0079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Tschope C, Walther T, Escher F et al. Transgenic activation of the kallikrein-kinin system inhibits intramyocardial inflammation, endothelial dysfunction and oxidative stress in experimental diabetic cardiomyopathy, FASEB J. 2005;19:2057–9. doi: 10.1096/fj.05-4095fje. [DOI] [PubMed] [Google Scholar]
- 27.Poornima IG Parikh P, Shannon RP. Diabetic cardiomyopathy: the search for a unifying hypothesis, Circ Res. 2006;98:596–605. doi: 10.1161/01.RES.0000207406.94146.c2. [DOI] [PubMed] [Google Scholar]
- 28.Clark RJ, McDonough PM, Swanson E et al. Diabetes and the accompanying hyperglycemia impairs cardiomyocyte calcium cycling through increased nuclear O-GlcNAcylation, J Biol Chem. 2003;278:44230–7. doi: 10.1074/jbc.M303810200. [DOI] [PubMed] [Google Scholar]
- 29.Torella D, Ellison GM, Torella M et al. Carbonic anhydrase activation is associated with worsened pathological remodeling in human ischemic diabetic cardiomyopathy, J Am Heart Assoc. 2014;3(2):e000434. doi: 10.1161/JAHA.113.000434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Greco S, Fasanaro P, Castelvecchio S et al. MicroRNA dysregulation in diabetic ischemic heart failure patients, Diabetes. 2012;61:1633–41. doi: 10.2337/db11-0952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Briasoulis A, Tousoulis D, Vogiatzi G et al. MicroRNAs: Biomarkers for cardiovascular disease in patients with diabetes mellitus, Curr Top Med Chem. 2013;13:1533–9. doi: 10.2174/15680266113139990102. [DOI] [PubMed] [Google Scholar]
- 32.Oikonomou E, Siasos G, Tousoulis D et al. Diagnostic and therapeutic potentials of microRNAs in heart failure, Curr Top Med Chem. 2013;13:1548–58. doi: 10.2174/15680266113139990104. [DOI] [PubMed] [Google Scholar]
- 33.Swindle JP, Ye X, Mallick R et al. Colesevelam, Ezetimibe, and Patients With Type 2 Diabetes Mellitus: Characteristics and Clinical Outcomes From a Health Care Database, Ann Pharmacother. 2014;48(7):847–55. doi: 10.1177/1060028014531737. [DOI] [PubMed] [Google Scholar]
- 34.Afsar B, Turkmen K, Covic A et al. An Update on Coronary Artery Disease and Chronic Kidney Disease, Int J Nephrol. 2014;2014:767424. doi: 10.1155/2014/767424. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Toyama M, Watanabe S, Miyauchi T et al. Diabetes and obesity are significant risk factors for morning hypertension: From Ibaraki Hypertension Assessment Trial (I-HAT), Life Sci. 2014;104(1-2):32–7. doi: 10.1016/j.lfs.2014.03.029. [DOI] [PubMed] [Google Scholar]
- 36.Krumholz HM, Chen YT, Wang Y et al. Predictors of readmission among elderly survivors of admission with heart failure, Am Heart J. 2000;139:72–7. doi: 10.1016/s0002-8703(00)90311-9. [DOI] [PubMed] [Google Scholar]
- 37.Shindler DM, Kostis JB, Yusuf S et al. Diabetes mellitus, a predictor of morbidity and mortality in the Studies of Left Ventricular Dysfunction (SOLVD) Trials and Registry, Am J Cardiol. 1996;77:1017–20. doi: 10.1016/s0002-9149(97)89163-1. [DOI] [PubMed] [Google Scholar]
- 38.Yiu KH, Lau KK, Zhao CT et al. Predictive value of high-sensitivity troponin-I for future adverse cardiovascular outcome in stable patients with type 2 diabetes mellitus, Cardiovasc Diabetol. 2014;13:63. doi: 10.1186/1475-2840-13-63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Cubbon RM, Woolston A, Adams B et al. Prospective development and validation of a model to predict heart failure hospitalisation, Heart. 2014;100:923–9. doi: 10.1136/heartjnl-2013-305294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Kishimoto I, Makino H, Ohata Y et al. Hemoglobin A1c predicts heart failure hospitalization independent of baseline cardiac function or B-type natriuretic peptide level, Diabetes Res Clin Pract. 2014;104(2):257–65. doi: 10.1016/j.diabres.2014.02.009. [DOI] [PubMed] [Google Scholar]
- 41.Amato L, Paolisso G, Cacciatore F et al. Congestive heart failure predicts the development of non-insulin-dependent diabetes mellitus in the elderly. The Osservatorio Geriatrico Regione Campania Group, Diabetes Metab. 1997;23:213–8. [PubMed] [Google Scholar]
- 42.Andersson C, Norgaard ML, Hansen PR et al. Heart failure severity, as determined by loop diuretic dosages, predicts the risk of developing diabetes after myocardial infarction: a nationwide cohort study, Eur J Heart Fail. 2010;12:1333–8. doi: 10.1093/eurjhf/hfq160. [DOI] [PubMed] [Google Scholar]
- 43.Heck PM, Dutka DP. Insulin resistance and heart failure, Curr Heart Fail Rep. 2009;6:89–94. doi: 10.1007/s11897-009-0014-8. [DOI] [PubMed] [Google Scholar]
- 44.Doehner W, Rauchhaus M, Ponikowski P et al. Impaired insulin sensitivity as an independent risk factor for mortality in patients with stable chronic heart failure, J Am Coll Cardiol. 2005;46:1019–26. doi: 10.1016/j.jacc.2005.02.093. [DOI] [PubMed] [Google Scholar]
- 45.Guglin M, Maguire K, Missimer T et al. Improvement in Blood Glucose Control in Patients with Diabetes after Implantation of Left Ventricular Assist Devices, ASAIO J. 2014;60(3):290–3. doi: 10.1097/MAT.0000000000000064. [DOI] [PubMed] [Google Scholar]
- 46.Elliott WJ, Meyer PM. Incident diabetes in clinical trials of antihypertensive drugs: a network meta-analysis, Lancet. 2007;369:201–7. doi: 10.1016/S0140-6736(07)60108-1. [DOI] [PubMed] [Google Scholar]
- 47.Maisel AS, Krishnaswamy P, Nowak RM et al. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure, N Engl J Med. 2002;347:161–7. doi: 10.1056/NEJMoa020233. [DOI] [PubMed] [Google Scholar]
- 48.Koizumi M, Watanabe H, Kaneko Y et al. Impact of obesity on plasma B-type natriuretic peptide levels in Japanese community-based subjects, Heart Vessels. 2012;27:287–94. doi: 10.1007/s00380-011-0143-3. [DOI] [PubMed] [Google Scholar]
- 49.Wu AH, Omland T, Duc P et al. The effect of diabetes on B-type natriuretic peptide concentrations in patients with acute dyspnea: an analysis from the Breathing Not Properly Multinational Study, Diabetes care. 2004;27:2398–404. doi: 10.2337/diacare.27.10.2398. [DOI] [PubMed] [Google Scholar]
- 50.Montalescot G, Sechtem U, Achenbach S et al. 2013 ESC guidelines on the management of stable coronary artery disease: the Task Force on the management of stable coronary artery disease of the European Society of Cardiology, Eur Heart J, 2013;34:2949–3003. doi: 10.1093/eurheartj/eht296. [DOI] [PubMed] [Google Scholar]
- 51.Opie LH, Schall R. Old antihypertensives and new diabetes, J Hypertens. 2004;22:1453–8. doi: 10.1097/01.hjh.0000133732.24501.9e. [DOI] [PubMed] [Google Scholar]
- 52.Rydén L, Grant PJ, Anker SD et al. ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD: the Task Force on diabetes, pre-diabetes, and cardiovascular diseases of the European Society of Cardiology (ESC) and developed in collaboration with the European Association for the Study of Diabetes (EASD), Eur Heart J. 2013;34:3035–87. doi: 10.1093/eurheartj/eht108. [DOI] [PubMed] [Google Scholar]
- 53.Celik T, Iyisoy A, Kursaklioglu H et al. Comparative effects of nebivolol and metoprolol on oxidative stress, insulin resistance, plasma adiponectin and soluble P-selectin levels in hypertensive patients, J Hypertens. 2006;24:591–6. doi: 10.1097/01.hjh.0000209993.26057.de. [DOI] [PubMed] [Google Scholar]
- 54.Bakris GL, Fonseca V, Katholi RE et al. Metabolic effects of carvedilol vs metoprolol in patients with type 2 diabetes mellitus and hypertension: a randomized controlled trial, JAMA. 2004;292:2227–36. doi: 10.1001/jama.292.18.2227. [DOI] [PubMed] [Google Scholar]
- 55.Deedwania PC, Giles TD, Klibaner M et al. Efficacy, safety and tolerability of metoprolol CR/XL in patients with diabetes and chronic heart failure: experiences from MERIT-HF, Am Heart J. 2005;149:159–67. doi: 10.1016/j.ahj.2004.05.056. [DOI] [PubMed] [Google Scholar]
- 56.Pitt B, Remme W, Zannad F et al. Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction, N Engl J Med. 2003;348:1309–21. doi: 10.1056/NEJMoa030207. [DOI] [PubMed] [Google Scholar]
- 57.Malmberg K, Rydén L, Hamsten A et al. Effects of insulin treatment on cause-specific one-year mortality and morbidity in diabetic patients with acute myocardial infarction. DIGAMI Study Group. Diabetes Insulin-Glucose in Acute Myocardial Infarction, Eur Heart J. 1996;17:1337–44. doi: 10.1093/oxfordjournals.eurheartj.a015067. [DOI] [PubMed] [Google Scholar]
- 58.Gerstein HC, Miller ME, Byington RP et al. Effects of intensive glucose lowering in type 2 diabetes, N Engl J Med. 2008;358:2545–59. doi: 10.1056/NEJMoa0802743. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Patel A, MacMahon S, Chalmers J et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes, N Engl J Med. 2008;358:2560–72. doi: 10.1056/NEJMoa0802987. [DOI] [PubMed] [Google Scholar]
- 60.Beltowski J, Rachanczyk J, Wlodarczyk M. Thiazolidinedione-induced fluid retention: recent insights into the molecular mechanisms, PPAR Res. 2013;2013:628628. doi: 10.1155/2013/628628. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Agrawal R, Jain P, Dikshit SN. Balaglitazone: a second generation peroxisome proliferator-activated receptor (PPAR) gamma (gamma) agonist, Mini Rev Med Chem. 2012;12:87–97. doi: 10.2174/138955712798995048. [DOI] [PubMed] [Google Scholar]
- 62.Nikolaidis LA, Elahi D, Hentosz T et al. Recombinant glucagon-like peptide-1 increases myocardial glucose uptake and improves left ventricular performance in conscious dogs with pacing-induced dilated cardiomyopathy, Circulation. 2004;110:955–61. doi: 10.1161/01.CIR.0000139339.85840.DD. [DOI] [PubMed] [Google Scholar]
- 63.Gomez N, Touihri K, Matheeussen V et al. Dipeptidyl peptidase IV inhibition improves cardiorenal function in overpacing-induced heart failure, Eur J Heart Fail. 2012;14:14–21. doi: 10.1093/eurjhf/hfr146. [DOI] [PubMed] [Google Scholar]
- 64.Sokos GG, Nikolaidis LA, Mankad S et al. Glucagon-like peptide-1 infusion improves left ventricular ejection fraction and functional status in patients with chronic heart failure, J Card Fail. 2006;12:694–9. doi: 10.1016/j.cardfail.2006.08.211. [DOI] [PubMed] [Google Scholar]
- 65.Aguilar D, Chan W, Bozkurt B et al. Metformin use and mortality in ambulatory patients with diabetes and heart failure, Circ Heart Fail. 2011;4:53–8. doi: 10.1161/CIRCHEARTFAILURE.110.952556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Masoudi FA, Inzucchi SE, Wang Y et al. Thiazolidinediones, metformin, and outcomes in older patients with diabetes and heart failure: an observational study, Circulation. 2005;111:583–90. doi: 10.1161/01.CIR.0000154542.13412.B1. [DOI] [PubMed] [Google Scholar]
- 67.Gerstein HC, Bosch J, Dagenais GR et al. Basal insulin and cardiovascular and other outcomes in dysglycemia, N Engl J Med. 2012;367:319–28. doi: 10.1056/NEJMoa1203858. [DOI] [PubMed] [Google Scholar]
- 68.Luna B, Feinglos MN. Drug-induced hyperglycemia, JAMA. 2001;286:1945–8. doi: 10.1001/jama.286.16.1945. [DOI] [PubMed] [Google Scholar]
- 69.Liu X, Zhong C, Zhao P et al. Analysis of therapeutic effect and safety of target-dose metoprolol in the treatment of patients with diabetes mellitus with chronic heart failure, Pak J Med Sci. 2014;30:7–11. doi: 10.12669/pjms.301.3908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Culic V, Busic Z. Severity of acute heart failure in men according to diabetes mellitus: the role of testosterone and renal dysfunction, Int J Cardiol. 2013;168:5039–41. doi: 10.1016/j.ijcard.2013.07.220. [DOI] [PubMed] [Google Scholar]
- 71.Home PD, Pocock SJ, Beck-Nielsen H et al. Rosiglitazone evaluated for cardiovascular outcomes--an interim analysis, N Engl J Med. 2007;357:28–38. doi: 10.1056/NEJMoa073394. [DOI] [PubMed] [Google Scholar]
- 72.Vila Petroff MG, Egan JM, Wang X, Sollott SJ. Glucagon-like peptide-1 increases cAMP but fails to augment contraction in adult rat cardiac myocytes, Circ Res. 2001;89:445–52. doi: 10.1161/hh1701.095716. [DOI] [PubMed] [Google Scholar]
- 73.Lønborg J, Vejlstrup N, Kelbaek H et al. Exenatide reduces reperfusion injury in patients with ST-segment elevation myocardial infarction, Eur Heart J. 2012;33:1491–9. doi: 10.1093/eurheartj/ehr309. [DOI] [PubMed] [Google Scholar]
- 74.Halbirk M, Nørrelund H, Møller N et al. Cardiovascular and metabolic effects of 48-h glucagon-like peptide-1 infusion in compensated chronic patients with heart failure, Am J Physiol Heart Circ Physiol. 2010;298:H1096–102. doi: 10.1152/ajpheart.00930.2009. [DOI] [PubMed] [Google Scholar]
- 75.Tousoulis D, Koniari K, Antoniades C et al. Combined effects of atorvastatin and metformin on glucose-induced variations of inflammatory process in patients with diabetes mellitus, Int J Cardiol. 2011;149:46–9. doi: 10.1016/j.ijcard.2009.11.038. [DOI] [PubMed] [Google Scholar]
- 76.Eurich DT, Majumdar SR, McAlister FA et al. Improved clinical outcomes associated with metformin in patients with diabetes and heart failure, Diabetes Care. 2005;28:2345–51. doi: 10.2337/diacare.28.10.2345. [DOI] [PubMed] [Google Scholar]
- 77.Shen X, Zheng S, Metreveli NS, Epstein PN. Protection of cardiac mitochondria by overexpression of MnSOD reduces diabetic cardiomyopathy, Diabetes. 2006;55:798–805. doi: 10.2337/diabetes.55.03.06.db05-1039. [DOI] [PubMed] [Google Scholar]
- 78.Huynh K, Kiriazis H, Du XJ et al. Targeting the upregulation of reactive oxygen species subsequent to hyperglycemia prevents type 1 diabetic cardiomyopathy in mice, Free Radic Biol Med. 2013;60:307–17. doi: 10.1016/j.freeradbiomed.2013.02.021. [DOI] [PubMed] [Google Scholar]
- 79.Ritchie RH, Love JE, Huynh K et al. Enhanced phosphoinositide 3-kinase(p110alpha) activity prevents diabetes-induced cardiomyopathy and superoxide generation in a mouse model of diabetes, Diabetologia. 2012;55:3369–81. doi: 10.1007/s00125-012-2720-0. [DOI] [PubMed] [Google Scholar]
- 80.Anna Z, Angela S, Barbara B et al. Heart-protective effect of n-3 PUFA demonstrated in a rat model of diabetic cardiomyopathy, Mol Cell Biochem. 2014;389:219–27. doi: 10.1007/s11010-013-1943-9. [DOI] [PubMed] [Google Scholar]
- 81.Plante E, Menaouar A, Danalache BA et al. Treatment with brain natriuretic peptide prevents the development of cardiac dysfunction in obese diabetic db/db mice, Diabetologia. 2014;57(6):1257–67. doi: 10.1007/s00125-014-3201-4. [DOI] [PubMed] [Google Scholar]
- 82.Westermann D, Rutschow S, Van Linthout S et al. Inhibition of p38 mitogen-activated protein kinase attenuates left ventricular dysfunction by mediating pro-inflammatory cardiac cytokine levels in a mouse model of diabetes mellitus, Diabetologia. 2006;49:2507–13. doi: 10.1007/s00125-006-0385-2. [DOI] [PubMed] [Google Scholar]
- 83.Salvemini D, Riley DP, Cuzzocrea S. SOD mimetics are coming of age, Nat Rev Drug Discov. 2002;1:367–74. doi: 10.1038/nrd796. [DOI] [PubMed] [Google Scholar]
- 84.Huynh K, Kiriazis H, Du XJ et al. Coenzyme Q10 attenuates diastolic dysfunction, cardiomyocyte hypertrophy and cardiac fibrosis in the db/db mouse model of type 2 diabetes, Diabetologia. 2012;55:1544–53. doi: 10.1007/s00125-012-2495-3. [DOI] [PubMed] [Google Scholar]
- 85.Ghosh S, Qi D, An D et al. Brief episode of STZ-induced hyperglycemia produces cardiac abnormalities in rats fed a diet rich in n-6 PUFA, Am J Physiol Heart Circ Physiol. 2004;287:H2518–27. doi: 10.1152/ajpheart.00480.2004. [DOI] [PubMed] [Google Scholar]