

Abstract
Introduction
In Turkey, scuba diving has become more popular and accessible in the past decade and there has been a commensurate rise in the number of certified divers. This new generation of recreational divers has not been described in detail previously. The aim of this study was to profile this group, while investigating any gender differences and making comparisons with the global diving community.
Methods
Turkish dive club members and diving forum/blog readers were invited to complete an online questionnaire investigating their demography, medical issues and diving history and habits.
Results
The questionnaire was completed by 303 female and 363 male divers. Significant differences were found between the sexes in terms of demographics, diving experience and attitudes toward safety. Previous or ongoing medical conditions were reported by 100 female divers and 141 males. Only 29% of females and 22% of males had been examined by a physician trained to conduct assessments of fitness to dive. Female divers did not report problems while diving during menstruation or while taking oral contraceptives. There was no significant difference in the occurrence of decompression sickness (DCS) and DCS-like symptoms between the sexes.
Conclusions
This is the largest study to date conducted on recreational divers in Turkey and so carries some value. It profiles their physical and behavioral attributes as well as differences in diving practices between the sexes in Turkey. Our findings should have implications for medical screening and dive training standards.
Keywords: Scuba diving, Sex, Medical conditions, Decompression sickness, Menstruation, Pregnancy, Survey
Introduction
Scuba diving is a popular recreational pursuit. In the USA, it is estimated that 3,145,000 divers made at least 9,396,000 dives in 2015 alone.[ 1] According to PADI statistics, approximately 900,000 divers are certified each year.[ 2] In countries like the UK and Australia, where diving has a long-standing background, many studies on diver demographics, behaviour and accident analyses have been published.[ 3 , 4]
In Turkey, however, scuba diving has become popular in only the past decade. The number of beginner divers is currently more than 5,000 per year, whereas before 2005, it was in the hundreds only.[ 5] According to the Turkish Underwater Sports Federation's (TSSF) 2014 records, the number of certified divers has increased from 66,283 to 101,377 since 2010.[ 6] This 'new' group of recreational divers has not been studied before so, given the increasing number of participants, a report seemed timely. Females account for a large part of this increase in the diver population. Currently, 21% of certified divers in Turkey are females, whereas they made up only 8% in 2000.[ 5] Worldwide, females are reported to make up 28% of all recreational divers, so the proportional increase of female divers in Turkey is starting to come into line with the global trend.[ 7] This raises questions about sex differences and susceptibility to diving-related diseases, but studies on the topic are limited.[ 8 , 9] Also, any differences in diving behaviour and safety between the sexes are of interest. We aimed to profile Turkish divers, particularly this younger group, their demographics, diving habits, health status, attitudes toward diving safety and any difference between the sexes, while comparing them with other 'experienced' diving communities and their practices.
Methods
The study was approved by the Institutional Review Board of Istanbul University, Istanbul Faculty of Medicine, Turkey. From the 01 May until 16 June 2010, a web link for a Turkish language online questionnaire (80 questions), which took about 20 minutes to complete, was sent to dive club members and posted on internet blogs and diving forums in Turkey. Information regarding the aim of the questionnaire and use of the results were provided with the link. The questionnaire was anonymous but nicknames were requested to eliminate duplicates. It was possible to leave the questionnaire at any point and unless participants saved it at the end, a record was not generated.
The first part of the survey investigated diver demography, asking questions on anthropometric characteristics, occupation, education, family and medical background. All of these questions allowed the responders to reply descriptively, apart from two on alcohol and tobacco use that required yes/no responses. The second part aimed to collect data on diving history and diving habits, including years diving, number of dives, diving experience and training. They were also asked about diving beyond the safe recreational limits advised by their tables/dive computers. The third part of the survey addressed current health status including chronic diseases, medications, and decompression sickness (DCS) and other diving-related diseases. A DCS episode diagnosed by a physician and treated in a recompression chamber was defined as confirmed DCS. Numbness, extremity weakness, tingling, paraesthesia and pain after a dive were accepted as DCS-like symptoms. Most of the questions in this section required yes/no answers, although some invited descriptive answers. An additional section to be completed by diving instructors included their instructing history, how they trained and differences in their approach to female and male divers. After one and a half months of the questionnaire being live, the data were collected and evaluated. The records were reviewed for duplicates and incomplete answers. Replies that had more than five answers missing were excluded.
ANALYSIS
All demographic data were expressed as mean (± standard deviation) or percentages, as appropriate; categorized data were given as percentages. Statistical analyses were performed with Medcalc® for Windows (version 11.2.1.0). Simple z-test and 'N-1' chi-squared tests were used to compare proportions. Student's t-test was used to compare paired values. Significance was accepted at P < 0.05.
Results
Upon initial examination, 317 female divers and 381 male divers supplied responses. Records were scrutinized for completion and duplication, with 27 failing to fulfill completion criteria and five being duplicates. A total of 666 records, 303 female and 363 male, were analyzed. The mean age of females was 32 ± 8 years (range: 19–59) and for males was 36 ± 10 (range: 15–67). Males were significantly older than females (P < 0.001). Mean body mass index (BMI, kg·m⁻²) was 22 for female and 26 for males. Eight female and forty-three male divers had a BMI ≥30, categorizing them as obese. The distribution of BMI is given in Table 1.
Table 1. Body mass index (BMI, kg·m⁻²) of 303 female and 363 male Turkish recreational divers responding to the survey; number and percentage shown.
| Female divers | Male divers | P-value | |
| BMI < 25 | 264 (87) | 139 (38) | < 0.0001 |
| BMI 25–25.9 | 31 (10) | 181 (50) | < 0.0001 |
| BMI 30−34.9 | 4 (1.3) | 33 (9) | < 0.0001 |
| BMI > 35 | 4 (1.3) | 10 (3) | 0.14 |
DIVING HISTORY
All divers replied to the question about diving certification (Figure 1). Details about diving history are given in Table 2; 17% of females and 9% of males had 20 or fewer dives. The total number of dives reported by females was 65,311 and 239,772 for males. (P < 0.0001). Males completed a significantly higher mean number of dives than females per year (61 ± 75 vs 35 ± 54, P < 0.0001).
Figure 1.
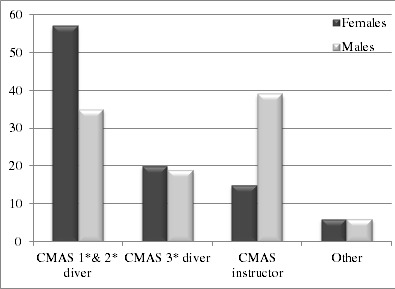
Diving certification level of 303 female and 363 male Turkish recreational divers responding to the survey (percentages shown)
Table 2. Diving history of 303 female and 363 male Turkish divers responding to the survey; n = number of respondents answering the question.
| Female divers | Male divers | |||||||
| n | Mean | (SD) | Range | n | Mean | (SD) | Range | |
| Years diving | 290 | 5.9 | (4.4) | 2−25 | 351 | 10 | (8.1) | 3–48 |
| Total dives | 271 | 241 | (566) | 4−6000 | 318 | 754 | (1306) | 3−9000 |
| Maximum depth (m) | 290 | 39.9 | (14.3) | 8−89 | 354 | 48.6 | (17.7) | 8−137 |
Diving behaviour is described in Table 3. Sixty-seven per cent of females (n = 204) and 81% of males (n = 294) declared they regularly made a safety stop, but only 57% of the females (n = 173) and 63% of males (n = 203) defined it as the 'industry standard' safety stop of 3−5 min at 3−6 metres' sea water (msw). Forty per cent of females (n = 121) and 62% of males (n = 225) reported using a dive computer to plan their dives.
Table 3. Diving behaviour of 303 female and 363 male Turkish recreational divers responding to the survey (number of respondents and percentage shown).
| Female divers | Male divers | ||||
| n | % | n | % | P-value | |
| Safety stop | |||||
| Always | 204 | (67) | 294 | (81) | < 0.0001 |
| No response | 74 | (24) | 45 | (12) | |
| Decompression diving | |||||
| Yes | 127 | (42) | 213 | (59) | < 0.0001 |
| No | 57 | (19) | 56 | (15) | |
| No response | 119 | (39) | 94 | (26) | |
| Diving deeper than 30 m | |||||
| Yes | 201 | (66) | 284 | (78) | 0.0006 |
| No | 35 | (12) | 31 | (9) | |
| No response | 67 | (22) | 48 | (13) | |
| Diving deeper than 42 m | |||||
| Yes | 116 | (38) | 248 | (68) | < 0.0001 |
| No | 174 | (57) | 106 | (29) | |
| No response | 13 | (4) | 9 | (3) | |
| Diving deeper than 55 m | |||||
| Yes | 32 | (66) | 284 | (78) | < 0.0001 |
| No | 258 | (85) | 234 | (64) | |
| No response | 13 | (4) | 9 | (3) | |
Forty-two per cent of the female divers (n = 127) and 59% of males (n = 213, P < 0.001) reported that they performed dives that required decompression stops. However, almost as many females did not reply to the question. Sixty-six per cent of female (n = 201) and 78% (n = 284) of male divers did not adhere to the recreational diving depth limit, 30 msw in Turkey (P = 0.0006).10 Moreover, another 11% (n = 32) of female divers reported diving deeper than 55 msw, which is the limit for professional divers (with air) in Turkey.[ 11]
HEALTH ISSUES
Similar numbers of female and male divers were smokers (35% and 34% respectively). Ninety per cent of female and 84% of male divers reported that they consumed alcohol occasionally. Almost half of the females (n = 148) did or would do so within 12 hours of diving, compared to 61% (n = 220) of the male respondents (P = 0.002).
Thirty-three per cent of females (n = 100) and 39% of males (n = 141) reported having an ongoing medical condition or having experienced one. For both sexes, the three most common medical conditions were ear, nose and throat problems, previous trauma and spinal disc herniation. Of the females, one reported having hypertension (HT) and hypercholesterolemia, one reported diabetes mellitus (DM) and HT, two reported cardiac problems (arrhythmia and rheumatic valve insufficiency) and one had hypoglycaemia. One female reported manic depression and had been evaluated by a general practitioner for diving. Of the male respondents, HT, DM or hypercholesterolemia were reported by five males, three of whom had two of these conditions at the same time. Three reported cardiac problems; previous surgery for aortic coarctation, arrhythmia and mitral valve prolapse. One male had a history of tuberculosis but had not been assessed for diving by a physician.
Only 55% female and 53% male respondents indicated they had undertaken a medical assessment for diving at least once. Twenty-nine per cent of females and 39% of males had been examined by a physician trained to conduct assessments of fitness to dive. Twenty per cent of females (n = 60) and 31% of males (n = 111) went for repeated medical examinations. Of these, 23 females and 77 males were instructors, so were obliged to do so. Details about health issues and diving-related diseases are given in Table 4.
Table 4. Health issues and diving related accidents in 303 female and 363 male Turkish recreational divers responding to the survey (number of respondents and percentage shown).
| Female divers | Male divers | ||||
| n | % | n | % | ||
| Smoker | 105 | (35) | 122 | (34) | |
| Alcohol | |||||
| Occasional drinker | 274 | (90) | 306 | (84) | |
| Never | 27 | (9) | 43 | (12) | |
| Alcohol pre-dive | 148 | (49) | 220 | (61) | |
| Exercise regularly | 45 | (15) | 47 | (13) | |
| Medical assessment | |||||
| Only before training | 168 | (55) | 193 | (53) | |
| Regularly | 63 | (21) | 50 | (14) | |
| No response | 12 | (4) | 9 | (2) | |
| Assessment by | |||||
| Diving physician | 89 | (29) | 143 | (39) | |
| Other (GP or specialist) | 133 | (44) | 155 | (43) | |
| No response | 81 | (27) | 65 | (18) | |
| DCS | |||||
| Signs of DCS | 3 | (1) | 11 | (3) | |
| Treated DCS | 1 | (0.3) | 4 | (1) | |
| Other | |||||
| Non-DCS trauma | 15 | (5) | 27 | (7) | |
| Barotrauma | 8 | (3) | 13 | (4) | |
| Hip/shoulder pain | 11 | (4) | 31 | (9) | |
Twenty per cent of females (n = 61) and 16% of males (n = 59) were on regular medications (Figure 2). The most commonly taken medication was thyroid hormone by the female divers (6%, n = 18). Anti-hypertensives (antiHT) were the most common taken by males (3%; n = 12). Only 0.6% of female respondents took this type of drug; however, 3% of females (n = 9) and 9% of males (n = 34) reported taking medication associated with cardiovascular diseases (CVD); antiHT, lipid lowering agents and antiplatelet drugs. Of these 43 divers, only one female and seven males had been assessed by a dive physician. One female diver was on antiepileptic drugs and she had not received any medical advice.
Figure 2.
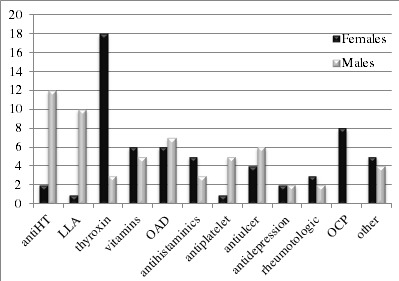
Numbers of respondents by gender reporting regular medications; AntiHT – hypertension medication; LLA – lipid lowering agent; OAD – oral anti-diabetics; OCP – oral contraceptive pills (not all respondents answered the questions)
Middle ear and/or sinus barotrauma were reported by eight females and 11 male divers. One male had a penetrating injury made by a sharp object during diving.
DECOMPRESSION SICKNESS
Five confirmed DCS cases were reported. One female diver had neurological DCS. One male was a commercial diver and developed DCS during a work dive, two males reported having neurological DCS about twenty years previously and one had had non-neurological DCS. None of these divers had any signs or symptoms of chronic disease or were on any medication, but the male divers were all overweight. Of the three females and 11 males who reported having had 'DCS-like' symptoms, one female and eight males had a BMI ≥ 30. Otherwise they were all healthy and none were on medication. Neither DCS nor reported DCS-like symptoms were statistically significantly different in occurrence between the sexes. The rate of physician-diagnosed DCS per 1,000 dives was 0.015 for females and 0.017 for males (n.s.). The rates of reported DCS-like symptoms per 1,000 dives also did not differ statistically between the sexes.
DATA SPECIFIC TO FEMALES
Twenty-one (7%) female divers reported undergoing cosmetic surgery of some type, of which four were silicone implants. None reported having problems related to these surgeries during diving.
Ninety-nine per cent of female divers (n = 299) answered the questions about children. Twenty-one per cent (n = 62) were mothers, with a total of 72 children and one still birth. Fifty-one females had one child and 11 females had two children, none had three or more. Of the 72 children, 41 were boys and 31 were girls.
Sixty of the 62 mothers answered the question about their children’s birth. Fifty-six of the first-born children were healthy and on time while four were premature. There was a history of diving during the first trimester for two of these premature births. All of the second children (n = 11) had a full-term birth. One hundred and two females replied to the question "did you dive during pregnancy" and seven stated that they dived in the first trimester. Of these seven pregnancies, one ended in a still birth and two ended with premature births (as mentioned above).
With regards to menstruation, 285 females answered the related questions. Of these, 90% (n = 255) usually complained of pain or discomfort during menstruation.
Regardless, 74% (n = 212) had dived during menstruation and did not encounter related problems. Of the 180 females who used tampons in daily life, 71% (n = 127) also used them during diving and none reported experiencing a complication during or after diving. Nine female divers took oral contraceptive pills (OCP) and none of these divers had been diagnosed with decompression sickness (DCS) or reported experiencing DCS-like symptoms.
Discussion
Whilst there was a higher number of male than female respondents, this response rate is not completely representative of the proportion of male divers reported by Turkish national certification data (79 %), nor by global data (72%). This may be owing to a male reluctance to complete surveys.[ 6 , 12 , 13] Female respondents were significantly younger than the males, which is in general agreement with data from other countries.[ 2 , 8 , 12] In comparison to data from a study conducted 10 years previously in Turkey, there was no significant change in the female divers' mean age (P = 0.13), but the mean BMI of the present group was significantly higher (P = 0.01).[ 5] There are no previous data to compare these results to for male divers.
DIVING HISTORY
Our findings suggest that in the decade since our first study on female divers, the mean time elapsed since learning to dive had lengthened by three years and the mean number of dives had increased three-fold.[ 8] It appears that Turkish female divers are now more actively involved in and continue diving after training. Despite this increase, males were still more experienced, with their mean time since learning to dive and the number of dives performed per year being significantly higher; 50% of female divers made less than 100 dives whereas the majority of males made over 100.
This probably reflects that 40% of males but only 15% of female respondents were diving instructors. This also reflects the data from other countries, where males have higher certifications and more dives per year.[ 8 , 14]
Whilst about two-thirds of divers reported making safety stops for all dives (including those not requiring decompression), only about half defined the nature of the stops used, e.g., at 3–5 msw for 3–5 minutes. Further research is needed, perhaps using depth-time loggers, before we can have a better understanding of the types of safety stops undertaken by recreational divers in Turkey.
Significantly more male than female divers performed decompression dives and did not adhere to recreational depth limits. It is not known whether this behaviour is related to overconfidence arising from experience or if it stems from cultural issues. However, many female divers also seem to violate recreational dive rules. This general noncompliance by divers in Turkey may well reflect an inadequacy in the training programmes offered by local diving schools. Unfortunately, 232 (32%) of respondents did not answer this question, so this result may not be representative of the diver population as a whole. These findings are worthy of further study.
HEALTH ISSUES
Smoking was as prevalent among female divers as among male divers (35% and 34% respectively) but had declined from 10 years previously (42%). This decrease seems promising, but smoking in divers is still greater than that observed in the general female population (25% in 2002, and 15% in 2010).[ 15 , 16] Conversely, smoking among male divers was less prevalent than in the general male population (48%).[ 16] When compared with other diving populations, such as the UK and Australia, smoking amongst Turkish divers is much commoner.[ 12 , 13] This is probably owing to increased awareness in other countries of the risks of smoking both for diving and generally.
Alcohol consumption among Turkish divers is not excessive and not very different from previously reported groups.[ 12 , 13] However, a considerable number of divers, especially males, drink before diving despite evidence that diving under the influence of alcohol increases the risk of diving incidents.[ 17] None of the questions asked if problems had occurred during a dive due to alcohol consumption beforehand.
The use of thyroid hormone in female divers is in line with that of the general Turkish population.[ 18] Endemic iodine deficiency (ID) from lack of iodine in natural resources is a major health problem in Turkey; it causes impairment of thyroid hormone synthesis and so hypothyroidism, and is more common among females. Despite a mandatory salt iodization programme being initiated after severe ID was reported in the 1990s, severe to moderate ID persists in Turkey, along with a few other countries in the region.[ 18 , 19]
An inconsistency was evident between the cardiovascular diseases reported and cardiovascular medication used. Cardiac disease was reported by only 13 divers (five female and eight male), whereas 43 reported that they were taking cardiovascular medication. Similar usage is reported from other countries, but an adequate comparison with the general Turkish population could not be made as there are no clear national data available on cardiac diseases and dyslipidaemia or medication use.[ 12 , 13] However, hypertension and diabetes are more comprehensively studied. The prevalence of HT in the general population for both women and men is 30%, but in the present study, only 4% of male divers and fewer than 1% of female divers were reportedly taking anti-HT treatment. Even fewer reported having hypertension. These results are significantly lower than observed in the general Turkish population (P < 0.0001). Divers who reported being treated for diabetes were also less common than found in the general population (14%).[ 20]
One important implication identified was that Turkish divers may be at increased risk during diving due to a high prevalence of CVD and associated conditions. Divers Alert Network (DAN) report that a history of CVD and age greater than 40 years constitute one fourth of disabling injuries in diving fatalities.[ 21] Fifty-five per cent of male Turkish divers were of age 35 or older and 10% were already on CVD medication. Additionally, smoking and obesity are factors known to increase the risk for cardiac incidents.[ 22] In the present study, 34% of male respondents were smokers, 50% were overweight and 12% were obese or morbidly obese. In this regard, Turkish male divers seem to have an increased risk for cardiac injury.
Fitness to dive assessments were not commonly sought by Turkish divers. Evaluations made by a physician trained in diving medicine were even less common. Some people continue to dive with medical conditions that may have a negative impact on diving safety. Without more dive medicals, it cannot be established whether participants are fit to dive or not. Similar situations are reported from other countries where health clearance is based on self declaration.[ 12 , 13] It may be necessary to review the safety implications of the current system in Turkey.
DECOMPRESSION SICKNESS
There are few data about DCS occurrence in Turkish divers. In a previous study, DCS cases treated with recompression were analyzed but these were not specific to recreational diving.[ 23] In a more recent Turkish study, of 132 recreational divers, DCS was reported by three (2.2%).[ 24] This was higher than that in our study (0.8%). Further analysis of the relationship between DCS occurrence and factors like experience, diving depths and weight/BMI could not be carried out, as the group with confirmed DCS was too small.
There has been long-term discussion over the effect of sex, if any, on the occurrence of DCS.[ 9] Recently, diving was shown to induce inflammatory changes which may have a role in DCS.[ 25] There is cumulative evidence that inflammation pathways and cells work differently in females and males especially after exercise.[ 26] Also, it is known that female hormonal cycles modulate endothelial functions that have been shown to be impaired by bubbles.[ 25 , 27] Therefore, sex may still be a relevant issue for DCS. In this study, physician-diagnosed DCS and DCS-like symptoms were slightly more prevalent in male divers than females but, given the small numbers, no inferences can be made from this survey. Nevertheless, our results are consistent with previous studies that have reported lower intravascular bubbles counts in females and a higher incidence of DCS in male divers.[ 9 , 14 , 28]
DATA SPECIFIC TO FEMALES
The mean age, maternity rate and number of children of female divers were consistent with the general Turkish population of the same socio-economic status.[ 29] Whether diving influences an infant's sex has long been a speculative topic. However, we found no statistical difference between the proportion of male to female offspring born to Turkish diving mothers and that in the general Turkish population.[ 30]
Diving during pregnancy is not advised due to possible deleterious effects on foetal development.[ 31] Of seven women who dived during the first trimester, one had a stillbirth and two babies were born prematurely. Once again, it is not possible to comment on the effect of diving while pregnant, given the small numbers in this survey.
Safety of diving during menstruation is a concern for many women. Mucosal congestion may predispose divers to barotrauma.[ 7] Moreover, there are studies showing that the incidence of DCS may increase during the first phase of menstruation.[ 27 , 32] However, the women in our study did not report any diving-related diseases while menstruating.
None of the female divers who were taking oral contraception (OCP) pills (OCP) reported any related problems. Interestingly, OCP use among the general Turkish female population (6%) is twice that reported by the divers (3%) in this study.[ 33] This differs from European countries, where the rate of OCP use among divers is similar to or higher than the general female population (around 30%).[ 9 , 34 , 35] The low use of OCPs among Turkish females is not unexpected, and is explained by cultural differences; traditional contraceptive methods are commoner in Turkey.[ 33] However, the fact that OCP use in divers is half that of the general population is surprising; this trend has only been reported in one other country (Australia; 9% in divers, 30% in the general population), but their uptake is still much higher than in Turkish female divers.[ 12 , 35] It was thought that OCPs could heighten DCS risk and contraindicate diving because of an increased risk of thromboembolism. However, there is insufficient data to support this claim.[ 7] Whether this anecdotal belief or cultural factors influenced the lower uptake of OCPs within the Turkish female diving population needs further investigation.
LIMITATIONS
This study has some limitations: mainly potential selection bias, limited numbers and incomplete survey responses. Most of the participants left one or two questions unanswered, thus there was a different number of respondents for every question, which might impair the consistency of the results. To avoid selection bias and confusion, the number of 'no response' answers for each question was also reported. Surveys of this type may also be subject to recall bias and verification of the data is not possible. Nevertheless, anonymous surveys may have benefits compared to face-to-face surveys; the participants may be less likely to conceal medical conditions or dangerous diving practices, and so might provide less biased data.
Conclusion
This is the first large-scale recreational diving survey profiling female and male Turkish divers. Turkish divers are like those of other countries in terms of demographic composition, diving practices and medical conditions. Similarly, they continue diving with medical conditions that may contraindicate diving and most are not examined for fitness to dive. Consequently, dive organizations and local federations should probably consider regulating medical screening for divers. There are clear differences between Turkish female and male divers in their demographic characteristics, experience levels and diving behaviour. Safe diving practices seemed to be neglected by both genders, though more commonly by males. This neglect might indicate that the training standards of local dive schools, which are also relatively new to the industry, should be reviewed and regulated better. No statistical differences between females and males were found in the rates of confirmed DCS and DCS-like symptoms. However, it should be noted that this study did not evaluate susceptibility to DCS and does not rely on objective observations, but self-reported data only.
Footnotes
Acknowledgement
The authors would like to thank Peter Buzzacott for his invaluable help in developing and improving this manuscript.
Funding and conflicts of interest: nil
Contributor Information
B Mirasoglu, Istanbul Faculty of Medicine, Underwater and Hyperbaric Medicine Department.
S Aktas, Istanbul Faculty of Medicine, Underwater and Hyperbaric Medicine Department.
References
- Sports and Fitness Industry Association . Silver Springs MD: SFIA; 2015. [cited 2016 March 12]. Participation in recreational diving report 2015 . Available from: https://www.sfia.org/reports/331_Scuba-Diving-Participation-Report-2015. [Google Scholar]
- PADI Worldwide Corporate Statistics 2016 . [cited 2017 May 18]; Available from: https://www.padi.com/sites/default/files/documents/about-padi/statistics/PADI_2016_WW_Statistics.pdf.
- Brıtısh Sub-Aqua Club annual diving incident reports for 2014 through 2016 . [cited 2016 July 15]; (restricted access) Available from: https://www.bsac.com/page.asp?section=1038.
- Lippmann J, Lawrence C, Fock A, Jamieson S, Harris R. Provisional report on diving-related fatalities in Australian waters in 2011 . Diving Hyperb Med. 2016;46:207–240. [PubMed] [Google Scholar]
- Aktas S, Isıl S, Isler H. [Underwater Sciences and Technology Meeting Proceedings, 1998, Dec 12−13] Istanbul: Istanbul Tıp Fakültesi; 1998. Türk kadın dalıcıları dalıs profili anketi (Turkish female divers profile survey). Sualtı Bilim ve Teknolojisi Toplantısı Bildiriler Kitabı 1998 Aralık 12−13 ; pp. 130–138. [Google Scholar]
- Istanbul: 2015. TSSF 2014 yılı aktivite raporu [Turkish Underwater Sports Federation 2014 activity report] . [Google Scholar]
- Edmonds C, Bennett M, Lippman J, Mitchell S. Diving and subaquatic medicine 5th ed. Boca Raton FL: CRC Press; 2015. [Google Scholar]
- St Leger Dowse M, Bryson P, Gunby A, Fife W. Comparative data from 2250 male and female sports divers: diving patterns and decompression sickness . Aviat Space Environ Med. 2002;73:743–749. [PubMed] [Google Scholar]
- Boussuges A, Retali G, Bodere-Melin M, Gardette B, Carturan D. Gender differences in circulating bubble production after SCUBA diving . Clin Physiol Funct Imaging. 2009:400–405. doi: 10.1111/j.1475-097X.2009.00884.x. [DOI] [PubMed] [Google Scholar]
- TSSF. Donanımlı Dalıs Yönetmeligi. Resmi Gazete. Sayı: 26993. [Turkish Underwater Sports Federation, SCUBA diving regulations. Official gazete no. 26993] . [cited 2016 April 7];2008 Available from: http://www.resmigazete.gov.tr/eskiler/2008/09/20080910-10.htm.
- Profesyonel Sualtı Adamları Yönetmeligi. Resmi Gazete. Sayı:23098. [Professional Diving Regualtions. Official gazete no 23098] . [cited 2016 March 12];1997 Available from: http://www.resmigazete.gov.tr/eskiler/2008/02/20080215-6.htm.
- Taylor DM, O'Toole KS, Ryan CM. Experienced, recreational scuba divers in Australia continue to dive despite medical contraindications . Wilderness Environ Med. 2002;13:187–193. doi: 10.1580/1080-6032(2002)013[0187:ersdia]2.0.co;2. [DOI] [PubMed] [Google Scholar]
- St Leger Dowse M, Waterman MK, Penny CE, Smerdon GR. Does self-certification reflect the cardiac health of UK sport divers? . Diving Hyperb Med. 2015;45:184–189. [PubMed] [Google Scholar]
- Ranapurwala SI, Bird N, Vaithiyanathan P, Denoble PJ. Scuba diving injuries among Divers Alert Network members 2010-2011 . Diving Hyperb Med. 2014;44:79–85. [PubMed] [Google Scholar]
- Emri S, Basoglu A, Turnagöl A, et al. Istanbul, Turkey: Military Cultural Center; 2003. Epidemiology of smoking among Turkish adults: a national household survey, 2002. The Second International Symposium on Medical Geology, Nutrition, and Cancer, March 31−April 03, 2003. ; pp. 33–36. [Google Scholar]
- Ankara: Anıl Press; 2010. Global Adult Tobacco Survey, Turkey Report, 2010, In: Primary Health Care General Directorate. Ministry of Health publication number: 803 . [Google Scholar]
- Davis M. The Editor's offering. Alcohol and scuba diving . Diving Hyperb Med. 2012;42:193–10. [PubMed] [Google Scholar]
- Erdogan MF, Agbaht K, Altunsu T, Ozbas S, Yucesan F, Tezel B, et al. Current iodine status in Turkey . J Endocrinol Invest. 2009;32:617–622. doi: 10.1007/BF03346519. [DOI] [PubMed] [Google Scholar]
- WHO Nutrition . The WHO Global Database on Iodine Deficiency. 2008 . [cited 2017 May 18]; Available from: http://www.who.int/vmnis/en/.
- Satman I, Omer B, Tutuncu Y, Kalaca S, Gedik S, Dinccag N, et al. Twelve-year trends in the prevalence and risk factors of diabetes and prediabetes in Turkish adults . Eur J Epidemiol. 2013;28:289–296. doi: 10.1007/s10654-013-9771-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mitchell SJ, Bove AA. Medical screening of recreational divers for cardiovascular disease: consensus discussion at the Divers Alert Network Fatality Workshop . Undersea Hyperb Med. 2011;38:289–296. [PubMed] [Google Scholar]
- Pougnet R, Di Constanzo L, Lodde B, Henckes B, Dherbecourt L, Lucas D, et al. Cardiovascular risk factors and cardiovascular risk assessment in professional divers . Int Marit Health. 2012;63:164–169. [PubMed] [Google Scholar]
- Toklu AS, Cimsit M, Yildiz S, Uzun G, Korpinar S, Sezer H, et al. Decompression sickness cases treated with recompression therapy between 1963 and 1998 in Turkey: review of 179 cases . Undersea Hyperb Med. 2014;41:217–221. [PubMed] [Google Scholar]
- Ozdemir L, Duru-Asiret G, Bayrak-Kahraman B, Henckes B, Devrez N, Akbayir A, et al. Health-related adverse events and associated factors in recreational divers with different certification levels . J Travel Med. 2013;20:289–295. doi: 10.1111/jtm.12059. [DOI] [PubMed] [Google Scholar]
- Lambrechts K, Balestra C, Theron M, Henckes A, Galinat H, Mignant F, et al. Venous gas emboli are involved in post-dive macro, but not microvascular dysfunction . Eur J Appl Physiol. 2017;117:335–344. doi: 10.1007/s00421-017-3537-9. [DOI] [PubMed] [Google Scholar]
- Abbasi A, de Paula Vieira R, Bischof F, Walter M, Movassaghi M, Berchtold NC, et al. Sex-specific variation in signaling pathways and gene expression patterns in human leukocytes in response to endotoxin and exercise . J Neuroinflammation. 2016;13:289. doi: 10.1186/s12974-016-0758-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- St Leger Dowse M, Gunby A, Phil D, Moncad R, Fife C, Morsman J, et al. Problems associated with scuba diving are not evenly distributed across a menstrual cycle . J Obstet Gynaecol. 2006;26:216–221. doi: 10.1080/01443610600555261. [DOI] [PubMed] [Google Scholar]
- Klingmann C, Gonnermann A, Dreyhaupt J, Vent J, Praetorius M, Plinkert PK. Decompression illness reported in a survey of 429 recreational divers . Aviat Space Environ Med. 2008;79:123–128. doi: 10.3357/asem.2126.2008. [DOI] [PubMed] [Google Scholar]
- TR Ministry of Development and TUBITAK . Ankara: Elma Teknik Basım Matbaacılık Ltd; 2014. The 2013 Turkey Demographic and Health Survey. In: Hacettepe University Institute of Population Studies . [Google Scholar]
- Turkish Statistical Insititute; 2015. [cited 2016 March 15]. 2014 Birth statistics. TUIK news bulletin no:18621 . Available from: http://www.turkstat.gov.tr/PreHaberBultenleri.do?id=18621. [Google Scholar]
- Conger J, Magann EF. Diving and pregnancy: what do we really know? . Obstet Gynecol Surv. 2014;69:551–556. doi: 10.1097/OGX.0000000000000105. [DOI] [PubMed] [Google Scholar]
- Lee VM, St Leger Dowse MS, Edge C, Gunby A, Bryson P. Decompression sickness in women: a possible relationship with the menstrual cycle . Aviat Space Environ Med. 2003;74:1177–1182. [PubMed] [Google Scholar]
- Istanbul: Cortex Iletisim Hizmetleri AS; 2012. [Turkish oral contraception guide]. (Türkiye Oral Kontrasepsiyon Kılavuzu) . [Google Scholar]
- St Leger Dowse M, Gunby A, Moncad R, Fife C, Smerdon G, Bryson P. The combined oral contraceptive pill and the assumed 28-day cycle . J Obstet Gynaecol. 2007;27:481–484. doi: 10.1080/01443610701405671. [DOI] [PubMed] [Google Scholar]
- United Nations . Ankara: Elma Teknik Basım Matbaacılık Ltd; 2014. [cited 2017 May 18]. TWorld contraceptive pattern 2013 . Available from: http://www.un.org/en/development/desa/population/publications/pdf/family/worldContraceptivePatternsWallChart2013.pdf. [Google Scholar]